
Abstract
Background:
A symmetrical gait affords the most efficient walking pattern. Bionic prostheses should provide better gait symmetry than mechanically passive prostheses with respect to a nonpathological gait.
Objectives:
To compare the basic temporal–spatial parameters of gait in transfemoral amputees fitted with bionic or mechanically passive prosthetic knees with those of subjects with a nonpathological gait.
Study design:
Three-dimensional gait analysis using an optoelectronic device.
Methods:
Eight transfemoral amputees participated in the study. Subjects walked across two dynamometric platforms a total of 15 times. Movement kinematics were measured using optoelectronic stereophotogrammetry.
Results:
The swing time of the affected limb in patients fitted with a mechanically passive knee joint was longer than that of the nonaffected limb by 0.055 s (effect size = 1.57). Compared with the control group, the swing time of the prosthetic limb in patients fitted with a mechanically passive knee was longer by 0.042 s (effect size = 2.1). Similarly, the stance time of the nonaffected limb was longer by 0.047 s (effect size = 1.07).
Conclusions:
Compared with a mechanically passive knee joint, a bionic knee joint evinced gait symmetry. Both the stance time and the swing time for amputees with a bionic knee were similar to those of nonamputees.
Clinical relevance
Prosthetists aim to design prostheses that achieve a good symmetry between the healthy and affected limbs. The use of bionic technology achieves a level of symmetry approaching that observed in nonamputees.
Introduction
Approximately 200–500 million amputations are performed annually worldwide. Amputation of the lower extremities accounts for approximately 85% of these. 1 About half of all amputations are transtibial; the rest are through-knee disarticulations or transfemoral.2,3 Loss of a part of the lower limb results in the inability to walk without a prosthesis. A functional prosthesis is the most important method of restoring locomotion. Regarding above-knee amputations, prosthetic knee joints must substitute the function of the human knee joint to enable stable weight transfer during the stance phase and controlled movement during the swing phase. The appropriate choice and use of prosthetic components, which provide increased stability under difficult conditions, are essential to improve safety, function, and quality of life. 4
The development of new technologies has resulted in improvements in prosthetic knee design. Modern prosthetic knees use a microprocessor to control the stance and swing phases. Intelligent prosthetic designs also use bionic technology. The cardinal objective of a bionic prosthesis is to reproduce the natural functions of the lost limb, and to restore normal sensory and locomotor drive after amputation. Bionic knee designs use artificial intelligence to adapt continuously to the user’s walking style and to the external environment. Artificial intelligence systems transmit a constant flux of output signals to the prosthetic parts, thereby controlling performance and providing optimal function. 5 Based on parameters such as knee position, angular velocity, and load, which are measured during walking, the microprocessor of the bionic joints with magnetorheological fluid modulates the strength of a magnetic field, which changes the fluid viscosity to effectively increase or decrease the resistance during the swing and stance phases. 6 Mechanically passive designs rely on manual adjustments made by the prosthetist during the fitting process. 6
New prosthetic knee designs are supposed to provide amputees with greater comfort, and achieve symmetry between the nonaffected and affected limbs. During nonpathological gait, the stance and swing times of the right and left limbs are very similar. As far as pathological gait is concerned, these parameters may differ significantly between limbs, which leads to an arrhythmic gait pattern. 7 Temporal–spatial parameters, and their symmetry between limbs, are the basic characteristics of gait. Measuring gait asymmetry in amputees relative to nonamputees is the first step in identifying the degree of asymmetry that is acceptable for a prosthetic gait during rehabilitation. 8 Several studies compared gait patterns among transfemoral amputees wearing different types of prosthetic knee joint;9–13 however, most of the subjects were given only a short time to become accustomed to the new type of prosthetic knee design, and they moved at their own “natural speed,” which was different in many cases.9–11 Berry 6 suggested that the gait of subjects fitted with a microprocessor-controlled knee joint is more natural and symmetrical than that of subjects wearing other prosthetics. Nevertheless, no study has compared microprocessor-controlled knee joints and mechanically passive knee joints with respect to a nonpathological gait. Thus, the objective of this study was to compare basic temporal–spatial gait parameters and symmetry in amputees using the bionic knee joint with those in patients wearing a mechanically passive knee joint with respect to a nonpathological gait. To reduce the effect of potentially confounding variables, all subjects walked at identical range of speed.14–16
Methods
Participants
Eight subjects (four females and four males; age = 38.2 ± 6.1 years; height = 171.3 ± 5.5 cm; and weight = 68.5 ± 8.0 kg) with a transfemoral amputation participated in the study. Six of the subjects had an amputation of the right lower limb, and two had an amputation of the left lower limb. Four were fitted with a bionic (Rheo, Őssur, Reykjavik, Iceland) knee joint (two females and two males), while the others used a mechanically passive (Mauch SNS) knee joint based on hydraulic technology. All the subjects fell into the third activity level (high impact level) by the Össur company. 11 Subjects with mechanically passive knee joint were candidates for a bionic knee joint. All other prosthetic equipment was of a similar type (Solid Ankle Cushion Heel (SACH) foot, ischial containment socket). All of the patients had been using the prosthetic knee joint for more than 2 years. The control group was selected from 50 individuals who participated in a gait analysis. The control group comprised 10 subjects without pathology (8 males and 2 females; aged = 27.6 ± 5.2 years; height = 175.2 ± 6.8 cm; and weight = 70.1 ± 6.1 kg) whose natural walking speed corresponded to that of the amputees. All subjects provided written informed consent. The study was approved by the Ethics and Research Committee of the Human Motion Diagnostic Center, University of Ostrava.
Protocol
Due to an insufficient number of people using the expensive bionic knee joint, the research was conducted over a long period of time (from 2008 to 2012). This enabled a minimum of eight similar patients with a transfemoral amputation to be enrolled and compared. Each subject visited the Human Motion Diagnostic Center twice on two different days per month. On each day, after the initial training runs (three to five attempts), the participants performed 15 trials along a 16 m walkway, which contained the force plates embedded in the floor to ensure that they met the conditions for an optimal step cycle. Only those trials in which the footsteps of both limbs fell entirely on either the right or left force plate were considered valid. Participants were instructed to walk at self-selected walking velocity, but only trials at a speed ranging from 1.09 to 1.21 m/s were considered valid. Gait speed was controlled online using wireless photocells. The selected speed range was representative of the speed at which most transfemoral amputees move. 11 If neither of the two above-mentioned conditions were met, the trial was repeated.
Calibration markers were placed (bilaterally) on the lateral and medial malleoli, the medial and lateral femoral condyles, the greater trochanter, and on the first and fifth metatarsal heads. The tracking and calibration markers were positioned to define the trunk (the left and right acromion), the pelvis (both iliac crests, both posterior superior iliac spines, and both anterior superior iliac spines), both thighs, both shanks (four light-weight rigid plates holding a quaternion of reflexive markers), and both feet (a triad of markers on the heel (over the calcaneus)).
Measurements
Two dynamometric platforms (Kistler 9286AA and 9286BA, Kistler Instrumente AG, Winterthur, Switzerland) fitted with an integrated repeater and connected to an analog/digital (A/D) converter (5691A) and a compatible computer were used to measure the impact force distribution. Furthermore, a set of seven infrared cameras (Qualisys, Oqus 100, Qualisys AB, Göteborg, Sweden), which were connected to an A/D converter and temporally and spatially synchronized with the force plates, were used for kinematic analysis. The recording frequency of the cameras was 247 Hz.
Data analysis
Qualysis Track Manager (QTM) software was used to acquire kinematic data. In addition, Visual3D v4 software (C-motion, Germantown, MD, USA) was used to create the models and for data processing. Particular segments of the lower limb were modeled as truncated cones. The local coordinate system for the thigh, shank, and leg was derived from calibration videos made during stance phase. Temporal instants of the right and left heels at initial contact with the surface and the toe off were determined from the records of the retro-reflective markers located on the feet. 17 Step time is time between the event labels representing contralateral heel strike to ipsilateral heel strike. Stance time is time between the event labels representing ipsilateral heel strike to ipsilateral toe off. Swing time is time between the event labels representing ipsilateral toe off to ipsilateral heel strike.
Statistical analysis
The symmetry index (SI) was used to assess gait symmetry

SI values can range from −100% to +100%, where SI = 0 represents absolute symmetry. 8 The effect size (ES) was used to assess practical significance. The ES values were as follows: 0–0.2, insignificant effect; 0.2–0.6, low effect; 0.6–1.2, mean effect; 1.2–2.0, high effect; 2.0–4.0, very high effect; and ≥4.0, excellent effect. 18 The Shapiro–Wilk test was applied to verify the normality of data distribution. Furthermore, the reliability of the measurements was verified using intraclass correlation coefficients (ICCs). In addition, the average relative typical measurement error for the temporal–spatial parameters was calculated for both the affected and nonaffected limbs and expressed as a percentage. 19
It was found out that the ICC value was higher than 0.85 in all observed variables, and the relative typical measurement error was lower than 4% in all monitored variables.
Results
The step time for the affected limb in subjects using a mechanically passive knee joint was longer than that of the nonaffected limb by 0.055 s (ES = 1.57). A significant difference was evident in the swing phase; the swing time of the prosthetic limb was 0.063 s longer than that of the nonaffected limb (ES = 1.75) (Table 1).
Comparison of temporal parameters of gait between the nonaffected (N) and affected (A) limb when using the bionic knee joint (Rheo, ES R) and mechanically passive knee joint (Pasiv, ES P).
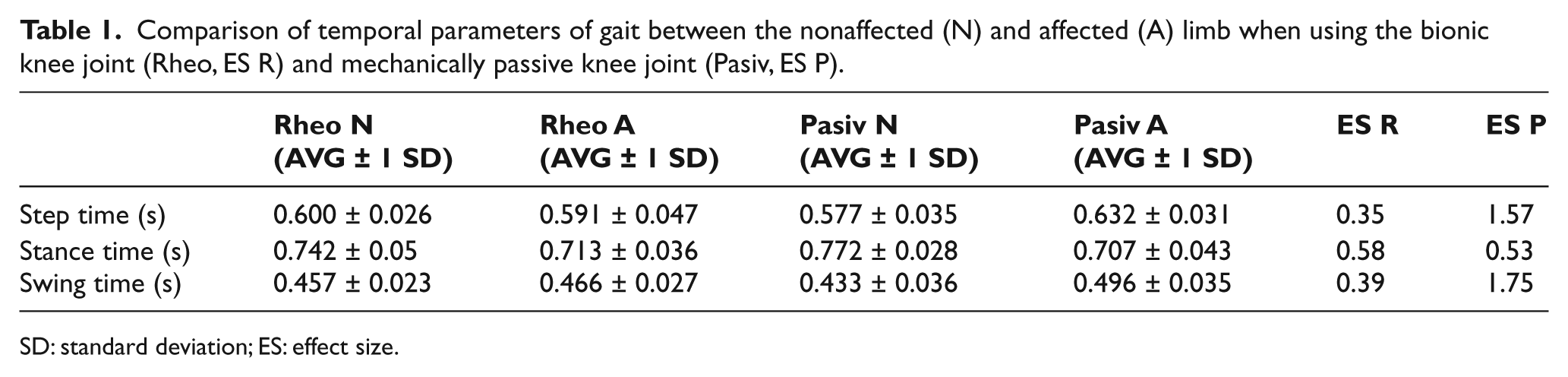
SD: standard deviation; ES: effect size.
The bionic knee showed a shorter swing time (0.03 s; ES = 0.87) and a shorter step time (0.041 s; ES = 1.1) than the mechanically passive design (Table 1). The SI values for the chosen temporal and spatial parameters revealed better gait symmetry for the bionic knee joint. The results also showed that the step length in amputees was longer on the prosthetic side, but that the stance time was longer on the nonaffected side (Table 2).
SIs for chosen temporal–spatial quantities (SI Rheo—bionic knee joint, SI Pasiv—mechanically passive knee joint, SI Control—control group). ES 1 marks the difference in parameters between the bionic knee joint and the control group. ES 2 represents the difference between the mechanically passive amputee and the control group parameters.
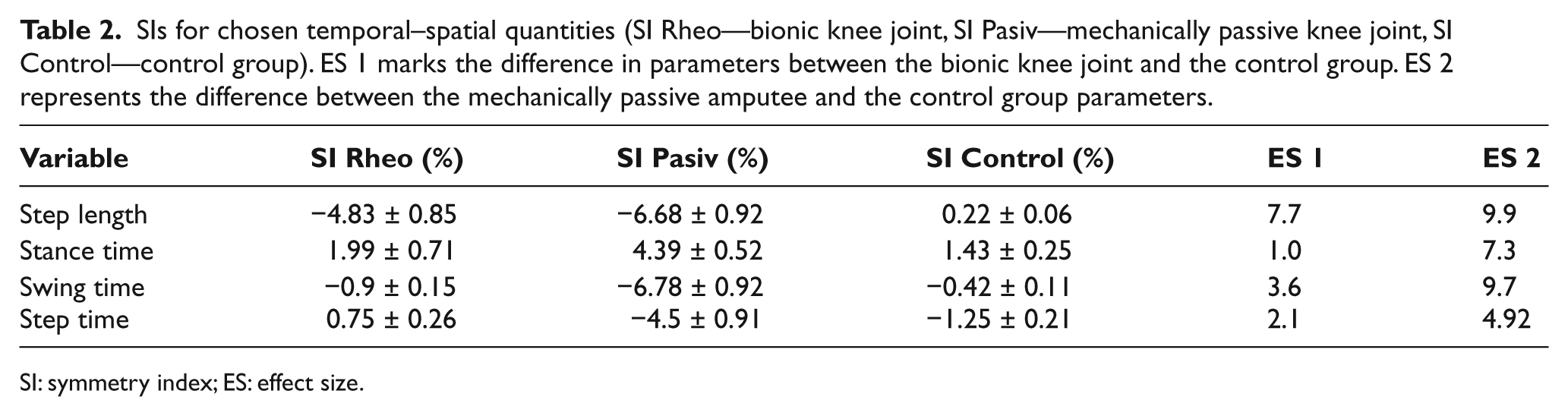
SI: symmetry index; ES: effect size.
The swing time for the amputated limb in patients fitted with a mechanically passive knee joint was 0.042 s longer than that in the control group, and showed a very high effect (ES = 2.1). Also, the stance phase of the nonaffected limb was 0.047 s longer, and showed a high effect (ES = 1.07). By contrast, we did not detect a high effect in bionic knee amputees when we compared their temporal gait parameters with those of the control group. The step length of the affected limb in both groups of prosthetic patients was longer, and showed a high effect for bionic group (ES = 1.65) and very high effect for mechanically passive group (ES = 2.82). The step cadence of the subjects fitted with a mechanically passive knee joint was also greater than that of the control group (Table 3). With respect to ES, the gait pattern of the subjects fitted with bionic or mechanical prostheses primarily differed from that of subjects in the control group in terms of the swing phase of the prosthetic limb. The swing phase was significantly longer for patients wearing mechanical prostheses than that of patients in the bionic group and the control group.
Comparison of the temporal–spatial parameters of gait in bionic knee amputees (Rheo) and mechanically passive patients (Pasiv) with the control group. The differences are expressed by the ES. ES Rheo marks the difference in parameters between the bionic knee joint and the control group. ES Pasiv represents the difference between the mechanically passive amputee and the control group parameters.
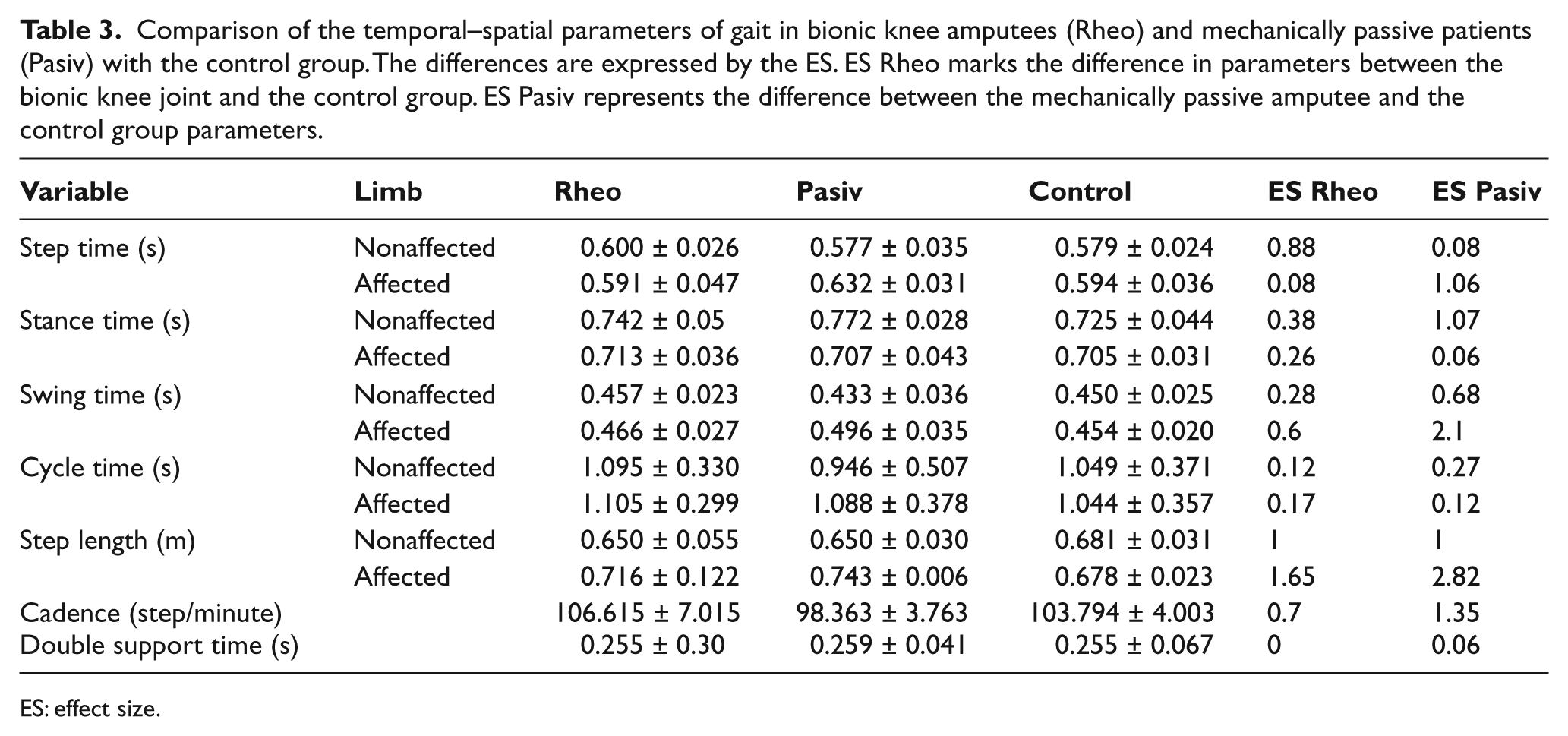
ES: effect size.
ICC value was higher than 0.85 in all observed variables, and the relative typical measurement error was lower than 4% in all monitored variables.
Discussion
The aim of this study was to examine differences in the temporal–spatial gait characteristics and gait symmetry in amputees using different types of prosthetic knee joint. A symmetrical gait is thought to afford the most efficient walking pattern. 20 Gait asymmetry is considered to indicate pathology. 21 For unilateral amputees, a symmetrical gait is important to prevent excessive loading of the intact leg. 14 Asymmetry appears to be a relevant measurement for investigating the gait characteristics of amputees, and for assessing their risk of future joint pain and degeneration. 14 The results showed that the difference between the step time of the affected and nonaffected limbs was smaller in subjects with a bionic knee, which contributed to better gait symmetry. This was further confirmed by the SI, which reached 4% for the bionic knee joint. Only step length reached 4.83%, a value (±4%) considered to indicate natural symmetry. 22 Silver-Thorn and Glaister 23 reported differences in speed, cadence, step length, stance time, and swing time in five subjects using two different prosthetic knee joints. Their results showed that the stance time of the affected limb was shorter, whereas the swing time of the prosthetic limb was longer. The shorter stance time for the prosthetic limb is most likely attributable to the reduced stability afforded by the prosthesis. 24 Our results suggest that the stance time for the nonaffected limb in subjects with a mechanically passive knee joint was longer than that in subjects fitted with a bionic knee joint. We believe that this may indicate the greater stability of microprocessor-controlled knee joints. In addition, it was also evident from the measurements that the swing time of the affected limb was longer for subjects with a mechanically passive knee joint, which may result in greater energy expenditure when walking. 25 Furthermore, Johansson et al. 11 reported that energy expenditure by patients wearing a microprocessor-controlled knee joint while walking was lower than that by subjects wearing a mechanically passive knee joint. This may be due to the shorter swing time associated with bionic prostheses. We therefore hypothesize that the shorter swing time associated with bionic knee designs may be related to an improved moment of inertia and the correct timing of flexion and extension during the swing phase. The gait of subjects fitted with a bionic knee joint demonstrated better temporal and spatial parameters than that of subjects fitted with the mechanically passive joint. We believe that this can be beneficial, as it may result in reduced loading of the iliac joint and spine. Further detailed studies are needed to examine the kinetics of bionic, mechanical, and unaffected lower limb joints further. Such studies may help to explain gait asymmetry and to identify the mechanisms underlying joint function during gait.
Conclusion
The results of this study suggest that bionic prostheses result in better gait symmetry than mechanically passive prostheses. They also show that the stance and swing times for bionic knee joints approximate to those of nonamputees. It is therefore concluded that the temporal and spatial gait characteristics of subjects wearing a bionic knee joint are more similar to those of subjects with a nonpathological gait than those of patients wearing a mechanical prosthesis were. Bionic knees allow an individual with a transfemoral amputation to walk in a manner similar to an able-bodied individual. This should be taken into account when selecting prosthetic knee joints.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by IGS Grants 6108/2010 and 6113/2011 of the University of Ostrava, research grant of Silesian region RRC/04/2009 and research grant No MSM 6198959221 of the Ministry of Education, Youth and Sport, Czech Republic, “Physical activity and inactivity of inhabitants of the Czech Republic in the context of behavioral changes.”