
Abstract
In able-bodied individuals, the ankle joint functions to provide shock absorption, aid in foot clearance during the swing phase, and provides a rocker mechanism during stance phase to facilitate forward progression of the body. Prosthetic ankles currently used by persons with lower limb amputations provide considerably less function than their anatomical counterparts. However, increased ankle motion in the sagittal plane may improve the gait of persons with lower limb amputations while providing a more versatile prosthesis. The primary aim of this study was to examine and quantify temporal-spatial, kinematic, and kinetic changes in the gait of four male subjects with bilateral trans-femoral amputations who walked with and without prosthetic ankle units. Two prosthesis configurations were examined: (i) Baseline with only two Seattle LightFoot2 prosthetic feet, and (ii) with the addition of Endolite Multiflex Ankle units. Data from the gait analyses were compared between prosthetic configurations and with a control group of able-bodied subjects. The amputee subjects' freely-selected walking speeds, 0.74 ± 0.19 m/s for the Baseline condition and 0.81 ± 0.15 m/s with the ankle units, were much less than that of the control subjects (1.35 ± 0.10 m/s). The amputee subjects demonstrated no difference in walking speed, step length, cadence, or ankle, knee, and hip joint moments and powers between the two prosthesis configurations. Sagittal plane ankle range of motion, however, increased by 3–8° with the addition of the prosthetic ankle units. Compared to the control group, following initial contact the amputee subjects passively increased the rate of energy storage or dissipation at the prosthetic ankle joint, actively increased the power generation at the hip, and increased the extension moment at the hip while wearing the prosthetic ankle configuration. The amputee subjects increased the power generation at their hips, possibly as compensation for the reduced rate of energy return at their prosthetic ankles. Results from subject questionnaires administered following the gait analyses revealed that the prosthetic ankle units provided more comfort during gait and did not increase the perceived effort to walk. The subjects also indicated that they preferred walking with the prosthetic ankle units compared to the Baseline configuration. The results of the study showed that the prosthetic ankle units improved sagittal plane ankle range of motion and increased the comfort and functionality of the amputee subjects’ prostheses by restoring a significant portion of the ankle rocker mechanism during stance phase. Therefore, prosthetic ankle mechanisms should be considered a worthwhile option when prostheses are prescribed for persons with trans-femoral amputations.
Introduction
The anatomical ankle joint and foot in able-bodied individuals are integral components of a complex system of joints, muscles, and limbs that operate simultaneously and efficiently during walking. The foot aids in absorption of shock forces and provides the base on which individuals stand and walk. The ability of the ankle joint to rotate in three dimensions enables it to provide multiple functions during gait, including shock absorption, aiding foot clearance, and providing coordinated motion with the foot during the stance phase of gait to create a functional rocker shape and facilitate forward progression of the body. Persons with lower limb amputations are typically fitted with prosthetic feet that provide considerably less function than their anatomical counterparts, which probably contribute to their walking at slower speeds (James and Oberg 1973; Waters et al. 1976; Huang et al. 1979; Boonstra et al. 1993, 1994; Ruhe 2004) and with higher energy expenditure (Waters et al. 1976; Huang et al. 1979; Wainapel et al. 1985; Crouse et al. 1990; Boonstra et al. 1994; Wu et al. 2001; Perry et al. 2004) compared to able-bodied individuals. Of the studies that have been published concerning amputee gait biomechanics, several have evaluated the biomechanical effects of different prosthetic feet (Gitter et al. 1991; Colborne et al. 1992; Arya et al. 1995; Underwood et al. 2004), but few have specifically considered the effect of prosthetic ankle mechanisms on gait (Cappozzo et al. 1980; Wirta et al. 1991; Zmitrewicz et al. 2006). While these aspects of prosthetic research are beneficial in determining the prosthetic components that best reproduce characteristics of able-bodied gait, improve symmetry, or generally restore gait aesthetics, they do not necessarily provide any quantitative results that foster a more in-depth understanding of amputee gait biomechanics.
Several studies have reported on the qualitative nature of rehabilitation programs for bilateral trans-femoral amputees (Watkins and Liao 1958; Hunter and Holliday 1978; Doraisamy et al. 1983; Volpicelli et al. 1983; Evans et al. 1987), but there have been no quantitative gait analyses reported in the literature that have examined specifically how different prosthetic components affect their gait performance. Lower limb amputees and, in particular, bilateral trans-femoral amputees, may benefit from having prosthetic ankle units in their prostheses to increase motion in the sagittal plane and potentially improve prosthetic function during stance phase. There is, unfortunately, a lack of research investigating the quantitative effect of prosthetic ankle devices on the gait of this population. Investigating kinematic and kinetic variables at the prosthetic ankle, prosthetic knee, and sound hip will facilitate understanding of how prosthetic ankle motion influences gait. Moreover, examining persons with bilateral amputations is advantageous because it eliminates sound limb compensatory effects that typically occur in studies involving unilateral amputees. Therefore, the data are presumed to better indicate deficiencies in prosthetic mechanisms that may prevent amputees from walking with patterns that more closely resemble those of able-bodied persons.
The purpose of the present study was to determine if the addition of prosthetic ankle motion would improve gait in persons with bilateral trans-femoral amputations. This study addresses the lack of quantitative investigations of walking performance in users of prosthetic ankle devices. It was hypothesized that the prosthetic ankle units would allow prosthesis users to walk with increased functionality and with gait characteristics that more closely resemble their able-bodied counterparts. It was also hypothesized that the addition of the prosthetic components would enable the amputee subjects to walk with joint moments and powers that better approximated those of able-bodied individuals. In particular, the prosthetic ankle was expected to add an energy storage and return mechanism to the system that would reduce differences between joint moments and powers of the amputee and able-bodied subjects.
Methods
Study participants
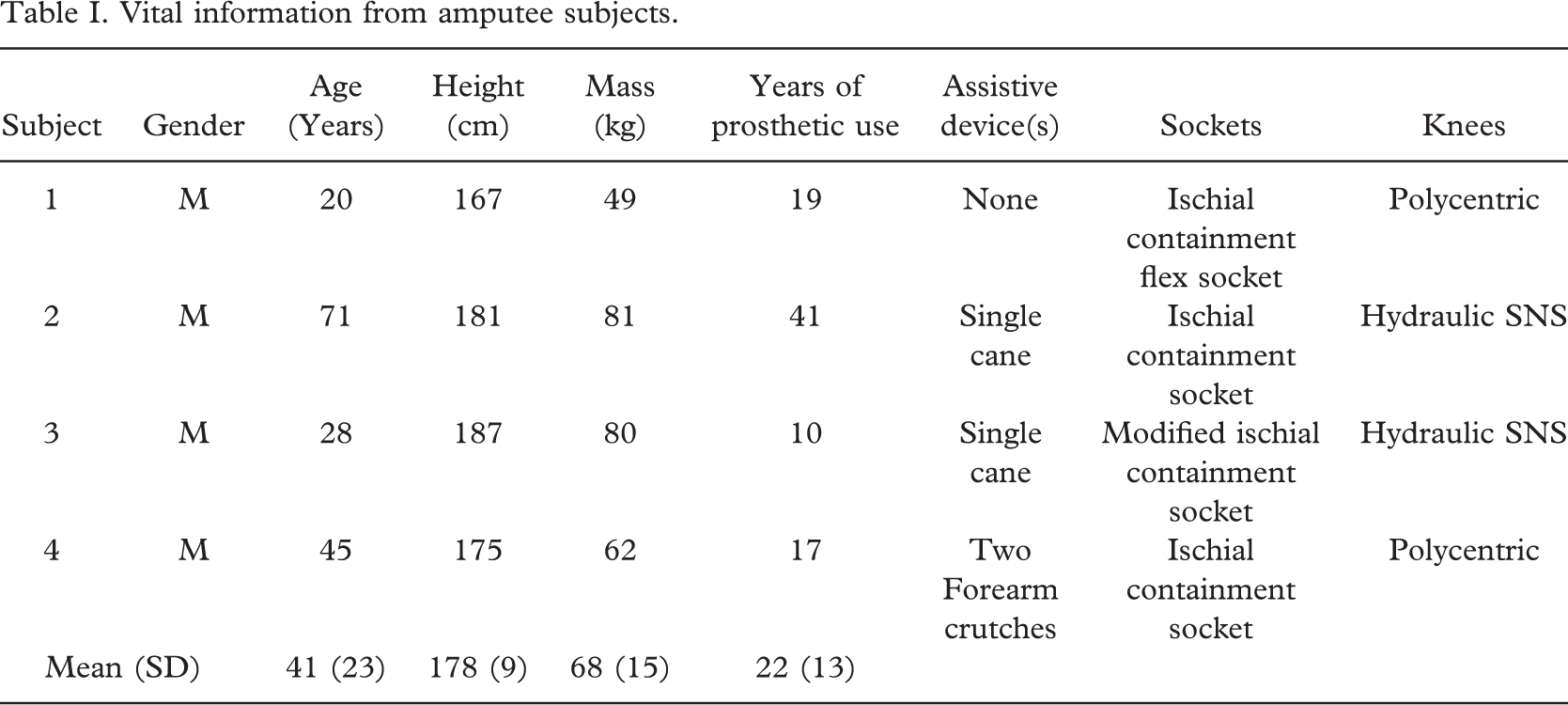
The study included four male subjects with bilateral trans-femoral amputations who used their prostheses daily. The age of the participants was 41 ± 23 (mean ± SD) years and their mean mass was 68 ± 15 kg. The mean time of prosthetic use was 22 ± 13 years (Table I). The aetiology of limb loss was due to congenital deformity in one subject, and the other three subjects had amputations due to trauma. Three of the subjects normally walked with assistive devices, two subjects walked with a single cane and one subject used two forearm crutches, but one subject used none. Prior to testing, all of the study participants provided informed consent that was approved by the Northwestern University Institutional Review Board.
Data from nine able-bodied ambulators were used from previous studies (Konz et al. 2004; Miff 2004) to form a group of control subjects for comparison with the amputee subjects’ data. The control group consisted of eight males and one female. The group's mean age and mass were 28 ± 4 years and 80 ± 13 kg, respectively. During their gait evaluations the able-bodied subjects were asked to walk at three self-selected speeds, slow, freely-selected, and fast.
Data collection and processing
Gait analyses were performed at the VA Chicago Motion Analysis Research Laboratory (VACMARL). Kinematic data were sampled at 120 Hz using eight Eagle Digital Real-Time cameras (Motion Analysis Corporation, Santa Rosa, CA). Three-dimensional position data were acquired from reflective markers placed on the body in the Helen Hayes configuration (Kadaba et al. 1990) using hypoallergenic double-sided tape. Raw marker position data were edited and smoothed with EVa Real-Time (Motion Analysis Corporation, Santa Rosa, CA) using a second-order bi-directional Butterworth filter with an effective cutoff frequency of 6.0 Hz (Winter 1990). Kinetic data were sampled at 960 Hz using six force platforms from Advanced Mechanical Technology, Inc. (Watertown, MA) that were mounted flush with the floor. The gait data were averaged and compiled using OrthoTrak software (Motion Analysis Corporation, Santa Rosa, CA) and custom programs written in MATLAB® (Version 6.5.0, MathWorks, Inc, Natick, MA).
All subjects were fitted with two Seattle LightFoot2 prosthetic feet at least two weeks prior to the first gait analysis. No other component of their prostheses was changed or modified (Table I). In the Baseline gait analysis, the amputee subjects walked with only the pair of Seattle LightFoot2 prosthetic feet at three self-selected walking speeds, slowest, freely-selected, and fastest, for data collection. A minimum of five ‘clean’ trials per speed per subject were collected. To be accepted as a clean trial, initial contact and ipsilateral toe-off were required to occur (without interference from the contralateral foot and/or assistive device) on a single force platform. The amputee subjects were then fitted with a pair of Endolite Multiflex Ankles, which allow passive ankle dorsiflexion/plantarflexion, and given another two-week accommodation period before returning to VACMARL to repeat the experimental gait analysis procedure. Subjective questionnaires were administered to the study participants following each gait analysis to assess their opinions of the two prosthesis configurations. Subjects were allowed to keep any or all of the prosthetic components upon completion of the study.
Joint moments were derived using an inverse dynamics model that used kinematic and ground reaction force data as input. The sign convention used in this study was such that, generally, extension moments were positive and flexion moments were negative (Winter 1990). Joint powers were derived from the net moments acting at the joint and were found using the following equation:

where M is the net moment at the joint and, ω is the angular velocity. At the prosthetic ankle and knee joints, negative powers denote the rate of energy storage or dissipation while positive powers denote the rate of energy return. At the anatomical hip joint, negative and positive powers reflect the rates of energy absorption and energy generation, respectively.
Results
Walking speed is known to affect the characteristics of gait. Only the slow walking speed of the able-bodied group was within the comfortable range of speeds recorded for the amputee group. Therefore, to reduce variation in the data that may result from differences in speed, kinematic and kinetic data were compared with the amputee subjects walking at their fastest speed (1.01 m/s) and the control group walking at their slow speed (0.93 m/s). Individual moment and power data from the amputee subjects are presented and compared with those from the control group. The terminology used to describe the energy bursts in the power profiles is consistent with that previously reported in the literature (Winter and Sienko 1988). Amputee data acquired from the left and right sides of the body were similar; thus, only the right side will be presented for analysis.
Temporal-spatial data
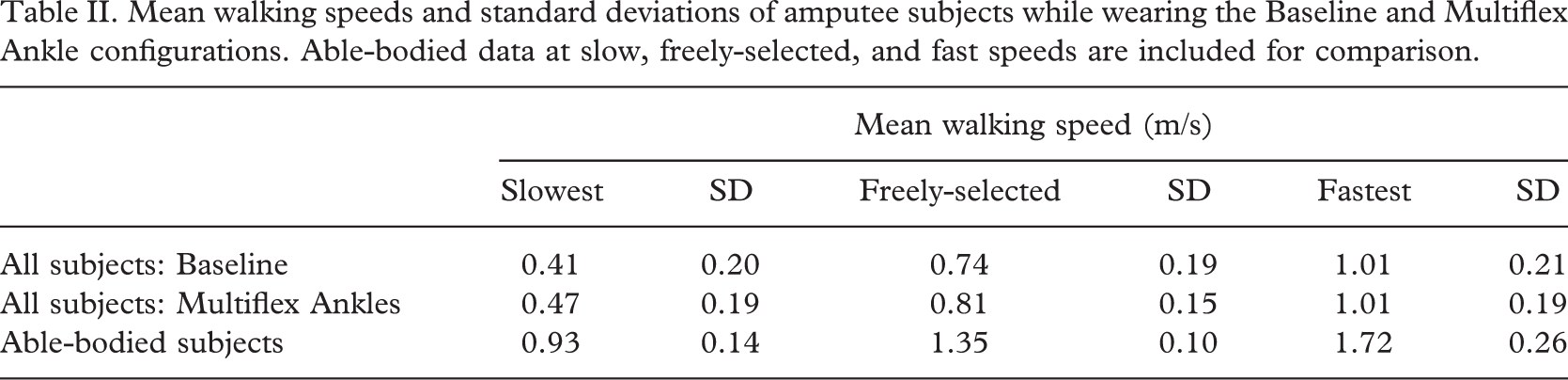
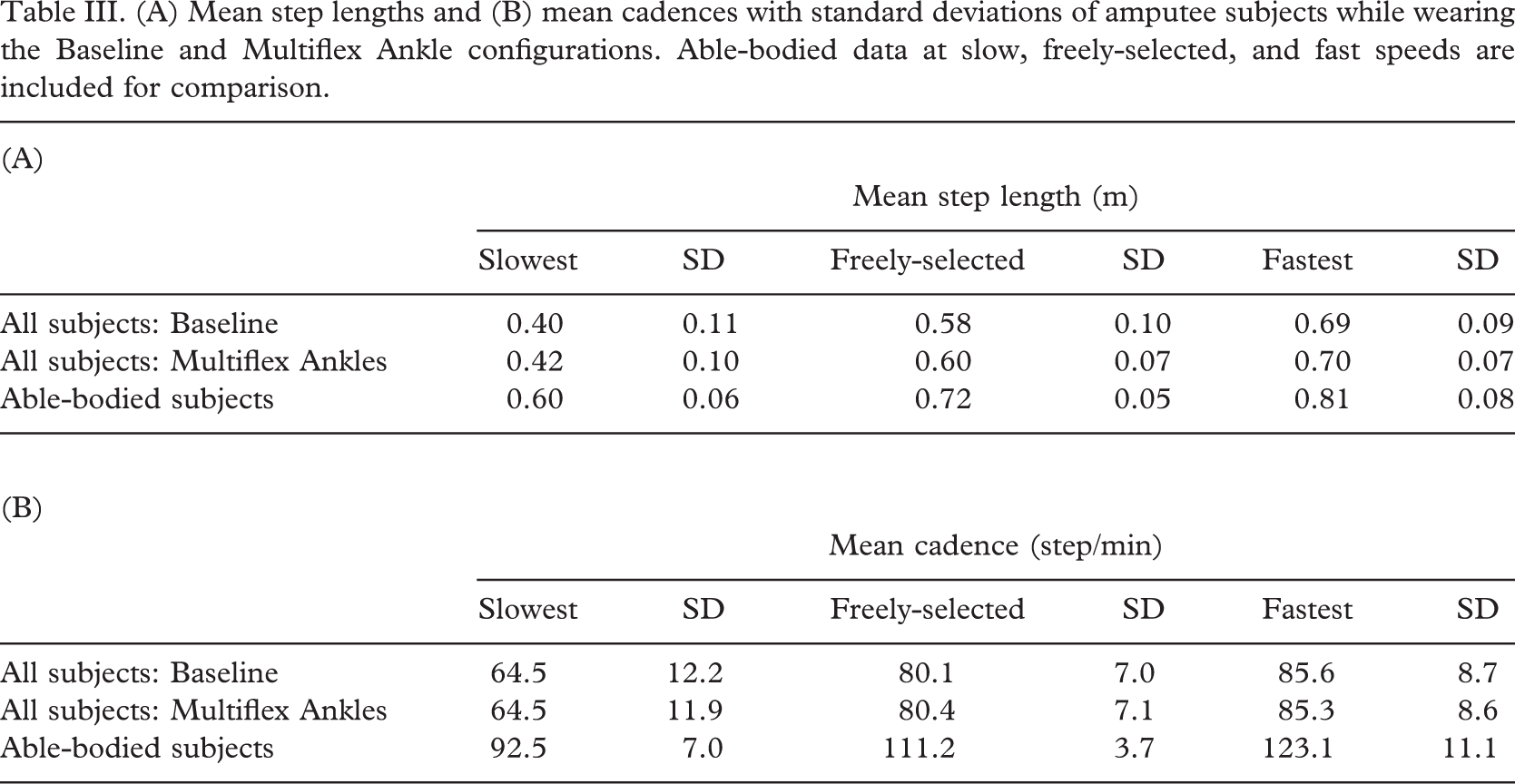
The results of this study showed that subjects with bilateral trans-femoral amputations walked more slowly than able-bodied individuals with the Seattle LightFoot2 prosthetic feet, and the speed did not change appreciably with the addition of the Multiflex Ankle units (Table II). Additionally, there was no difference in cadence or step length between the two prosthesis configurations (Table III). It should be noted that the amputee subjects generally took longer step lengths than the able-bodied controls for the speed-matched data (Table IIIA). Specifically, the step length of the amputee subjects walking at their freely-selected speeds (0.74–0.81 m/s) was similar to that of the able-bodied subjects walking at their slow speed (0.93 m/s), and the step length of the amputees at their fastest speed (∼0.70 m) was comparable to that of the control group walking at their freely-selected speed (0.72 m). However, the cadence demonstrated by the amputee group (∼85 step/min) was observed to be lower than that of the able-bodied group walking at their slow speed (∼93 step/min) (Table IIIB).
Vital information from amputee subjects
Mean walking speeds and standard deviations of amputee subjects while wearing the Baseline and Multiflex Ankle configurations. Able-bodied data at slow, freely-selected, and fast speeds are included for comparison
(A) Mean step lengths and (B) mean cadences with standard deviations of amputee subjects while wearing the Baseline and Multiflex Ankle configurations. Able-bodied data at slow, freely-selected, and fast speeds are included for comparison
Ankle motion
The mean sagittal plane ankle range of motion (ROM) of the control group during the stance phase of the gait cycle was 18°. The ankle ROM of the amputee group in the Baseline configuration was between 11 and 17°. While walking with the Multiflex Ankles, the amputee group's ankle ROM was increased to a range of 14–25°. Additionally, all of the amputee subjects had an ankle ROM at their fastest speed that was comparable to the able-bodied subjects at their slow speed (Figure 1). Ankle ROM was observed to increase with speed in all amputee subjects for both prosthesis configurations (Figure 2).
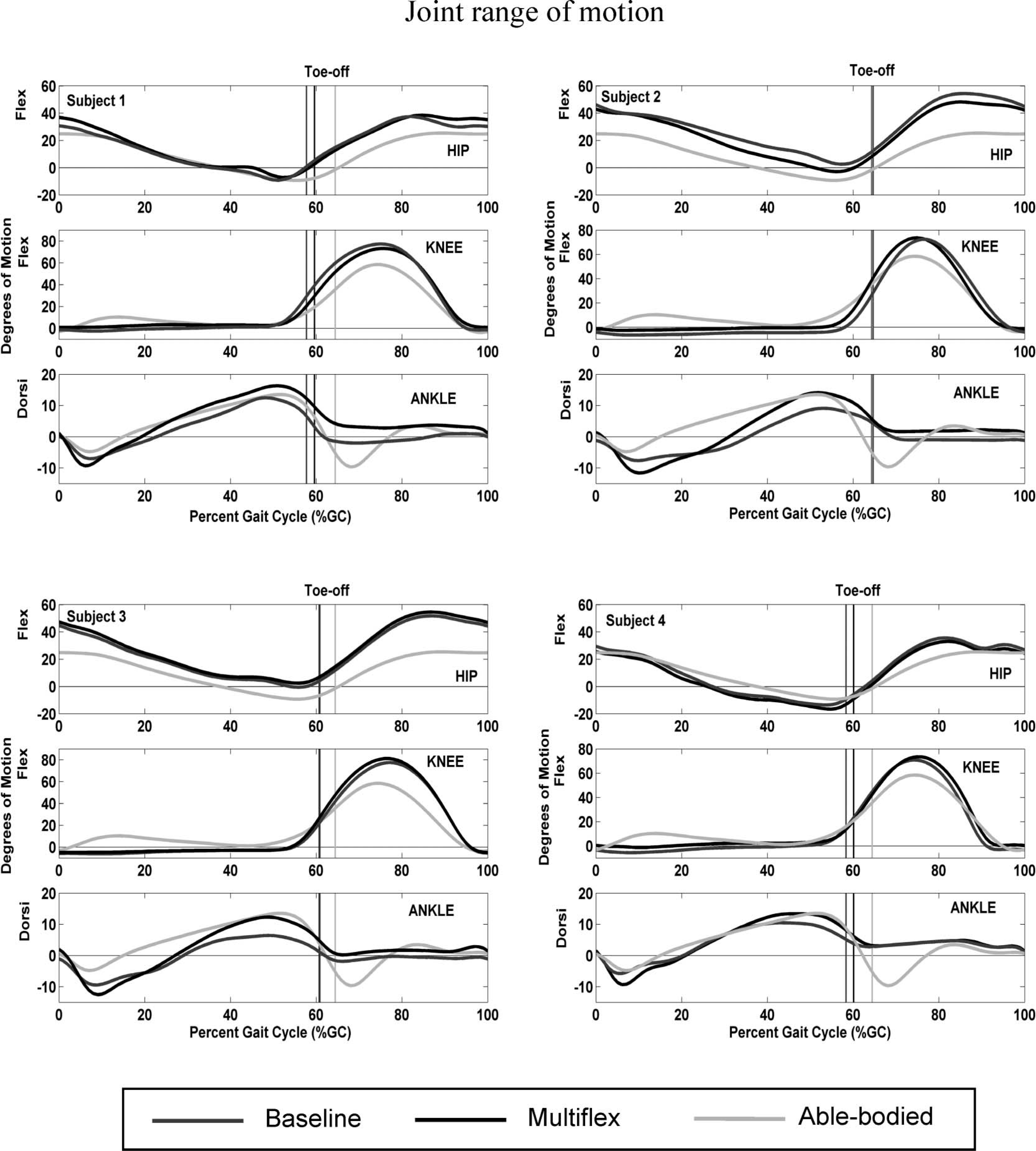
Mean sagittal plane joint range of motion plots of study participants while wearing the Baseline and Multiflex Ankle configurations at fastest walking speed (1.01 m/s). Able-bodied data at slow speed (0.93 m/s) is shown for comparison. Initial contact occurs at 0% and 100% of the gait cycle. The vertical lines denote ipsilateral toe-off.
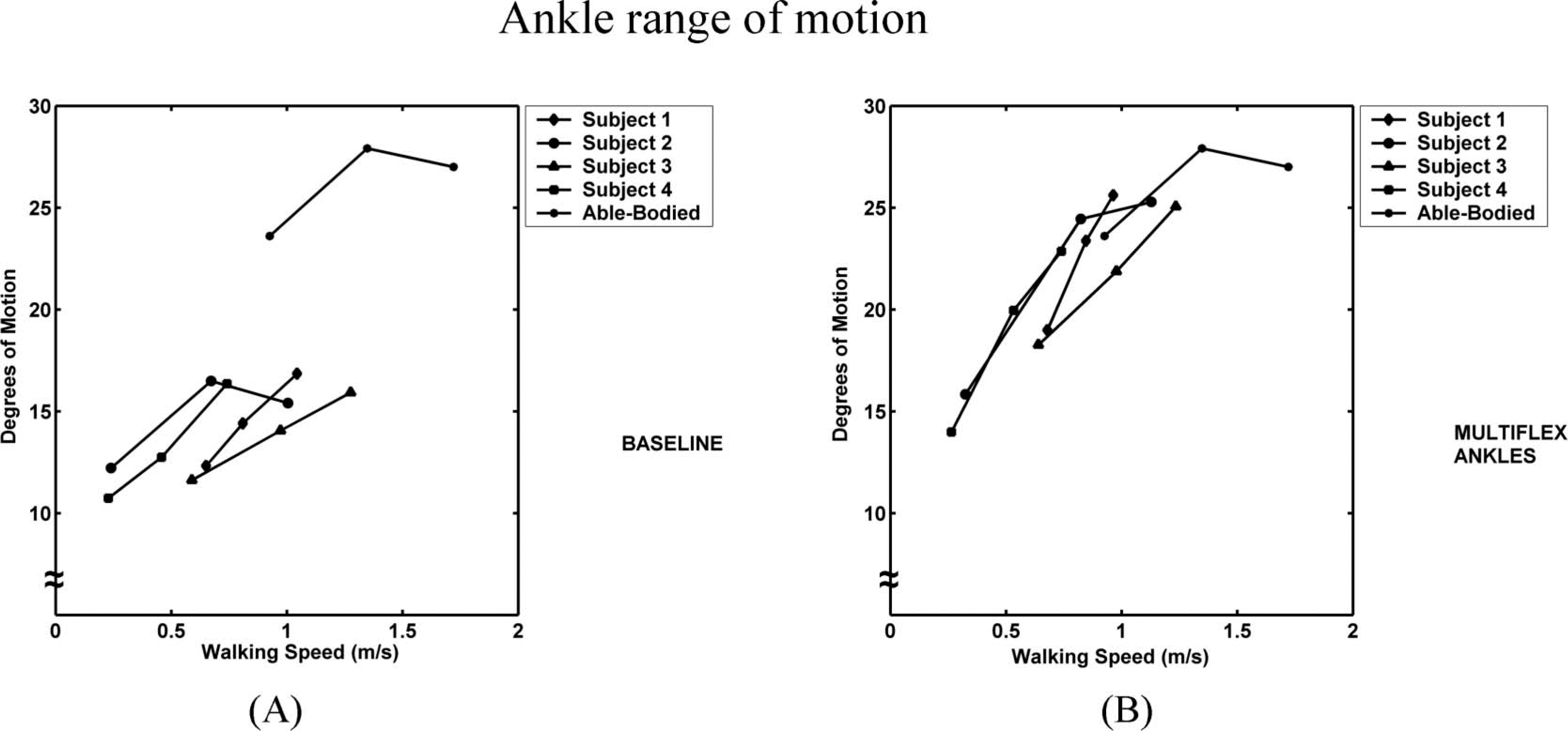
The sagittal plane ankle range of motion (ROM) plot of study participants wearing (A) the Baseline and (B) Multiflex Ankle configurations. The able-bodied ankle ROM plot is shown for comparison. Note the increase in ROM with the Multiflex Ankles compared to that of the Baseline configuration.
Ankle moments and powers
The prosthetic ankle units appeared to have little effect on the prosthetic ankle moment and power curves. As a group, the amputee subjects exhibited negative moments for the first 20% of the gait cycle during both the Baseline and Multiflex Ankle configurations (Figure 3). In contrast, the control subjects demonstrated negative moments only for the first 9% of the gait cycle. The amputee and control groups demonstrated similar peak moments per unit body mass in late stance at +1.1 Nm/kg and +1.3 Nm/kg, respectively.
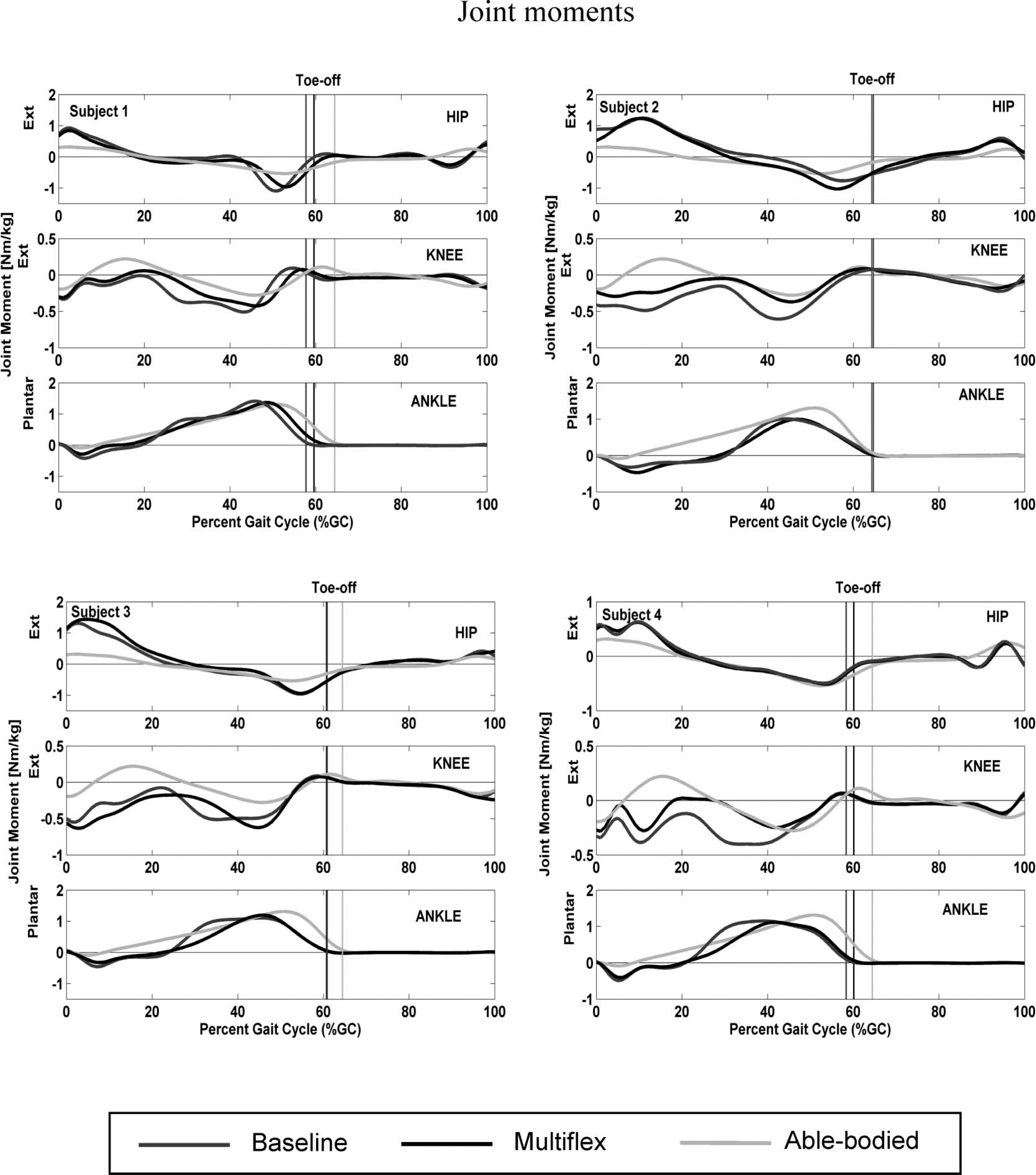
Sagittal plane moment profiles of the amputee subjects during fastest walking speed at the hip, knee, and ankle joints. Able-bodied data at slow speed is shown for comparison. Extension moments at the hip and knee joints, and plantarflexion moments at the ankle joint, are defined to be positive.
The sagittal plane ankle power magnitudes of the amputee subjects were generally smaller than those of the able-bodied control subjects and had greater variability between subjects (Figure 4). The amputee group exhibited a period of energy storage or dissipation at loading response prior to the A1 power peak in terminal stance. Between the peak at loading response and the A1 peak, the power was zero. The control group, however, increased their rate of energy absorption steadily during the first half of the gait cycle. The magnitudes of the A2 bursts were +0.4 J/kg·s and +1.6 J/kg·s for the amputee and control groups, respectively.
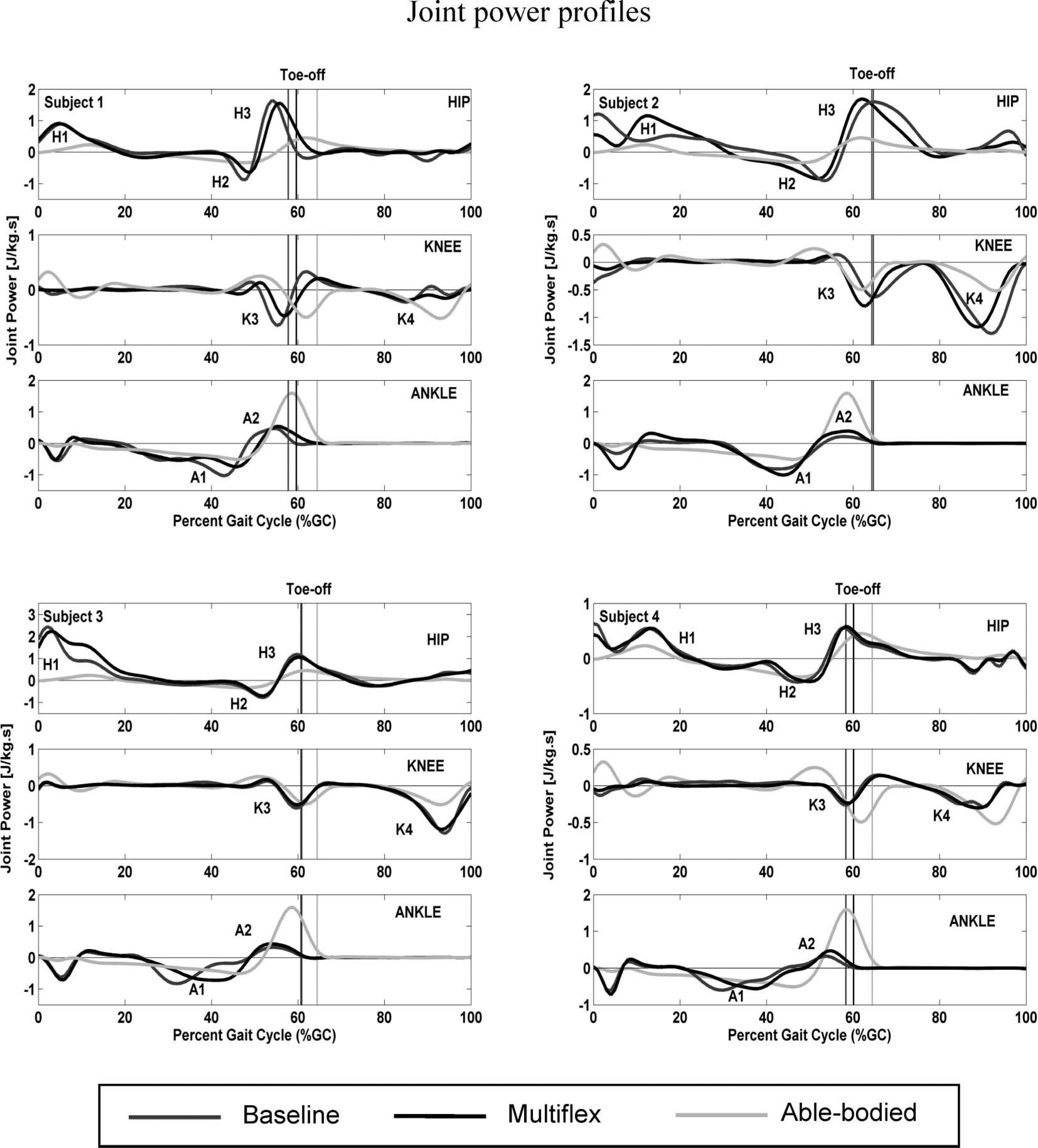
Sagittal plane joint power profiles of the amputee subjects during fastest walking speed at the hip, knee, and ankle joints. Able-bodied data at slow speed is shown for comparison. For the prosthetic ankle and knee joints in the amputee subjects, positive values denote the rate of energy return while negative values denote the rate of energy storage or dissipation. In able-bodied individuals and in the anatomical hip joints of the amputee subjects, positive and negative values represent power generation and power absorption, respectively.
Knee motion
Unlike the able-bodied group, the amputee group showed no sagittal plane knee flexion during stance phase. In swing phase the amputee subjects exhibited knee flexion, similar to the able-bodied group, with a mean maximum flexion peak of 74 and 75° while wearing the Baseline and Multiflex Ankle configurations, respectively. The mean flexion peaks of the able-bodied subjects during stance and swing phases were, respectively, 10 and 58°.
Knee moments and powers
The amputee group generally exhibited a negative moment throughout stance phase (Figure 3). In contrast, the control group demonstrated a positive moment followed by a negative moment in early to mid-stance. During late stance, the study participants exhibited a negative moment that was similar to the able-bodied subjects. There were no K1 (energy storage) or K2 (energy return) bursts in the amputee group (Figure 4). The amputee and control subjects both had similar K3 and K4 bursts just prior to toe-off and during late swing, respectively.
Hip motion
The amputee and control groups demonstrated similar sagittal plane hip motion curves, though the amputee subjects' curves tended to be offset slightly into flexion. The Multiflex Ankles did not appear to affect the pattern of the hip motion curve compared to that from the Baseline analysis. The amputee group exhibited hip ROM from 40–46° while wearing both prosthetic ankle configurations. The able-bodied hip ROM was 34° during the gait cycle.
Hip joint moments and powers
At initial contact, the amputee subjects exhibited a mean moment of +0.8 Nm/kg at the hip joint, which was more than twice that (+0.3 Nm/kg) observed in the able-bodied subjects (Figure 3). In mid-stance, the moment acting at the hip of the amputee subjects was approximately zero, a pattern that was similar to that of the able-bodied subjects. In terminal stance, the study participants demonstrated a negative moment similar to that of the control group. For most of swing phase the hip joint moments were comparable between the two groups, having a value of approximately zero.
The amputee group demonstrated a considerably higher rate of energy generation at the hip during early stance phase (+0.8 J/kg·s) compared to the able-bodied group's H1 burst magnitude (+0.2 J/kg·s) (Figure 4). The H2 power peak magnitudes were similar between the amputee and control groups, while the H3 power peak magnitudes were almost twice that of the control group. However, the amputee group's H3 bursts were highly variable relative to the H1 and H2 peak magnitudes.
Subject questionnaire
Subjects 1, 2, and 3 agreed that the prosthetic feet alone did not provide enough motion, while Subject 4 felt that the configuration provided too much motion (Table IV). Two subjects liked the Baseline configuration while the other two did not. None of the subjects indicated that the prosthetic ankle units decreased stability during standing, nor did they feel unstable during walking. Subjects 1, 3 and 4 agreed that the prosthetic ankles made it easier for them to walk on uneven ground and up an incline. Subjects 2, 3 and 4 agreed that the prosthetic ankles made the prostheses feel less rigid and did not increase the effort to walk. The general consensus among the study participants was that they perceived having the prosthetic ankle units in their prostheses improved their walking performance. Additionally, the subjects preferred the prosthetic ankle configuration to the Baseline configuration and chose to keep the ankle units at the conclusion of the study.
Summary of Questionnaire results
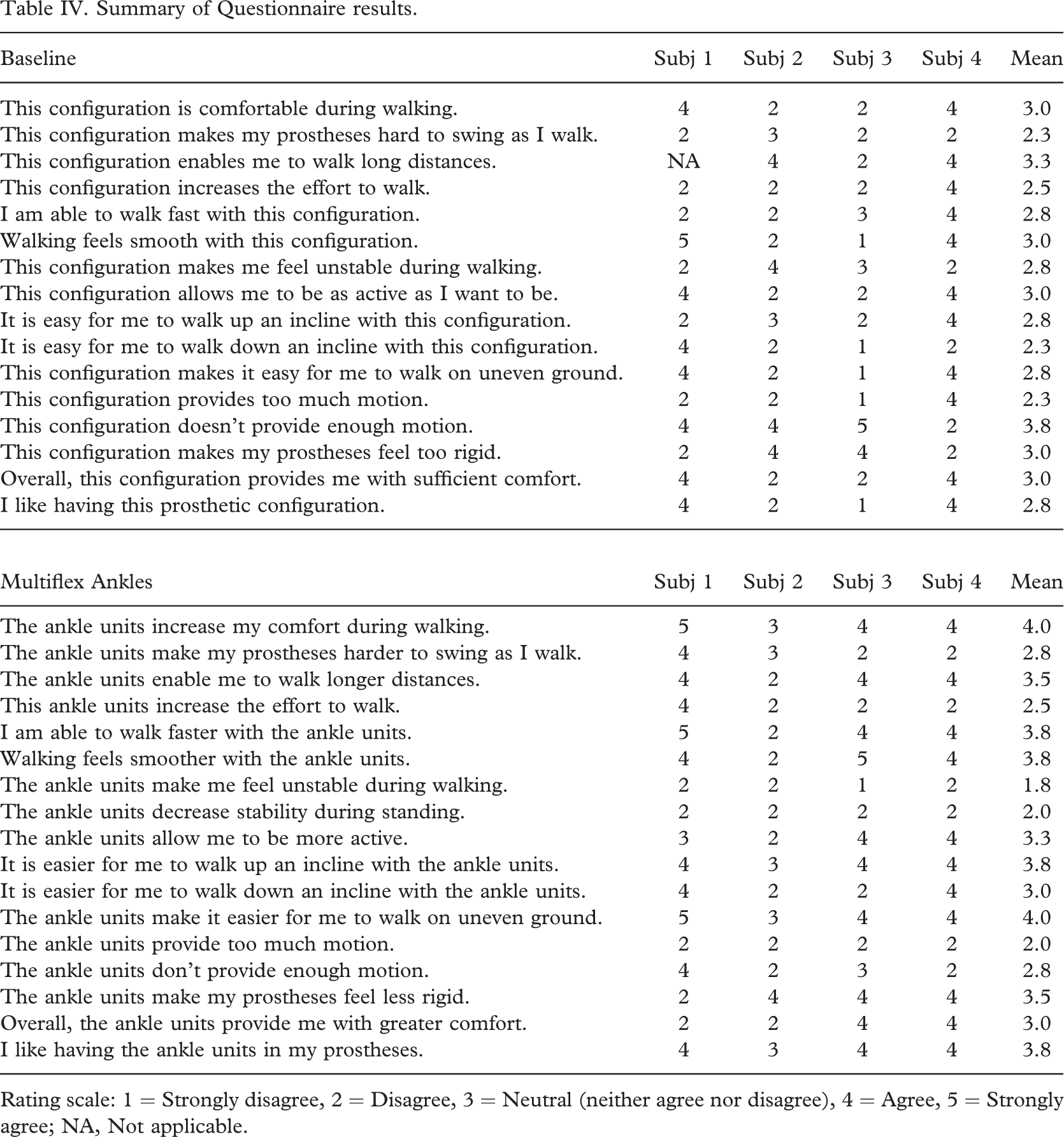
Rating scale: 1 = Strongly disagree, 2 = Disagree, 3 = Neutral (neither agree nor disagree), 4 = Agree, 5 = Strongly agree; NA, Not applicable.
Discussion
Compared to the able-bodied group, the study participants walked with slower self-selected walking speeds and lower cadences while wearing both the Baseline and Multiflex Ankle configurations. The addition of the prosthetic ankle units did not appear to affect speed, step length, or cadence in the amputee subjects. There were differences, however, in the amputee group's sagittal plane ankle motion between the Baseline and Multiflex Ankle configurations.
While wearing the Baseline configuration the amputee subjects' sagittal plane ankle ROM was considerably less than that of the able-bodied group since the rigid ankle-foot component limited the motion allowed in the sagittal plane (Figure 2A). It is important to note, however, that the perceived ankle dorsiflexion/plantarflexion, as determined by the motion analysis system included a relative measurement of the prosthetic foot's deflection as the amputee subjects rolled over the foot during single support stance. The motion measurement system calculated the ankle joint angle in the sagittal plane from the positions of the prosthetic foot and shank segments defined by the marker arrangement. Additionally, the Delrin® keel of the Seattle LightFoot2 was deflected by the ground reaction forces as the amputee walked. During loading response phase the amputee group transferred their body weight to the prosthetic foot, and the heel of the Seattle LightFoot2 compressed as the body rolled forward over the foot. The resulting compression was reflected as plantarflexion in the ankle motion curve. In mid-stance the body continued to roll over the foot, increasing compression of the keel. As a result, the forefoot marker position changed relative to the heel marker, which appeared as ankle dorsiflexion. Thus, the ankle rotation recorded for the Baseline condition reflected deformation of the prosthetic foot and the shoe during loading.
The amputee subjects increased their sagittal plane ankle ROM while wearing the prosthetic ankle units (Figure 2B). During their fastest walking speed Subjects 1, 2, and 3 were able to exhibit ankle ROM that was closer to that of the control group walking at their slow speed. The ankle units allowed the prosthetic feet to passively dorsiflex/plantarflex during loading. As stated previously, the ankle rotation measured by the motion measurement system was due to a combination of the bending of the keel in the prosthetic foot and the passive function provided by the prosthetic ankles, which was reflected as increased ankle ROM.
No appreciable differences were found between the ankle moment and power patterns from the Baseline and Multiflex Ankle configurations. There were, however, consistent differences between the amputee and control subject groups. In particular, the amputee subjects exhibited deviations from the able-bodied ankle moment curve during initial contact. For the amputees a positive moment was developed over the first 20% of the gait cycle, whereas for the normal subjects it was present only for the first 9% of the gait cycle (Figure 3). Able-bodied individuals are able to rapidly achieve foot flat and transfer load onto the leading leg during loading response phase in preparation for single support (Figure 1), and in doing so advance the centre of pressure under the foot to a position anterior to the ankle joint axis. Additionally, the occurrence of stance phase knee flexion in the able-bodied subjects (Figure 1) probably contributes to a reduction in the duration of their negative ankle moment (Figure 3). Therefore, due to the presence of the rigid ankle in the Baseline configuration and the passive function provided by the Multiflex Ankle configuration, combined with the lack of stance phase knee flexion, the study participants spent relatively more time rotating their prosthetic legs forward until foot flat was achieved compared to the control group. Thus, the duration of the ankle plantarflexion exhibited by the amputee group following initial contact was extended well into mid-stance (Figure 1).
The ankle power profiles of the amputee and control groups also revealed differences due to the relationship between joint moments and powers (Equation 1). The sagittal plane ankle power magnitudes of the amputee subjects were comparable to those reported in a previous study of unilateral trans-femoral amputees (van der Linden et al. 1999), but the magnitudes varied from those demonstrated by the control group. The elastic properties of the Seattle LightFoot2 prosthetic feet and the rubber bumper (which allows ankle dorsiflexion/plantarflexion) inside the Multiflex Ankles contributed to a significantly higher rate of energy storage/dissipation in the prosthetic ankle during loading response (Figure 4), having a magnitude that was approximately six times that of the control group. Similar to the able-bodied subjects, the amputee subjects exhibited an A1 power peak magnitude later in stance, which probably reflects the energy stored or dissipated in the prosthetic feet and ankle units. It appears that much of this energy was returned in the A2 phase (Figure 4). The A2 power peak magnitude of the study participants, however, was four times less than that of the able-bodied subjects, which reflected the low rate of energy returned at the prosthetic ankle prior to toe-off.
None of the amputee subjects exhibited stance phase knee flexion during gait, a consequence of their prosthetic knee designs. Perry (1992) noted that flexion at the knee joint during loading response provides shock absorption. The absence of stance knee flexion also affected the knee joint moments and powers of the amputee subjects. A negative knee moment, generally regulated via prosthetic design and/or prosthetic knee alignment, acted at the knee to prevent buckling of the prosthesis throughout single support (Figure 3). Because the negative moment did not allow prosthetic knee motion in stance, there was no energy storage (K1) or energy return (K2) in the knee power curves of the amputee subjects during this period of the gait cycle (Figure 4). Thus, the knee joint did not contribute to shock absorption, rate of energy storage, or rate of energy return during the majority of the gait cycle. The amputee subjects instead appeared to use the hip joint as an alternative means for shock absorption, power absorption and generation.
The sagittal plane hip motion in the amputee group was similar to that of the control group, and was unaffected by the different prosthetic ankle configurations. The hip joint moments and powers of the amputee and control groups, however, differed during early and terminal stance. The amputee subjects exhibited a positive peak moment at the hip joint following initial contact that was generally twice the magnitude of that in the able-bodied subjects. As a result, the magnitude of the H1 power burst was approximately four times that of the control subjects. Thus, it appeared that the hip joint in the amputee group was critical in generating power during early stance. Since the amputee group did not have active control of the ankle and knee joints, the power generated at the hip probably helped the study participants progress forward and make up for lost anatomical function.
The amputee group exhibited another large source of power generation (the H3 power peak), relative to the control subjects, at the hip joint prior to toe-off (Figure 4). The H3 power burst represents the action of the hip flexors pulling the lower limb upwards and forward (Winter and Sienko 1988). As shown in able-bodied individuals, the A2 and H3 power bursts occurred simultaneously during the gait cycle as the leading limb prepared for swing phase (Figure 4). Thus, the amputee subjects apparently compensated for the lack of energy produced at the prosthetic ankle (A2) by increasing power generation at the hip (H3) immediately prior to toe-off.
Although no appreciable differences in the data were found between the Baseline and Multiflex Ankle configurations, the amputee group perceived disparities between the two prosthetic ankle conditions. The amputee subjects indicated in the questionnaire that the Multiflex Ankles increased their comfort during walking (Table IV). The anatomical ankle/foot complex in able-bodied persons is believed to provide shock absorption during loading response (Perry 1992). The compliance provided by the prosthetic ankle units could have reduced the shock forces felt by the study participants at initial contact, thereby increasing comfort. Alternatively, the amputee subjects may have perceived increased comfort as a direct result of the additional motion provided by the prosthetic ankle during stance phase.
Following the Baseline gait analysis, three of the amputee subjects indicated that the prosthetic feet did not provide enough motion. While walking with the prosthetic ankle units, however, none of the study participants indicated that the components provided too much motion or increased the perceived effort to walk. The range of rotation of the Multiflex Ankle is dependent on elastic bumpers inside the device, which enabled the amputee subjects to passively plantarflex and dorsiflex their prosthetic ankle during the stance phase of the gait cycle, exhibit sagittal plane ankle motion similar to the control group, and increase their ankle ROM with speed. Additionally, the gait analyses revealed that the prosthetic ankles allowed the amputee group to increase their ankle ROM compared to the Baseline gait analysis (Figure 2), which likely eased their walking on uneven terrain as they reported in the questionnaire results (Table IV). Three of the four study participants perceived that they were able to walk faster with the prosthetic ankle units compared to the Baseline configuration. Although there were no overall group differences in walking speed between the two configurations during the experimental gait analyses, the amputee subjects may have used faster walking speeds outside of the laboratory.
It should be recognized that persons with amputation may develop unique gait characteristics apart from others with similar pathological conditions. Therefore, consideration should be given for these individuals to be evaluated in a motion analysis laboratory. These data would serve to quantify their gait mechanics in order to better understand their abilities and to identify particular prosthetic deficiencies. Quantification of gait parameters for persons with bilateral trans-femoral amputations can help improve the functionality of prosthetic devices available to this population. This study has shown that prosthetic ankle units are beneficial to amputees, primarily to increase the user's comfort during walking while providing them with a more functional prosthesis. The authors feel that prosthetic ankles should be considered by prosthetists when fitting prostheses on clients with trans-femoral amputations.
Limitations
There are several noteworthy limitations of this investigation. This sample size was small, primarily because individuals with bilateral trans-femoral amputation who walk with prostheses were difficult to locate. Small sample sizes do not produce a high statistical confidence level, which indicates how results may represent the larger study population. Moreover, since the study sample size was so small, no statistical analyses were performed on the data. Rather, characteristics and trends were highlighted to supplement the sparse information concerning the gait of persons with bilateral trans-femoral amputations that is available in current literature. Additionally, the protocol for this research study did not require the amputee subjects to wear similar prosthetic knee units. As a result, two different types of knees, hydraulic SNS and polycentric, were used which may have increased variability in the data between subjects. Shoes are also an important consideration when aligning prosthetic components. Providing the amputee subjects with similar shoes might have further reduced or eliminated differences in the data. Finally, the two-week accommodation period prior to each gait analysis may not have provided sufficient time for the study participants to fully accommodate to the prosthetic ankle configuration since some prosthesis users may require many weeks of training to take full advantage of the capabilities afforded by their prosthetic components. Further investigation into issues concerning accommodation by prosthesis users is recommended.
Conclusion
The addition of the Multiflex Ankles to the prostheses of persons with bilateral trans-femoral amputations measurably increased the range of motion at the ankle joint during gait, but did not alter the temporal-spatial parameters. Further, negligible differences were observed between the joint moments and powers when subjects walked with and without the Multiflex Ankle units. Nonetheless, the amputee group's gait data showed discernible differences from those of an able-bodied control group, even while walking with the prosthetic ankle units. The results from the subject questionnaires revealed that the Multiflex Ankles increased the amputee group's comfort during walking without increasing the perceived effort, and made it easier for them to walk on uneven terrain. Moreover, the amputee subjects clearly preferred having the prosthetic ankle units in their prostheses than not. Therefore, even though gait may not significantly improve, the results from this study indicate that increased sagittal plane ankle motion provides considerable benefit to persons with bilateral trans-femoral amputations.
Footnotes
Acknowledgements
The authors acknowledge Rebecca Stine, MS and Robert D. Lipschutz, CP for their assistance in the data acquisition and prosthetic fitting of the study participants, respectively. This project was supported by Grant Number 1R01HD42592 from the National Institute of Child Health and Human Development (NICHD), the National Institutes of Health (NIH), and the National Science Foundation Graduate Research Fellowship Program. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NICHD. Data for this project were acquired in the VA Chicago Motion Analysis Research Laboratory of the Jesse Brown VA Medical Center, Chicago, IL.