
Abstract
Introduction:
Partial knee replacement (PKR) is one of the treatment options in middle-aged patients with less extensive knee osteoarthritis, with unicompartmental knee replacement (UKR) most commonly done for medial osteoarthritis. There are numerous advantages like bone/ligament preserving and faster recovery. However, the indications of UKR remain controversial, as most patients have some patellofemoral joint (PFJ) osteoarthritis. We performed modular bicruciate-retaining bicompartmental knee replacement (BKR) in this group of patients and compared the outcome with total knee replacement (TKR).
Materials and Methods:
From 2016 to 2017, 14 BKR were performed in patients with medial and PFJ osteoarthritis. They were retrospectively compared with 14 TKR performed in patients with similar age and severity. The incision length, operative time, blood loss (in terms of hemoglobin drop), and length of stay were recorded. Pre- and postoperative range of motion and Knee Society knee score at 1-year follow-up were compared.
Results:
The mean incision length for BKR was shorter than TKR (130.1 vs. 185.1 mm), but the mean operative time was also longer (152.6 vs. 88.1 min). There was also less mean hemoglobin drop (1.8 vs. 2.6 g/dL) and shorter length of stay (7.4 vs. 9.2 days). The mean postoperative function score is better in BKR group (90.4 vs. 77.5), and the mean postoperative knee score (87.2 vs 88.9) and flexion (115.7° vs. 111.4°) were similar for both groups.
Discussion:
In selected patients, BKR is a good alternative to TKR. It preserves advantages of UKR while also tackle the PFJ which is the most controversial aspect of UKR. The early clinical outcome in our study is promising. However, there is a learning curve. Longer follow-up is necessary to study on the performance and survivorship as compared with UKR and TKR.
Keywords
Introduction
Primary osteoarthritis of the knee is a common problem in the aging population, and total knee replacement (TKR) is an effective surgical option with excellent clinical outcome. Middle-aged patients may also suffer from knee pain due to degeneration, with the medial compartment most commonly affected, followed by the patellofemoral joint (PFJ). Many surgeons do not prefer TKR in these relatively young active patients as the involvement usually still not tricompartmental, and there is possibility of future revision to another TKR. Unicompartmental knee replacement (UKR) is one of the treatment options in this group of patients, with numerous advantages like bone/ligament preserving and faster recovery. However, its indications remain controversial. The major debate is whether the PFJ, which is usually diseased in various degrees, could be ignored in UKR. Therefore, we performed bicruciate-retaining modular bicompartmental knee replacement (BKR) in this group of patients and compared the outcome with total knee replacement (TKR).
Materials and methods
From 2016 to 2017, BKR was performed in selected middle-aged patients who suffered from primary osteoarthritis of the knee with involvement of the medial compartment and PFJ, as indicated by their symptoms and preoperative X-rays. All of them had no more than 10° of varus and 15° of fixed flexion contracture, and with at least 90° of flexion. They were retrospectively compared with TKR performed in patients of the same age-group and similar severity of knee osteoarthritis. The incision length, operative time, blood loss (in terms of hemoglobin drop after operation), and length of stay were recorded. Pre- and postoperative knee range and Knee Society score at 1-year follow-up were compared.
All the operations were performed by the same group of surgeons in a joint replacement center of a regional hospital in Hong Kong. The medial parapatellar approach was used for all cases. After arthrotomy, the condition of both cruciate ligaments and lateral compartment was confirmed to be good before proceeded to BKR. Prostheses used for the BKR group were Zimmer (Zimmer Inc., Warsaw, IN, USA) Gender Solutions Patello-Femoral Joint System, and Zimmer Unicompartmental High Flex Knee (Figures 1 and 2). For the medial compartment, some of the cases were performed with patient-specific instruments (PSI), in which patient specific cutting jigs were created from preoperative magnetic resonance imaging (MRI) of the lower limb. Conventional instruments were used in the rest of the cases and all the PFJ replacement. For the TKR group, all the surgeries were performed with conventional instruments and the same prosthesis, Zimmer Nexgen LPS-flex PS knee, was implanted.
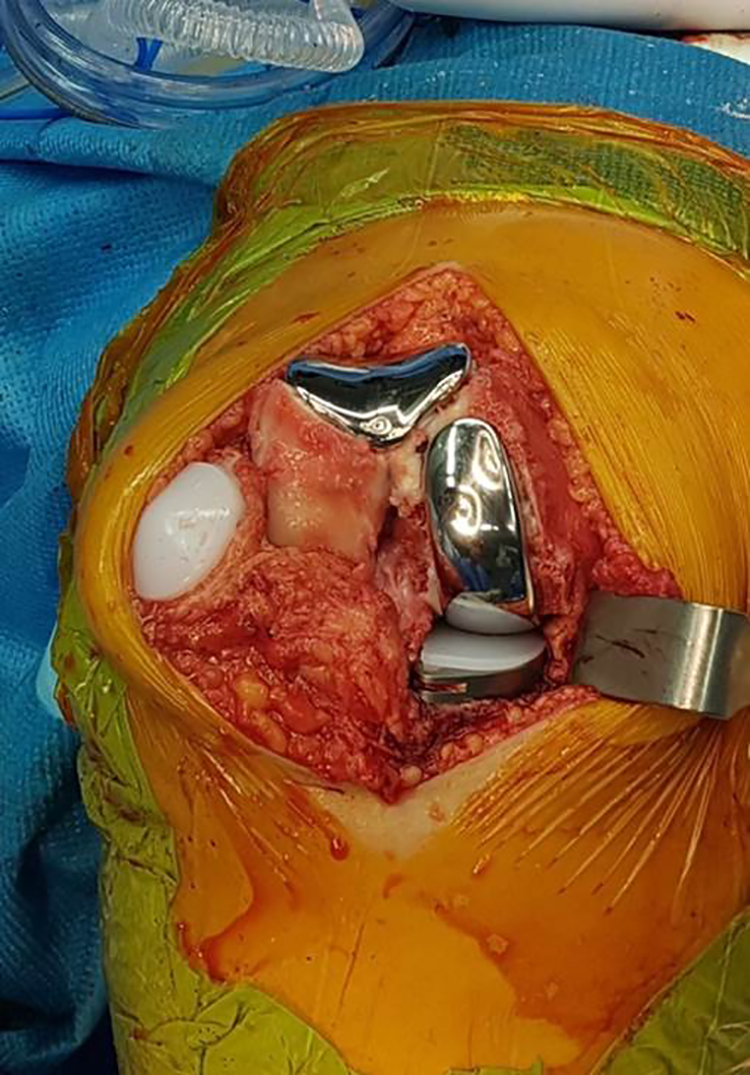
Intraoperative photo of modular BKR. BKR: bicompartmental knee replacement.
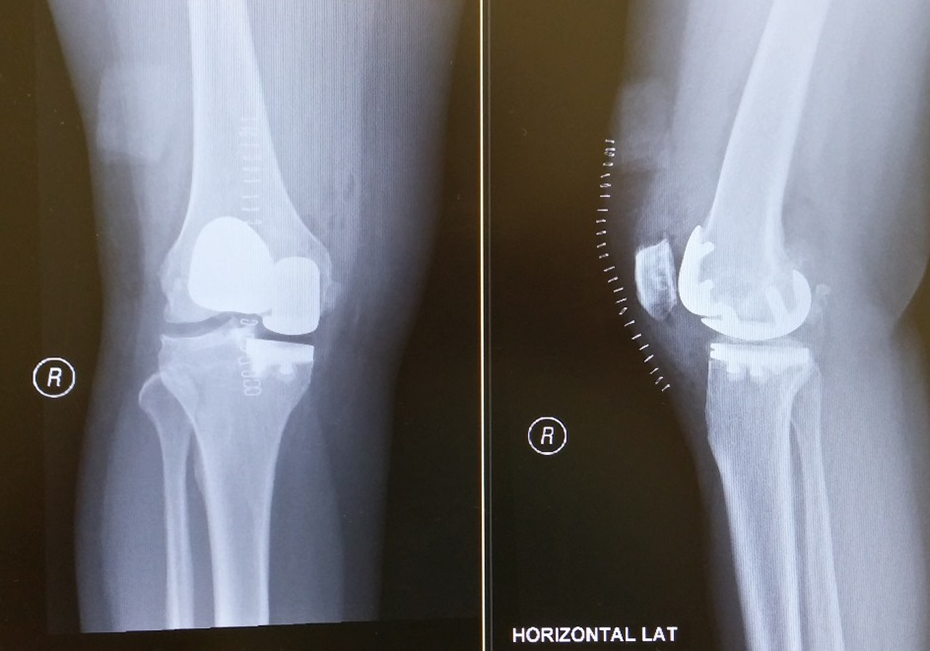
Postoperative X-ray of modular BKR. BKR: bicompartmental knee replacement.
Data analysis was performed in Microsoft Excel with Student T test and p value less than 0.05 is considered statistically significant.
Results
There were 14 knees in each group. The mean incision length for BKR was significantly shorter than TKR (130.1 vs. 185.1 mm), but the mean operation time was also longer (152.6 vs. 88.1 min) as we need more time for the first several cases. In the BKR group, there was less mean hemoglobin drop (1.8 vs. 2.6 g/dL) and shorter length of stay (7.4 vs. 9.2 days) (Table 1). No complication was noted in the study period for both groups.
Demographics and operative parameters of BKR and TKR group.
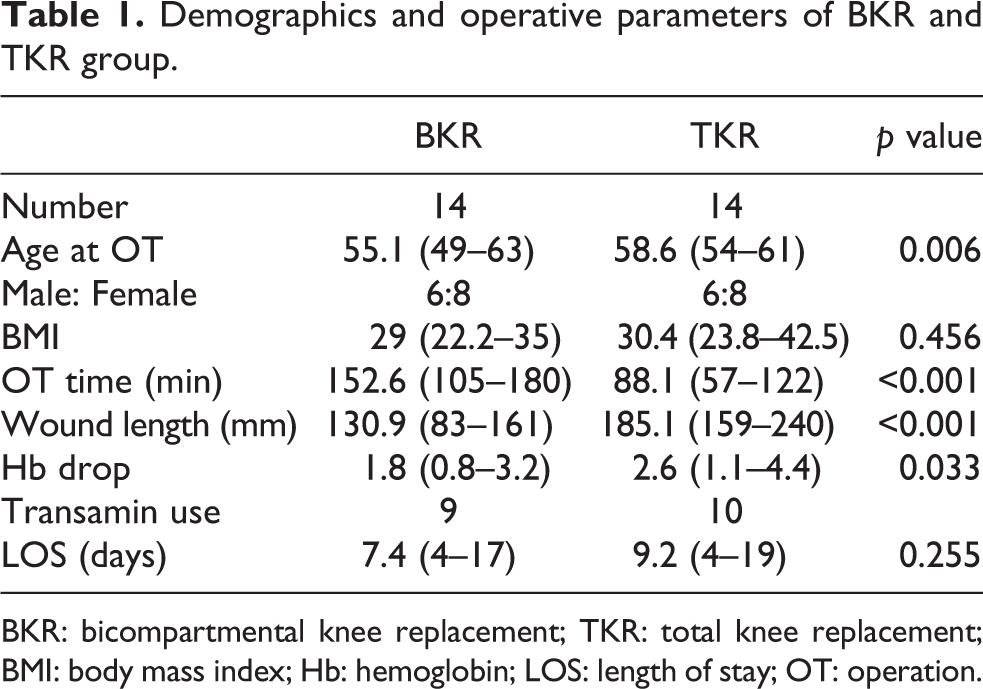
BKR: bicompartmental knee replacement; TKR: total knee replacement; BMI: body mass index; Hb: hemoglobin; LOS: length of stay; OT: operation.
Both groups had similar preoperative Knee Society knee score and function score. The mean postoperative function score was significantly better in BKR group (90.4 vs. 77.5). The BKR group had better preoperative flexion range than TKR group (111.8° vs. 96.8°), but the mean postoperative flexion range was similar for both groups (115.7° vs 111.4°) (Table 2).
Clinical parameters of BKR and TKR group.
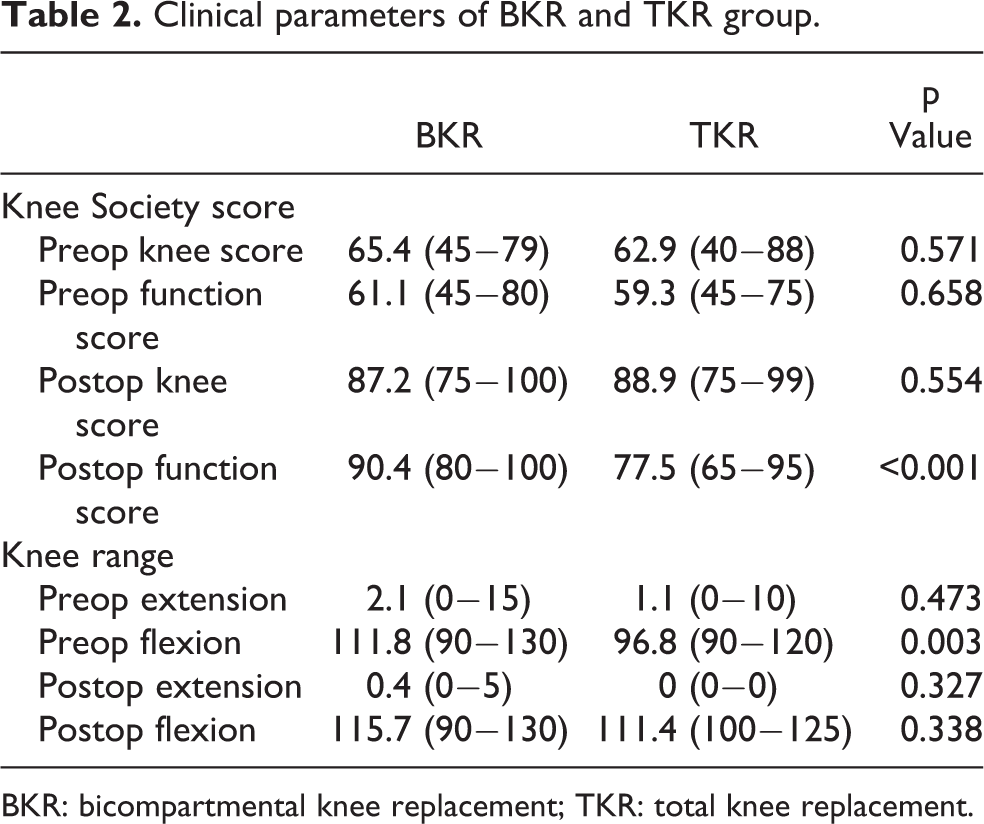
BKR: bicompartmental knee replacement; TKR: total knee replacement.
We also performed a subgroup analysis for the BKR group. There were eight cases of PSI and six cases of conventional instruments. All the parameters did not have significant difference statistically. However, it is worthwhile to note that the mean incision length is longer in PSI group (122.5 vs. 137.1 mm) due to bigger size of the PSI cutting jigs compared to conventional instruments.
Discussion and conclusion
In the literature, BKR is not a common procedure when compared to UKR and TKR. Previous studies showed that the monolithic BKR had poor result, 1 –3 as the medial and PFJ component position could not be adjusted individually. Short-term result of modular BKR is good, 4 –8 with most studies showing similar or better function than TKR. 9,10 Other advantages include less blood loss, 11,12 better gait pattern, and knee kinematics 13 –16 as BKR is more bone/ligament preserving than TKR. However, there is still no conclusion whether it is a worthwhile procedure when compared to UKR and TKR in the long run, in terms of clinical outcome, survivorship, and late complications.
Our study showed BKR is a good alternative to TKR in selected patients. BKR can be performed with a shorter incision, with less soft tissue trauma as we do not need to expose the lateral compartment and anteriorly sublux the tibia. The lateral compartment and both cruciate ligaments, which are usually still in a good condition in this group of patients, can be preserved. The PFJ, which usually has variable degree of degeneration which may progress after UKR, 17 can also be tackled and hopefully prolong the survivorship of partial knee replacement. The early clinical outcome is also good in our series, with better knee and function score. However, there is a learning curve, as reflected by the increase operative time.
Our study had several limitations. It was retrospective and the sample size was small due to strict patient selection criteria. The postoperative radiological alignment was also not reviewed in this study.
To conclude, the early clinical outcome of modular BKR is promising, with less surgical trauma as reflected by the shorter incision and less blood loss, and better knee function score when compared with TKR. It preserves the advantages of UKR but also resurface the PFJ which is the most controversial aspect of UKR. However, there is an increase in operative time in the initial cases due to learning curve. Long-term follow-up is necessary to study on its clinical performance, any late complications, and survivorship.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.