
Abstract
Introduction
Total knee replacement (TKR) is performed to treat different knee joint diseases, most commonly osteoarthritis. 1 Good postoperative rehabilitation is essential for a successful surgery. However, rehabilitation protocol varies among different centers. The use of continuous passive motion (CPM) is a common, yet controversial component. 2 In the 1970s, Salter et al. developed the concept of CPM, which intended to prevent joint immobilization due to postoperative pain and muscle weakness to reduce stiffness based on laboratory study. 3 Controversies existed since its introduction. Some studies believed postoperative use of CPM reduced the length of hospital stay,4,5 swelling, 6 improved range of movement (ROM),4,6 and reduced deep vein thrombosis (DVT). 7 However, some other studies showed that CPM is not useful to improve the final ROM, prevention of DVT, or patient-reported outcomes.8,12 Although CPM is still frequently used after manipulation under anesthesia for postoperative stiffness after TKR, 13 the routine use of CPM is not recommended. Although the cost of CPM is relatively low, 14 it is not free of complications. Wound care problems may occur if CPM is used immediately after operation, 15 including wound staining 16 or persistent swelling. 12 The recent introduction of ERAS (Enhanced Recovery after Surgery) pathway, which aimed to reduce the morbidity and length of hospitalization, was beneficial to TKR. 17 Most previous studies on CPM were based on results before the era of ERAS. For TKR patients under ERAS with slow progress to obtain a satisfactory postoperative ROM during the in-hospital period, whether CPM is useful to help them achieve a better ROM earlier and thus facilitate discharge is still unclear. In this study, we aim to study whether CPM is beneficial to patients who were slow to achieve adequate in-hospital ROM for rehabilitation under ERAS pathway and therefore help facilitate discharge.
Clinical implication
This retrospective study aims to evaluate the short-term clinical outcomes and determines whether CPM could be used in selected cases under ERAS pathway.
Methodology
Study design
A retrospective study was performed. Clinical records of patients who had TKR done between January 2017 and September 2019 with ERAS pathway were reviewed. Patients with slow progress in attaining an adequate postoperative range of motion during hospitalization were identified. They were defined as patients not able to reach 45 degrees of active flexion range on postoperative day (POD) 3. Total of 1089 TKR were performed during the study period and we identified 73 patients (6.7% of the total number) who met our inclusion criteria. Patients were excluded if they had any major complications including postoperative fracture (n=4) or DVT (n=1). Total of 68 patients (14 males and 54 females) were included in the study. Patients were checked if they were given CPM according to available records. Relevant outcomes would be compared between patients who were given CPM (study group, n=30) and patients who were not given CPM (control group, n=38) (Figure 1). The data was retrieved from available medical records created by the case doctors in daily ward round. All ranges of movement were measured by a goniometer. The ROM would be counted in a 5-degree interval of difference by convention. All patients received standard daily one-on-one rehabilitation. Patients were discharged if they achieved satisfactory stability in independent walking (Modified Functional Ambulatory Score 5 or above) with quadriceps power in Medical Research Council (MRC) muscle power grading 3 or above according to protocol.
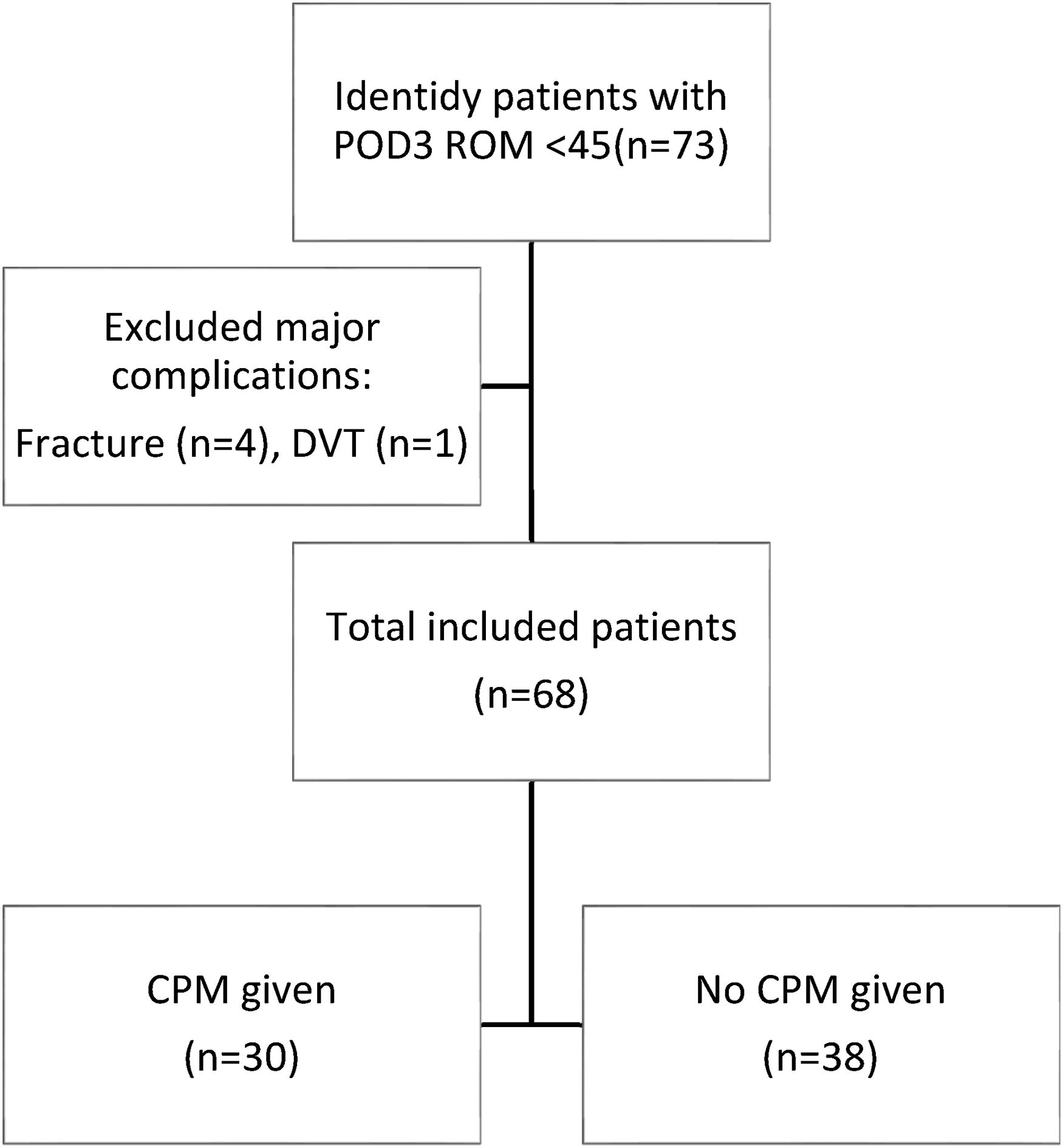
Selection flowchart of patients.
Surgical approach and ERAS protocol
All operations were done through a midline incision with tourniquet. Medial parapatellar capsulotomy approach was used with a cemented posterior stabilizing implant applied. All patients were enrolled in ERAS program with standard multi-disciplinary pre-operative, intra-operative, and post-operative care.
During pre-operative period, patients would be assessed by the Pre-Admission Services (PAS) team in a multidisciplinary approach for pre-operative investigations and assessments. The PAS team consisted of surgeons, anesthetists, nurses, physiotherapists, occupational therapists, and medical social workers. Patients would attend Pre-Admission Clinic and were assessed for fitness by anesthetists, surgeons, and nurses about 3 weeks before the operation. Physiotherapists, occupational therapists, and medical social workers would also assess the patients before the operation to minimize the potential physical and social difficulties related to the operation. Medical team would also be consulted if there was significant patient co-morbidity including poorly controlled diabetes, hypertension, heart failure, and so on, with appropriate pre-operative investigations and optimization performed before surgery. The aim of PAS was to prepare patients both physically and psychologically for the whole procedure and helped to minimize the length of hospital stay.
During operation, a 1 gm Tranexamic acid (TXA) capsule was given 2 hours before induction of anesthesia unless contraindicated. 1 gm Cephazolin (2 gm if bodyweight > 80 kg) was given intravenously for antibiotic prophylaxis (Vancomycin would be the alternative if drug allergy existed). Local intra-articular injection of analgesics, which was a mixture of 30 mg Ketorolac, 100 mg levobupivacaine, and 0.5 mg adrenaline diluted in 100 ml normal saline, would be given intra-operatively for pain control. Patients with renal impairment or drug allergy would receive a modified dosage or regimen of drugs according to protocol. No drain was used.
During the postoperative period, medical DVT prophylaxis would be given as low molecular weight heparin or oral direct thrombin inhibitor for the high-risk group (i.e. previous DVT/pulmonary embolism, on oral contraceptive pills, malignancy), started on POD1 until fully ambulatory. Patients would have Doppler Ultrasound to look for DVT before discharge. 1 gm TXA capsule would be given for two doses (6 hours and 12 hours postoperatively) after operation unless contraindicated. Multi-modal analgesics were used for postoperative pain control and patients would be reviewed by anesthetists daily. We aimed avoidance of transfusion if the hemoglobin level of patient is >8 mg/dL. There would be immediate postoperative rehabilitation conducted by physiotherapists and occupational therapists, including knee mobilization exercise, quadriceps exercise, bed mobility training, activity-of-daily-living training and full weight-bearing walking exercise. Patients would be discharged once they met the discharge criteria.
CPM protocol
CPM would only be started on POD3 during hospital stay if patients were found to have limited active ROM over the operated knees. Once CPM was prescribed, it was set to begin at 0–90 degrees and feasible to adjust according to patient's need and tolerance. Optiflex® knee CPM was used, with a minimum of 4 hours as 1 session per day. It could be removed at night for patients’ comfort. The use of CPM would be assessed by case doctors daily and adjusted the regimen accordingly. Other rehabilitations including physiotherapy and occupational therapy would be given in addition to CPM under ERAS program. During the use of CPM, patients were assessed for any wound complications or pain. The compliance would be monitored as well by nursing colleagues. Patients would be reminded of relevant CPM techniques, including not turning the leg sideways to prevent peroneal nerve palsy and changing the leg position to avoid local pressure against the device.
Outcomes
1. Length of hospital stay
The length of stay would be counted from the day of operation to the day of discharge. The number of days in the intensive care unit, if any, for postoperative monitoring would be included as well.
2. The active ROM at POD 4, upon discharge and during the latest follow-up 3. Pain on POD 4 4. Quadriceps power at POD 4
The active ROM was measured by goniometer on daily basis during morning ward round by case doctors before physiotherapy. They will be recorded in a 5-degree interval of difference by convention. As the CPM were started on POD 3 if needed, the knee active ROM would be compared on POD 4 between the two groups to assess any immediate improvement, which may facilitate discharge under ERAS setting. Our mean follow-up time is 30 months. The ROM would be measured by attending doctors during the outpatient joint clinic. All the records were documented in the clinical notes.
The pain was assessed by a numeric rating score from 1 to 10 according to patient's subjective feeling. There was a standard multi-modal analgesic regimen protocol.
The quadriceps power was assessed according to the MRC muscle power grading on daily basis. The results would be compared on POD 4 between the two groups to see any immediate improvement after starting CPM.
Statistical analysis
We used Statistical Package for the Social Sciences (SPSS) software to perform statistical analysis. The distribution of data was determined by the Kolmogorov–Smirnov (K–S) test for normality. Data will be assessed by T-test for independent means or Mann–Whitney U-test for numeric variables according to their normality. The Chi-square test was used for the nominal variables. The effect size of a statistically significant result was calculated by Hedges’ g-method, with effect size categorized as small (0.2), medium (0.5), and large (0.8). A statistically significant result is considered as p ≤ 0.05. The 95% confidence interval (CI) was also shown. A Multiple linear regression model was used to evaluate the relative effect of variables.
Results
Both groups had matched demographics. The age, body mass index (BMI), ROM just before using CPM, and mean follow-up time in terms of months were tested in normal distribution by using K–S test with value having p >0.05 considered as normally distributed (Table 1). American Society of Anesthesiologists (ASA) grading was not in a normal distribution, thus Mann–Whitney U-test was used. The mean follow-up time for the CPM group is 31 months and 29.2 months for the control group. All the difference is statistically insignificant with p > 0.05. The chi-square statistic value for gender with p > 0.05 showed both groups were matched in gender as well. The pre-operative ROM is 97.67 degrees (95% CI: 88.73–106.59) and 103.15 degrees (95% CI: 97.55–108.76) for study group and control group respectively (p = 0.14).
Demographics and the respective p-values.
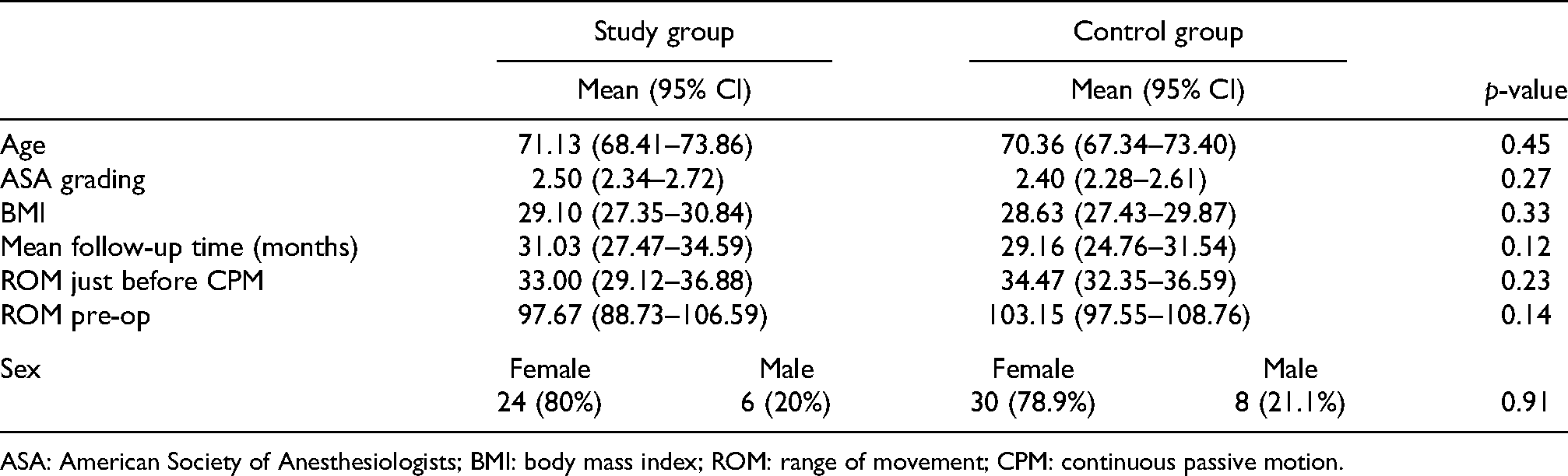
ASA: American Society of Anesthesiologists; BMI: body mass index; ROM: range of movement; CPM: continuous passive motion.
The outcomes were analyzed as shown in Table 2. Only the difference in length of stay and active ROM upon discharge were statistically significant. The mean length of stay is 7.3 (95% CI: 6.15–8.44) for the study group and 5.9 (95% CI: 5.14–6.71) for the control group with p < 0.05. The difference is 1.4 days. The Hedge's g is 0.52, which showed a moderate effect size. The mean active ROM upon discharge is 76.00 degrees (95% CI: 71.34–80.66) for the study group and 68.42 degrees (95% CI: 63.45–73.39) for the control group with p <0.05. The Hedge's g is 0.54, which showed a moderate effect size. The difference was 7.58 degrees (Figure 2).
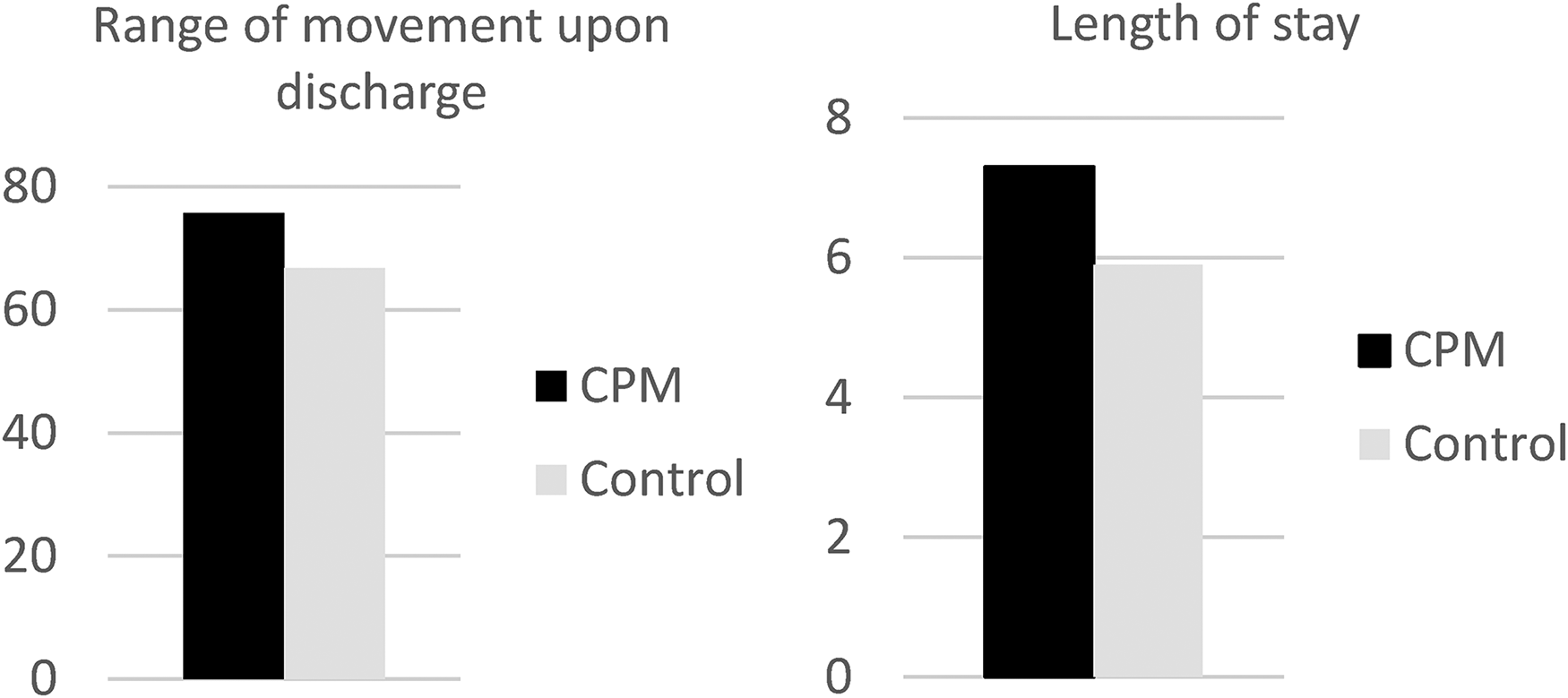
Charts showing range of movement and length of stay of both groups.
Outcomes of both groups.
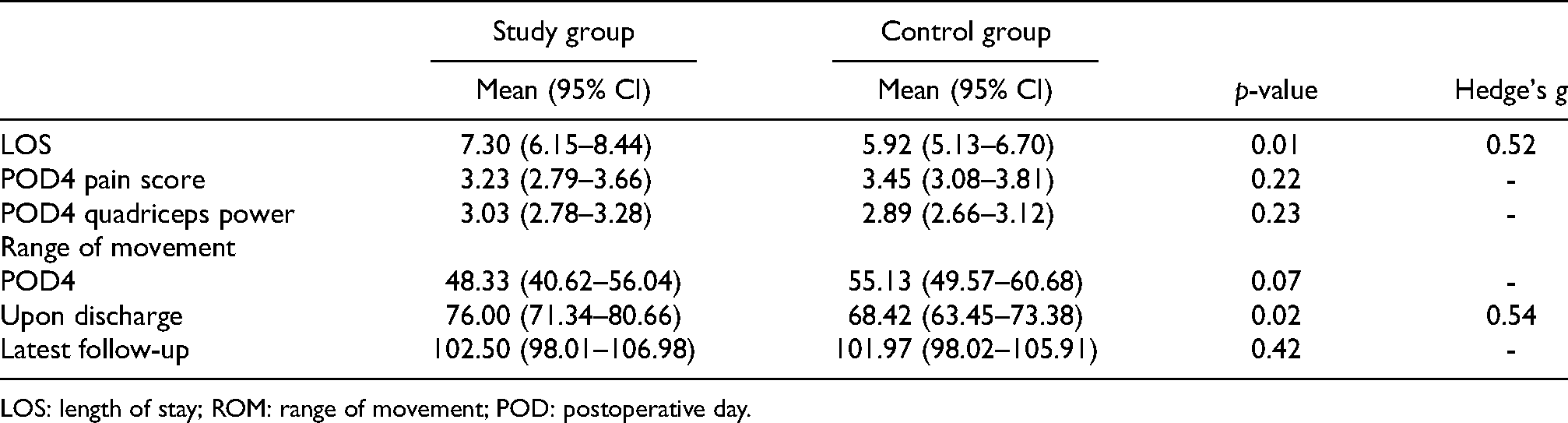
LOS: length of stay; ROM: range of movement; POD: postoperative day.
The shortest LOS for these patients was 4 days. There was no statistically significant difference between the two groups on POD 4 quadriceps power, pain score, and ROM. The mean score of pain on POD 4 is 3.23 (95% CI: 2.79–3.66) for the study group and 3.45 (95% CI: 3.08–3.81) for the control group with p > 0.05. The mean active flexion range on POD 4 is 48.33 (95% CI: 40.62–56.04) for the study group and 55.13 (95% CI: 49.57–60.69) for the control group with p > 0.05. The active ROM in the latest follow-up in study group is 102.5 (95% CI: 98.01–106.99) and that of control group is 101.9 (95% CI: 98.03–105.92) with p >0.05.
We observed that although there was no difference in the baseline active ROM on POD4 between the two groups, the active ROM for the study group was higher upon discharge, despite no significant difference during the latest follow-up. However, the LOS for the study group is longer than the control group by 1.4 days. The multiple linear regression model was used to evaluate the effect of confounding on the active ROM upon discharge by pre-operative active ROM, the use of CPM, LOS, BMI, and age (Table 3). It showed that both the effect of the use of CPM (p = 0.04) and pre-operative active ROM (p = 0.05) were statistically significant factors, but not the LOS (p = 0.25). The T-statistic of the use of CPM (t=2.08) is also larger compare to that of the LOS (t=1.15). It showed that the effect from the use of CPM is more significant than the longer LOS.
Multiple linear regression model component.
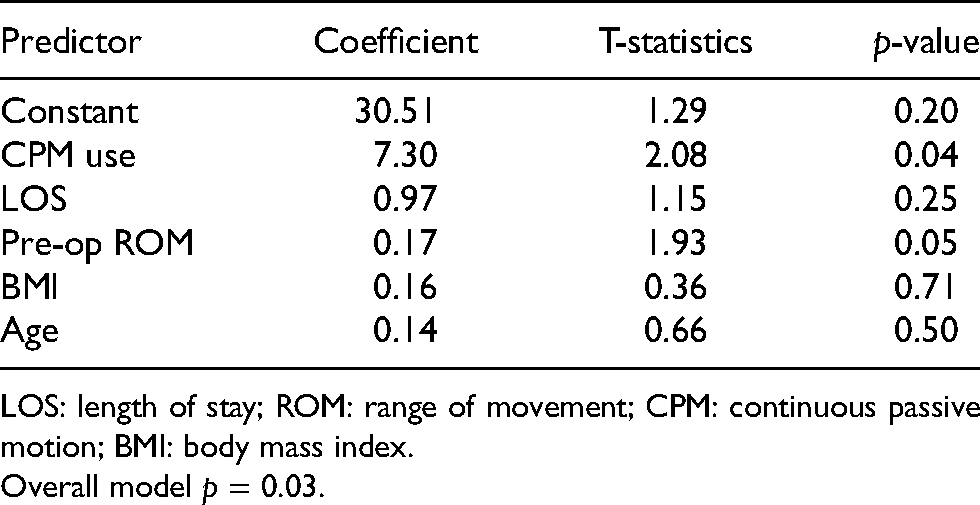
LOS: length of stay; ROM: range of movement; CPM: continuous passive motion; BMI: body mass index.
Overall model p = 0.03.
Discussion
Effects of CPM after TKR had been a controversy since its introduction. Some studies showed CPM could improve the flexion range,4,6 reduce the length of hospital stay,4,5 reduce the chance of future manipulation8,14 and the incidence of DVT, 7 while others showed CPM caused more swelling,12,16 higher demand on analgesics 16 and no improvement in ROM.7,18,19 2014 Cochrane Review with an analysis of 24 randomized clinical trials reported that routine use of CPM had no clinically significant effects on knee active flexion, pain, function, or quality of life. 8 This review provided good evidence to stop its routine use.
With the implementation of a “fast track” perioperative care protocol, shorter hospital stay after operation with an improvement of patient outcomes became a recent focus in perioperative care development. ERAS was introduced by a group of surgeons from Northern Europe who formed a research group intending to explore the ultimate care pathway for patients undergoing surgeries. 20 It has been shown to reduce the length of hospital stay and complications for different surgical specialties, including orthopedic surgeries like total joint replacement.21,22 It provided benefits to both patients and the healthcare system.21,24 Most studies about CPM were conducted without the implement of ERAS. Therefore, although we understood CPM could not provide clinical benefits on final patient outcomes, which was also seen in our study, it was still unclear whether CPM could be considered to improve in-hospital outcomes in selected patients with poor postoperative rehabilitation progress in ERAS pathway.
Our study again showed no effect on CPM upon final ROM. However, we showed that CPM could improve the active flexion range upon discharge, with a mean difference of 7.58 degrees. With CPM, the active ROM upon discharge achieved 76 degrees, in contrast to 68.4 degrees observed in the control group. We believed it was the short-term effect of CPM. A previous gait study suggested that in the sagittal plane, the average knee motion used for the swing phase of gait is 70 degrees, lifting an object without instructions is 71 degrees and the last step during going downstairs by the alternate method is 76 degrees. 25 The amount of range in CPM group (76 degrees) may provide a better gait performance and thus improve in-hospital rehabilitation progress in daily activities. It needs further study to evaluate this effect.
Some studies showed CPM might increase pain, 16 although a decrease in pain was also seen in others.12,26 2014 Cochrane review found no statistically significant effect on pain level or quadriceps power caused by CPM. 8 In this study, we observed CPM did not increase postoperative pain nor weaken the quadriceps power, which matched with the 2014 Cochrane review. This supported its use in ERAS pathway as any increase in pain might further increase the LOS by slowing down the rehabilitation.
We also observed that the CPM group had a longer hospital stay by an average of 1.4 days. The increase in hospital stay may explain the increase in ROM in the study group due to a natural clinical improvement with time. However, the use of CPM still showed statistically significant effect on active ROM upon discharge despite adding LOS as confounding factor using multiple linear regression model. This suggests the use of CPM is a significant factor to improve active ROM in patients with poor early in-hospital progress under ERAS protocol. One may argue that the increase in LOS is not worthwhile under ERAS setting. Although our study observed an increase in LOS, which was also seen in other previous studies,9,10,27 some other studies concluded no relationship between these two 6 or even found opposite result.4,5 2014 Cochrane review found no statistically significant association between LOS and CPM use. 8 In fact, the exact detail of the protocol of CPM might have affected the LOS.10,27 Whether another CPM protocol on these selected patients would change the result in LOS under ERAS pathway also needs further study.
Some believed that CPM could save cost per patient. 28 However, the increase in LOS would instead impose a higher cost, in addition to the extra cost due to the use of CPM. Despite this, we need further study to determine whether the improvement in ROM upon discharge was worthwhile to increase the expenditure caused by CPM under ERAS pathway. We also noticed that the technique and compliance of using CPM were difficult to monitor, especially for those older patients.
There are strengths and weaknesses of this study. This study benefited from a standard rehabilitation protocol and perioperative care plan for patients. It helped to minimize the confounding effect of rehabilitation. They also received the same postoperative multi-modal analgesic regime as standard protocol. However, potential bias might happen as patients could not be blinded due to the nature of CPM. The strength of this study is also limited by its relatively small sample size and retrospective nature. As the measurement was based on 5-degree interval of difference, any difference less than 5 degrees would be bounded to have measurement bias. Further studies were needed to identify the best CPM protocol under ERAS pathway which may affect the outcome. Therefore, we suggested a future larger-scale randomized control trial to study the effect of in-hospital CPM with different protocols on these selected patients.
Conclusion
For post TKR patients with limited rehabilitation progress under ERAS pathway, the use of CPM could attain better active ROM upon discharge with no adverse effect on pain control and quadriceps power, but at the expense of an increase in length of stay.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.