
Abstract
Purpose
In unicompartmental knee arthroplasty (UKA) procedures, maximizing the bone coverage of the tibial implant and eliminating the medial and posterior overhang would be optimal. We commonly used Physica ZUK® (ZUK), which is a symmetrical design. Alternatively, since Persona Partial Knee® (PPK) was developed in 2017 with an anatomical design to improve bone coverage, we started PPK. We hypothesized that the PPK facilitated better bone coverage than the ZUK without obvious overhangs. This study evaluated the bone coverage and the medial and posterior overhang of these differently designed tibial implants.
Methods
Seventy-nine knees from 68 patients who underwent UKA were evaluated. Cases were categorized into the ZUK (41 knees) and PPK (38 knees) groups. CT images were acquired before surgery and 1 week after surgery. We measured the tibial bone coverage, and the medial and posterior overhang by 3D software.
Results
The bone coverages were 103.8 ± 4.8% and 102.0 ± 3.0%, the medial overhangs were 2.2 ± 1.2 mm and 1.4 ± 1.1 mm, and the posterior overhangs were 0.6 ± 1.3 mm and 0.4 ± 1.2 mm for the ZUK and PPK groups, respectively. The bone coverage and medial overhang were significantly different between the groups, with ZUK being larger.
Conclusion
Patients who received PPK had significantly smaller medial overhangs and better bone coverage. PPK is more likely to give better results than ZUK.
Brief introduction
Unicompartmental knee arthroplasty (UKA) reportedly has faster postoperative recovery, resulting in better knee function and higher patient satisfaction, than total knee arthroplasty (TKA).1,2 Moreover, UKA has shown positive long-term results for more than 10 years and has become a widely used minimally invasive surgical procedure.3–5 Conversely, reports have also shown that the revision rate is significantly higher if the surgeon has little experience with the procedure.6,7 UKA procedures require more accurate osteotomy and implant placement than TKA. Undersized tibial implants increase stress at the osteotomy surface and the risk of tibial fracture underneath the implants. 8 Medial and posterior overhangs of ≥ 3 mm can also cause postoperative pain.9,10 Therefore, maximizing the implant–bone coverage without medial and posterior overhangs on the tibial osteotomy surface is optimal.
For fixed-bearing type UKA, our department commonly used Physica ZUK® (ZUK), which is designed without distinguishing between medial and lateral UKA. However, in an actual knee, the medial and lateral condyle of the tibia are not symmetrical, and the medial condyle is narrower than the lateral condyle. 11 Therefore, the risk of medial overhang may increase if we attempt to maximize the tibial bone coverage in the anteroposterior diameter with ZUK. In 2017, the Persona Partial Knee® (PPK) was designed especially for medial UKAs to improve bone coverage by reproducing the medial portion of the Persona® TKA implant. The asymmetrical design of the PPK can reproduce the anatomical knee shape, making the PPK width smaller than that of the ZUK if the anteroposterior diameter is the same. However, there are very few reports on the evaluation of bone coverage of new anatomical designed implants. To our knowledge, only the study by Escudier et al. 12 discussed the differences in positioning of the ZUK and PPK tibial implants. They reported less overhang and better clinical results with PPK for Caucasians. Although the tibial bone morphology is different between Caucasians and Japanese, we hypothesized that using PPK (anatomical design) in Japan would provide better bone coverage and clinical results than using ZUK (symmetrical design). Therefore, this study aimed to compare the surgical outcome by measuring the bone coverage and medial and posterior overhangs between ZUK and PPK for Japanese patients.
Materials and methods
Ethics and informed consent
This study was approved by the ethics committee of (approval no. [blinded for review]). The requirement for informed consent was waived by the ethics committee because of the retrospective nature of this study. The study was conducted in accordance with the Declaration of Helsinki.
Patient demographics
This study is the retrospective comparative study. The study included 68 Japanese patients (79 knees total; 14 men, 19 knees; 54 women, 60 knees; mean age at the time of surgery, 75.1 ± 7.2 years) who underwent medial UKA in our department between January 2017 and April 2018. All patients had experienced osteoarthritis of the knee. In our department, medial UKA is indicated for cases without obvious osteoarthritis of the lateral compartment or patellofemoral joint and without varus deformity, which was uncorrectable. Patients who underwent computed tomography (CT) from the hips to the ankles before and after the UKA procedure were included. Patients who underwent UKA for diseases other than osteoarthritis were excluded from this study. Additionally, cases in which CT was not taken before and after surgery were also excluded. ZUK was used for cases between January 2017 and August 2017, and PPK was used for cases between September 2017 and April 2018 (Figure 1). 41 knees underwent UKA using ZUK (ZUK group), and 38 knees underwent UKA using PPK (PPK group). Cases in whom CT images were not obtained before and after surgery were excluded from the study population. TKA, Total knee arthroplasty. UKA, Unicompartmental arthroplasty. OA, Osteoarthritis. CT, Computed tomography.
Surgical procedure
Although three surgeons performed the surgeries in this study, all surgeries were performed following the same protocol. The spacer block method surgical technique was used. The tibial osteotomy was targeted at a 7° posterior tilt angle and a 2°varus angle, avoiding valgus implantation as much as possible. The sagittal osteotomy was performed after the horizontal osteotomy. The sagittal osteotomy line was marked parallel to Akagi’s line 13 at the rising part of the medial tibial intercondylar ridge to avoid cutting to the ACL. The osteotomy was performed with an assistant holding the knee joint in a neutral position. The tibial implant size was determined according to the anteroposterior diameter. If a medial overhang was likely to occur, we prioritized the anteroposterior fit by additional osteotomy in the center.
Bone coverage and overhang Calculations
CT images were obtained before surgery and 1 week after surgery. All CT images were taken at a 2 mm slice thickness. We used the three-dimensional preoperative planning software ZedKnee (version 14.0). The line connecting the center of the proximal third and the distal third of the tibial shaft was defined as the z-axis. The line connecting the posterior cruciate ligament (PCL) attachment and the medial edge of the patella tendon in the plane perpendicular to the z-axis was defined as the y-axis, and the line perpendicular to both the y- and z-axes was defined as the x-axis (Figure 2). Using the ZedKnee ZedEdit Mode, we measured the tibial implant area (Figure 3(a)) and the area of the osteotomy surface immediately underneath the tibial implant (Figure 3(b)). We then divided the tibial implant area by the area of the osteotomy surface immediately underneath the tibial implant to calculate the tibial bone coverage. Coordinate axis setting by ZedKnee. The line connecting the center of the proximal third and the distal third of the tibial shaft was defined as the z-axis. The line connecting the PCL attachment and the medial edge of the patella tendon in the plane perpendicular to the z-axis was defined as the y-axis, and the line perpendicular to both the y- and z-axes was defined as the x-axis PCL, posterior cruciate ligament. Osteotomy surface coverage calculated using ZedKnee ZedEdit Mode with (a) the tibial implant area and (b) the area of the osteotomy surface immediately underneath the tibial implant.

Using the ZedKnee Postop Mode, we measured the external rotation angle of the tibial implant and the medial and posterior overhang. The rotational angle of the tibial implant was the angle between the y-axis and the outer edge of the tibial implant (Figure 4). The medial overhang was measured in the coronal section, where the medial edge of the implant overhung the osteotomy surface (negative sign = no overhang) (Figure 5(a)). Similarly, the posterior overhang was measured in the sagittal section (Figure 5(b)). All measurements were performed three times by three orthopedic surgeons and averaged. To analyze the interobserver and intraobserver reproducibility of the measurements, the intraclass and interclass correlation coefficients were calculated for each analysis. They were greater than 0.8 for each measure, demonstrating good intraobserver and interobserver reproducibility. Tibial rotation angle measured with ZedKnee Postop Mode using (a) the y-axis and (b) outer edge of the tibial implant. IR, Internal rotation; ER, External rotation. Medial and posterior overhangs measured using ZedKnee Postop Mode in (a) the coronal section for medial overhangs and (b) the sagittal section for posterior overhangs.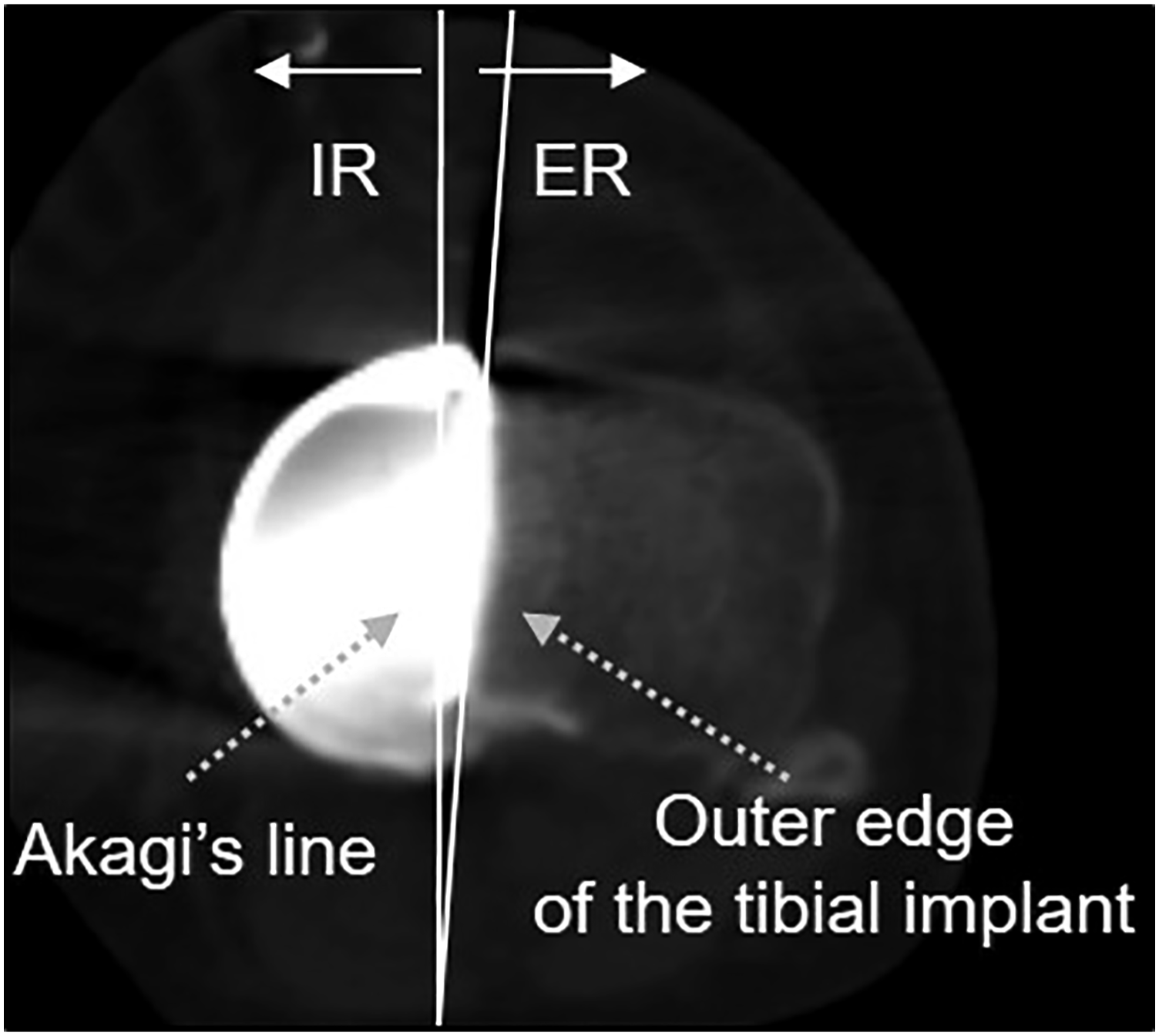

Differences between ZUK and PPK
Differences in all measurements between the ZUK and PPK groups were analyzed using the Mann–Whitney U test. Fisher’s exact tests were performed to determine the associations among medial and posterior overhang ratios. Pearson’s correlation coefficients were used to determine correlations between the tibial rotation angle and the bone coverage or the medial and posterior overhangs in the ZUK and PPK groups. All statistical analyses were performed using SPSS (version 23.0). Statistical significance was considered at p < 0.05.
Results
Patient demographics.

Tibial rotation angle, bone coverage, and medial and posterior coverage results.

The bone coverage and medial overhang were significantly different between the groups, with ZUK being larger than PPK.
Correlations between the tibial rotation angle and measured values.
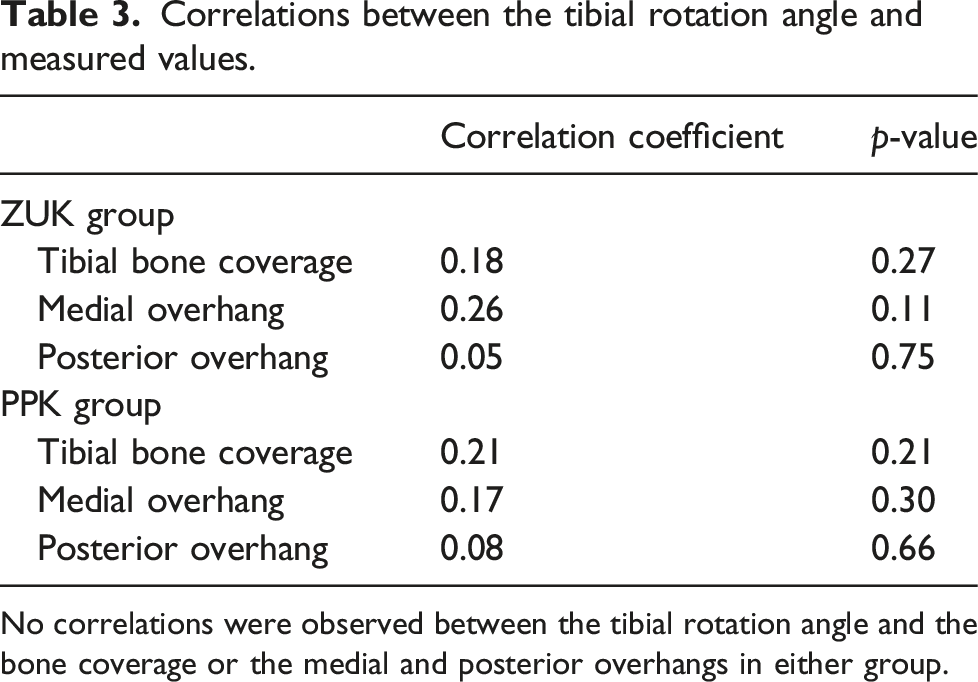
No correlations were observed between the tibial rotation angle and the bone coverage or the medial and posterior overhangs in either group.
Discussion
In this study, patients who received PPK had significantly smaller medial overhangs and better bone coverage than patients who received ZUK.
The ability to achieve good tibial implant coverage over the osteotomy surface may be affected by the implant design and rotation angle. Stulberg et al. 14 simulated symmetrically designed tibial implants and anatomically designed tibial implants using magnetic resonance images and reported that the symmetrical implants significantly increased the external rotation angle to obtain maximum bone coverage. In this study, the ZUK and PPK implants were placed using the same technique, and in both cases, the neutral position was aimed. Subsequently, no difference was noted in the external rotation angle. We also did not identify correlations between the rotation angle and tibial bone coverage or the implant’s medial and posterior overhang. Therefore, we propose that the PPK implant’s design improved bone coverage in the PPK group.
Until PPKs were released in Japan, our department used the same ZUK implants for right medial and left lateral UKAs and left medial and right lateral UKAs. However, since the medial and lateral condyles of the tibia differ in shape, achieving optimum bone coverage in both cases was difficult. In vitro studies have indicated that implants with an anatomical design specific to the medial side provide better coverage than those with a symmetrical design.15,16 Servien et al. 11 measured the anteroposterior (AP) diameter and the mediolateral (ML) diameter at the osteotomy surface immediately underneath the tibial implant in 19 medial and 18 lateral UKA knees. The mean ML/AP ratio was 0.56 and 0.63 in the medial and lateral UKA groups, respectively, indicating that the medial condyle width to the AP diameter was significantly smaller than the lateral condyle (p = .0005). Therefore, if medial UKA is performed using a symmetrically designed implant, the medial overhang becomes a concern. The newly developed PPK implant has an asymmetrical design, which aims for compatibility with the anatomical knee shape, and a smaller width than the ZUK implant, with the same AP diameter. Thus, the PPK implant should provide better bone coverage than the ZUK implant; however, only one report by Escudier et al. 12 has compared these differences.
Escudier et al. 12 reported that the bone coverage with ZUK and PPK was 97.3% and 94.7%, respectively, with no significant difference. However, the report also mentioned that the mean medial overhang for ZUK and PPK was 1.5 ± 2.0 mm and −0.3 ± 1.8 mm, respectively, showing that the mean PPK medial overhang was significantly smaller. The authors also reported that the rate of medial overhangs >3 mm was 35% for ZUK and significantly less for PPK at 0%. Additionally, they indicated that PPK produced better clinical scores, such as the Global Knee Society Score, Knee injury and Osteoarthritis Outcome Score SF, and EuroQol-5D-3 L score. However, it was a French report, and we could not find any reports from Asia. Miyasaka et al. 17 previously reported on the tibial morphology of Japanese and compared the results with those of Mensch and Amstutz, 18 who measured tibial morphology using a similar method in Caucasians. The ML diameter of the medial tibia condyle divided by the AP diameter of the medial tibia condyle was 1.64 mm in Japanese and 1.54 mm in Caucasians, and the Japanese had a larger ML diameter to AP diameter ratio. Assuming that the tibial AP diameter is 50 mm, the ML diameter of the medial tibia condyle is 2–3 mm larger in Japanese than in Caucasians. Therefore, Caucasians are more likely to have a medial overhang if the implants have the same AP diameter.
Our results are consistent with those of Escudier et al., 12 showing no medial overhang >3 mm in PPK. However, medial overhangs >3 mm occurred less frequently in the ZUK group in this study than in that of Escudier et al. 12 Both studies have shown that Japanese and Caucasians had better bone coverage with PPK. However, the incidence of medial overhangs may have been lower in this study (even with ZUK) because the medial condyle of the tibia in the Japanese had a larger ML diameter. The report of Escudier et al. showed < 100% bone coverage and a negative mean overhang, whereas this study showed >100% bone coverage and a positive mean overhang. We believe that this is because the surgical procedure in our department allows < 3 mm overhang and uses implants with as large anteroposterior diameter as possible.
This study had some limitations. First, this study was a retrospective design. However, the ages and sex ratios of the target patients were nearly the same, and all surgeries were performed using the same procedure. Second, the postoperative clinical results were not examined. However, since the PPK group had better bone coverage than the ZUK group without >3 mm overhangs, good clinical results have likely been obtained. Therefore, future research is needed to investigate the relationship between bone coverage and clinical results. However, we consider that PPK is more likely to give better clinical results than ZUK in Japanese patients.
Conclusion
PPK (anatomical design) had better bone coverage than ZUK (symmetrical design) without obvious overhangs. We consider that PPK, which is anatomically designed, is more likely to give better results than ZUK.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.