
Abstract
Introduction:
There are a lot of debates on the advantages and safety profile of one stage bilateral knee arthroplasty. Most of the studies focus on total knee replacement, and it may not be applied directly to unicompartmental knee replacement (UKR). We would like to compare the early results of one and two stage bilateral UKR in our center.
Methods:
This is a retrospective review of all the bilateral medial UKR done in our center in 2018–2019. Patients’ demographic data, operative time, postoperative blood, length of stay (LOS) and complications were recorded. The number of admissions, pre-operative assessment sessions (PAS), and weeks of post-operative physiotherapy were analyzed. Clinical outcome was measured by Knee society knee score and range of motion (ROM).
Results:
Our center performed 97 UKR in 2018–2019, with 50 UKR performed in 25 patients, among which 16 received one stage while 9 received two stage bilateral UKR. Both groups had similar mean age, BMI, sex ratio, ASA grading, pre-operative knee score and ROM. Patient in the one stage group required only 1 PAS/admission/operation to treat both knees with a mean LOS of 7.3 days and 7.8 weeks of physiotherapy, while those in the two stage group required 2 PAS/admissions/operations with a mean cumulative LOS of 9.8 days and 14.1 weeks of physiotherapy. The mean cumulative operative time was similar for both groups but the one stage group only required 1 operative session. There was no difference in blood loss and there was no transfusion or complication. The post-operative knee score and ROM at 3 and 6 months were similar for both groups.
Conclusion:
In suitable patients with bilateral medial OA knee, one stage bilateral UKR offers simliar early clinical outcome with shorter rehabilitation duration but without increasing complications compared with two stage. Resources can therefore be better utilized.
Keywords
Introduction
Prevalence of knee osteoarthritis (OA) is increasing worldwide, 1,2 and knee replacement is now the gold standard in the treatment of severe OA knee. Knee replacement can be classified into total (TKR) and partial (PKR). There are different types of PKR, 3 with the most common being unicompartmental knee replacement (UKR) for medial compartment OA, as this compartment is usually involved in primary OA knee. Comparing with TKR, advantages of UKR include tissue preserving, less blood loss, shorter length of stay (LOS), faster recovery, 4 –6 less complications 7 with better clinical outcome 8 in correctly selected patients. This is especially beneficial to middle-aged patients, 9 as UKR permit them to resume work and social activities earlier 5 while avoiding TKR in a relatively young age. Implants for medial UKR can be further classified into mobile bearing or fixed bearing, with both types showing comparable satisfactory outcome. 10 –12
Our center also offered one stage bilateral UKR for patients with bilateral medial OA knee (Figure 1), with the potential advantage of treating both knees with one operation and hence better resources utilization. However it may only be justified if there is no increased complication compared with one sided operation. The postoperative rehabilitation would also be a concern. We would therefore like to review the early result of this group of patients.
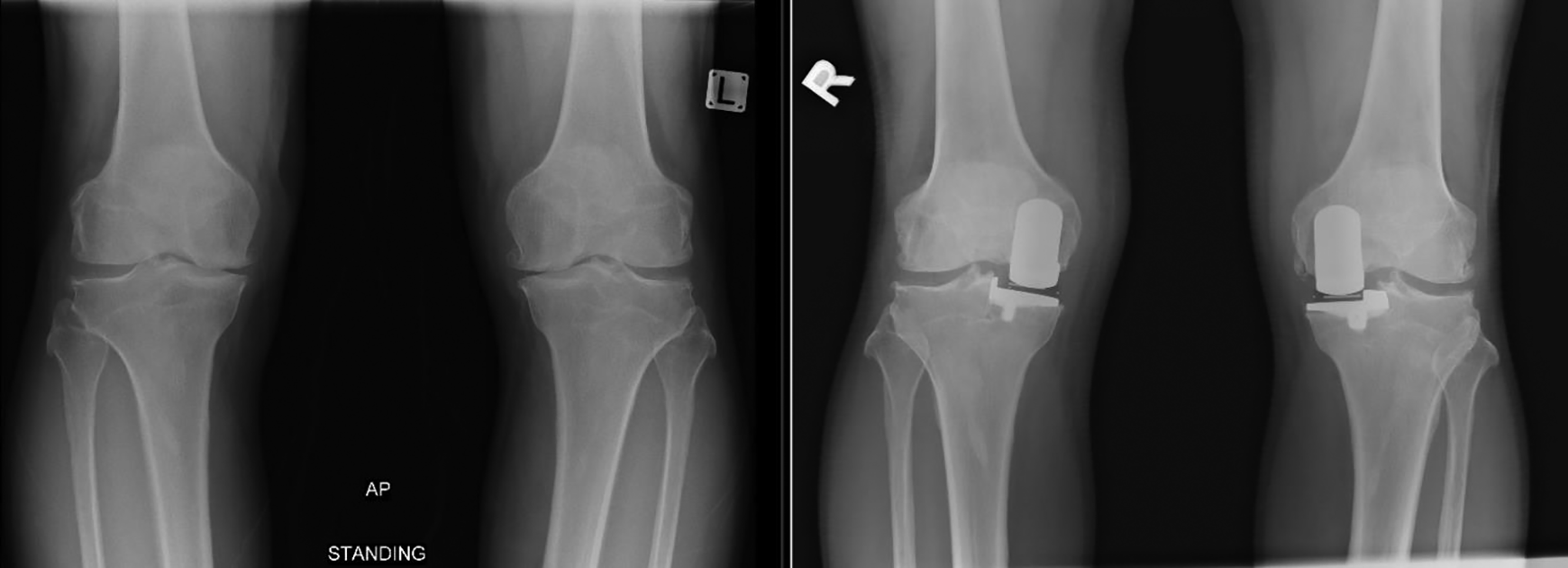
Bilateral medial unicompartmental knee replacement.
Method
This is a retrospective review of all UKR performed in our center in 2018–2019, with a focus on bilateral UKR (one and two stage). Patients were selected for UKR if they had medial joint line pain with compatible xray showing severe medial knee OA. Lateral compartment and patellofemoral joint should have no or minimal OA changes only. Varus deformity <= 15°, flexion contracture <= 15°, and flexion range >= 90° were accepted. More severe deformity, worse range of motion (ROM), or tricompartmental OA would be excluded from UKR and TKR would be performed instead.
The concept of bilateral UKR in one operation vs two operations were then introduced to patients with bilateral symmetrical medial OA knee, and they were allowed to choose. All patients needed to undergo standardized pre-operative assessment sessions (PAS), during which they would be assessed by anesthetists, physiotherapists and occupational therapists.
All the operations were performed by the same group of arthroplasty surgeons in a joint replacement center of a regional hospital, with the same surgical technique. Either a mobile or fixed bearing UKR implant would be used. All patients received standardized blood and pain management protocol, and all were referred to post-operative physiotherapy.
Their demographic data, American Society of Anesthesiologists (ASA) grading, cumulative operative time and LOS, postoperative haemoglobin (Hb) drop after each operation, and complications were recorded. The cumulative number of admissions, PAS, and weeks of post-operative physiotherapy were analyzed. Clinical outcome (pre-operative, post-operative 3 and 6 months) was measured by Knee society knee score and ROM.
For statistical analysis, continuous variables were analyzed with T-test and categorical variables were analyzed with Chi-squared test in Excel. P-value of <0.05 was taken as statistical significant.
Ethical approval for this study was obtained from the Research Ethics Committee of our hospital (Ref. No: NTWC/REC/20056).
Results
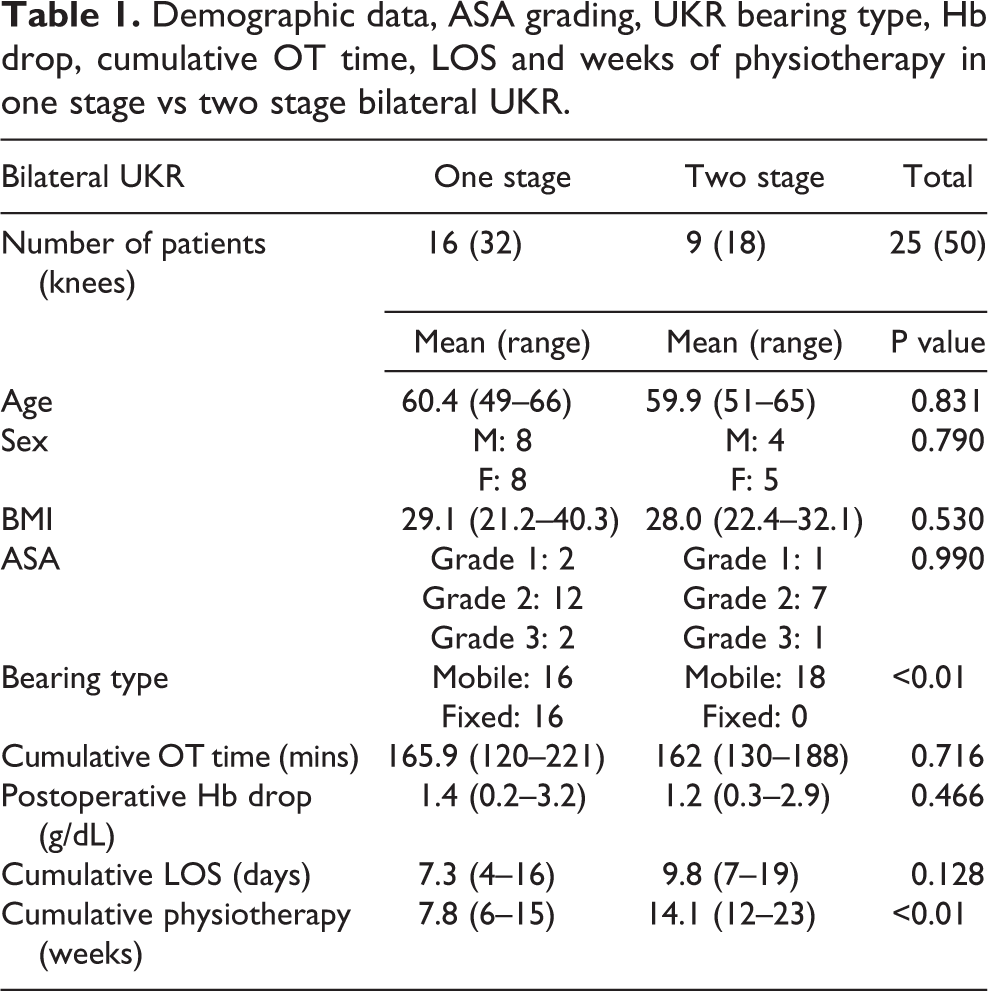
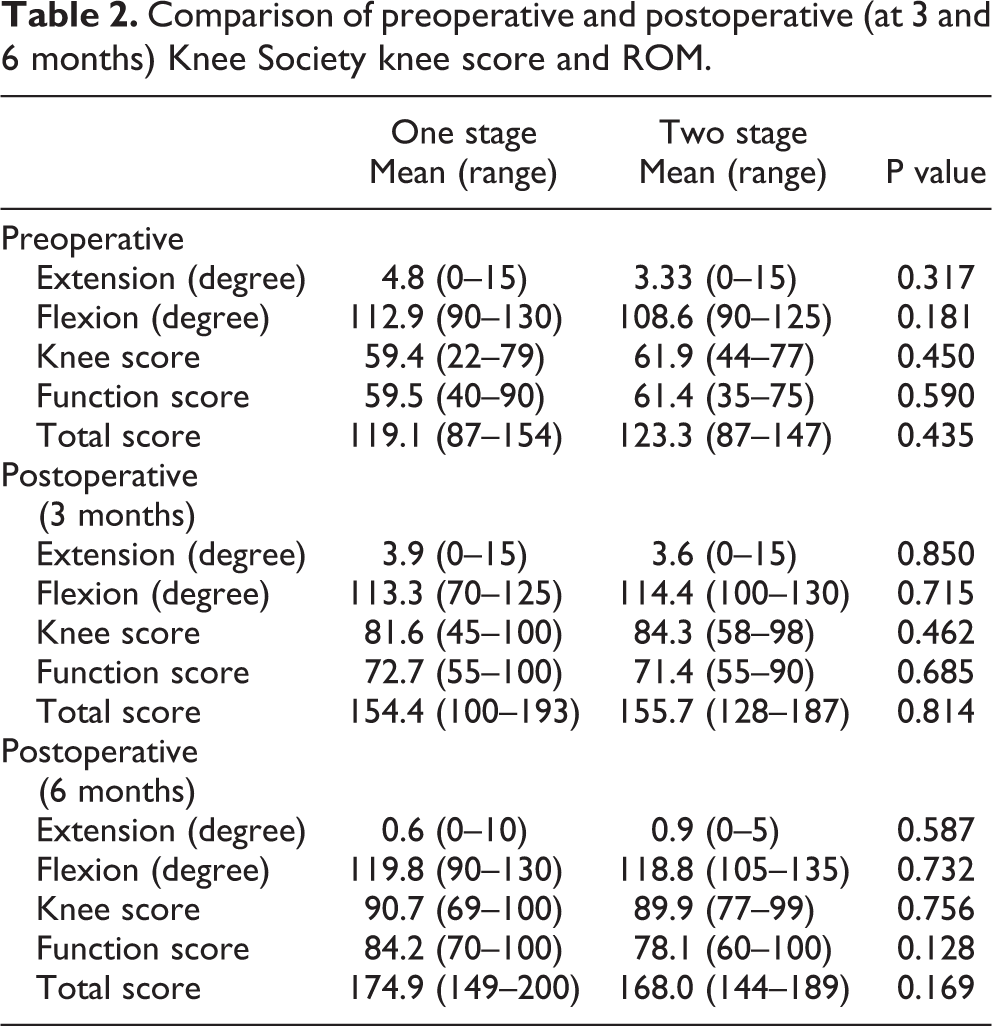
We performed 97 UKR in 2018–2019. There were 50 UKR performed in 25 patients with bilateral medial OA knee, among which 16 received one stage while 9 received two stage bilateral UKR. Both groups had similar mean age, BMI, sex ratio and ASA grading. Patient in the one stage group required only 1 PAS/admission/operation to treat both knees with a mean LOS of 7.3 days and 7.8 weeks of physiotherapy, while those in the two stage group required 2 PAS/admissions/operations with a mean cumulative LOS of 9.8 days and 14.1 weeks of physiotherapy. There was no re-admission for both groups. The mean cumulative operative time (165.9 vs 162 mins) was similar but the one stage group only required 1 operative session. Mean Hb drop after each operation (1.4 vs 1.2 g/dL) was similar and no transfusion or complication occurred in both groups (Table 1). The knee score and ROM at pre-operation, post-operative 3 and 6 months were similar in both groups (Table 2).
Demographic data, ASA grading, UKR bearing type, Hb drop, cumulative OT time, LOS and weeks of physiotherapy in one stage vs two stage bilateral UKR.
Comparison of preoperative and postoperative (at 3 and 6 months) Knee Society knee score and ROM.
Discussion
One stage (or single/same stage) bilateral knee replacement has been reported extensively, but most of the literatures focus on TKR instead of UKR. 13 –21 The advantages include single operation and anesthesia, 13 –16,22 –26 overall faster recovery and shorter total LOS, thereby reducing the financial cost. 14,22 –26 However, there are still a lot of debates about the safety of one stage bilateral TKR. Some studies showed more transfusion was required, 14,20 more medical complications and mortality 17 –21 while some showed no increased risk 13,15,16 compared with staged operation.
On the other hand, there are less studies focusing on one stage bilateral UKR. TKR and UKR are two different operations, thus study results of bilateral TKR may not be applied to UKR directly. UKR has been proven to have less mortality and medical complications compared with TKR. 7 For one stage bilateral UKR, most studies have shown it has all the advantages of one stage bilateral arthroplasty without increased complications compared with staged operation 22 –26 and only one study showed the opposite. 27
Our center offered one stage bilateral UKR for patients with bilateral medial OA knee without severe anesthetic risks. Therefore in our study patients’ ASA grading was at most grade 3. Moreover most of them were middle-aged as this group of patients are usually still working and active, but severe medial knee pain greatly limit their daily activities, yet usually their knees are not to the extent of tricompartmental involvement.
Our study showed that in this group of patients, one stage bilateral UKR is safe with similar minimal blood loss and no complications compared with one sided UKR. They required only a single admission, anesthesia and operative session to have both knees treated. The cumulative LOS is 2 days shorter despite not statistical significant. Duration of cumulative postoperative physiotherapy was significantly shorter by about 7 weeks as both knees could have rehabilitation simultaneously. The early postoperative knee score and ROM at 3 and 6 months were similar. Therefore having both knees replaced and trained together does not slow down the rehabilitation, with the same early satisfactory clinical outcome achieved. Our study confirmed that one stage bilateral UKR is beneficial to both patients and the healthcare system as the overall financial cost is reduced with better resources utilization.
There were some limitations in our study. It was retrospective in nature and only the early outcome was investigated. In addition, the postoperative social function (e.g. return to work) was not studied. Moreover, most patients were middle-aged and all were less than 70 years old. Whether one stage bilateral UKR has the same safety profile in the older patients could not be confirmed.
To conclude, in middle-aged patients with ASA grade <=3, one stage bilateral UKR offered the same satisfactory early clinical outcome and no increased complication compared with one-sided UKR. Total LOS and duration of rehabilitation were shorter than two stage operation and this is beneficial to patients and hospital resources utilization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.