
Abstract
Study Design
Retrospective cohort study.
Objectives
To evaluate national trends in management and outcomes of posterior spinal fusion for adolescent idiopathic scoliosis (AIS) over a 12-year period and characterize postoperative opioid utilization.
Methods
We used the PearlDiver Mariner database to identify patients aged 10-18 years with AIS undergoing posterior spinal fusion of >7 levels from 2010-2022. Patients were stratified into 2 epochs (2010-2015 and 2016-2022) to compare demographics, Elixhauser Comorbidity Index (ECI), surgical techniques, length of stay, complications, readmissions, revisions, and postoperative opioid prescriptions using chi-squared and t-tests. We also summarized characteristics across 3 eras (2010-2013, 2014-2017, 2018-2022) and fit year-by-year logistic regression models with 2010 as reference.
Results
Among 17,541 AIS patients, prevalence increased while the surgery-to-prevalence ratio declined. The later cohort had higher comorbidity burden (ECI 0.99 vs 1.25, P < 0.001), greater use of Ponte osteotomies, navigation, and robotics, and less pelvic fixation. Length of stay decreased (5.04 vs 4.12 days, P < 0.001), along with 30-, 90-day, and 1-year readmissions; 30-day complications; 90-day infections; and 2-year revision and hardware removal rates. Opioid exposure declined across all intervals, with reduced prescription rates, cumulative MME, MME/day, and duration.
Conclusion
From 2010-2022, posterior spinal fusion for AIS shifted toward greater technological adoption and increased Ponte osteotomy utilization in patients with higher comorbidity burden, while also being associated with shorter hospitalization, fewer complications, lower revision and readmission rates, and reduced opioid exposure, supporting an overall improved safety profile of AIS surgery.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) affects 1-3% of U.S. adolescents and is defined by a coronal Cobb angle greater than 10° in the absence of congenital or neuromuscular causes.1,2 Recent literature demonstrates that AIS is associated with impaired body image, mental health conditions, and quality of life in this particularly young population.3–6 Surgery is typically indicated in patients with a Cobb angle of at least 45°, while bracing and physical therapy aim to limit curve progression. 1
Current surgical intervention aims to correct coronal and sagittal deformity, yet optimal timing and technique is a subject of ongoing debate. 1 Furthermore, delayed surgical correction has been associated with worse outcomes and greater curvature progression into adulthood.7,8 Restoration of sagittal balance is influenced by multiple factors, including pre-existing kyphosis, curve flexibility, correction techniques, and the use of osteotomies. 9 Deformity correction relies on maneuvers such as rod rotation, with additional methods including osteotomies, in situ rod bending, direct vertebral rotation, and cantilevering. 9
Major concerns surrounding surgical correction include worsening pulmonary function, proximal junctional kyphosis particularly in patients with Lenke type 3 and 6 curves, instrumentation-related and neurological complications.10,11 However, the true incidence of these events complications is difficult to quantify given multifactorial etiologies. Lonner et al. reported that, between 1995-2013, use of the anterior approach, operative time, blood loss, length of stay, and 2-year complication rates declined, although radiographic curve corrections were not deemed clinically meaningful. 12 Existing AIS surgery trend data largely derive from single-institution series with small samples and older techniques, leaving the contemporary safety and efficacy of AIS surgery incompletely defined.
The primary aim of our study was to characterize evolving trends in AIS surgery and their potential impact on patient outcomes over a 12-year period (2010-2022). Secondary aims included describing changes in perioperative management, including comorbidity profiles and pain management strategies. By examining demographic characteristics, preoperative health status, surgical techniques, and postoperative complications, we sought to assess how these factors have changed over time in AIS patients and whether such changes were associated with differences in short-term outcomes.
Methods
Data Source and Study Population
The PearlDiver Mariner Database (PearlDiver Technologies, Fort Wayne, IN, USA) was queried for AIS patients who underwent posterior spinal fusion between 2010 and Q3 2022. PearlDiver is a robust nationwide dataset that includes approximately 157 million deidentified patient records encompassing demographics, diagnostic, and procedural data from all payer types and inpatient and outpatient settings. Due to the use of anonymized PearlDiver data and this study’s retrospective nature, informed consent was waived and Institutional Board Review approval was not required.
Identification of Study Cohorts
International Classification of Disease (ICD) 9th (ICD-9) and 10th (ICD-10) edition and Current Procedural Terminology (CPT) codes were used to identify patients (Supplemental Table 1). Patients aged 10–18 years with idiopathic scoliosis undergoing posterior spinal fusion of >7 levels were included. Patients were grouped by index procedure year (2010-2015 vs. 2016-2022). Exclusion criteria were age <10 or >18 years, less than 90 days of follow-up before or after surgery, rheumatoid arthritis, cauda equina syndrome, and indications of trauma, malignancy, or infection. Scoliosis due to neuromuscular, radiation, thoracogenic, or other secondary causes was also excluded. Demographics, comorbidities, and operative characteristics were compared between cohorts.
Primary Endpoints
Temporal trends in AIS surgical management and complications were evaluated by comparing 2010-2015 with 2016-2022. To examine temporal changes in practice while preserving power, we a priori divided the study period into 2 epochs: 2010-2015 and 2016-2022. We selected 2010 as the first study year because PearlDiver began data collection at that time. The binary structure ensured sufficient sample size and event counts within each period to allow stable estimation of complication, readmission, and revision rates, including relatively uncommon events such as robotic use and 2-year revisions. The 2015/2016 cut-point does not correspond to a single regulatory or guideline change but was chosen to contrast earlier vs later contemporary practice while avoiding over-fragmentation of the data into multiple small year strata. 13 Patients were additionally stratified into 3 eras (2010-2013, 2014-2017, 2018-2022) and modeled year-by-year to describe how case complexity, technology use (navigation/robotics), readmissions, complications, and opioid exposure evolved over time and to contextualize the primary epoch-based analyses.
Surgical management variables included Ponte Osteotomy (PO) and Pedicle Subtraction Osteotomy (PSO), as well as the use of computer navigation (NAV) systems and robotic technology. Intraoperative NAV and robotics were identified using adjunct procedure codes linked to the index posterior spinal fusion.14,15 Technology utilization was defined as the presence of at least one navigation or robotic adjunct code during the index hospitalization.
Primary outcomes included all-cause readmission at 30 days, 90 days and 1 year; 90-day infectious complications, 2-year revisions, and 30-day medical and surgical complications. Surgical complications included surgical site infection (SSI), deep infection, epidural hematoma, mechanical complications, graft complications, durotomy, post-op hemorrhage, spinal cord or nerve root damage, dehiscence, incision & drainage, irrigation & debridement, and hematoma. Medical complications included stroke, sepsis, acute kidney injury (AKI), transfusion, acute renal failure, GI/GU complications, blood loss anemia, pneumonia, bacterial infection, and urinary tract infection (UTI). Neurologic complications were defined using ICD-9 and ICD-10 diagnosis codes for spinal cord injury, nerve root injury, and central nervous system ischemia or stroke recorded within 30 days of the index procedure and should be interpreted at the population level; specific codes and groupings are provided in Supplemental Table 4.
Revisions included hardware removal and fusion. Secondary endpoints included postoperative opioid utilization, characterized by filled at 0-30 days, 30-90 days, 90-180 days, and 180-365 days, and quantified using total morphine milliequivalent (MME), MME/day, and prescription duration.
Statistical Analysis
Student’s t-test and Pearson chi-squared test of independence were used to compare continuous and categorical variables, respectively. The Pearson chi-squared test was employed to compare proportions between time periods, and Student's t-test was used to compare opioid utilization metrics. All analyses were performed using R studio (Version 4.4.2) within the PearlDiver Mariner Database program. A P-value <0.05 was considered statistically significant.
Results
Demographics of Patients Undergoing AIS Surgery
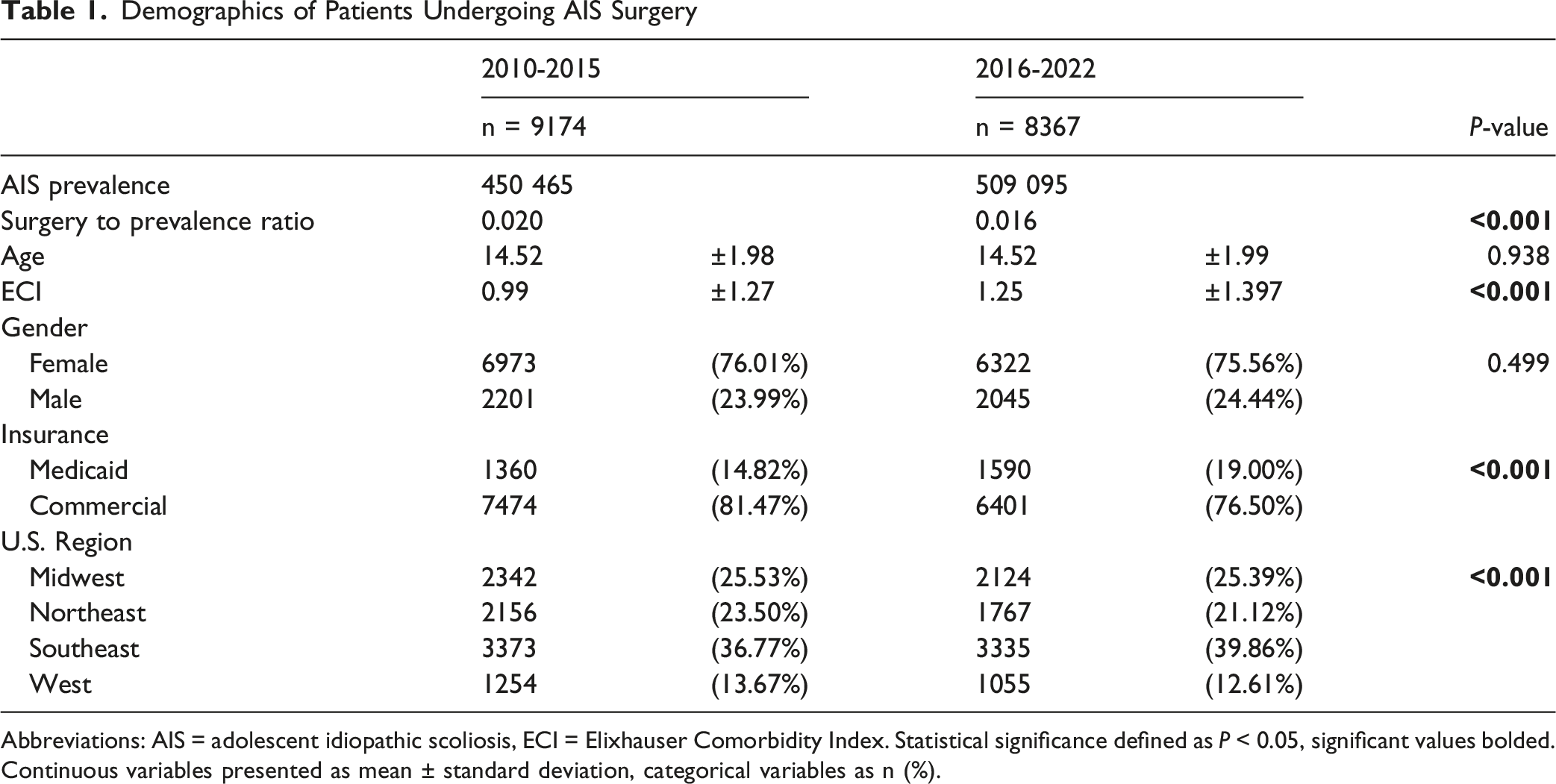
Abbreviations: AIS = adolescent idiopathic scoliosis, ECI = Elixhauser Comorbidity Index. Statistical significance defined as P < 0.05, significant values bolded. Continuous variables presented as mean ± standard deviation, categorical variables as n (%).
Patient Characteristics
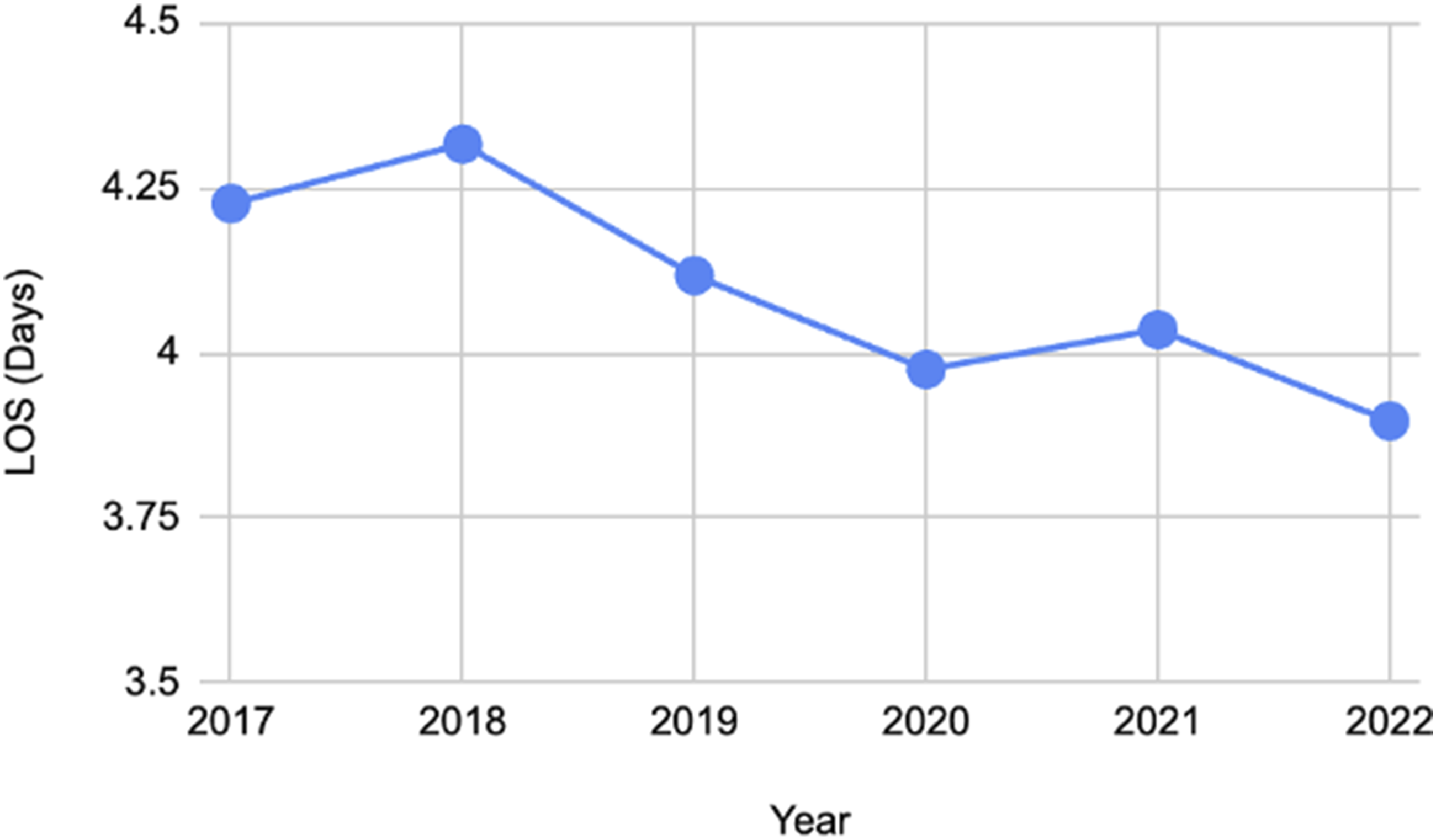
Between 2010-2015 and 2016-2022, there was no significant difference in the mean age of patients undergoing surgery for AIS with both periods having a mean age of 14.52 years (P = 0.938). The sex distribution remained consistent, with females comprising approximately 76% of both cohorts (P = 0.499). However, there were notable changes in preoperative health conditions across the 2 time periods. The Elixhauser Comorbidity Index (ECI) increased in the later time period from 0.99 (±1.27) to 1.25 (±1.39) (P < 0.001). The majority of AIS surgeries were paid with commercial insurance, 81.47% between 2010-2015 and 76.50% between 2016-2022, with medicaid coverage for AIS surgery increasing over time from 14.82% to 19.00% (P < 0.001). Geographically, AIS patients more commonly received surgery in the Southern United States across both time periods (36.77% to 39.86%, P < 0.001) (Table 1). Between pre-pandemic years (2017-2019) and peak pandemic years (2020-2022), the average annual number of surgical patients declined by 10.6%, from 1,238 to 1,107, with the largest decrease seen in 2022 (Figure 1). The average length of stay changed minimally, dropping from 4.22 to 3.97 days during the same periods (Figure 2). Annual number of surgical AIS patients from 2017 to 2022 Trend in average length of stay (LOS) for surgical patients from 2017 to 2022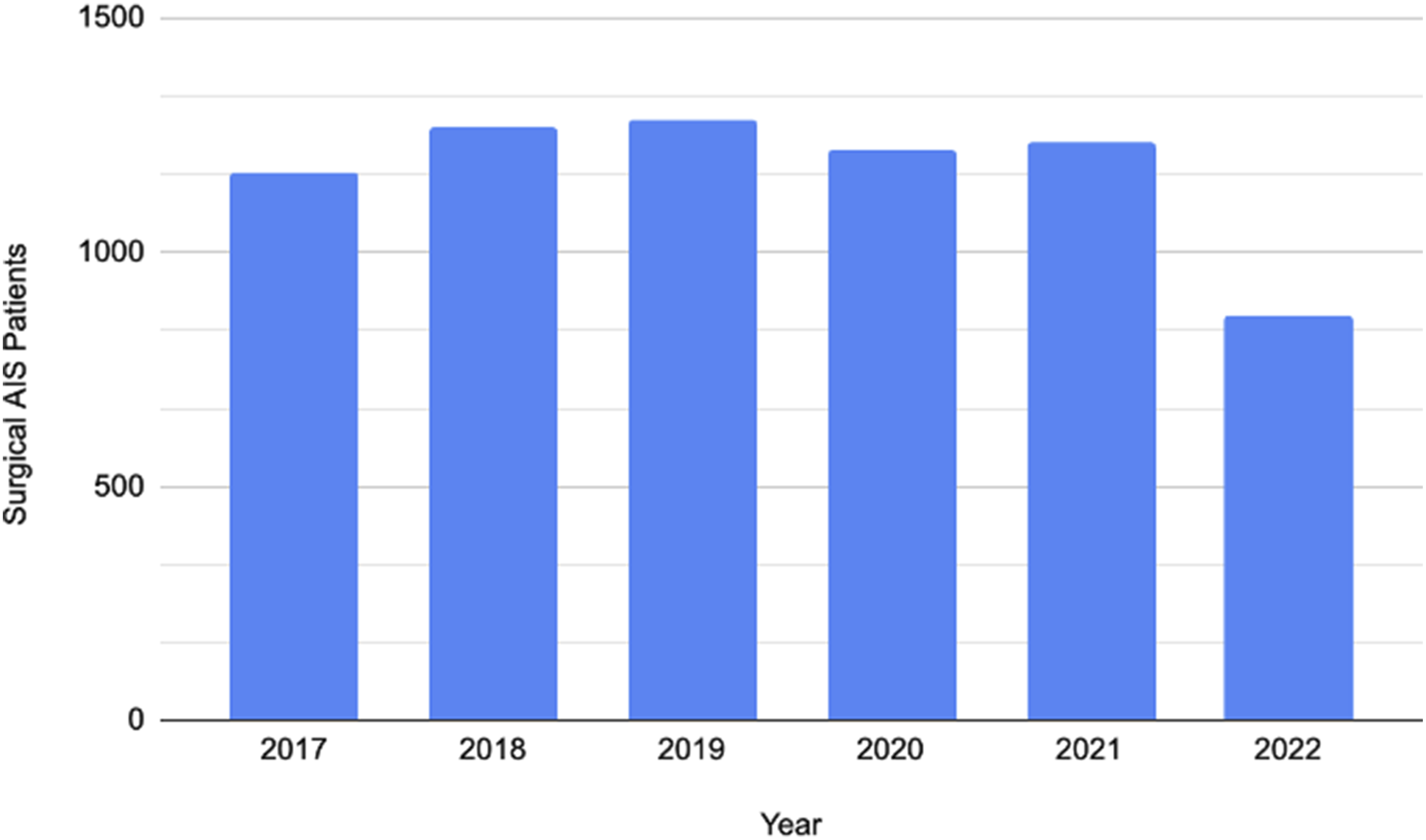
Surgical Interventions
Surgical practice demonstrated significant shifts between 2010-2015 and 2016-2022. The use of PO increased from 22.39% to 32.15% (OR 1.64, [1.54-1.76], P < 0.001), particularly in multi-level PO, which rose from 20.80% to 30.85% (OR 1.70, [1.59-1.82], P < 0.001). While the utilization of PSO remained somewhat stable from 0.81% to 0.56% (OR 0.69, [0.48-1.00], P = 0.052), multi-level PSO significantly declined from 0.41% to 0.13% (OR 0.32, [0.15-0.60], P < 0.001). Single-level PSO and anterior approaches both saw no difference in rates of use across both time periods.
Trends in Procedural Characteristics of AIS Surgery
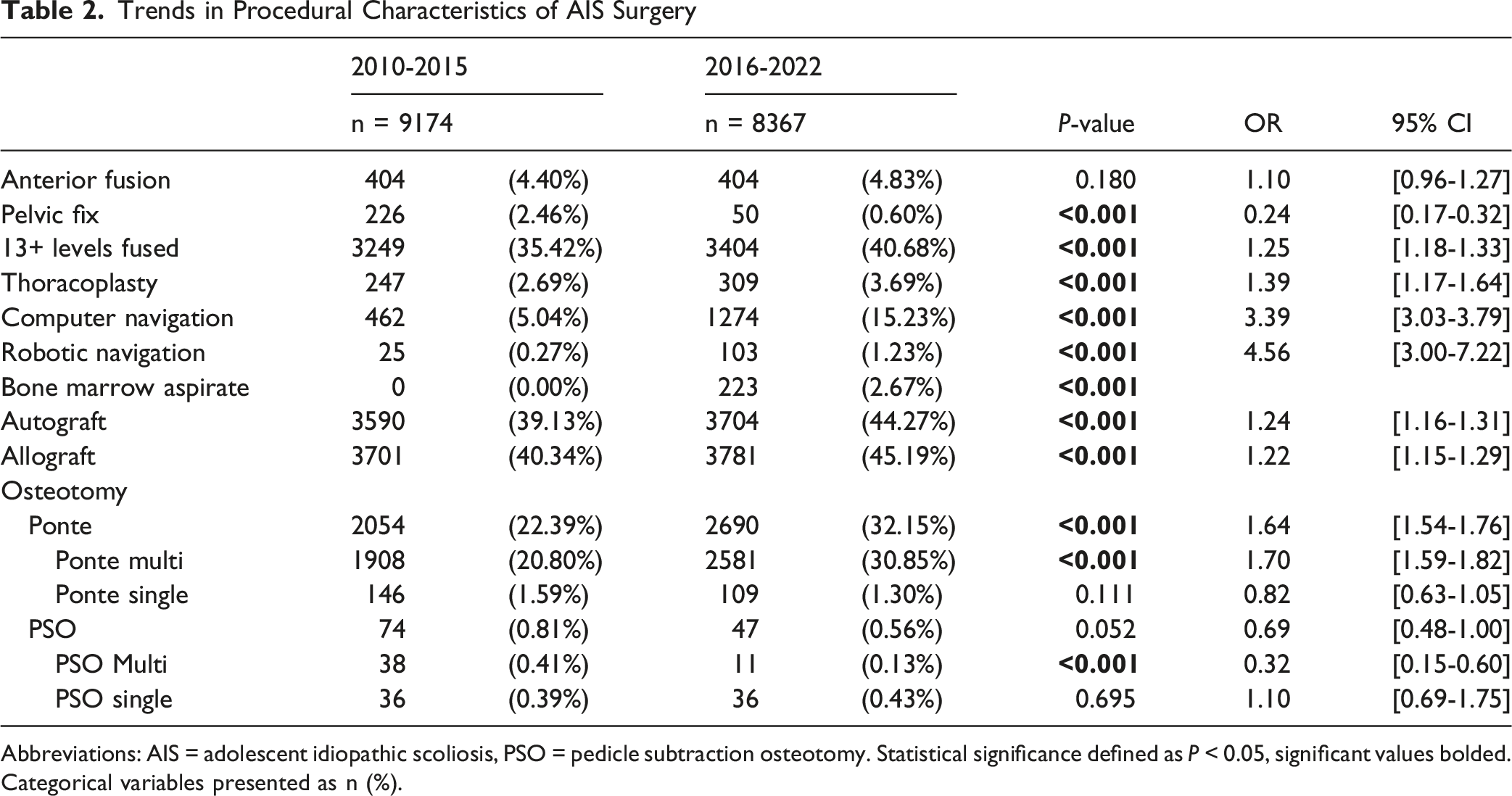
Abbreviations: AIS = adolescent idiopathic scoliosis, PSO = pedicle subtraction osteotomy. Statistical significance defined as P < 0.05, significant values bolded. Categorical variables presented as n (%).
Hospitalization Metrics
There were significant improvements in hospitalization metrics between 2010-2015 and 2016-2022. The length of stay (LOS) decreased from 5.04 ± 3.14 days in 2010-2015 to 4.12 ± 3.00 days in 2016-2022 (P < 0.001). Additionally, there were notable decreases in 30-day readmission rate from 6.73% to 3.99% (OR 0.58, [0.50-0.66], P < 0.001), 90-day readmission rate from 7.49% to 4.63% (OR 0.60, [0.53-0.68], P < 0.001), and 1-year readmission rate from 9.60% to 5.92% (OR 0.59, [0.53-0.66], P < 0.001).
The rates of 90-day infectious complications decreased over time. SSI decreased from 3.48% to 0.96% (OR 0.27, [0.53-0.68], P < 0.001), deep infection from 0.57% to 0.24% (OR 0.42, [0.25-0.69], P = 0.001), and incision & drainage from 1.18% to 0.76% (OR 0.65, [0.47-0.88], P = 0.006). Irrigation & debridement remained stable across both time periods.
Trends in Readmissions, Infections, and Revisions Following AIS Surgery
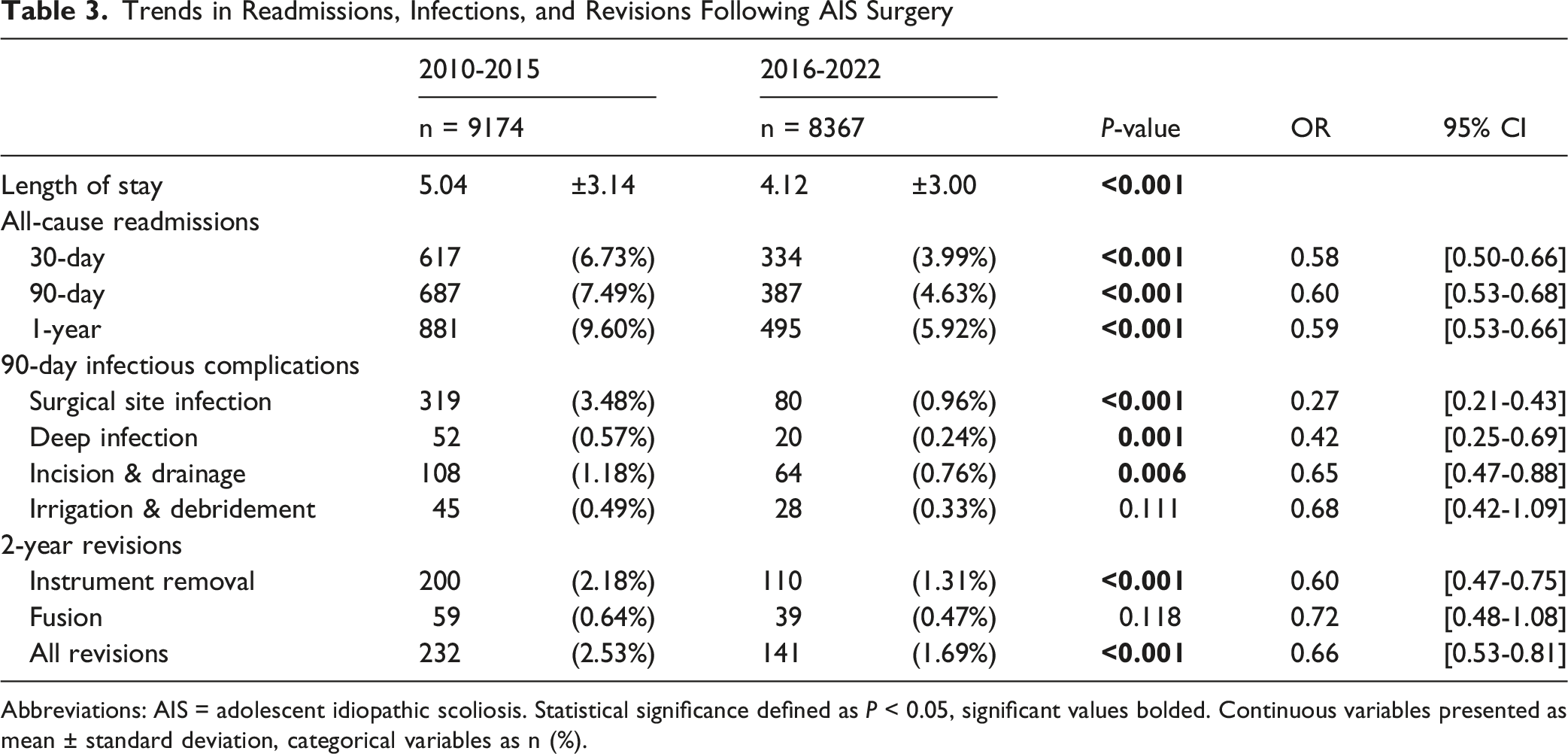
Abbreviations: AIS = adolescent idiopathic scoliosis. Statistical significance defined as P < 0.05, significant values bolded. Continuous variables presented as mean ± standard deviation, categorical variables as n (%).
30-Day Complications
Trends in 30-Day Medical and Surgical Complications Following AIS Surgery
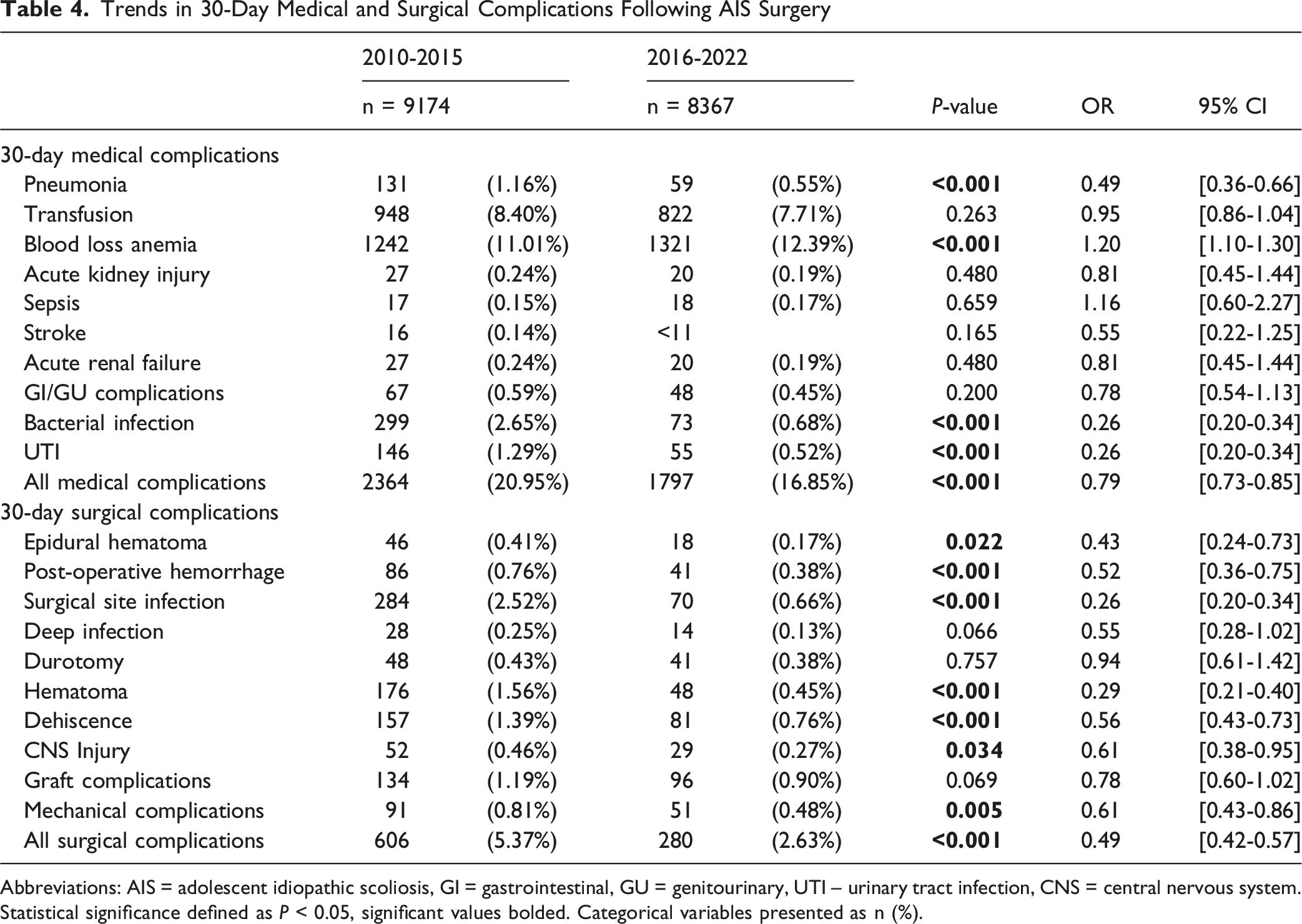
Abbreviations: AIS = adolescent idiopathic scoliosis, GI = gastrointestinal, GU = genitourinary, UTI – urinary tract infection, CNS = central nervous system. Statistical significance defined as P < 0.05, significant values bolded. Categorical variables presented as n (%).
The rate of all medical complications also decreased significantly from 20.95% to 16.85% (OR 0.79, [0.73-0.85], P < 0.001). Rates of bacterial infection and UTI notably fell from 2.65% to 0.68% (OR 0.26, [0.20-0.34], P < 0.001) and from 1.29% to 0.52% (OR 0.26, [0.20-0.34], P < 0.001), respectively. Pneumonia rates also declined significantly from 1.16% to 0.55% (OR 0.49, [0.36-0.66], P < 0.001). The rate of blood loss anemia showed a modest but significant increase from 11.01% to 12.39% (OR 1.20, [1.10-1.30], P < 0.001). Complication rates including blood transfusions, AKI, sepsis, acute renal failure, and GI/GU remained unchanged. Stroke was only able to be observed in the earlier period (0.14%) as 2016-2022 had <11 occurrences (Table 4).
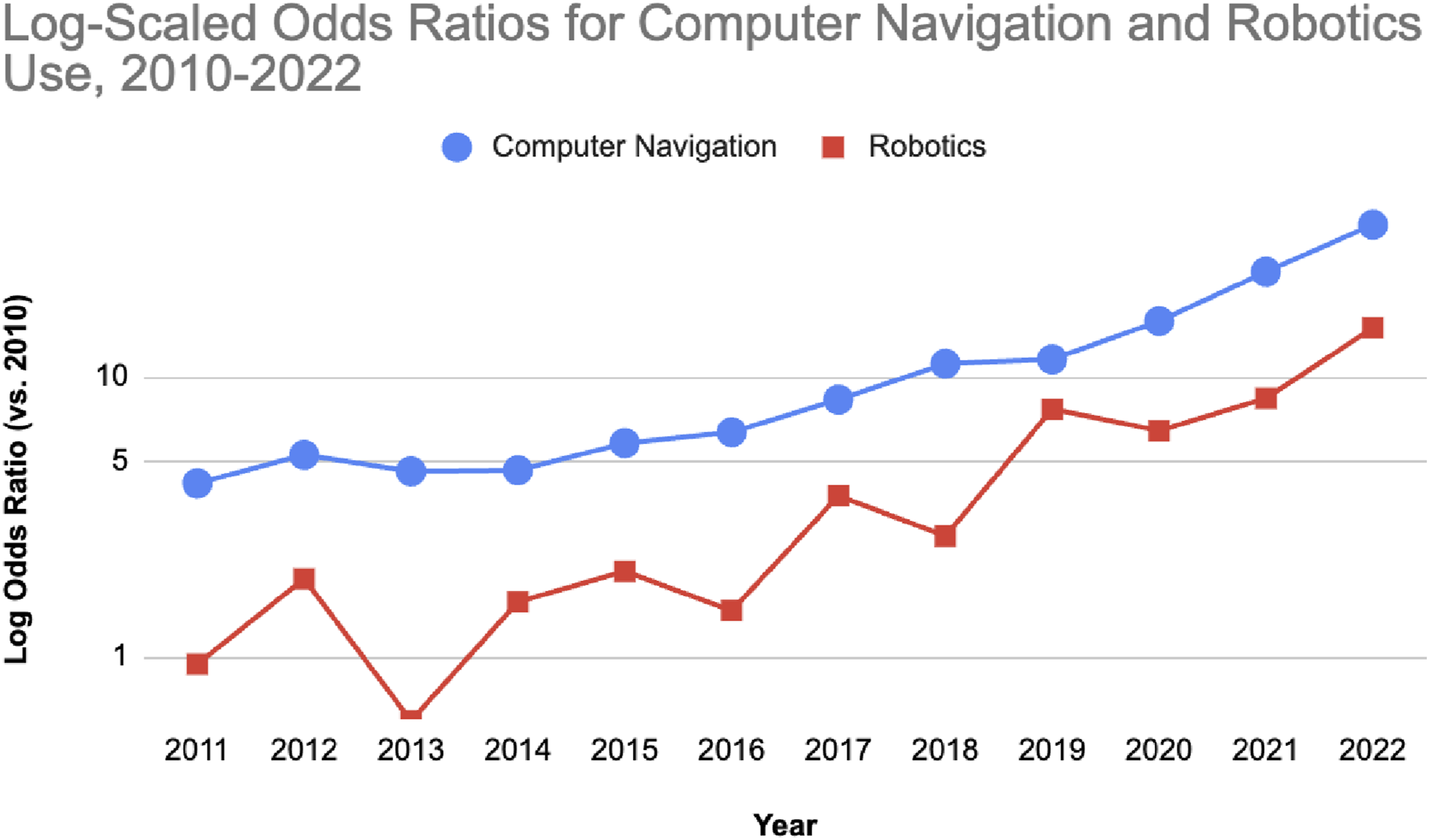
When calendar year was modeled as an independent variable, results supported a continuous trajectory rather than a single stepwise change between epochs (Supplemental Tables 2 and 3, Figures 3 and 4). Using 2010 as the reference, adjusted odds of 30-day surgical complications declined from 0.82 in 2011 to 0.38 in 2022 (P < 0.001 from 2016 onward), and 30-day medical complications from 0.95 in 2011 to 0.33 in 2022, with significant reductions beginning in 2015. One-year readmission odds fell to 0.57 (95% CI 0.41-0.77) by 2022. In contrast, technology utilization rose sharply (Supplemental Tables 2 and 3, Figure 4). Computer navigation use increased each year, with adjusted odds ratios rising from 4.17 in 2011 to 35.03 in 2022 (all P < 0.001), while robotic assistance, although infrequent, reached an odds ratio of 14.99 (95% CI 5.26-63.00) in 2022. Odds ratios for surgical complications, medical complications, and 30-day readmissions after AIS surgery from 2011 to 2022, plotted on a log scale relative to 2010 Odds ratios for computer navigation and robotics use in AIS surgery from 2011 to 2022, plotted on a log scale relative to 2010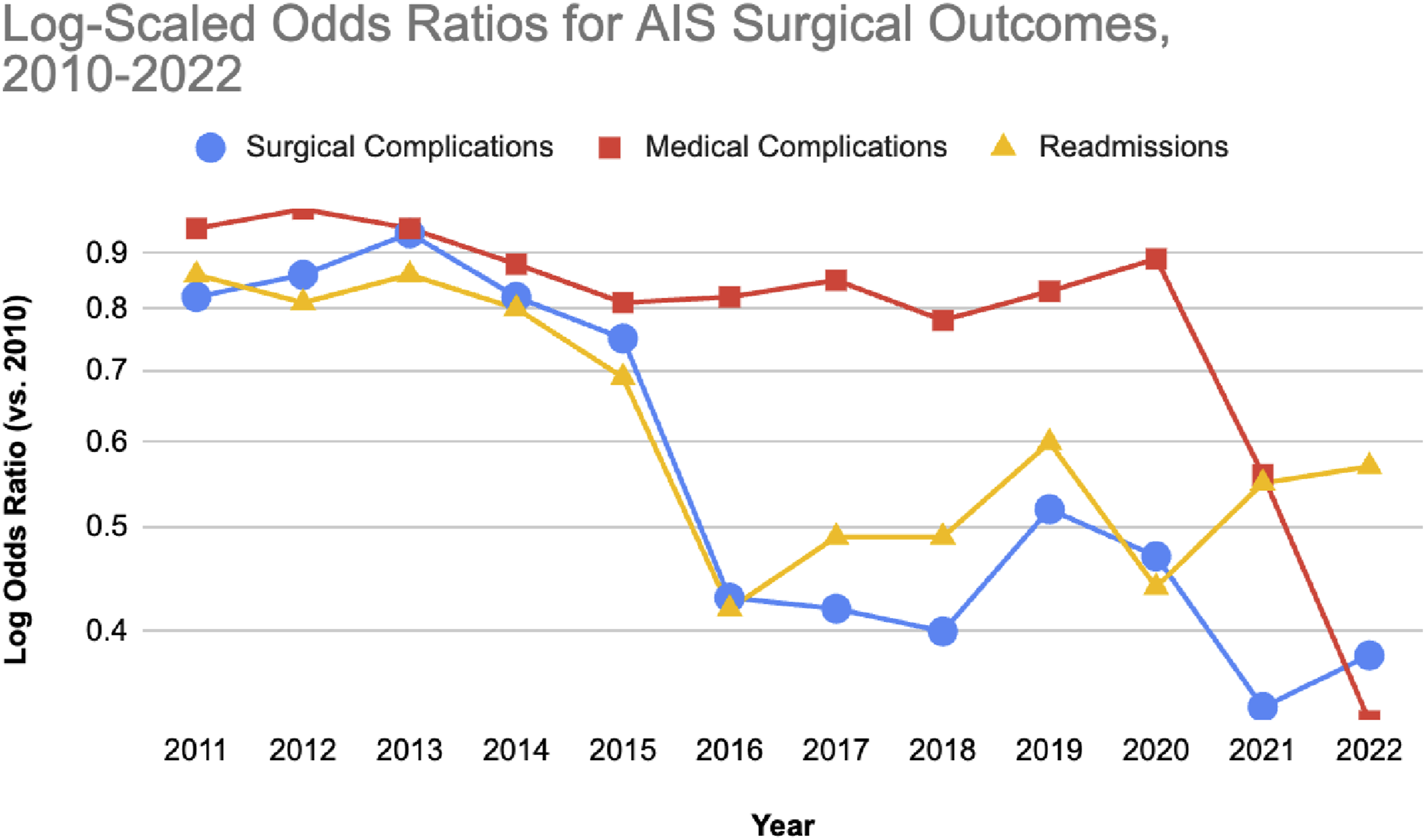
Opioid Usage
Trends in Opioid Prescriptions Following AIS Surgery
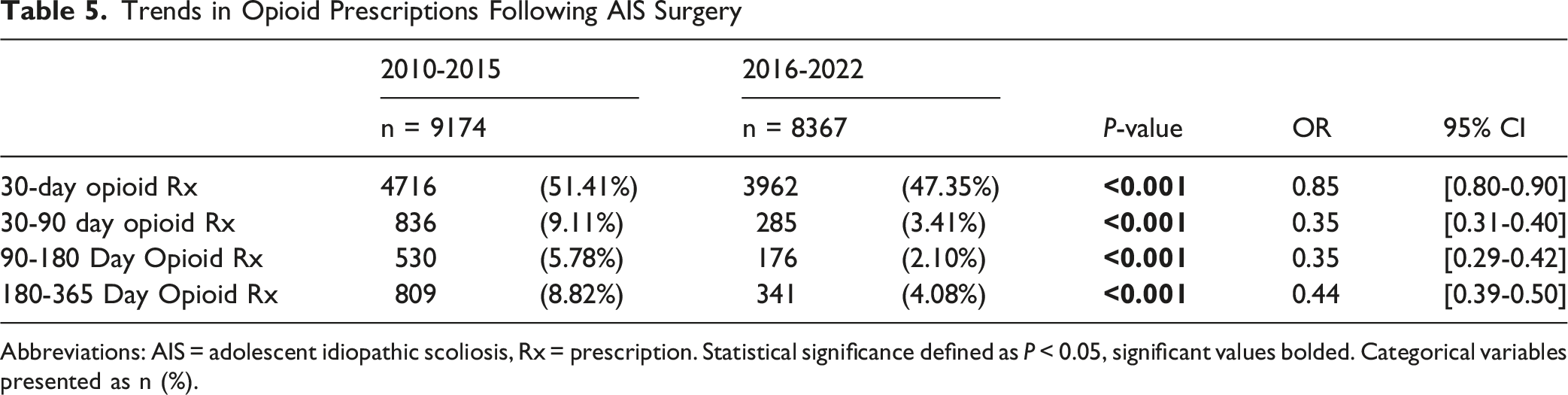
Abbreviations: AIS = adolescent idiopathic scoliosis, Rx = prescription. Statistical significance defined as P < 0.05, significant values bolded. Categorical variables presented as n (%).
Trends in Quantitative Opioid Use Following AIS Surgery
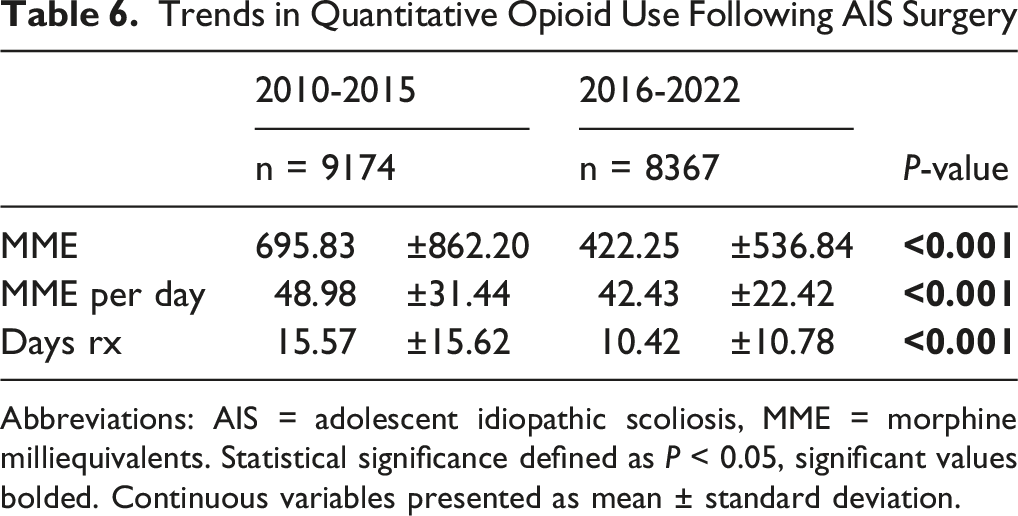
Abbreviations: AIS = adolescent idiopathic scoliosis, MME = morphine milliequivalents. Statistical significance defined as P < 0.05, significant values bolded. Continuous variables presented as mean ± standard deviation.
Discussion
Surgical trends for AIS have evolved over recent decades, with changes in surgical approaches, perioperative management, and complication profiles. Using a large national database, we found that from 2010-2015 to 2016-2022 more AIS patients were diagnosed but a smaller proportion underwent surgery, while those who did had higher coded comorbidity burden. Surgical practice appeared to shift toward greater use of NAV/robotic systems and Ponte osteotomies. Concurrently, 30-day medical and surgical complications, readmissions, and revisions declined, characterizing the trajectory of AIS surgery with respect to preoperative profiles, utilization, and safety. Year-by-year modeling using 2010 as the reference demonstrated a progressive decline in adjusted odds of surgical and medical complications and readmissions, and a monotonic rise in navigation and robotics use, supporting a picture of gradual, ongoing improvement in AIS surgical care and progressive technology diffusion, rather than a single inflection point tied to a particular year or policy change.
Diagnostic and Utilization Trends During COVID-19
Between 2017-2019 and 2020-2022, the average annual number of AIS surgery patients declined by 10.6% (from 1,238 to 1,107), with the largest reduction in 2022, reflecting the impact of the COVID-19 pandemic on elective surgical care. Length of stay changed little over this interval, suggesting that per-patient hospitalization patterns remained stable despite lower surgical volumes. These findings are directionally consistent with multicenter pediatric data showing sustained reductions in elective procedures—especially musculoskeletal cases—during the pandemic, with disproportionate effects in socioeconomically disadvantaged groups.16,17 The declining surgery-to-prevalence ratio from 0.020 to 0.016, despite improving outcomes, likely reflects a combination of more effective nonoperative management, including improved bracing efficacy in BRAIST, 18 the emergence of fusion-sparing options such as anterior vertebral body tethering,19,20 pandemic-related deferral of elective surgery, and persistent access barriers. Limited Medicaid acceptance among spine surgeons suggests that insurance status and geography may further suppress surgical utilization even as overall safety improves. 21
Safety Improvements in AIS Surgery: Declining Complication, Revision, and Readmission Rates
We observed significant reductions in 2-year revision rates (2.53% to 1.69%), 30-day surgical complications (5.37% to 2.63%), and 30-day medical complications (20.95% to 16.85%). Fusion rates remained stable, while instrumentation removal decreased significantly. Given that implant malposition/failed internal fixation and infections have historically been the leading causes of complications and early revision surgery, their reported decline may have contributed to the reduction in 2-year revision rates.22–25 Our findings parallel those of Bartley et al., who observed decreasing wound- and instrumentation-related complications between 1995 and 2014,
10
and Kwan et al., who reported a drop in overall complication rates from 4.95% to 0.98% over 13 years.
26
The decline in SSIs at both 30- and 90-days in our cohort—potentially aided by the increased use of intrawound antibiotic powder—further supports this trend.
27
Additionally, shorter hospital stays (5.04 to 4.12 days) and lower readmission rates at 30, 90 days, and 1 year are consistent with evolving perioperative strategies, including enhanced recovery pathways, optimized pain control, and early mobilization, which have been associated with improved outcomes in prior studies.11,28–30 Although operative times shortened and most medical complications decreased, acute blood-loss anemia rose modestly. This trend likely reflects increased case complexity (greater use of multilevel fusion, autograft, and allograft) as well as more vigilant recognition and coding of postoperative anemia, rather than worsening intraoperative hemostasis
Technological Advancements and Evolving Surgical Techniques in AIS Surgery
Surgical technique evolved toward greater use of low-grade osteotomies and image-guided technologies. Multilevel POs increased, whereas multilevel PSOs—associated with greater blood loss despite similar correction—declined, consistent with a preference for safer, less invasive correction strategies when feasible.33–35
The adoption of NAV and robotic systems also increased, with NAV use rising from 5.04% to 15.23% and robotic-assisted surgery from 0.27% to 1.23% (Table 2). Navigation and robotics adoption also increased, mirroring literature showing improved pedicle screw accuracy and, in some series, lower complication rates compared with freehand techniques, albeit with mixed effects on transfusion and operative time.33,36,37 While these technologies enhance precision and may reduce certain intraoperative risks, they also expose AIS patients to substantially higher cumulative radiation doses compared to lower-dose or non-ionizing imaging modalities, contributing to a projected increase in lifetime cancer risk. 38 Furthermore, their effect on surgical skill development in trainees remains a concern; however, Gofton et al. found that, despite the enhanced feedback associated with this technology, the navigation group demonstrated no reduction in long-term learning compared with conventional training in total hip replacement. 39
Notably, our observed adoption rates likely underestimate true use, particularly at academic centers where these technologies may already be standard practice. Claims-based data have limited sensitivity for technology capture; a recent validation study reported only 57.8% sensitivity for robotic coding overall, falling below 50% for outpatient procedures. 40 Under-ascertainment is likely to worsen as spine surgery continues to shift to ambulatory settings. Inconsistencies across datasets further support this, with prior work showing navigation use of 3.3% in the Nationwide Inpatient Sample vs 10.76% in MarketScan over similar periods, suggesting divergent coding practices.14,15 Several factors contribute to systematic underreporting. Underreporting is driven by incomplete use of navigation/robotic modifiers, immature technology-specific code sets (only recently standardized), 41 and persistent institutional variation in coding infrastructure. Accordingly, the NAV and robotic utilization rates in this study should be interpreted as conservative, exploratory estimates of diffusion rather than precise measures of true use.
Declining Opioid Prescriptions and Usage
Orthopedic surgeons are among the highest prescribers of opioids and lead all surgical specialties in opioid prescribing volume. 42 Reducing opioid exposure remains a national priority, reinforced by recent regulatory guidance, 43 and is particularly relevant in AIS surgery where postoperative pain is a central concern for patients and families. 44 Early exposure to prescription opioids has been associated with future opioid misuse.45–48 In this context, reductions in opioid prescription rates, cumulative MME, MME/day, and prescription duration across all postoperative intervals are encouraging and align with national trends toward more judicious prescribing.46,49,50 These changes likely reflect a combination of wider multimodal analgesia use, institutional and regulatory prescribing policies, greater awareness of opioid risks, and possible shifts toward less invasive techniques. Prior AIS studies have shown that multimodal analgesia can reduce opioid requirements and length of stay without worsening pain scores, and institutional guidelines have safely reduced prescribing in some settings.51,52
At the same time, lower opioid exposure is not uniformly beneficial in isolation. Because our dataset lacks pain scores, specific analgesic protocols, and center-level policy information, we cannot determine the relative contribution of these mechanisms or exclude undertreatment of pain in a subset of patients. 53 The persistent minority with prolonged opioid use highlights the need for future work incorporating patient-reported outcomes, detailed analgesic regimens, and policy-level data to distinguish effective stewardship from restrictive prescribing and to identify adolescents at risk for persistent opioid use.
Limitations
This study has several important limitations. First, it is a retrospective analysis of an administrative claims database and is therefore subject to coding errors, misclassification, and limited granularity of all relevant clinical details. Our identification of navigation and robotic use relies on ICD-9/10 and adjunct procedural codes, which may not capture all instances of technology utilization; these tools are sometimes bundled into institutional charges, may not be separately reimbursed, and are coded heterogeneously across hospitals and payers. As a result, absolute adoption rates are likely underestimated, even if the direction and relative magnitude of temporal trends are preserved. Furthermore, the database lacks information on the primary reason for readmission as well as severity and duration of neurologic deficits, detailed radiographic data, including Cobb angle measurements, sagittal parameters, and curve flexibility—factors that are critical to understanding deformity severity, surgical planning, and outcome interpretation. Without this information, we could not assess curve characteristics, degrees of correction achieved, or radiographic outcomes. Although we controlled for several comorbidities using the ECI, the database does not provide clinical nuance regarding the severity or functional impact of these conditions and therefore were not able to fully explore interactions between preoperative health conditions and postoperative opioid use.
Conclusion
This study underscores the evolving landscape of AIS surgery, describing temporal changes in surgical techniques, technology use, and perioperative care that coincided with lower complication, revision, and readmission rates over time. By delineating trends such as the increasing use of low-grade osteotomies and the adoption of technologies like computer navigation and robotics, this work adds to the growing evidence base characterizing contemporary surgical practice and complication profiles in AIS. Future research should investigate radiographic and patient-reported outcomes, the cost-effectiveness and safety of advanced technologies, and predictors of persistent opioid use in adolescents undergoing AIS surgery.
Supplemental Material
Supplemental material - Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022
Supplemental material for Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022 by Maya S. Abu-Zahra, BA, William J. Karakash, BS, Daniel Rusu, BS, Justin W. Zheng, BA, Aidan Lindgren, BS, Chimere O. Ezuma, MD, MBA, Henry Avetisian, MS, Jeffrey C. Wang, MD, Ram K. Alluri, MD, Raymond J. Hah, MD and Michael M. Safaee, MD in Global Spine Journal
Supplemental Material
Supplemental material - Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022
Supplemental material for Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022 by Maya S. Abu-Zahra, BA, William J. Karakash, BS, Daniel Rusu, BS, Justin W. Zheng, BA, Aidan Lindgren, BS, Chimere O. Ezuma, MD, MBA, Henry Avetisian, MS, Jeffrey C. Wang, MD, Ram K. Alluri, MD, Raymond J. Hah, MD and Michael M. Safaee, MD in Global Spine Journal
Supplemental Material
Supplemental material - Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022
Supplemental material for Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022 by Maya S. Abu-Zahra, BA, William J. Karakash, BS, Daniel Rusu, BS, Justin W. Zheng, BA, Aidan Lindgren, BS, Chimere O. Ezuma, MD, MBA, Henry Avetisian, MS, Jeffrey C. Wang, MD, Ram K. Alluri, MD, Raymond J. Hah, MD and Michael M. Safaee, MD in Global Spine Journal
Supplemental Material
Supplemental material - Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022
Supplemental material for Trends and Outcomes in Adolescent Idiopathic Scoliosis Surgery: A Nationwide Analysis of Improvements from 2010 to 2022 by Maya S. Abu-Zahra, BA, William J. Karakash, BS, Daniel Rusu, BS, Justin W. Zheng, BA, Aidan Lindgren, BS, Chimere O. Ezuma, MD, MBA, Henry Avetisian, MS, Jeffrey C. Wang, MD, Ram K. Alluri, MD, Raymond J. Hah, MD and Michael M. Safaee, MD in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
There are no direct conflicts of interest with this study. MA, WK, JZ, DR, AL, CE, HA, and MS have nothing to disclose. JW has received royalties from Biomet, Seaspine, Novapproach, Synthes, and GS Medical; has received consulting fees from Depuy, Synthes, Bioretec and has stock ownership in Bone Biologics, Electrocore, PearlDiver, Surgitech, Illuminant. RA has received consulting fees from Ecelsius Robotics, Globus, and Medtronic, and has stock ownership in HIA technologies. RH has received consulting fees from Medtronic, Globus, Orthofix, Cerapedics, SI-Bone, Evolution Spine and has spoken at NASS.
Data Availability Statement
Upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.