
Abstract
Study Design
Retrospective consecutive cohort study.
Objective
For patients with mild to moderate adolescent idiopathic scoliosis (AIS), bracing is the standard therapy to prevent progression of deformity. Still, not all patients benefit from treatment in the same way. Therefore, predictive parameters are needed to determine if patients are likely to benefit from brace therapy.
Methods
Fourty-five AIS patients treated with a Chêneau brace were evaluated retrospectively. Inclusion criteria were based on SRS-criteria. Whole spine X-rays were performed pre-brace, in-brace, and at least 6 months after termination of brace treatment. Gender, age, Risser’s sign, vertebral rotation determined by Nash and Moe grading system, in-brace correction and in-brace time per day were parameters evaluated. Treatment success and failure groups were compared to determine possible predictive parameters for successful brace treatment.
Results
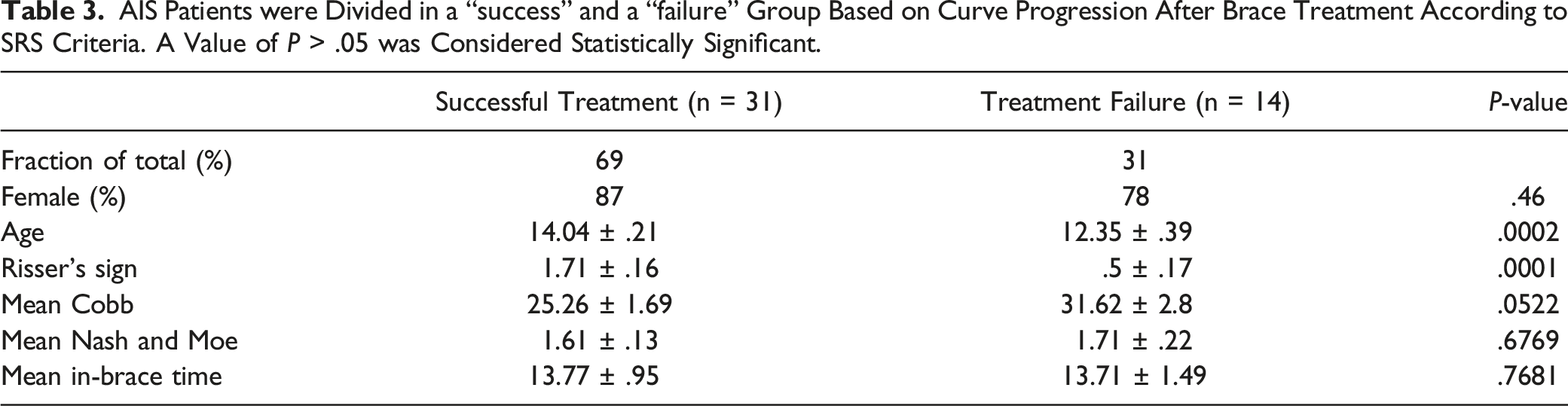
Chêneau brace treatment was successful preventing curve progression in 69%. We found significant differences between success and failure group concerning age (14 ± .22 vs 12.4 ± .4; P < .001) and Risser’s sign (1.71 ± .16 vs .5 ± .17; P < .001) at beginning of brace treatment. Most significantly, initial in-brace curve correction was correlated with successful outcome after brace treatment (r = .64 (P < .001)).
Conclusions
As one of few studies adhering to the criteria defined by the Scoliosis Research Society our study shows reliable predictive parameters for Chêneau brace treatment success in patients with AIS. Data shown in this paper will help to differentiate AIS patients who are likely to benefit from adequate bracing therapy from those who could rather benefit from early surgical treatment.
Introduction
Adolescent idiopathic scoliosis (AIS) is a spinal deformity defined by a Cobb angle of more than 10° in the coronal plane as well as vertebral body rotation. 1 For AIS patients with a mild to moderate curve (20-40°), data generally show the effectiveness of bracing to prevent or reduce curve progression. 1 However, for reasons we do not fully understand yet, not all patients benefit from adequate brace therapy in the same manner.
Efforts have been made to determine predictive parameters that could help decide if a patient is likely to benefit from bracing during an early stage of therapy. Factors like skeletal age at the time of bracing, initial severity of the curve, curve flexibility, in-brace time per day, initial in-brace curve correction as well as brace design were shown to have an influence on curve progression during brace therapy.2-4 Some data though is inconclusive, most likely due to the heterogeneity of the patient collective as well as the different types of braces used. The lack of uniformity of study inclusion criteria as well as variations in the definition of brace treatment success and failure pose a major obstacle in the comparison of different treatment protocols. Therefore, in 2005, the Scoliosis Research Society (SRS) published guidelines that future studies evaluating brace therapy could adhere to. 5 Inclusion criteria for this study were based on the criteria defined by the SRS.
Over the past years, growth-preserving surgical techniques as growing rod-systems and VBT have become an alternative to brace therapy in patients with progressive AIS. While the idea of growth preserving surgery for AIS patients was already introduced in the early 60s of the past century by Paul Harrington, 6 it was the introduction of magnetically controlled growing rod systems and anterior vertebral body tethering (aVBT) that might cause a paradigm shift in the treatment of progressive AIS.7,8 Despite the excitement that aVBT generated in some, a recent meta-analysis found significantly increased rates of complications and reoperations in patients receiving aVBT in comparison to posterior fusion. 9 Nevertheless, the need for predictive parameters for brace therapy has become more urgent with the establishment of modern growth-preserving surgical techniques. Valid predictive parameters could help to select patients who benefit from early surgical treatment rather than brace therapy. The aim of this retrospective study was (1) to evaluate results of Chêneau brace therapy in AIS patients that were included based on SRS-criteria and (2) to determine predictive parameters for brace treatment success in patients with AIS.
Methods
Exclusion Criteria for Patients with Adolescent Idiopathic Scoliosis that Received Treatment in Our Institution from 2015-2018.
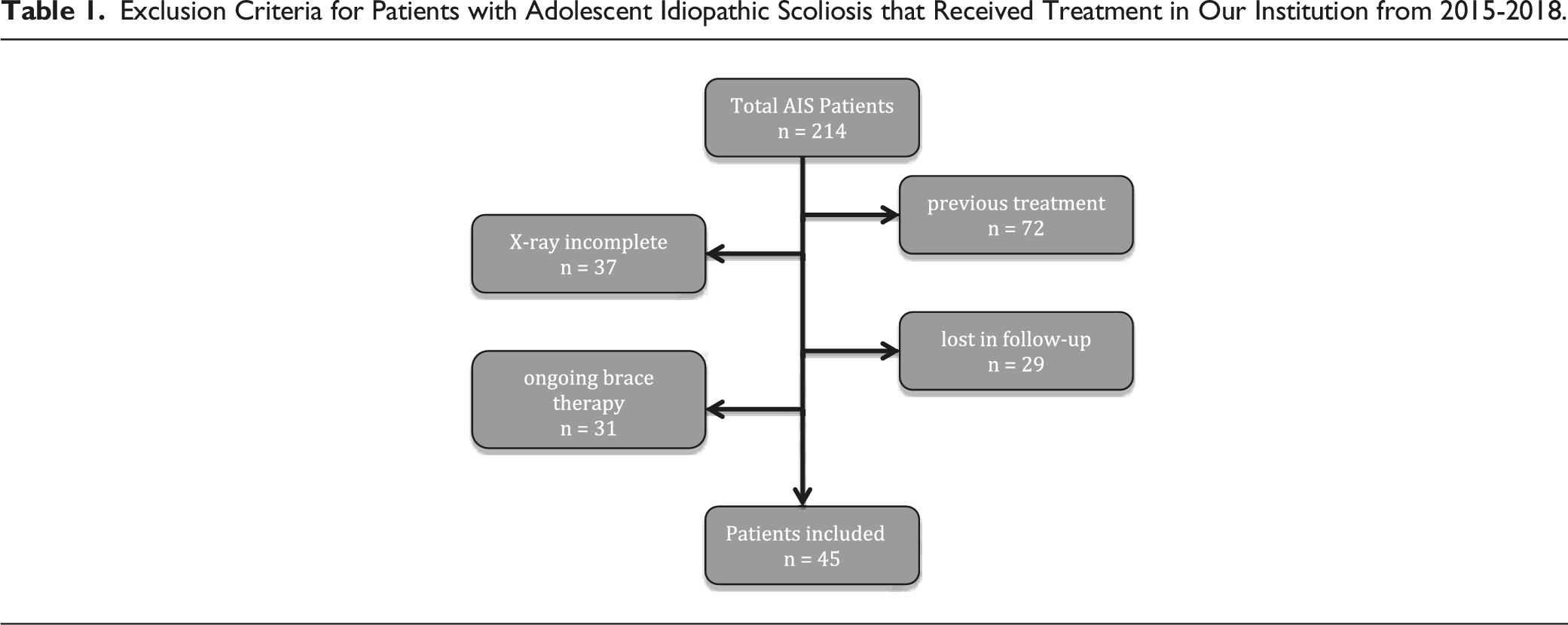
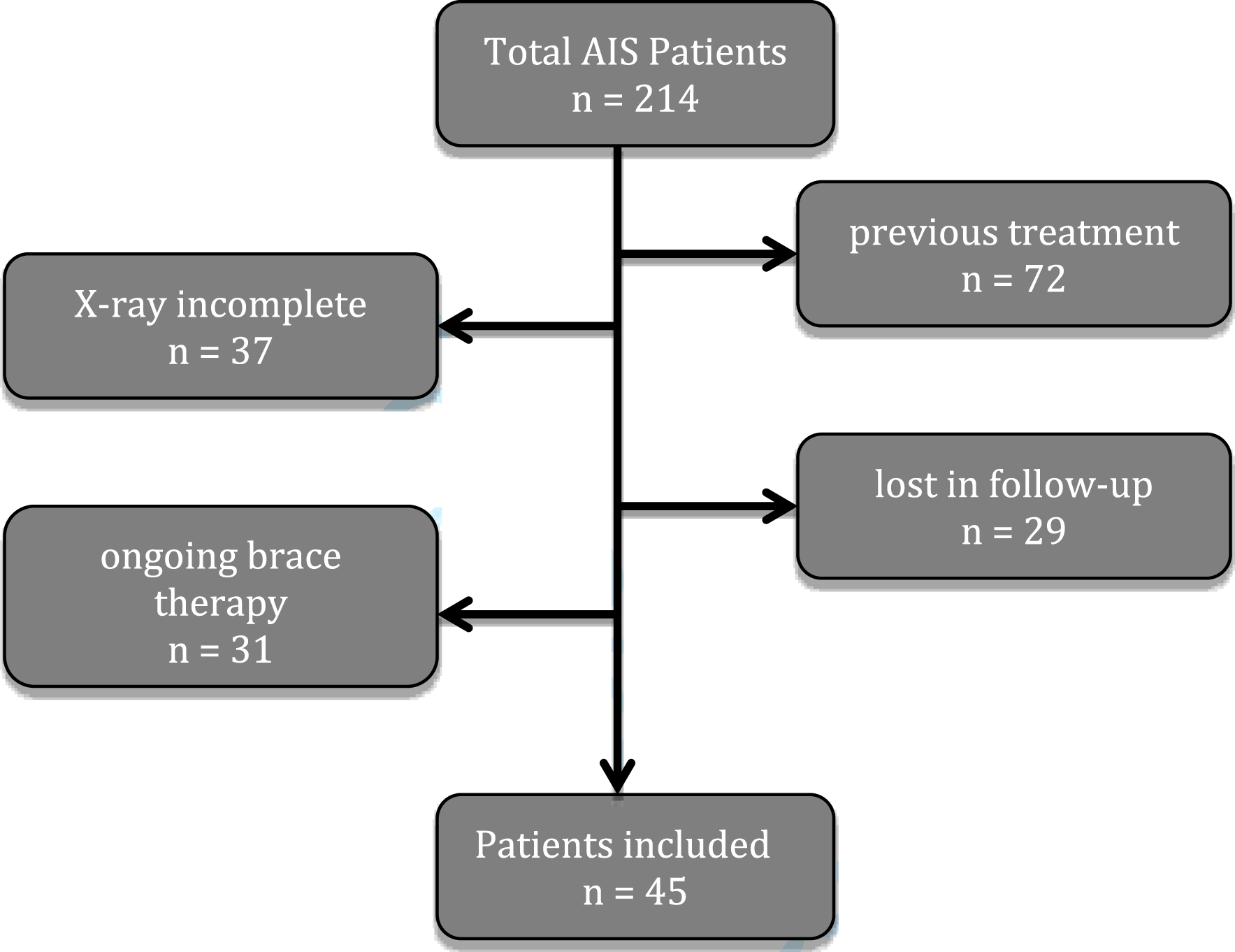
Inclusion criteria were based on SRS-criteria 5 : patients with adolescent idiopathic scoliosis with no prior brace treatment before presenting at our clinic; age >10 years; Risser 0-3 at the beginning of brace therapy; initial scoliotic curve of 20-45°. Female patients were included if they were either premenarcheal or less than 1 year postmenarcheal. Follow up after brace therapy had to be at least 6 months. Patients were only included if whole spine and X-rays were available before, during and after brace therapy. For Lenke classification, bending X rays are routinely performed using EOS-Xray technology.13,14 AIS patients curve pattern were analyzed independently by 2 spine surgeons and classified according to the Lenke system. To ensure an adequate fitting and curve correction of the braces, all braces were manufactured and customized by one of two orthopedic technicians during the entire period of the study. Optimal correction of the curve was ensured radiologically by an in-brace, whole spine EOS-Xray and clinically by one of two experienced spine surgeons (LWJ, AK). In accordance with available data, full time bracing was advised (at least 18 h per day). 1 All braces had integrated heat-sensors (Orthotimer®, Germany) to objectively measure in-brace time. 1 Additionally, patients were advised to perform physiotherapy and/or sport on a regular base (at least 2×/week for 1 h). 15
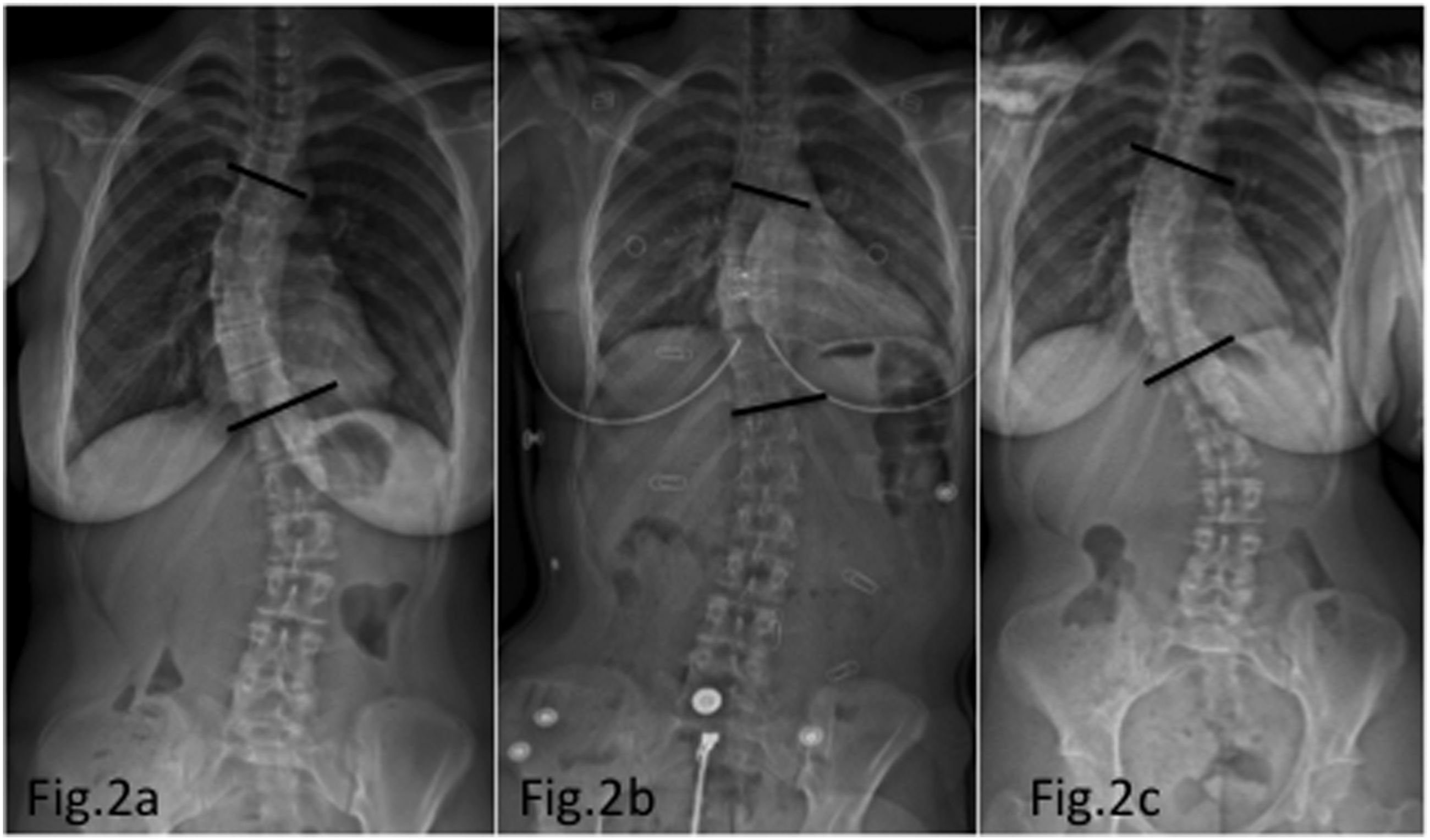
Follow up was subsequently performed every 6 months; in-brace standing whole spine EOS X-rays were taken every follow-up during brace therapy. Examples of successful and failed brace therapy X-ray imaging is shown in Figure 1 and Figure 2.) X-rays show example of patient with failed brace treatment before beginning of brace treatment (A), in-brace (B), as well as after brace treatment (C). The T6-T11 Cobb angle was 26°, 21° and 33°, respectively. According to SRS criteria, brace treatment was considered successful if curve progression was < 5°compared to pre-brace X-rays. X-rays show example of patient with successful brace treatment before beginning of brace treatment (A), in-brace (B), as well as after brace treatment (C). The T6-T11 Cobb angle was 45°, 27° and 47°, respectively. According to SRS criteria, brace treatment was considered successful if curve progression was <5° compared to pre-brace X-rays.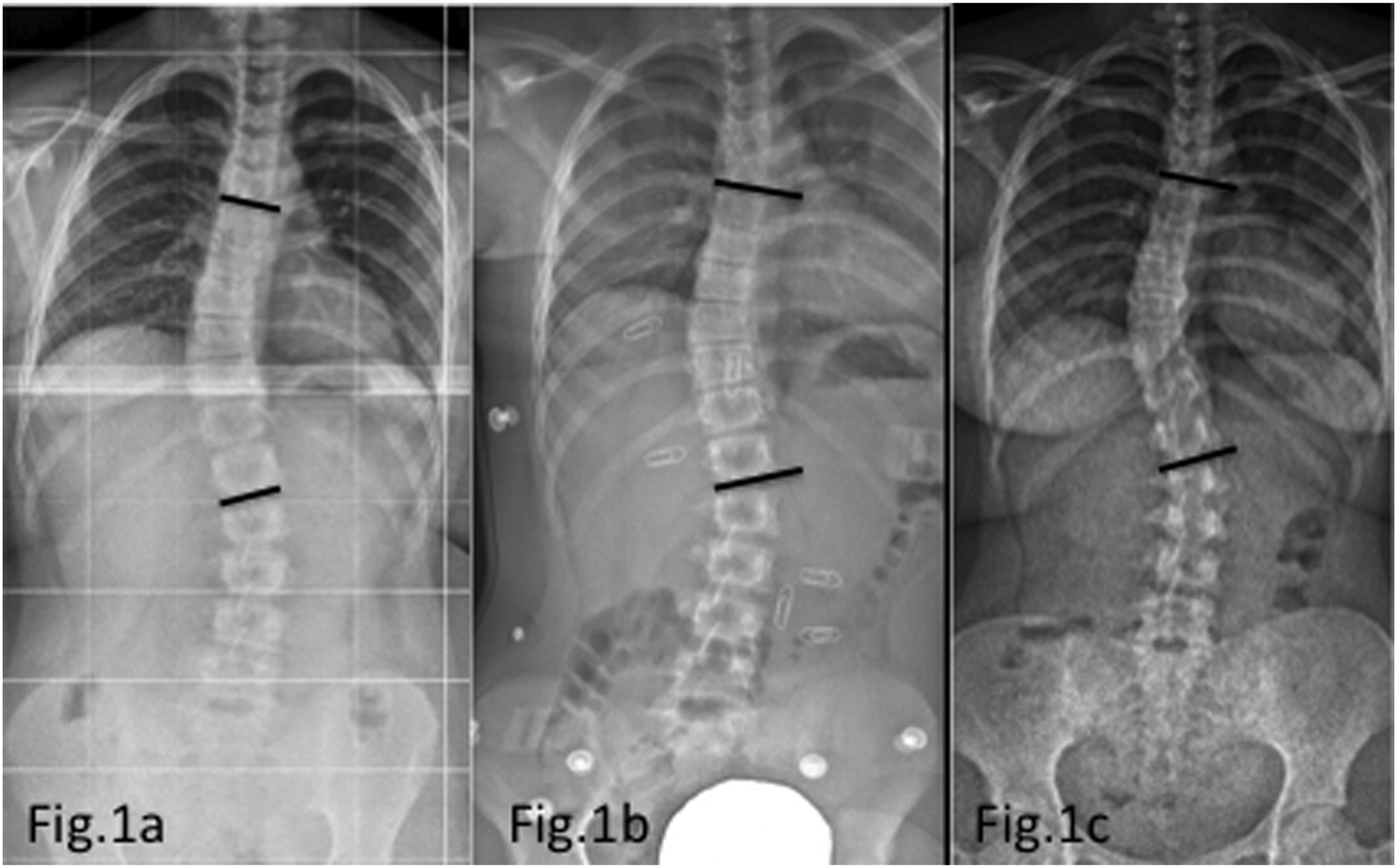
Once patients reached maturity (Risser IV-V), bracing was weaned over a period of 3-6 months. Final EOS X-rays were taken after at least 6 months without brace.
According to SRS criteria, brace treatment was considered successful if curve progression was <5° compared to pre-brace X-rays. Curve progression of >5° was considered as treatment failure. Patients were divided in a “success” group and a “failure” group based on curve progression after brace treatment.
For data analysis we measured a high thoracic, low thoracic and lumbar Cobb angle from each patient to calculate the mean Cobb angle before, during and after Chêneau brace therapy. By calculating the mean Cobb of the vertebral column, we avoided the flaw of an insufficient brace therapy that decreases the main/structural curve but increases side/non-structural curves.
Determination of Cobb angle and Nash and Moe grading was performed by 2 experienced spine surgeons. As we have demonstrated in a previous study, interobserver reliability of measurements using EOS imaging is excellent. 14 If curve measurement differed by <3°, the mean value was calculated. However, if measurement of Cobb angle differed by >3° or Nash and Moe grading differed, consensus was reached by reviewing X-rays together.
Other parameters evaluated were Risser’s sign (Grade 0-5); in-brace time per day; age at the beginning of brace therapy.
All statistics were calculated using Graph Pad Prism 6 software (GraphPad, San Diego, CA, USA). For all data, P > .05 was considered statistically significant with a 95% confidence interval. For Pearson’s Test, correlation was defined as follows: r > .7/ < −.7 strong correlation; r > .5/ < −.5 moderate correlation; r > .3/ < −.3 weak correlation; r < .3/ > −.3 no correlation)
Results
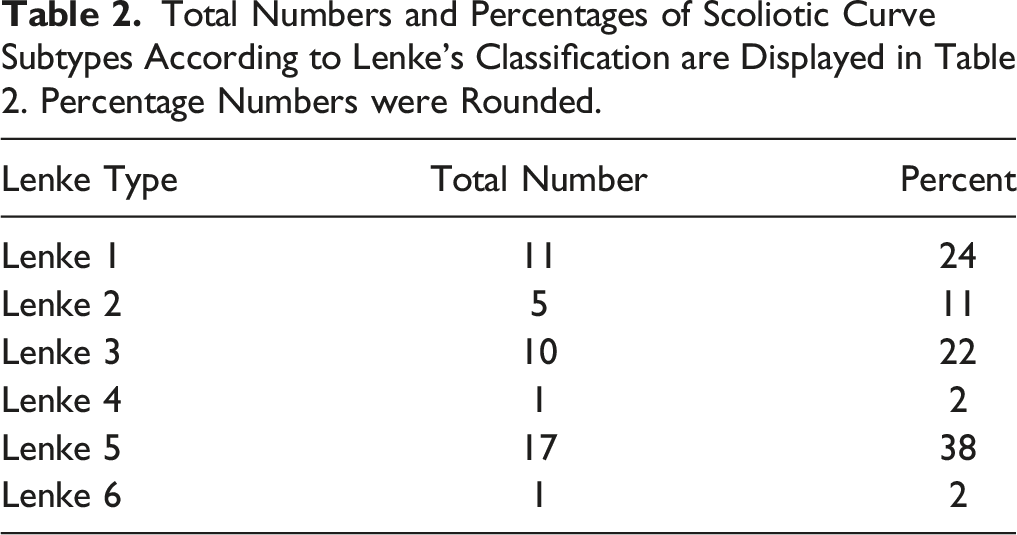
Total Numbers and Percentages of Scoliotic Curve Subtypes According to Lenke’s Classification are Displayed in Table 2. Percentage Numbers were Rounded.
AIS Patients were Divided in a “success” and a “failure” Group Based on Curve Progression After Brace Treatment According to SRS Criteria. A Value of P > .05 was Considered Statistically Significant.
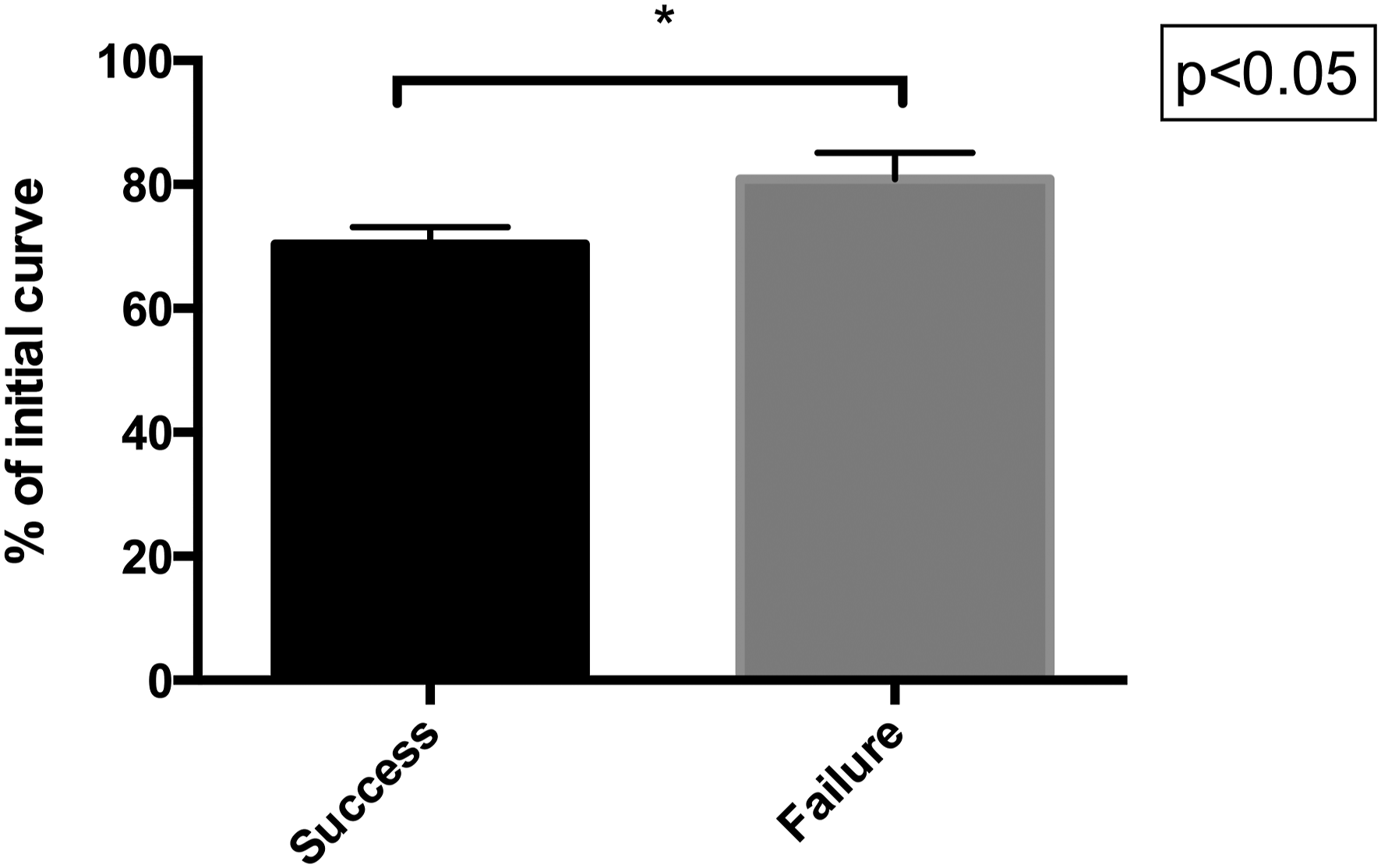
Displays the initial in-brace scoliotic curve correction as percent of initial curve in treatment success vs failure group. (70.4% ± 2.73 vs 80.9% ± 4.27 of pre-brace curve; P < .05).
Accordingly, we found the Pearson correlation coefficient of in-brace curve correction and the amount of the final curve after brace treatment to be r = .64 (P < .001) (Figure 4). Evaluating the influence of in-brace time per day on the treatment outcome, we did not find significant differences in the treatment success vs failure group. The extent of initial in-brace correction (delta Curve in brace) did correlate significantly with the outcome of the scoliotic curve after completion of brace treatment (r = 0.64; P < .001). The x-axis shows the amount of initial in-brace correction of the scoliotic curve, while the final curve is display on the y-axis as percent of the initial curve.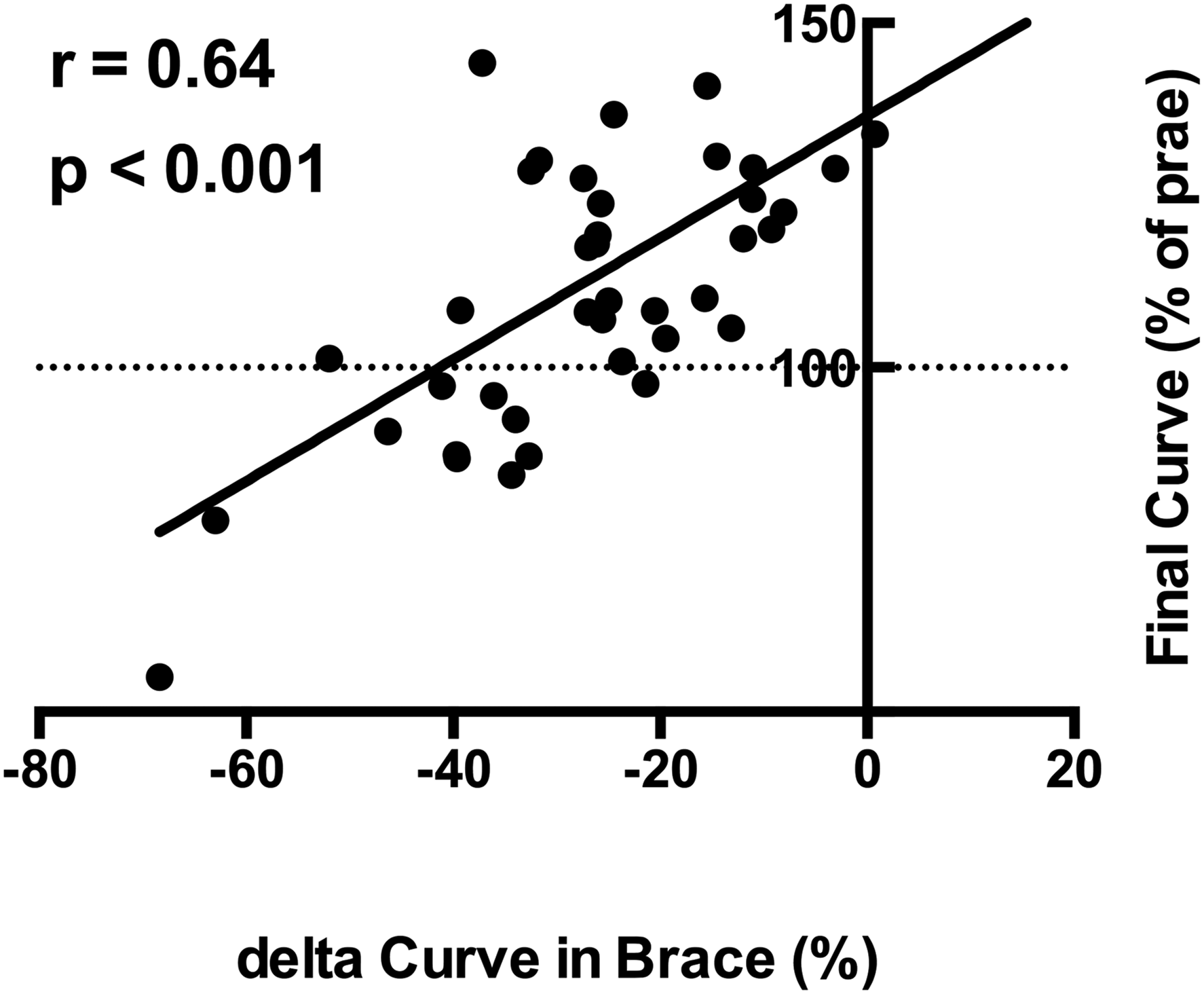
However, sub-analysis of the treatment success group revealed a correlation of high in-brace time per day with a better outcome (r = −.56 (P < .001)) Figure 5A and 5B. Pearson correlation coefficient of daily time in brace (y-axis) vs treatment outcome (x-axis) in patients with successful outcome after brace treatment (A) and treatment failure (B). While the treatment success group showed a significant correlation of high in-brace time per day with a better outcome (r = −0.56 (P < .001), we found no significant correlation in the treatment failure group.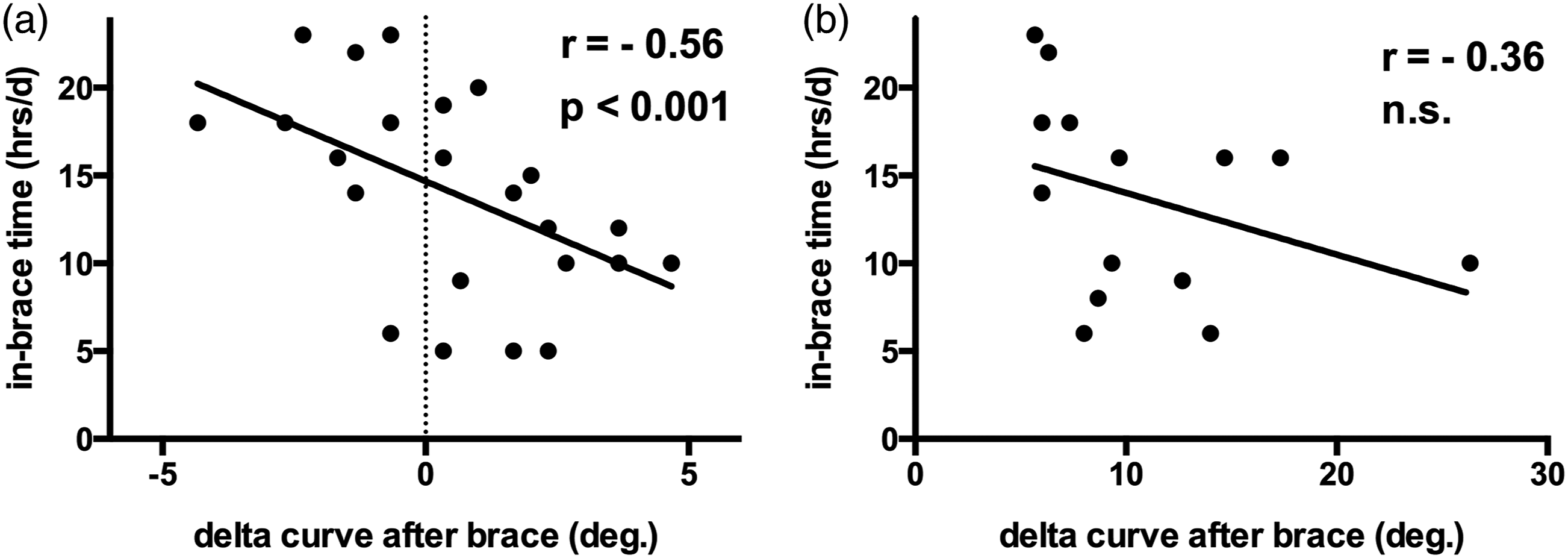
On the other hand, we found no significant correlation of in-brace time per day to curve outcome in the treatment failure group (r = −.36; n.s.).
Discussion
Rigid thoraco-lumbo-sacral orthosis (TLSO) brace treatment has been shown to be effective in changing the natural history of curve progression in patients with AIS and improve the outcome as compared to that of untreated patients.1,10,17 In Germany as well as in other European countries, the Chêneau brace is one of the most commonly used in the conservative treatment of eligible patients with AIS. Although there are several technical studies concerning Chêneau bracing,18-20 there is only a limited number of studies providing data on outcome after Chêneau bracing in patients with AIS.2,11,21 Also, due to the multitude of TLSO braces available and diversity of therapeutic regimes, little data is available concerning predictive parameter of successful Chêneau brace treatment.
Therefore, it is still not fully understood why some patients experience relevant curve progression despite of adequate brace treatment. For these non-responding patients, growth preserving surgical techniques have increasingly become an alternative. While some growth preserving techniques are still experimental, growing magnetic rod system were shown to be safe and effective.7,22,23 In order to achieve optimal postoperative results, surgical therapy should be offered to brace non-responsive patients as early as possible. Ideally, predictive parameters will help surgeons, patients and relatives to base their therapeutic decisions on objective parameters.
The main goals of our study were (1) to evaluate results of Chêneau brace therapy with existing data and (2) define predictive parameters for failure of brace therapy in patients with AIS. In our patient collective, we found that Chêneau brace treatment successfully prevented scoliotic curve progression in 69%. This is comparable to the success rates found by previous studies. Interestingly, study groups who looked at the treatment success rate using the Milwaukee brace found success rates only slightly above 50%,24,25 while other groups evaluating the Rigo System Chêneau (RSC-) brace found treatment success rates of 75% and more.11,21 In contrast to other studies, 26 we did not find that Lenke curve type had any significant influence on the brace treatment outcome. However, our number of patients included might not be sufficient to detect small differences in the outcome. Concerning predictive parameters for brace treatment outcome, our data also supports previous findings that scoliosis onset at early age/Risser’s sign as well as lack of sufficient in-brace curve correction are risk factors for brace treatment failure. 2 In our collective of patients, we found that a higher level of initial in-brace curve correction was significantly correlated with a successful outcome of brace therapy. Based on our results, we found the initial in-brace correction of the scoliotic curve to be the most valid single predictive parameter for therapy success or failure. This is in concurrence with results of other studies.2,3,17 For example, Landauer et al 27 did show that good compliance and sufficient initial in-brace correction were of significant impact for the outcome. However, Landauer et al only included patients with a right thoracic scoliosis. Also, compliance of the patients was examined by a subjective score, but not objectively quantified.
Other studies have already shown that sufficient in-brace time per day is crucial for a successful brace therapy outcome.2,3,27 Interestingly, we found that only patients with successful brace treatment outcome show a positive correlation with in-brace time per day. Conversely, we did not find the same correlation in patients with brace treatment failure. These different findings might be due to the fact that in-brace time was measured objectively, while other studies rely on data based on subjective patients indication.
Our findings implicate that patients who do not show sufficient initial in-brace correction might not benefit from simply increasing daily in-brace time but rather should consider early growth preserving surgery.
Naturally, our study has certain limitations: first, the number of included individuals is limited. Also, we did not evaluate the influence of body habitus on brace therapy outcome.
Despite these limitations, our study is one of few to evaluate the outcome of Chêneau braces in patients with AIS and also define predictive parameters to estimate brace treatment success early on. Furthermore, inclusion criteria of our study were based on criteria defined by the SRS. The data presented in this study will help to differentiate patients who are likely to benefit from adequate bracing therapy from those who could rather benefit from early surgical treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.