
Abstract
Study Design
Retrospective.
Objective
To evaluate the association between mechanical instability and neurological deficit in spinal tuberculosis (TB), and compare it against previously recognized radiological parameters.
Methods
Clinical and radiological data of patients with active thoracic spinal TB were evaluated. Instability was assessed using the Spinal Tuberculosis Instability Scoring System (STISS) by Rajasekaran et al. Neurological status and radiological parameters were analysed to identify the factors associated with neurological deficit.
Results
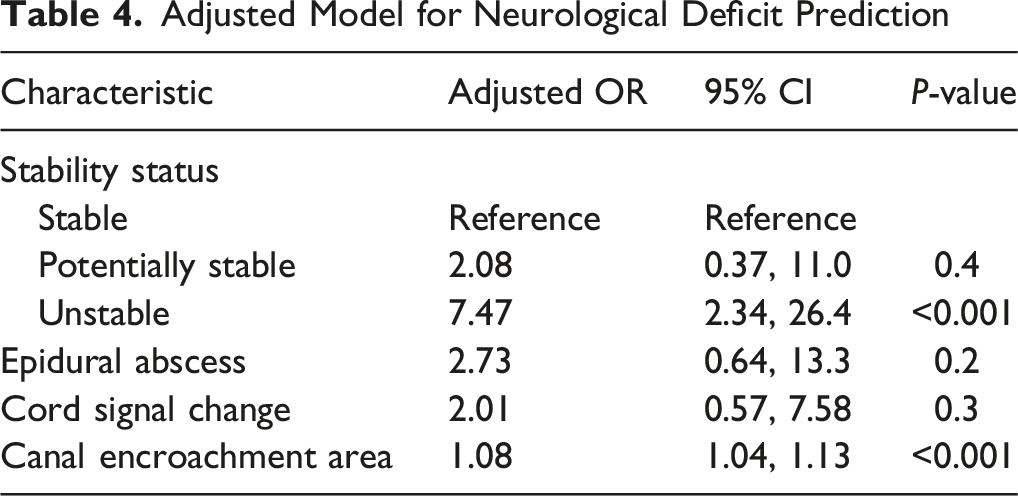
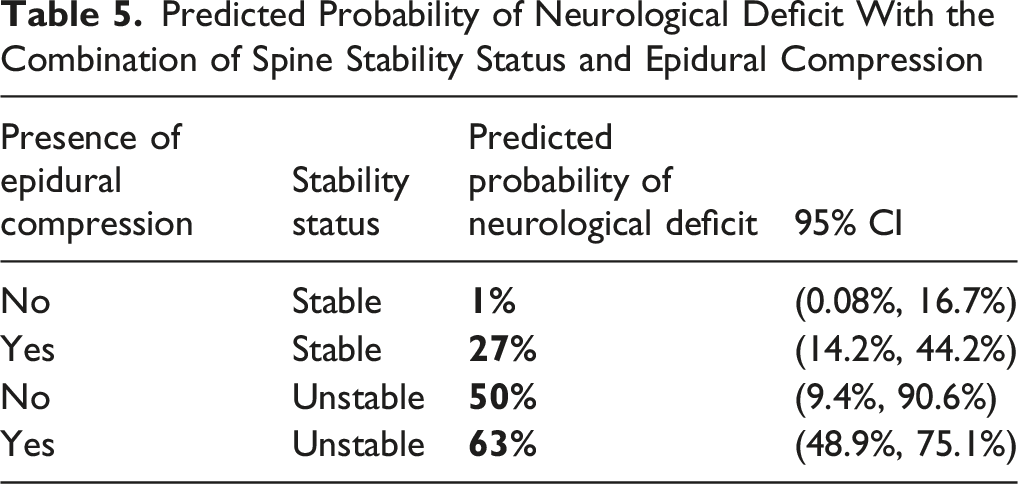
A total of 122 patients were included. The average age was 51 ± 18 years, and 54.9% were males. 40 (32.8%) patients had neurological deficits at presentation. Based on the STISS, 71 (58%) patients were categorised as stable, 10 (8.2%) as potentially unstable, and 41 (34%) as definitely unstable. On MRI, cord signal changes and epidural compression were noted in 18% and 64% of the patients, respectively. Definite instability was found to be the strongest independent association of neurological deficit (OR 9.77, 95% CI 2.85-38.9, P < 0.001), followed by greater canal encroachment area (CEA) (OR 1.08, 95% CI 1.03-1.13, P = 0.002). In a stable spine with epidural compression, the predicted probability of neurological deficit is 27%. In an unstable spine, the likelihood of neurological deficit is 50% even without epidural compression, and highest (63%) when instability was associated with epidural compression.
Conclusion
Mechanical instability is the strongest independent association of neurological deficit in spinal TB, even in the absence of epidural compression. Incorporating the Spine Instability Scoring System into routine clinical evaluation improves risk stratification, enables timely decision-making, and can prevent irreversible neurological deficits.
Keywords
Introduction
Spinal Tuberculosis (TB) remains a major global health concern. According to the 2024 World Health Organization (WHO) report, an estimated 10.8 million people developed TB worldwide. 1 The spine is the most commonly affected region in musculoskeletal TB, accounting for about 70%. 2 Delay in the diagnosis or management of spinal TB can result in significant long-term morbidity. Among these complications, neurological deficit is the most serious, occurring in nearly one-third of patients3-5 and often dictating prognosis and treatment strategy. The causes of neurological deficit differ between active and healed disease.5-7 In active spinal TB, neurological deficits typically result from compression by granulation tissue, epidural abscesses, or sequestrated bone fragments exerting a mass effect on the spinal cord. Additional mechanisms include instability, vascular compromise, cord edema, deformity, and inflammatory response.8-10
While canal encroachment, kyphotic deformity, and cord signal changes are well-recognized predictors of neurological deficits in spinal TB,11-14 the role of instability in spinal TB has been overlooked. In trauma and malignancy of the spine, instability is well-defined through systems such as the Thoracolumbar Injury Classification and Severity Score (TLICS) 15 and the Spinal Instability Neoplastic Score (SINS), 16 which highlights that instability alone, even without significant canal compromise, may predispose to neurological injury. In trauma, the presence of a neurological deficit is considered a marker of instability, even in the absence of radiological evidence of bony instability.
In spinal TB with Neurological deficit, most studies in the literature focus on radiological canal compromise and deformity, with little attention to instability. The role of instability is under-recognized until the recent development of the Spinal Tuberculosis Instability Scoring System (STISS), a structured scoring system for evaluating instability. 17 Although it provides a structured framework to assist clinicians in deciding when surgery is needed, the role of instability as an independent cause or predictor of neurological deficit has not been thoroughly studied.
This study aims to address this gap by evaluating the association between mechanical instability and neurological deficit in spinal TB and comparing its relative strength of association against previously recognized radiological parameters.
Materials and Methods
Study Design, Setting, and Population
We conducted a retrospective cohort study by including patients with active thoracic spinal TB treated at a tertiary-level spine care centre in India between 2018 and 2024. Written informed consent is not applicable as the study design is retrospective, and we used the anonymised clinical and imaging information of the patient records to analyse the data. Hence, we obtained waiver of consent from the Institutional Review Board (IRB/19/2025). Patients with microbiologically or histopathologically proven thoracic spinal TB with complete clinical and radiological data were included. Patients with spinal instability unrelated to tuberculosis and incomplete data were excluded (Figure 1). Patients with Frankel grades A, B, C, and D were categorized as having neurological deficits, whereas those with Frankel grade E were considered neurologically intact.
18
The neurological status was assessed at the time of presentation to the hospital. Flow diagram of patient selection
Data Abstraction Process
Patient demographic details, clinical history, and treatment information were retrieved from the hospital’s electronic medical record system. Radiological images were obtained from the Picture Archiving and Communication System (PACS). All datasets were linked using a unique hospital identifier.
The level of involvement was divided into proximal (C7-T1 junction, T1-T4), middle (T5-T8), and distal (T9-T12, T12-L1 junction) segments. Variables extracted from the dataset include age, sex, neurological deficit status, vertebral body loss, kyphotic deformity in single vertebra involvement or deformity angular ratio in ≥2 motion segment involvement, presence of spine at risk signs, cord signal change, cross-sectional area of cord at various levels, presence of epidural compression, and canal encroachment area (CEA).
Measurements
Anterior vertebral body loss by Rajasekaran et al
19
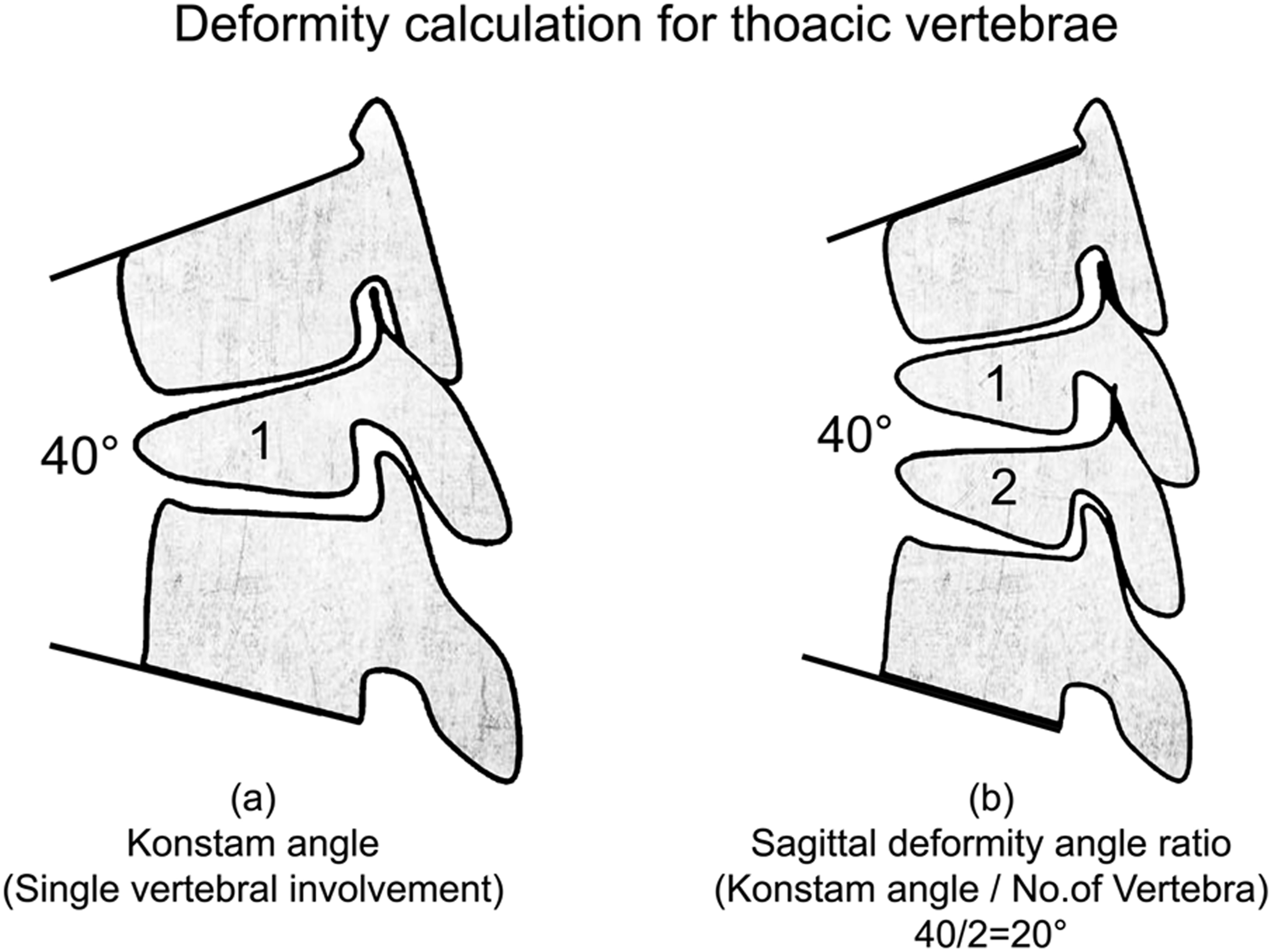
(Figure 2) and kyphotic deformity using the Konstam angle
20
were calculated. Sagittal deformity angle ratio (DAR) was calculated by dividing the Konstam angle by the number of involved vertebrae in the case of multilevel involvement
21
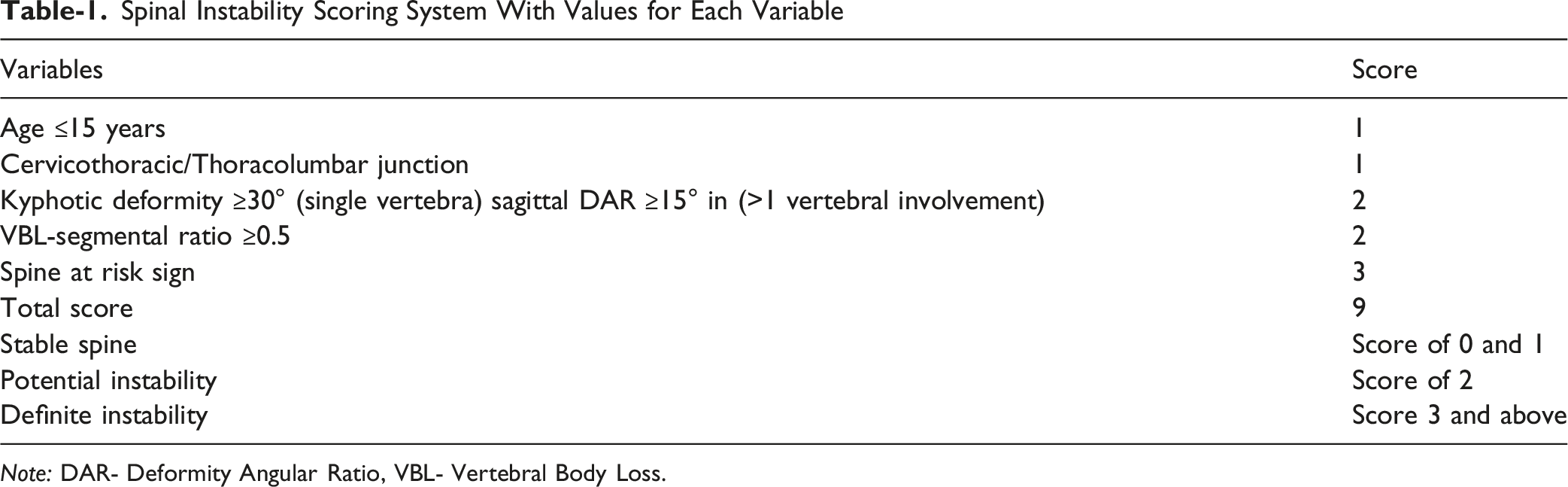
(Figure 3). The stability status of the spine was calculated using the STISS proposed by Rajasekaran et al.
17
and was classified as Stable (score of 0 or 1), Potential Instability (score of 2), and Definite Instability (score of 3 or above) (Table 1). The cord’s cross-sectional area (CSA) was measured at the level of maximum compression and at one level above and one level below. The space available for the spinal cord (SAC) was calculated by subtracting the sagittal cord diameter from the corresponding sagittal canal diameter at the diseased segment and at one level above and below.
22
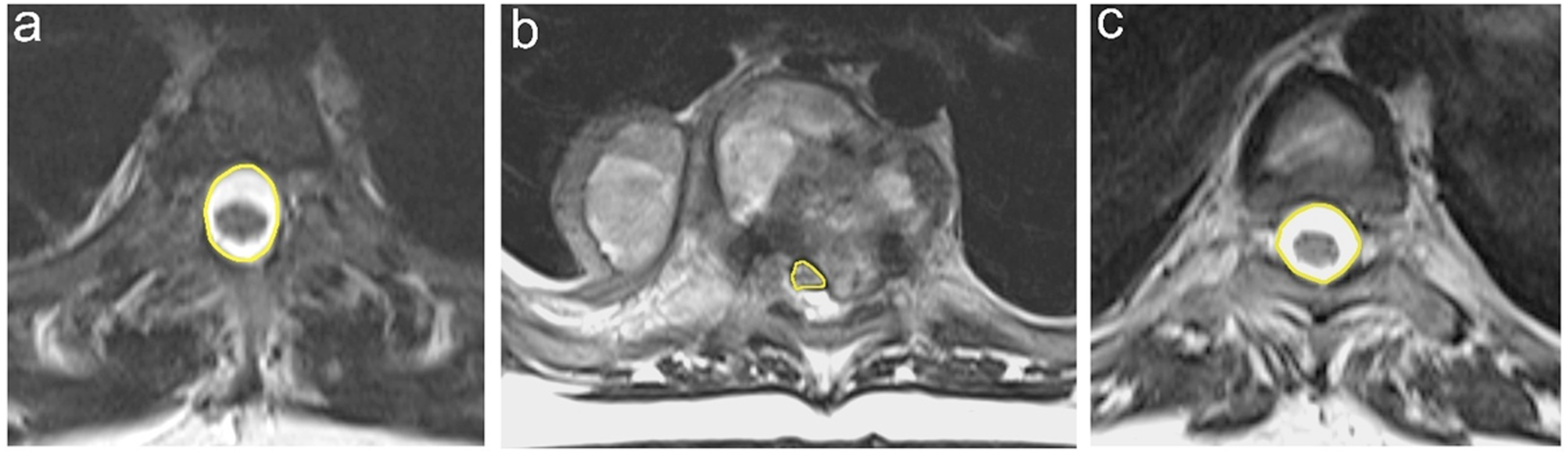
CEA was calculated on the axial MRI images (Figure 4). Epidural compression was recorded if MRI showed any epidural abscess or granulation tissue compressing the spinal cord based on the Epidural Spinal Cord Compression (ESCC) Scale with grades ≥2.
23
Calculation of VBL, the Vertebral body height is divided into ten equal fractions, and VBL was measured as the number of fractions lost. In the case of multiple vertebral Involvements, the sum of each vertebral loss will be mentioned as Total Vertebral Body Loss (TVBL). The TVBL-segmental ratio is calculated by dividing TVBL by the number of segments involved Deformity was assessed using (A) Konstam angle in case of involvement of a single vertebra, (B) the sagittal deformity angle ratio was used in multiple vertebrae involvement Spinal Instability Scoring System With Values for Each Variable Note: DAR- Deformity Angular Ratio, VBL- Vertebral Body Loss. Measurement of Canal Encroachment Area (CEA). (A) The cross-sectional area of the canal is one level above the site of maximum compression. (B) The area occupied by the spinal cord at maximum compression. (C) The cross-sectional area of the canal is one level below the site of maximum compression. Average canal area (D) was calculated as the mean of the canal areas one level above (A) and one level below (C) the diseased segment, ie, D = (A + C)/2. The percentage of canal encroachment was calculated using the formula: (D − B)/D × 100, where B represents the spinal cord area at the site of maximum compression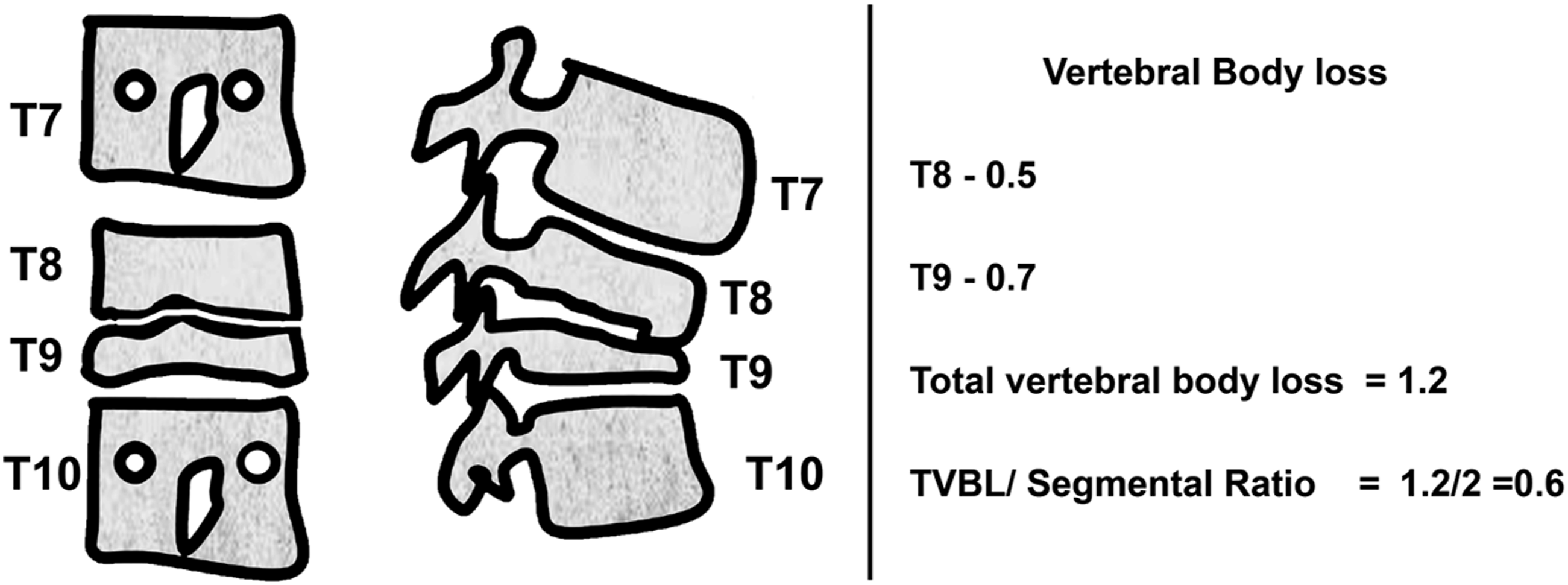
Statistical Analysis
We summarised qualitative variables as proportions with 95% confidence intervals (CIs) and quantitative variables as means with standard deviations. We used an unpaired t-test to compare quantitative variables and a chi-square/Fisher’s exact test to compare qualitative variables between two groups divided by neurological deficit status. Univariate and multivariate logistic regression were used to estimate the odds ratio (OR). Variables in the adjusted model were chosen based on the review of previously established confounders. A P-value of <0.05 was considered statistically significant. Stability status is calculated based on parameters including the presence of a spine at risk sign, vertebral body loss, kyphotic deformity, junctional involvement, and age. Epidural compression is calculated by incorporating parameter values such as CSA and SAC parameters. Hence, to prevent correlation and similarity in prediction between the independent variables, we included only stability status, epidural compression, cord signal change, and canal encroachment area in the multivariate model. To explore the interaction of mechanical instability and epidural compression contributing to neurological deficit in spinal tuberculosis, we used a Firth’s penalized logistic regression model to address smaller sample sizes. As this was a retrospective study, a pre-study sample size calculation was not performed. However, to assess the adequacy of the sample, we conducted a post-hoc power analysis with 71 exposed participants (stable spine) and 51 non-exposed participants (potentially unstable or unstable). Using a two-sided confidence level of 95%, the calculated statistical power was 99.92%, indicating that the study had adequate power to detect the observed difference between the groups. Data analysis was conducted in R software version 4.5.1.
Results
Comparison of Characteristics by Neurological Deficit Among Those Diagnosed With Thoracic Spinal Tuberculosis
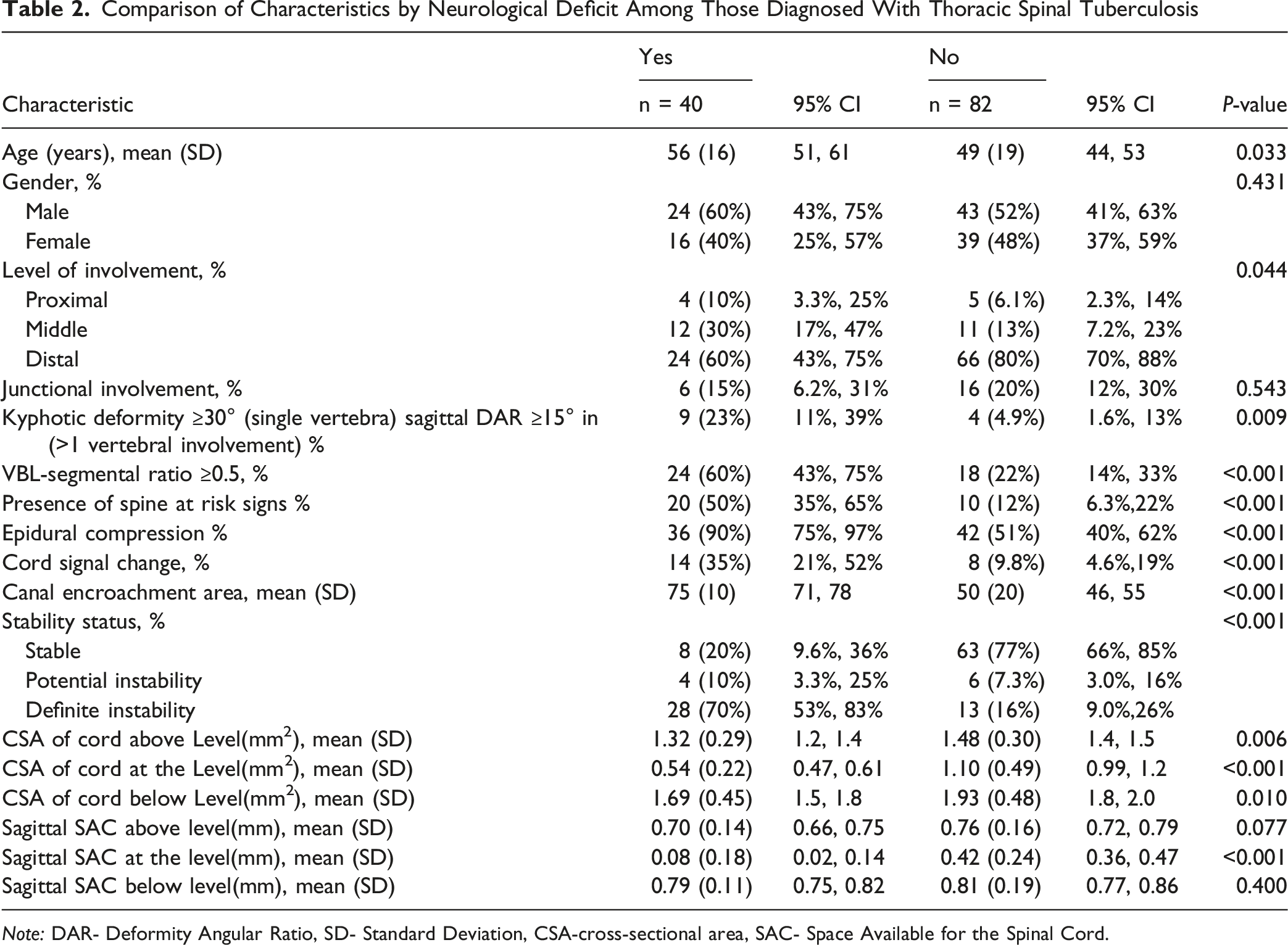
Note: DAR- Deformity Angular Ratio, SD- Standard Deviation, CSA-cross-sectional area, SAC- Space Available for the Spinal Cord.
Univariate Logistic Regression Analysis for Neurological Deficit
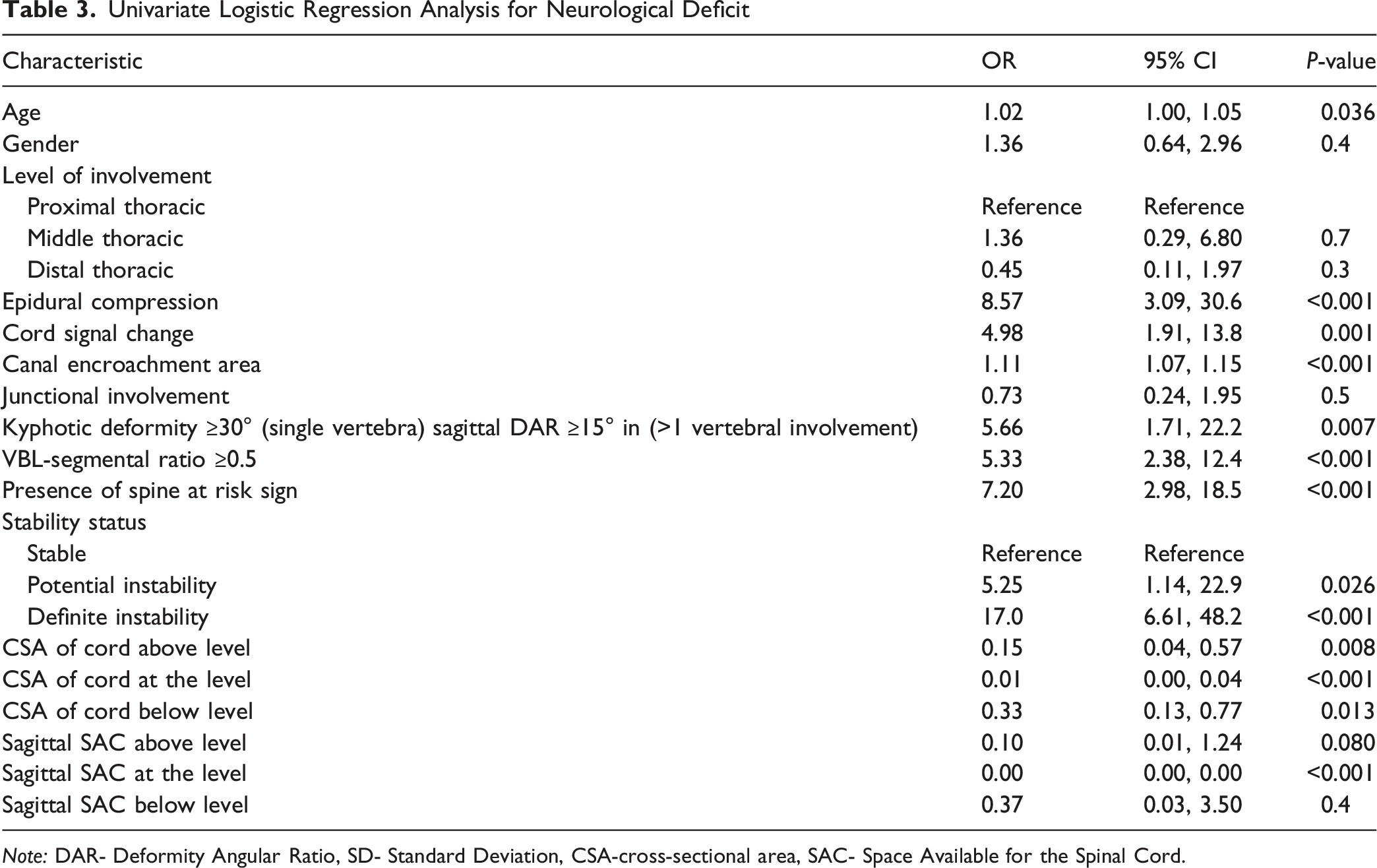
Note: DAR- Deformity Angular Ratio, SD- Standard Deviation, CSA-cross-sectional area, SAC- Space Available for the Spinal Cord.
Adjusted Model for Neurological Deficit Prediction
Predicted Probability of Neurological Deficit With the Combination of Spine Stability Status and Epidural Compression
Discussion
Spinal tuberculosis remains a major global health problem. The clinical presentation of spinal TB varies widely based on factors such as age, severity, duration, affected region, and the presence of complications like abscesses, deformities, instability, and neurological deficits. Among these, neurological impairment is the most severe complication of spinal TB. Over the decades, factors like canal compromise, epidural abscess, cord signal changes, and kyphosis have been identified as key predictors of neurological deficits in spinal TB.13,14,24,25 The importance of mechanical instability as a cause of neurological decline has been overlooked.
Role of Instability in Spinal TB
The mechanisms underlying neurological impairment in pyogenic (PSI) and tubercular spondylodiscitis differ in several key aspects. In PSI, even a minimal epidural abscess can cause early and severe neurological impairment. This is because pyogenic infections trigger intense acute inflammation, leading to oedema and rapidly expanding epidural collections. Several mechanisms, such as epidural collection exerting pressure on the cord, septic emboli affecting arteries, and ischemic injury to the spinal cord, contribute to this process. Studies show that most patients with neurological deterioration exhibit clear epidural inflammatory changes, which serve as an important predictor of neurological deficits in pyogenic spinal infections.
26
Spinal TB, by contrast, generates biologically “cold” compression, often sparing neurology despite severe destruction. In spinal TB, within this relatively low inflammatory environment, mechanical instability becomes a dominant pathogenic factor. Our study results show that instability, even without epidural compression increase the probability of neurological impairment by 50%. The progressive vertebral body destruction, posterior column involvement, and junctional disease lead to dynamic micromotion, angular collapse, and translation.17,27 Since the MRI is performed in the supine position, surgeons focus more on the epidural compression and deformity, while overlooking functional instability. Figures 5-7 highlight stability as a key differentiator of neurological status. Severe static compression was tolerated in stable spines, whereas dynamic instability caused deficits despite preserved canal dimensions. (A) Lateral X-ray and (B) T2-weighted mid-sagittal MRI of a 47-year-old male presented with neurological deficit. The white arrow in (B) highlights the area of pathology and kyphosis. (C) CT scan reveals significant Vertebral Body Loss (VBL). (D) Axial T2 MRI confirms a relatively preserved canal and no intrinsic cord signal changes. STISS score for this patient was 4 (Kyphotic deformity - 2 + VBL score 2)- definite instability (A) Lateral X-ray and (B) T2-weighted mid-sagittal MRI of a 26-year-old male presented with neurological deficit. (C, D, E): Axial T2-weighted images demonstrate the presence of posterior epidural fat and preserved CSF flow. The calculated STISS score for this patient was 6, indicating definite instability (A) Lateral X-ray and (B) T2-weighted mid-sagittal MRI of a 47-year-old female presented with normal neurology. (C, D): Axial T2-weighted images demonstrate significant cord compression by epidural abscess. The STISS score for this patient was zero, indicating a mechanically stable spine


Comparison With Previous Studies
Comparison of Studies in Literature Predicting Neurological Deficit in TB Spine
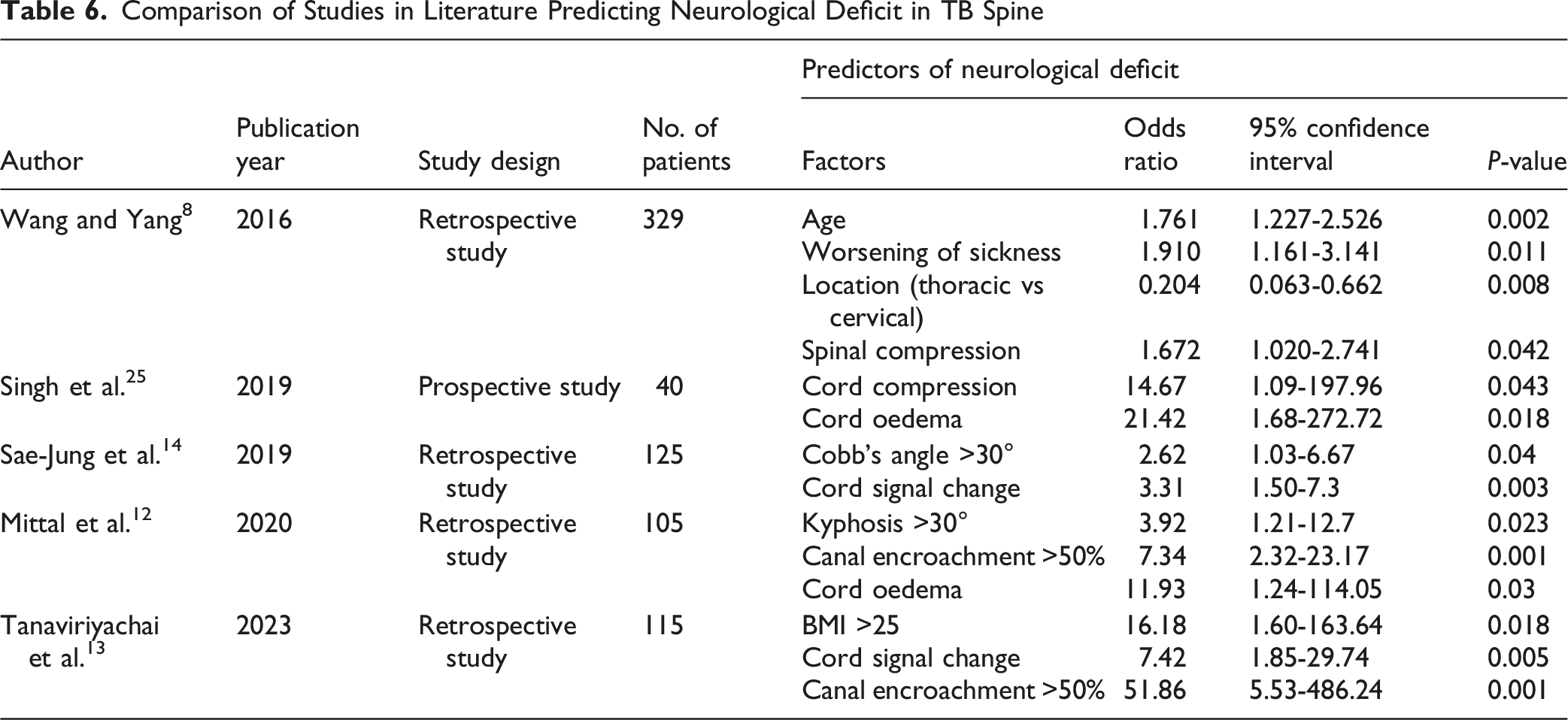
Spinal Tuberculosis Instability Score by Rajasekaran et al 17 was selected as the primary metric to quantify instability because it is the first validated, objective, and disease-specific scoring system for spinal tuberculosis. It incorporates parameters unique to TB pathology, including severity of kyphosis, vertebral body loss, junctional involvement, age, and posterior column failure. By utilizing this scoring system, our predictive analysis minimizes subjective variation in interpreting instability and provides a quantitative, repeatable framework for correlating mechanical failure with neurological outcome. This ensured that our findings were not only statistically robust but also clinically meaningful, particularly in early or subtle disease, where traditional radiological markers may underestimate biomechanical compromise.
Pathophysiological Basis
In spinal TB, vertebral body loss leads to progressive failure of both anterior and posterior columns, especially at junctional levels. Dynamic instability causes micromotion at the affected level. It can stretch or kink the spinal cord, disturb vascular supply, or disrupt cord alignment.28,29 These dynamic effects may cause neurological deficit even in the absence of significant canal encroachment or cord signal change. Importantly, dynamic instability can result in repetitive or sudden translation of the spinal cord; even a small degree of translation may precipitate severe neurological compromise in the thoracic spine, where the canal is already narrow and has limited reserve (Figure 8). Thus, relatively minor translation can have catastrophic consequences. A simplified basic geometric concept (Figure 9) is used to illustrate how a small degree of translation may disproportionately reduce the effective canal area.
30
Similar biomechanical mechanisms have been suggested in neoplastic spine conditions. Jung et al. noted that even in patients without high-grade compression, mechanical instability contributed to early-onset deficits, underscoring that dynamic factors may play a greater role than static imaging suggests.
31
(A) demonstrates the progressive collapse of vertebral bodies in chronic spinal tuberculosis, resulting in the formation of a gibbus deformity and stretching of the spinal cord at the apex of the angular kyphosis. In contrast, the (B) (Coronal) and (C) (Axial image) illustrate that in acute spinal TB, even a subtle displacement due to spinal instability can lead to significant canal stenosis, thereby precipitating early neurological deficit A Venn diagram represents the spinal canal as two overlapping circles (radius r). The blue circle represents the static canal, while the red circle represents the shifting vertebra. The shaded “lens” area represents the effective space available for the cord (SAC), dependent on the translation distance (d)

Clinical Implications
Our study uniquely incorporates instability into both unadjusted and adjusted multivariate models, providing the first evidence of radiologically quantified instability as the strongest independent association of neurodeficit in active thoracic Spinal TB. Patients with definite instability have an approximately 50% likelihood of neurological deficit even without epidural compression, indicating that waiting for compression or overt neurological signs may be unsafe. Early surgical stabilisation may help these patients to avoid irreversible cord damage. On the other hand, surgery may be reserved for patients with severe compression or deteriorating neurological symptoms in patients with a stable spine. Thus, incorporating the STISS into clinical decision-making offers a methodical, scientifically based approach to surgical planning and patient selection, while retaining conservative treatment when necessary.
In metastatic spine disease, the early stabilisation principle is well-established; to prevent neurological deterioration,32,33 unstable SINS or high-grade ESCC lesions warrant surgical consideration. Our results extend this reasoning to spinal tuberculosis, indicating that neurological risk in both infectious and neoplastic pathologies may be predicted by comparable biomechanical instability. Hence, in addition to assessment and investigations of common factors, we recommend evaluating spinal instability during the course of spine TB to prevent neurological deficits.
Since the present study is a retrospective, single-center analysis, generalizability is limited. In addition, the long-term neurological and functional follow-up parameters were not accounted for in the analysis.
Conclusion
Our study emphasizes that spinal instability is a strong and independent association of neurological deficits in spinal TB. Including an instability score in routine clinical practice provides a reliable, practical way to identify high-risk patients early. Timely stabilization of an unstable spine, even without epidural compression, can prevent neurological injury.
Footnotes
ORCID iDs
Consent to Participate
Written informed consent is not applicable as the study design is retrospective and we used the anonymised clinical and imaging information of the patient records to analyse the data. Hence, we obtained waiver of consent from the Institutional Review Board (IRB/19/2025).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Ganga Orthopaedic Research and Education Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.