
Abstract
Study Design:
Retrospective analysis of case series.
Objective:
The aim is to study the recovery of neurological deficit in pediatric spinal tuberculosis cases presenting to us more than 6 months after onset of motor weakness in lower limbs.
Methods:
This is a retrospective analysis of 13 consecutive patients of pediatric spinal tuberculosis presenting to us at least 6 months after the onset of neurologic deficit. All these patients underwent surgical intervention at our center and their neurological recovery was noted in terms of improvement in Frankel grading and spasticity improvement by modified Ashworth scale. All the patients were followed up to at least 18 months post op and final neurologic status was assessed at that time.
Results:
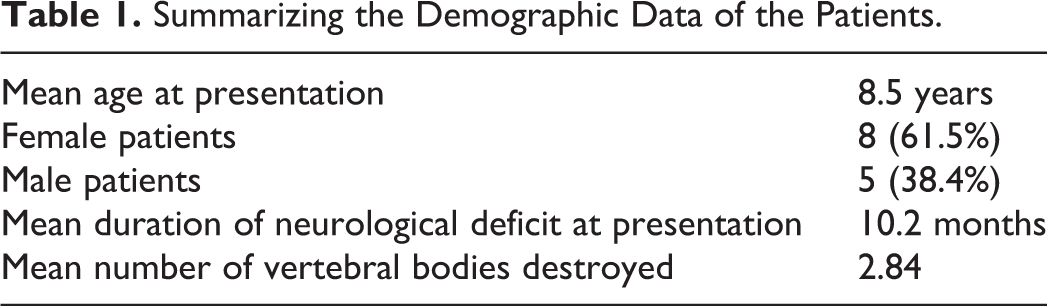
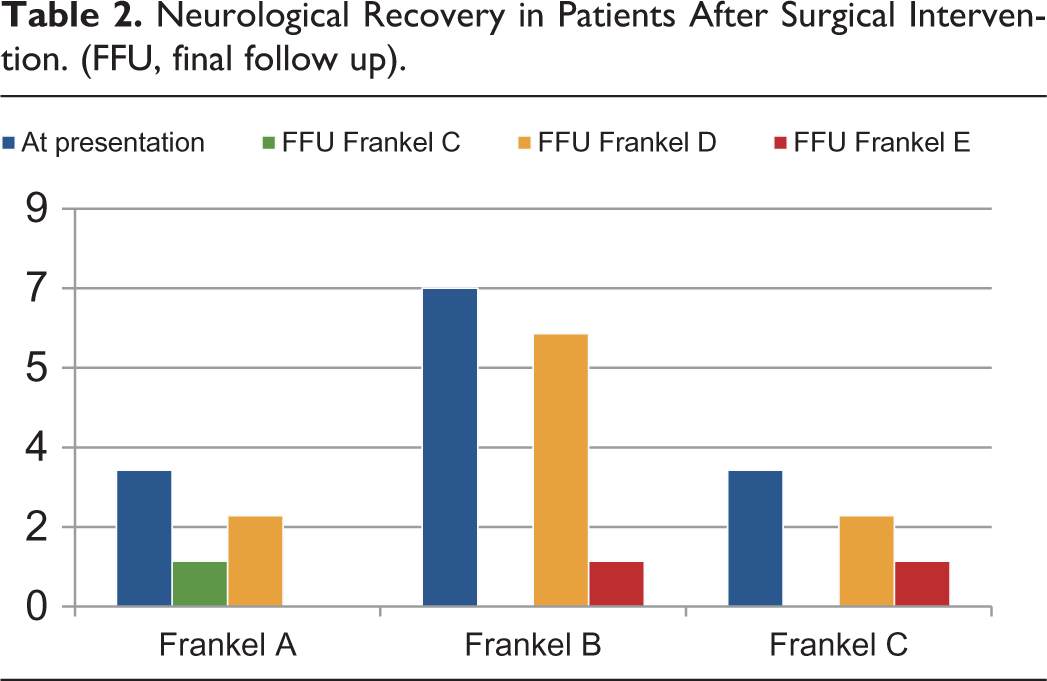
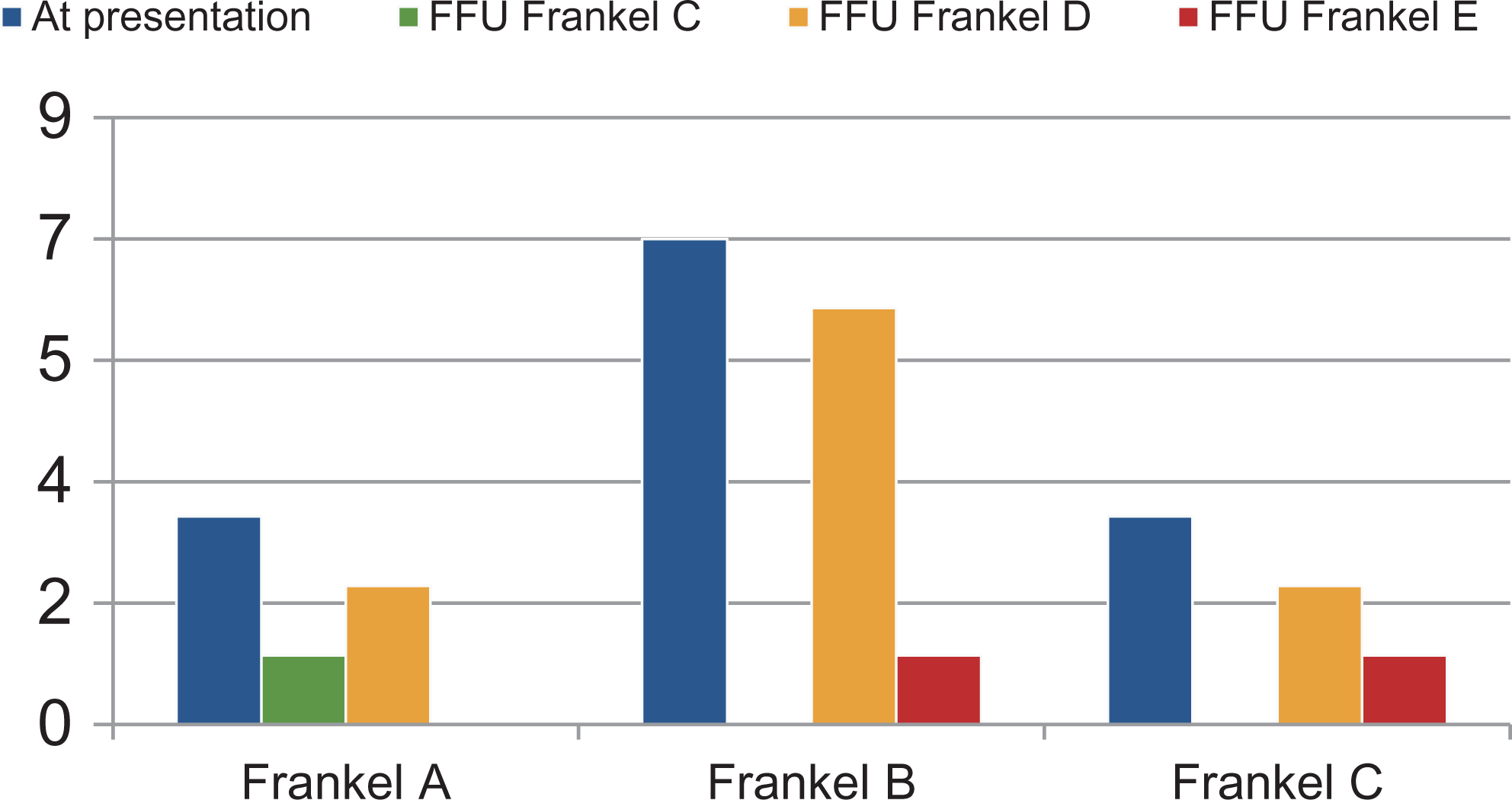
The mean age of the patients at presentation was 8.5 years. The mean duration of neurologic deficit at the time of presentation was 10.23 months (6-24 months). Seven patients had a Frankel grade B at presentation out of which 6 improved to Frankel grade D and one improved to Frankel C at final follow up. Out of the other 3 patients with Frankel A at presentation, 2 improved to Frankel grade D and 1 to Frankel grade C. The remaining 3 patients presented with Frankel grade C at presentation, 2 improved to Frankel D and one improved to Frankel E at the time of final follow up.
Conclusion:
Neurologic recovery in patients with neurological deficit is possible even in cases of long standing deficit more than 6 months and in some cases upto 24 months as shown in our study.
Keywords
Introduction
Neurological deficit among patients of spinal tuberculosis is still frequently found in the developing countries. Spinal tuberculosis is the most common extra articular manifestation of tuberculosis. 1 The most common site of spinal tuberculosis is dorsal and dorsolumbar region. Neurological deficit may range from 23-76% cases of spinal tuberculosis. 2 Patients in developing nations do have a protracted course of this disease and patients are frequently neglected in the low socioeconomic strata group. These patients may have an onset of neurological deficit and still present quite late in the course of disease. It is not uncommon for these patients to remain non ambulatory for a long period of time before approaching a clinician. Presence of extensive vertebral body destruction is common in these cases and patients often present with dense neurological deficit with variable amounts of deformity. The basic management of neurological deficit during the course of the disease is neural decompression following a short course of anti tuberculous chemotherapy. 3 Decompression surgeries are known to improve neurological recovery in patients with recent onset of neurological deficit. The effect of surgery on the neurologic recovery in patients with a long standing neurological deficit (> 6 months) is not described previously. This retrospective analysis aims to identify the effect of surgical intervention on the neurological recovery in such patients of pediatric spinal tuberculosis with long standing neurological deficit (> 6 months).
Materials & Methods
This study retrospectively analyses 13 consecutive patients of active pediatric spinal tuberculosis (age < 12 years) who presented to our institution from 2009-2017. The approval for the study was obtained from the Institutional Ethics Committee at Seth G.S Medical College & K.E.M Hospital, Mumbai (Approval number EC/39/2020). Informed consent from parents was obtained for inclusion in the study. These patients had involvement of dorsal or dorsolumbar junction of the spinal column. The data was analyzed from the departmental database. Demographic characteristics such as age and sex of the patients were noted. The duration of neurological deficit at the time of presentation was also noted. All the patients underwent standard neurological assessment by Frankel grading and modified Ashworth scale 4 was used for assessment of spasticity. This assessment was first done at the time of presentation and later periodically till the last follow up. All the patients underwent radiological intervention in the form of supine plain radiographs, computed topography(CT) scan and magnetic resonance imaging (MRI) at the time of presentation. The number of vertebral bodies involved was decided as per MRI and the kyphosis was calculated by Cobb’s method on plain radiographs. Plain radiographs were repeated at 3, 6 and 9 months of follow up. All the patients were followed up at least till 18 (18-30) months after intervention. The diagnosis of tuberculosis in these patients was made with the help of culture, antibiotic sensitivity, GeneXpert (cartridge based nucleic acid amplification technique) and histopathological examination. The culture was carried out on liquid culture medium by Mycobacterial growth indicator tube (MGIT) and antibiotic sensitivity was carried out afterward. All patients at the time of presentation were in active stage of the disease and none of these patients represented post tubercular deformity or late onset neurological deficit. All these patients underwent an initial trial of antitubercular chemotherapy (ATC) following which surgical management was planned owing to incomplete recovery of the neurological status. The ATC was continued as per institutional protocols till clinical, radiological and serological evidence of disease cessation was confirmed. The search for primary origin for the tuberculosis was carried out by clinical examination to search for stigmata of tuberculosis, sputum examination for acid fast bacilli smear and chest radiographs.
Results
All the patients had evidence of active spinal tuberculosis at the time of presentation. The mean age of the patients was 8.5 years (5-12 years) at the time of presentation. There were 8 female and 5 male patients. The mean duration of neurological deficit at presentation was 10.2 months (6-24 months). The maximum duration was that of a 5 year old female patient with neurological deficit of 24 months duration at the time of presentation. The demographic data is summarized in Table 1. Furthermore, 7 patients had a Frankel grade B at presentation, 3 had Frankel A at presentation and 3 had Frankel grade C at presentation. All these patients were non ambulatory when they presented at our institute. Similarly 10 patients had a modified Ashworth grade 3 and 3 patients had grade 2 spasticity at presentation. The mean number of vertebral body involvement was 2.84 (2-7). The maximum involvement was seen in a 5 year old female child with destruction of 7 contiguous vertebral bodies with neurological deficit of 24 months duration. The involvement of the vertebral bodies was decided on sagittal and coronal MRI images of the involved region to decide our surgical strategy as per segment salvage or sacrifice. The angle of kyphosis at the site of local deformity ranged from 36.40 to 62.20 at the time of presentation. The patients after the diagnosis of tuberculosis (9—culture positive 4—gene expert positive) were started on ATC if not already started. Three patients had already been started on empirical ATC at other centers before referring to our institution. One patient was diagnosed as multi drug resistant tuberculosis on culture and was started on ATC as per antibiotic sensitivity for 24 months as per national guidelines by consulting a chest physician. Two patients also showed a positive sputum smear for acid fast bacilli and 1 patient had a history of cervical lymphadenitis 2 years prior to presentation. An initial course of ATC was given in all patients upto 3 weeks before surgical intervention was planned. Six of these patients underwent a single incision transthoracic versatile approach and supplemented with hartshill rectangle and sublaminar wire fixation. The anterior reconstruction of the destroyed vertebrae was done with iliac crest bone graft and rib graft harvested during the exposure in these patients. Four patients were treated with hybrid fixation by posterior approach. The distal part of the construct comprised of pedicle screw system and the proximal part of the construct comprised of sublaminar wire over the rod. A single connecting rod was bent and contoured in an inverted U shape to achieve this construct. Among these 4 patients, 3 required reconstruction by iliac crest autograft and one required a fibula graft for additional reconstruction since there was an extensive destruction of vertebral bodies with a large resultant void anteriorly. The remaining 3 patients were operated with a pedicle screw and rod based system only with anterior reconstruction by locally harvested autograft. We have found anterior reconstruction to be a very important contributor of long lasting stability in these patients and hence meticulous reconstruction is mandatory.
Summarizing the Demographic Data of the Patients.
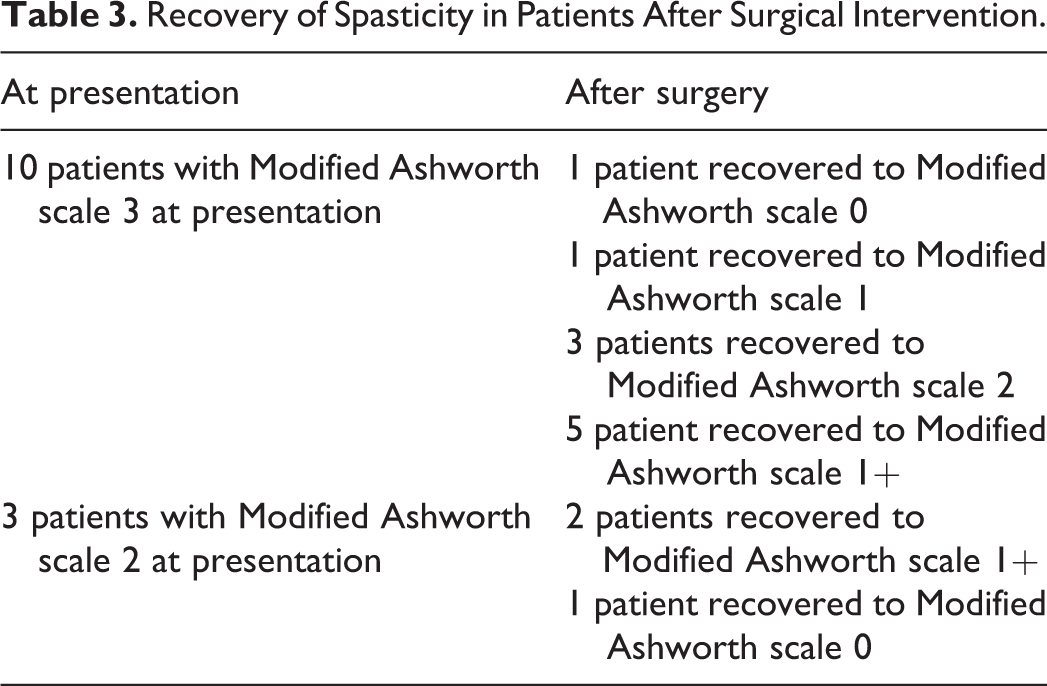
After surgery patients were kept in bed as per their neurological status and bedside sitting was allowed as soon as comfortable. A Thoraco-lumbo-sacral orthosis (TLSO) was advised for all the patients during mobilization. Out of the 7 patients with Frankel B at presentation, 6 recovered to a Frankel D and 1 to Frankel C at the final follow up. Out of the 3 patients with a Frankel A at presentation 2 recovered to a Frankel D and 1 to Frankel C at final follow up. Out of the remaining 3 patients with a Frankel grade C at presentation 1 recovered to a Frankel E and 2 recovered to Frankel grade D at final follow up (Table 2). A similar distribution for the Modified Ashworth scale is presented in Table 3. None of the patients showed a neurological worsening after the surgical intervention. Eleven out of 13 (84.6%) patients were ambulatory at the time of final follow up. The mean correction of kyphosis was achieved from 48.50 preoperatively to 4.80 (90% correction) at the time of final follow up. These patients were also found to be severely malnourished and neglected, belonging to the poor socioeconomic strata of the society. One of the patients, a 5 year old girl with D5-D11 tuberculosis. She was started on deworming therapy after consultation with the pediatrician after surgery since helminthic infestation was confirmed on investigations.
Neurological Recovery in Patients After Surgical Intervention. (FFU, final follow up).
Recovery of Spasticity in Patients After Surgical Intervention.
This 5 year old female presented to us with a history of deformity of back and and gradually progressing weakness of both lower limbs since 24 months. The child was bed bound since 24 months and was classified as Frankel grade A and Modified Ashworth scale 3 at presentation. She was started on empirical ATC elsewhere and then referred to us. We continued the drug therapy and planned for a surgical intervention. There was an extensive destruction of the vertebral bodies from D5-D11 and the spinal column had a kyphotic deformity at the apex of the lesion (Figure 1 A-D). Hybrid fixation with pedicle screw and sublaminar wire system was carried out by an all posterior approach (Figure 2 A-D). The anterior reconstruction was done with the help of autologous fibula graft through the posterior approach. The patient started showing improvement in neurological status by 3 weeks postoperatively. She started ambulation with support by 5 months post surgery and achieved a Frankel grade B at the time of final follow up along with a modified Ashworth scale of 1+. Shortly after the surgical intervention this patient was found to have simultaneous parasitic infestations for which deworming therapy was initiated following a pediatrician’s reference.

Preoperative imaging of patient in case illustration one. A) depicting plain lateral radiograph of the dorsal spine with kyphosis and destruction of vertebral bodies. B) depicting plain anteroposterior radiograph of the dorsal spine demonstrating crowding of ribs secondary to collapse of multiple vertebral bodies. C) sagittal CT scan of the dorsal spine demonstrating involvement of vertebral bodies from D5-D11 and resultant kyphosis. D) sagittal MRI of the dorsal spine depicting significant cord compression at the site of the lesion.
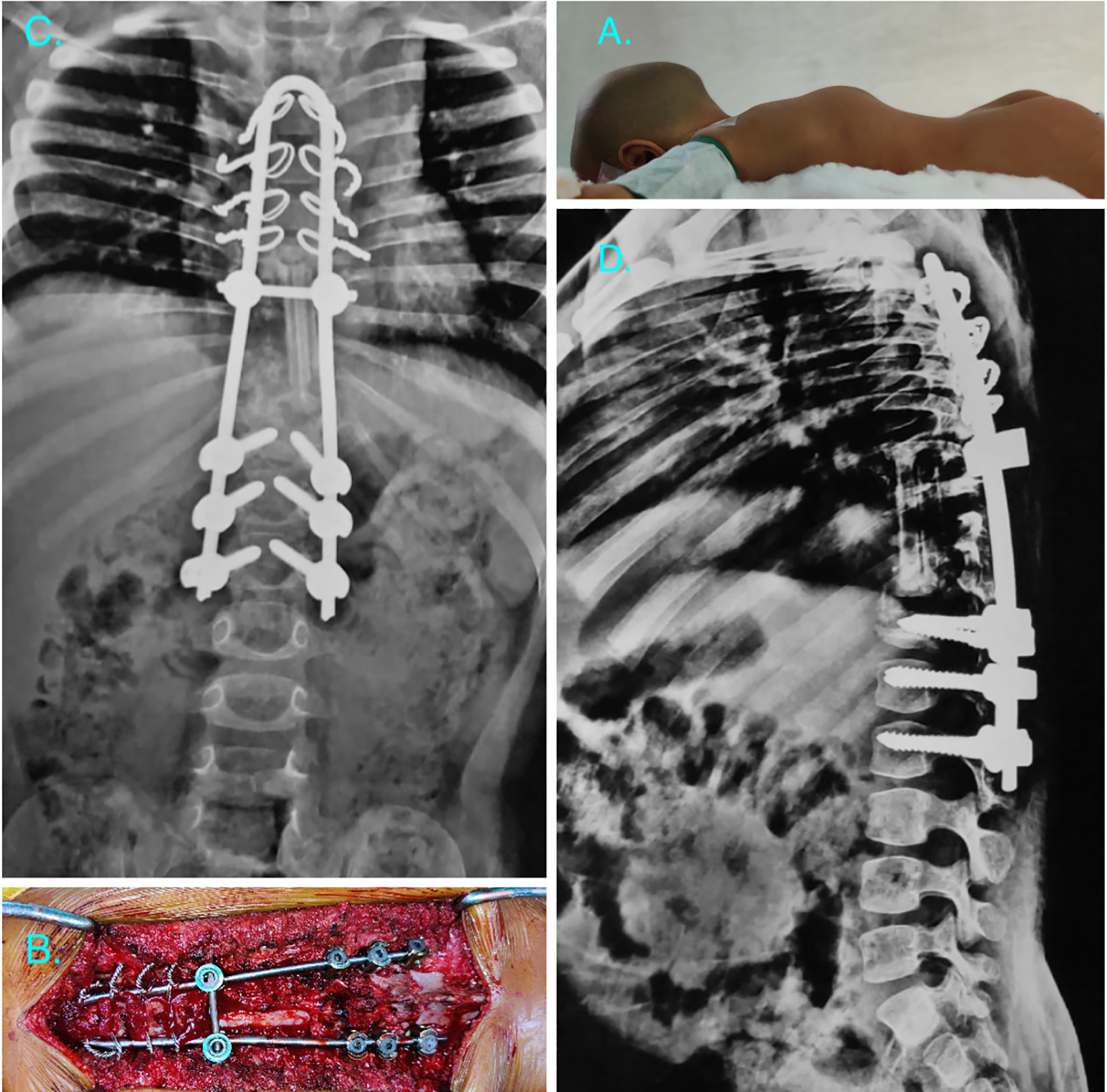
Intraoperative images and post operative radiograph of the patient in case illustration one. A) depicting the prone positioning of patient and kyphosis of the dorsal region prominent after positioning. B) intraoperative photo demonstrating final fixation with adequate decompression of spinal cord. C) plain anteroposterior radiograph of the dorsal spine showing the hybrid construct. D) plain lateral radiograph of the dorsal spine demonstrating the anterior reconstruction with fibula and adequate correction of kyphosis.
Another patient an 8 year old female with a history of paraplegia of 12 months duration was referred to our center for a suspected D7-D8 tuberculous spondylodiscitis (Figure 3 A, B, D). She presented with a Frankel grade B and a modified Ashworth scale of 3 at initial presentation. She also had a pressure sore over the sacral region at presentation (Figure 3C). We followed the similar protocol with this patient and started on ATC after a CT guided biopsy. After continuing the ATC surgical intervention was planned on similar grounds with a hybrid fixation as described in the previous case (Figure 4 A, B). The pressure sore healed by daily dressings by secondary intention. She regained movements of the lower limbs by 1 month post surgery and remained ambulatory at the final follow up with Frankel grade D and modified Ashworth scale 1 after surgical intervention.
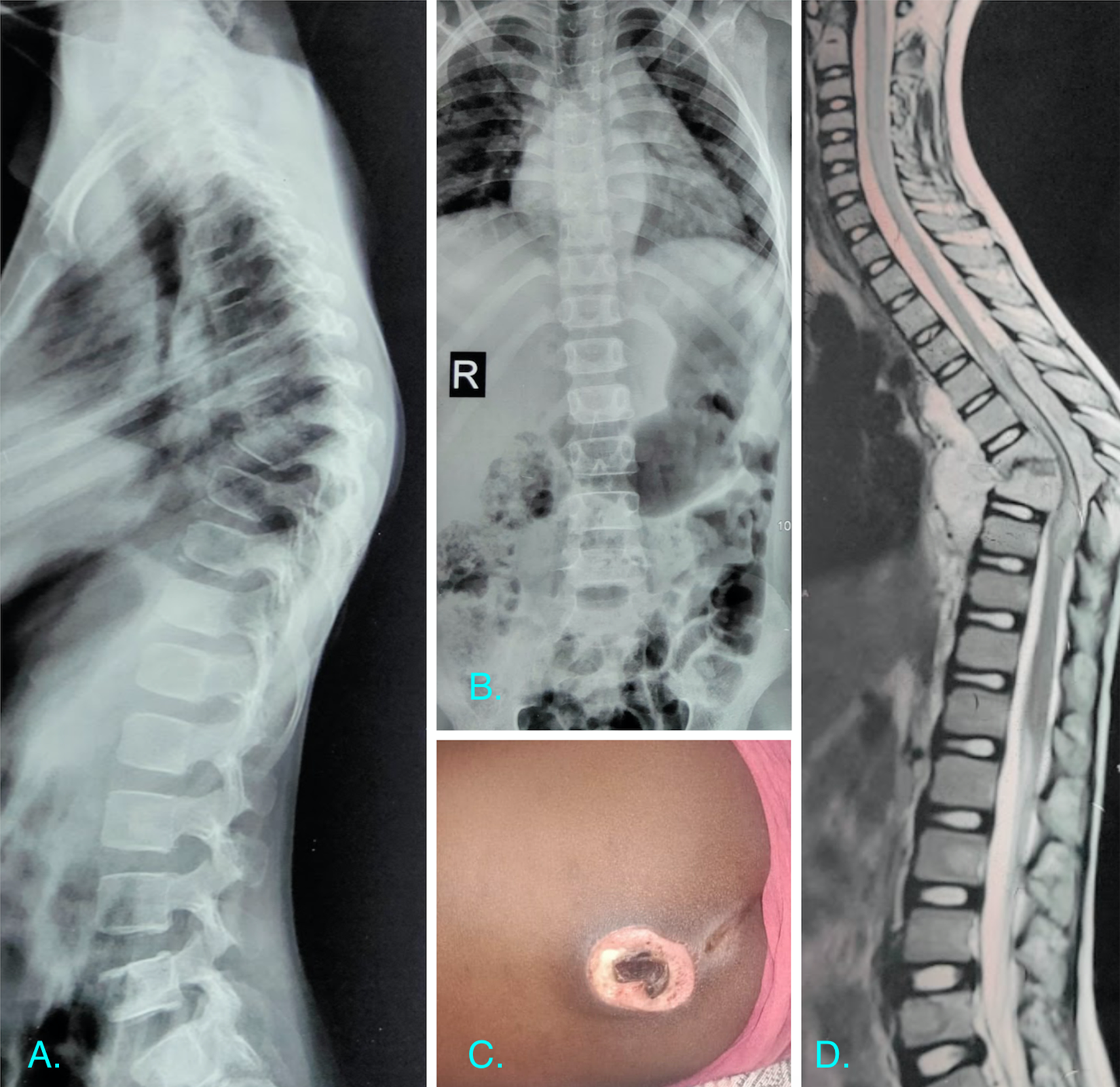
Preoperative imaging of the patient in case illustration 2. A) depicting plain lateral radiograph of the dorsal spine with paradiscal involvement and kyphosis. B) depicting plain anteroposterior radiograph of the dorsal spine with prominent paravertebral soft tissue shadows. C) the patient also had a sacral pressure sore at presentation with necrotic base. D) sagittal T2 W MRI of the dorsal spine showing destruction of vertebral bodies with ventral and dorsal epidural spinal cord compression.
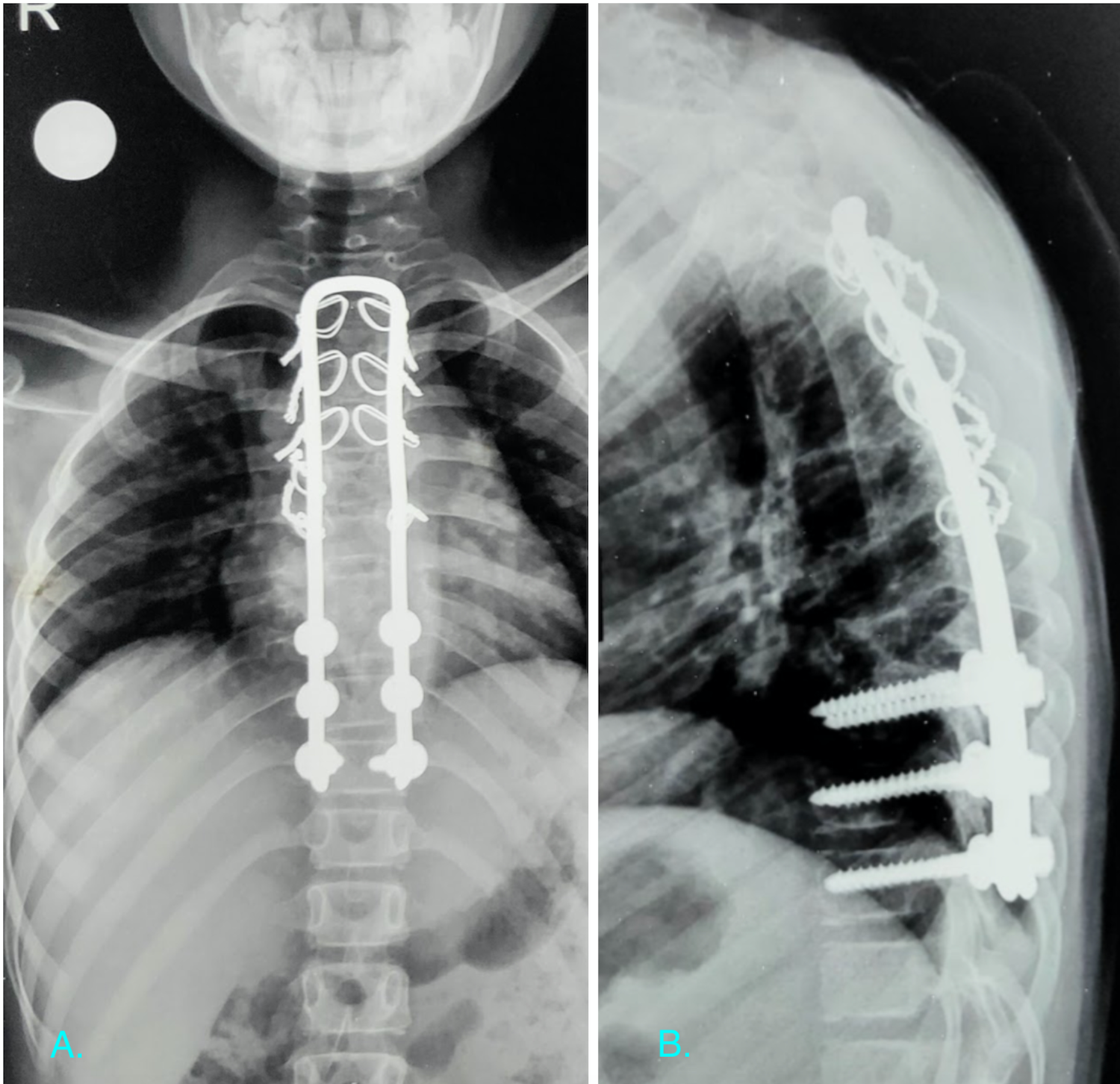
Post operative radiograph of the patient in case illustration 2. A) plain anteroposterior radiograph of the dorsal spine showing the final instrumentation. B) plain lateral radiograph of the dorsal spine demonstrating the restoration of normal thoracic kyphosis and alignment of spinal column.
Discussion
The reported incidence of spinal tuberculosis in children ranges from 58% of all spine tuberculosis in Korea5-7 to about 1/3 rd of all patients from Chennai (India) and 26% of all spinal tuberculosis patients from Hong Kong.8,9 Neurological compromise is a dreadful complication of tuberculous spondylodiscitis. It is often categorized into early and late onset depending on the appearance of symptoms during the course of disease as described by Sorrel and Dejerine in 1924. 10 Early onset neurological deficit is primarily attributed to direct cord compression secondary to the caseous debris, granulation tissue and stretching of the spinal cord over the kyphotic deformity. 11 The recovery from this insult in cases of early onset deficit is usually favorable and many patients recover by mere strict rest and a short course of steroids. This also emphasizes the fact that there is a dynamic component to the onset of neurological deficit related to motion of unstable spinal segments and consequent neurological compromise ensues. The deficit could also be attributed to the spread of the tubercular disease to the spinal cord itself in the form of tuberculoma or microvascular ischemic changes in the end vessels of the cord which often cause irreversible neural compromise. In a developing nation like ours, tuberculosis of spine is still considered a widely prevalent disease. It is not uncommon for patients to be bed bound because of the disease and still do not reach for medical attention. 12 The potential of recovery of the neurological deficit in these patients with a duration of more than 6 months is unpredictable and not reported in literature. Chemotherapy alone may be effective for recovery of these patients in early part of the disease but is not alone enough in advanced cases.3,13,14 The standard chemotherapeutic regimen followed for pediatric spinal tuberculosis consists of an intensive phase of 4 drugs (daily administration). This includes isoniazid (5 mg/kg/day), rifampicin (10 mg/kg/day), pyrazinamide (30 mg/kg/day) and ethambutol (15mg/kg/day) for period of 2 months. This is followed by a continuation phase of 2 drugs isoniazid and rifampicin for a variable duration of 16-18 months as per the institutional protocol. The completion of ATC is decided based on clinical, serological and radiological evidence of cessation of disease activity. The cases with drug resistance are treated as per specific drug sensitivity and are continued for a minimum duration of 24 months. By the consensus of most surgeons, it is found inappropriate for patients to stay in the paralyzed state for extended period of time to be managed only by conservative methods and hence decompression should be attempted early for recovery.3,13-16 It is also mandatory to identify the cause of neurological deficit as the surgical decompression in early cases would suffice by debridement but in late cases they may require internal gibbectomy and spinal osteotomy for decompression. The recovery rate of neurological deficit is dependent on many factors such as the patient’s age, the level of cord, the condition of the spinal cord, the duration and severity of neurological deficit, the presence of drug resistance and the time of onset of treatment. 17 It is commonly mentioned in previous literature about the unlikely chances of recovery in paralysis persisting for a period longer than 6 months especially in advanced cases. 18 They have also commented that the recovery is even poorer with significant kyphosis and vascular compromise of the spinal cord. 18
Our results have clearly demonstrated that the neurological recovery in pediatric patients even with longstanding neurological compromise is favorable and attempts for decompression should not be limited merely due to the duration of the deficit. The neurological recovery is better in children as compared to adults and our study has proven similar findings. There is definite evidence for use of short course of steroids for neurological recovery of acute onset in the adult population but similar guidelines for children are not unequivocal.19,20 Hence we do not rationalize the use of steroids in these children with long standing deficit for neurological recovery. A meticulous counseling is absolutely necessary in the patients approaching to us so late in the course of the disease. Although our results have proven that recovery may occur after surgical intervention, the chances of non recovery should be adequately explained to the parents. Patients with vascular compromise to the spinal cord are unlikely to recover and should always be kept in mind while treating and counseling these patients. 18 Children have a predominant cartilaginous skeleton of vertebral bodies and tuberculosis affection leads to rapid destruction of vertebral bodies. This was also found in our patients where maximum of 7 bodies were completely destroyed due to the disease. Whenever these patients undergo surgical intervention anterior debridement and fusion should always be supplemented by posterior arthrodesis to avoid unacceptable kyphosis secondary to unabated growth of posterior structures.21,22 The overall growth potential of spine is reduced both due to the tuberculosis disease and because of the added fusion of vertebral elements. Although we aim for anterior column fusion at some levels of the affected vertebral segments, there are a few segments with only a posterolateral fusion. This provides a theoretical risk of a future crankshaft phenomenon in patients where a significant growth potential is remaining at the the time of fusion. We have not found any such issue in our patients who were followed up till skeletal maturity. The growth potential can be assessed easily through a Risser’s grading and these patients require careful observation. There have also been recent reports of a decline in pulmonary function in these children requiring fusion before a significant lung development has been completed. This also warrants a follow up of these patients to skeletal maturity to document any development of deformity in the unfused spinal segments. Instrumentation in these children with long standing neurological deficit is also a problematic situation as there is paraspinal muscle atrophy along with osteopenia. It is difficult to find appropriate size pedicle screw without undue prominence under the skin. We therefore have preferred to use a Hartshill rectangle system with sublaminar wiring in these patients wherever possible and at other places we have used a hybrid system with pedicle screws in the distal part of the construct and sublaminar wiring in the proximal part. The extraosseous nature of the sublaminar wire fixation also enjoys the benefit of relatively more cortical nature of the laminae. Pedicle screw fixation in the upper lumbar area like in hybrid fixation has the benefit of sparing of more motion segments of lumbar spine. These children who show clear signs of neglected disease are also poor performers as far as their general condition is concerned and efforts should also be directed for adequate nutritional support including a pediatrician’s reference for malnutrition.
Similar literature providing the results of delayed intervention in tuberculosis of spine is rare especially in the pediatric population. In a study by Rathod et al. they have reported good post operative neurological recovery in adult patients with spinal tuberculosis where time interval from neurological deficit to surgical decompression was 23.5 days. 23 They have reported a range of interval from 5 days to 200 days and significant recovery in 52% cases. However the mean age of the sample was 34.7 years and hence it mainly concentrated on the adult population. Our study has reported good neurological outcomes in 84.6% cases and all these patients remained ambulatory at the final follow up. In a study by Dunn et al. they have reported significant neurological recovery in 92% patients with 74% patients improving from non ambulatory to ambulatory status. 24 The duration of neurological deficit varied from 1 week to 28 weeks. In a study from Kenya in patients of spinal tuberculosis, 61% patients had some kind of neurological involvement. Out of these, 70% patients had marked clinical improvement within 6 months of treatment. 25 Other sources of literature compare the result of late decompression after traumatic spinal cord injuries are not relevant to our discussion since the mode of spinal cord insult is gradual over period of many days in tuberculosis in contrast to traumatic cases where it is sudden onset with different pathomechanics. We strongly believe that the good results of surgical decompression obtained in our cases can predominantly be attributed to the younger age group of patients who show higher chances of recovery. It can also be a result of active lesion of tuberculosis where the predominant source of compression is the abscess and granulation tissue (soft compression) in contrast to healed tuberculosis where cord is stretched over in internal gibbus (hard compression). We believe that this soft nature of compression has lesser chances of producing cord ischemia and hence better chances of neurological recovery as shown in our series.
We had a single complication in the form of superficial wound dehiscence at the graft site in a patient operated for D4-D6 tuberculous spondylodiscitis which healed with daily dressings. We encountered no worsening of neurological deficit in any patient or any other major complication. All our patients showed solid bony fusion and no cases of pseudoarthrosis were noted.
Limitations
An important limitation of the study is the small sample size and a single center experience in treatment of these cases. Similar experience from other centers is required as corroborative evidence. The search for other factors which affect the outcome in these cases also needs to be investigated in detail. These children need to be followed up to skeletal maturity to look for any re appearance of deformity due to crankshaft phenomenon and a close watch is mandatory. This is problematic at our center since patients are not compliant for long duration follow up and do not follow up till skeletal maturity.
Conclusion
This study provides evidence in support of late surgical decompression in pediatric patients with dorsal spinal tuberculosis presenting after extended periods of neurological deficit and a chance for neurological recovery still exists. The surgical decompression should not be deferred only on the basis of time elapsed since the onset of deficit and an optimum neurological environment should be provided for recovery. Majority patients in this study attained ambulatory status by the final follow up.
Footnotes
Abbreviation
ATC: Anti tubercular chemotherapy
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.