
Abstract
Study design
Modified Delphi Consensus and Observational Study.
Objective
Instability in spinal tuberculosis (STB) leads to disabling spinal deformity and neurodeficit. Identifying and estimating instability remains subjective, mainly based on experience. This study aims to develop an objective scoring system to determine instability in STB.
Materials and Methods
The study included 4 phases. (1) A panel of 10 experienced spine surgeons developed a questionnaire based on literature. (2) 68 spine surgeons from 12 countries opined on the importance of each factor in a survey. Five factors deemed important by >70% of participants were further analyzed (3) 60 representative cases of STB were analyzed for instability. A preliminary scoring system was developed, a threshold score for determining instability was derived, and (4) Results were validated.
Results
All the 5 factors (“Spine at risk” signs, severity of vertebral body loss, Cervicothoracic/Thoracolumbar junction involvement, age ≤15, and kyphotic deformity ≥30°) considered important by >70% of participants were associated with instability and included in scoring: age ≤15 years (P-value, 0.05), cervicothoracic/thoracolumbar junction involvement (P-value, 0.028), sagittal deformity angle ratio (DAR) ≥ 15° (P-value, <.001), vertebral body loss-segmental ratio ≥.5 (P-value, <.001), and presence of spine at risk signs (P-value, <.001). A total score of ≥3/09 indicated definite instability with good sensitivity (77%) and excellent specificity (100%). Repeatability assessment showed a good agreement (.9625), and Cohen’s kappa coefficient was strong (.809).
Conclusion
A simple objective scoring system for predicting instability in STB has been developed using 5 main factors; young age, junctional involvement, severity of the deformity, vertebral body loss, and presence of spine at risk signs.
Introduction
Tuberculosis (TB) is the single most infectious cause of death above HIV/AIDS and continues to be among the top ten causes of mortality, affecting 10 million people worldwide. An increase in global travel and migration has made TB a global disease with an increase in incidence even in developed countries.1,2 Spinal Tuberculosis (STB) is the most common form of skeletal tuberculosis, and being inherently destructive is the most common cause of the spinal deformity, instability, and neurological deficits in many parts of the world. Due to multidrug chemotherapy’s effectiveness, surgery in STB is restricted to patients with instability and neurological deficits. 3 Development of neurological deficit, spinal instability, and intractable pain limiting mobilization are the current accepted indications for surgical intervention in spinal tuberculosis. While methods to assess neurological deficits are precise, instability assessment is still primarily based on experience and is subjective, with much variability in surgical indications globally as there is no consensus on factors that determine instability.
The purpose of the study was to use an evidence-based approach incorporating expert opinion consensus from international experts experienced in the treatment of STB and available literature to develop a reliable scoring system to define instability objectively.
Materials and Methods
The study was approved by the institutional review board and was exempted from consent. The study involves 4 phases.
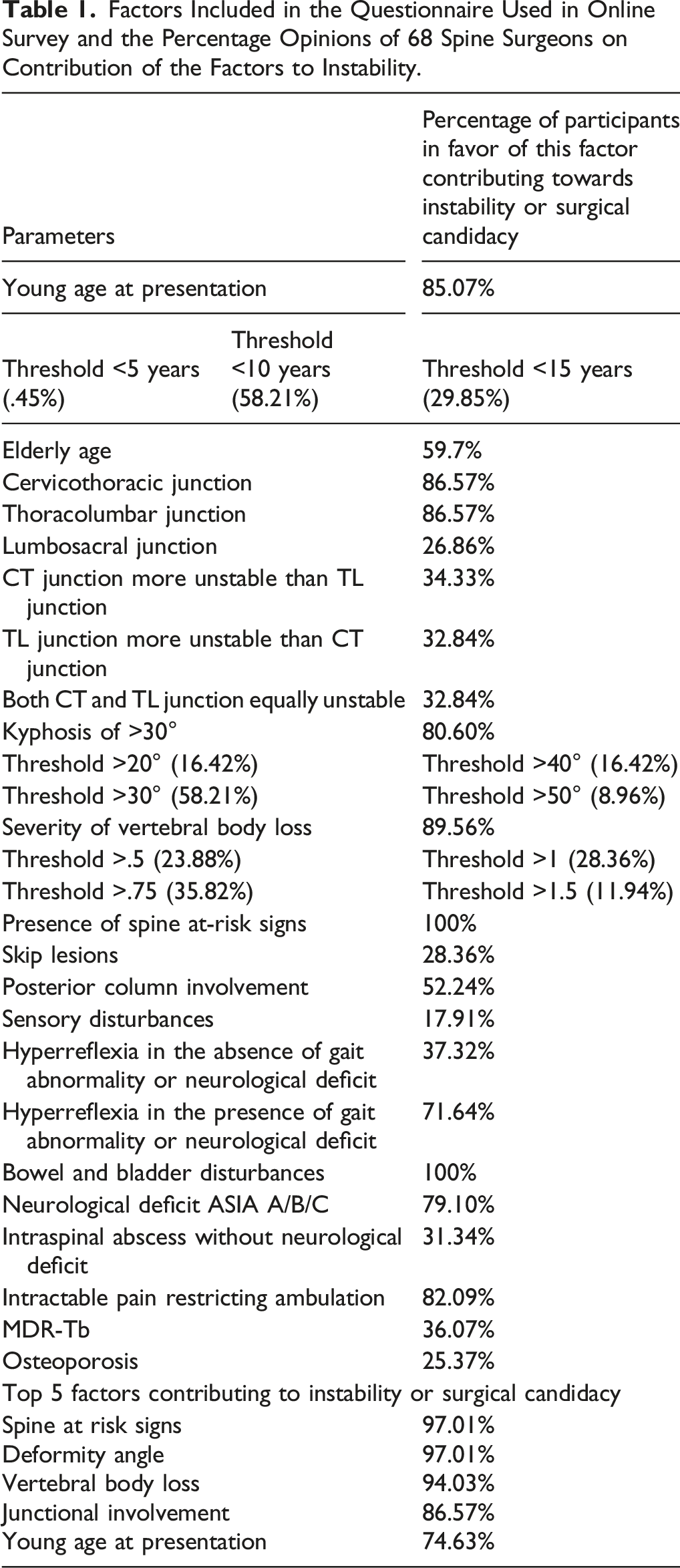
Factors Included in the Questionnaire Used in Online Survey and the Percentage Opinions of 68 Spine Surgeons on Contribution of the Factors to Instability.
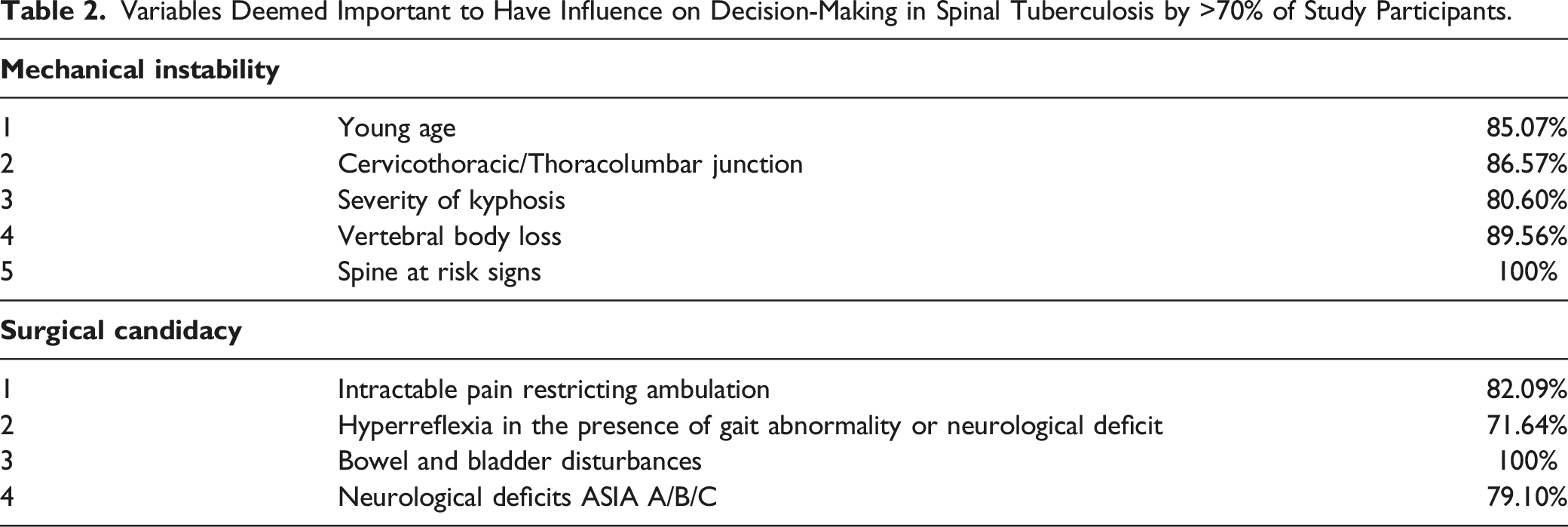
Variables Deemed Important to Have Influence on Decision-Making in Spinal Tuberculosis by >70% of Study Participants.
Statistical Analysis on the Various Factors Which can Influence Instability in 60 Representative Cases of Spinal Tuberculosis.
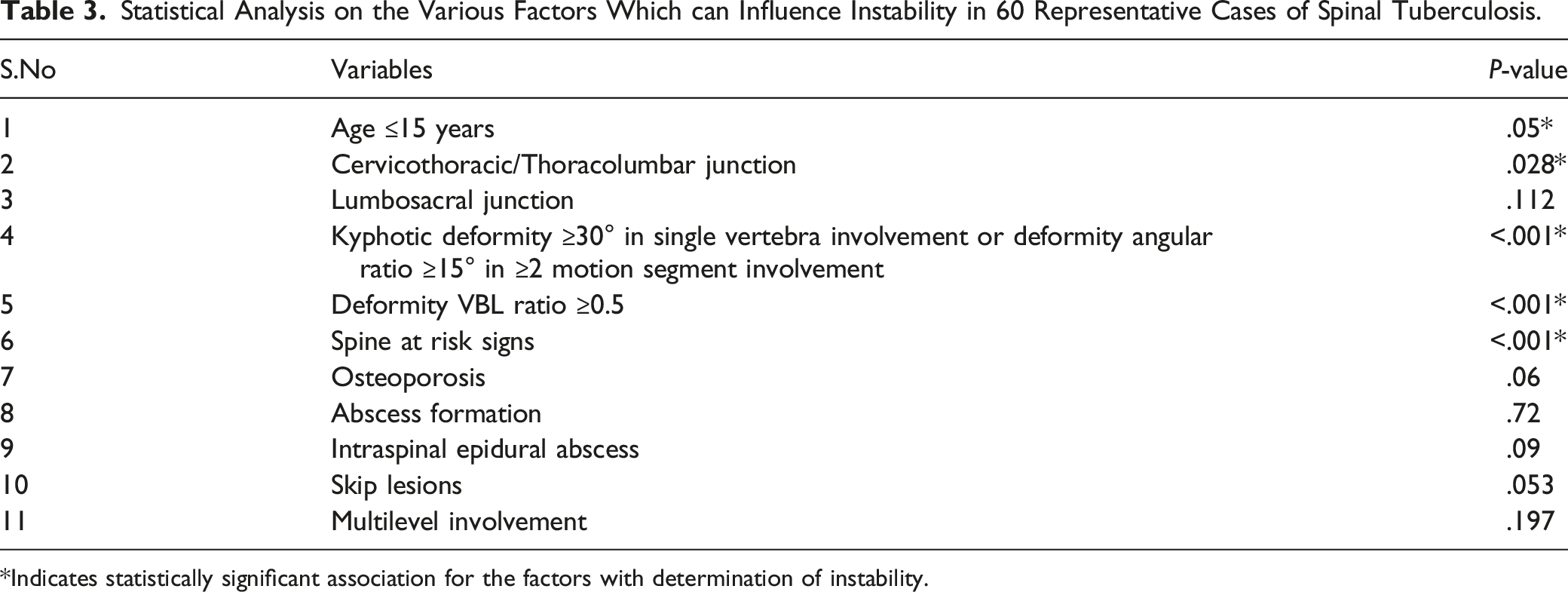
*Indicates statistically significant association for the factors with determination of instability.
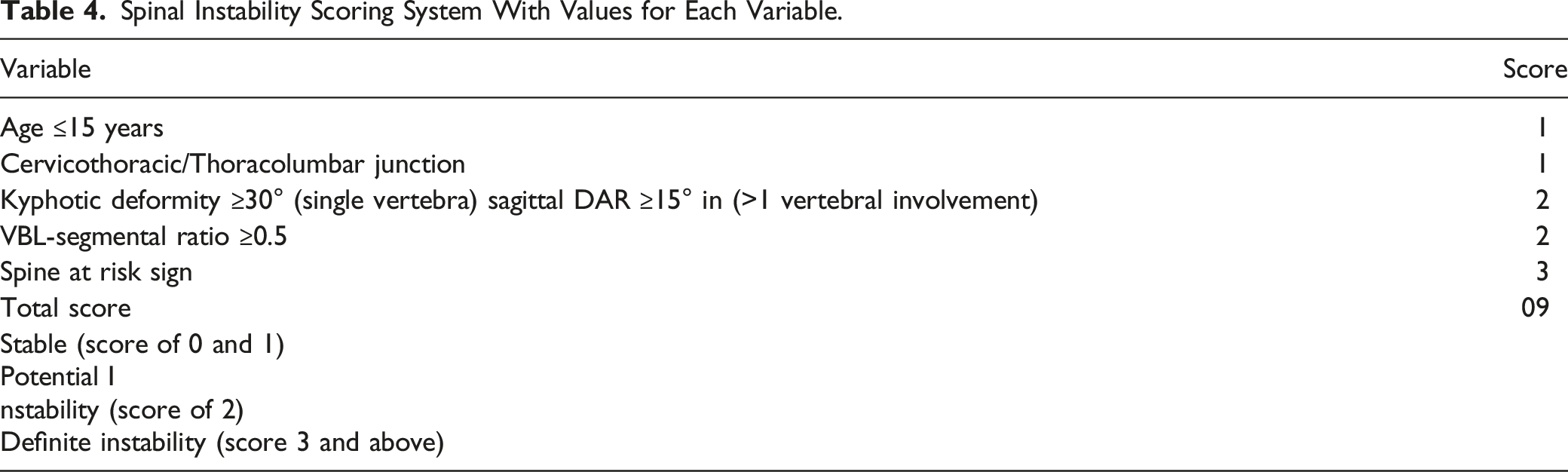
Spinal Instability Scoring System With Values for Each Variable.
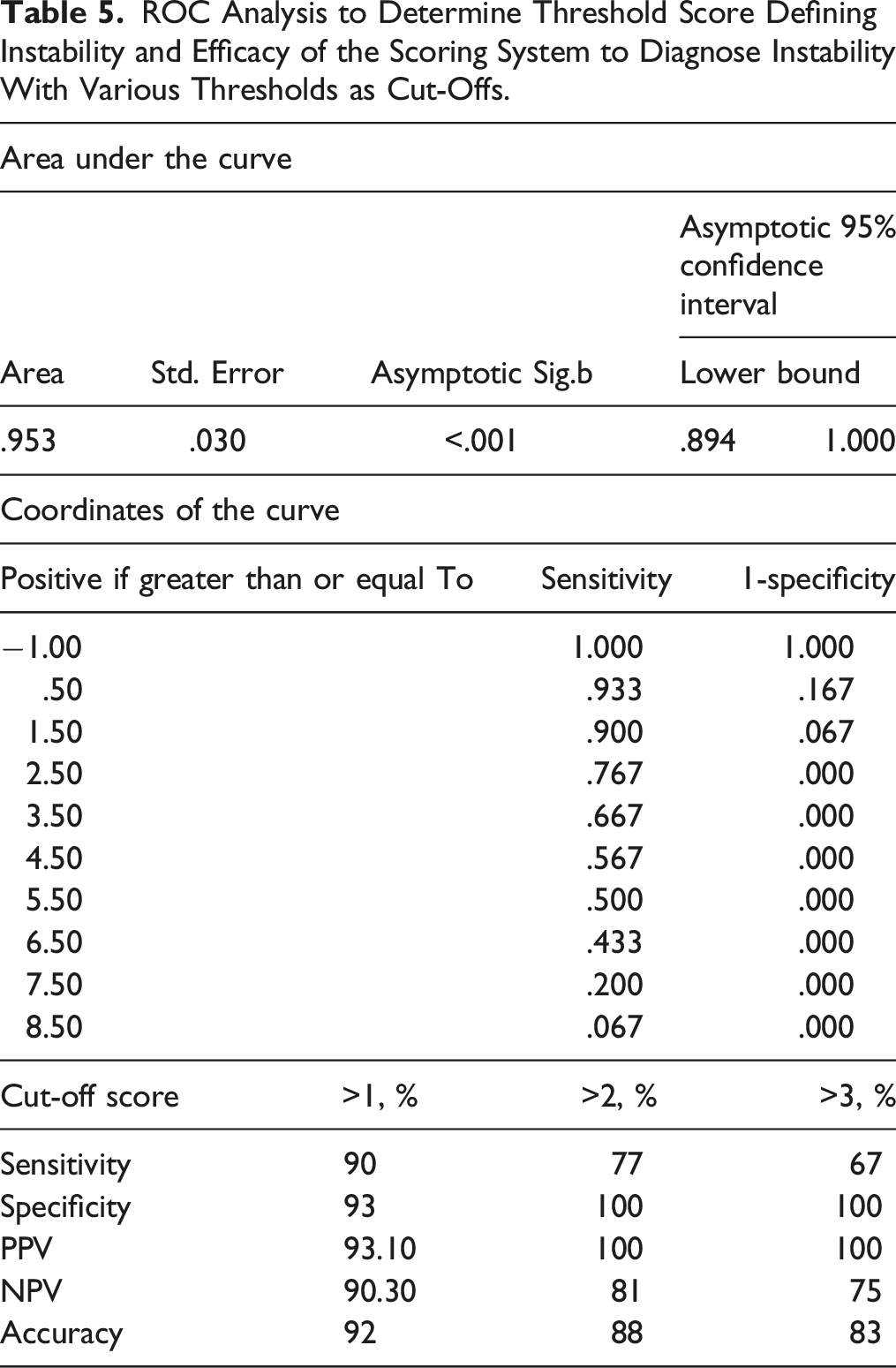
ROC Analysis to Determine Threshold Score Defining Instability and Efficacy of the Scoring System to Diagnose Instability With Various Thresholds as Cut-Offs.
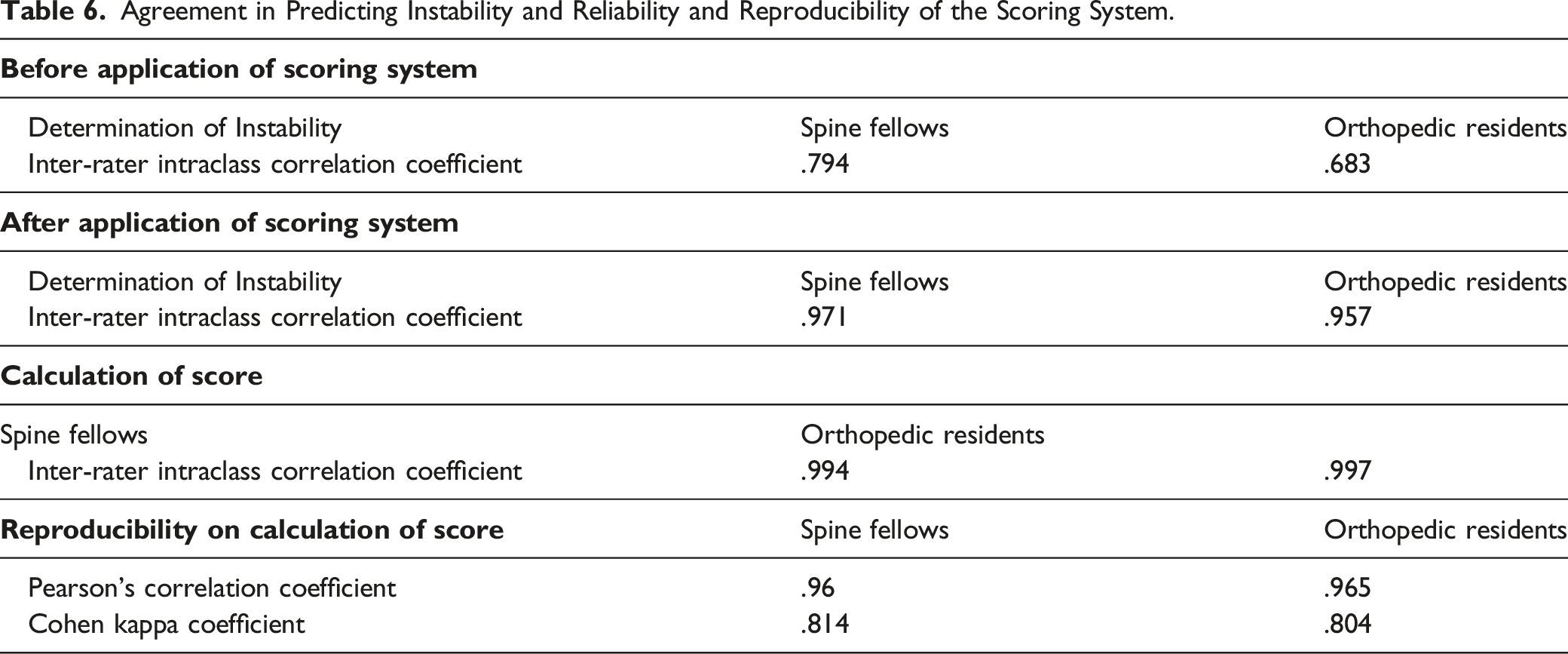
Agreement in Predicting Instability and Reliability and Reproducibility of the Scoring System.
Radiographic Measurements
Deformity
In the current study, we calculated deformity using Konstam angle, measured between the upper and lower endplates of normal vertebra. 4 In cases of lumbar spine involvement, the adjusted deformity was used to account for the loss of normal lumbar lordosis (60°). Since the upper three lumbar discs contribute less to lordosis, 8° were added to the calculated deformity for L1–L2/L2–L3/L3–L4 levels, and 15 and 20° were added for L4–L5 and L5–S1 involvement, respectively.
Sagittal deformity angle ratio (DAR) was calculated by dividing the Konstam angle by the number of involved vertebrae in the case of multilevel involvement
5
(Figure 1). Deformity was assessed using (A) Konstam angle in case of involvement of single vertebra, (B) sagittal deformity angle ratio was used in multiple vertebra involvement.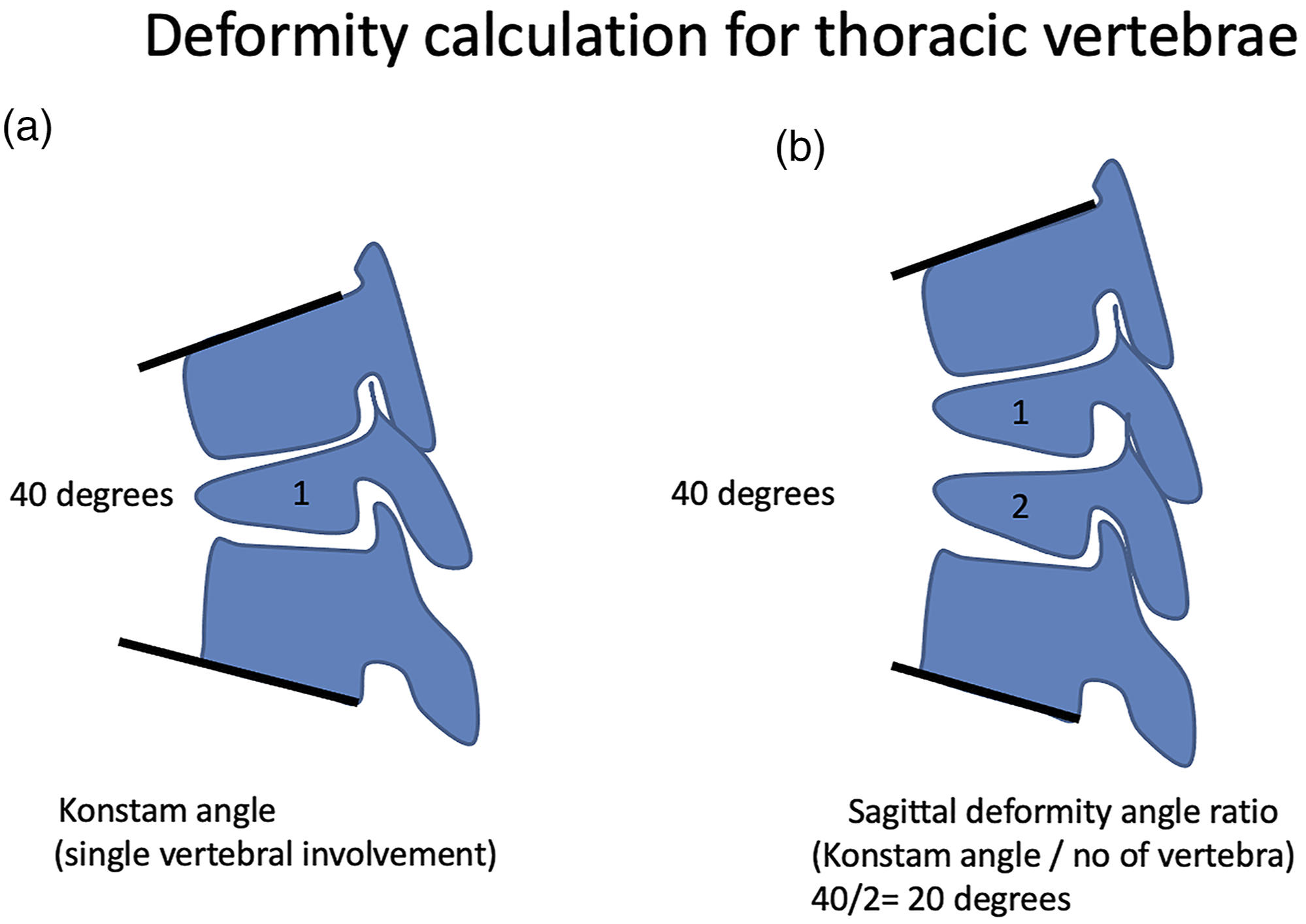
The Severity of Vertebral Body Loss
Anterior vertebral body loss was calculated as proposed by Rajasekaran et al. 6 Vertebral body height was divided into ten equal fractions, and vertebral body loss (VBL) was measured as a number of fractions lost. In multiple vertebral involvements, the VBL of each vertebra was added up to give the total vertebral body loss (TVBL).
The TVBL-Segmental ratio was calculated as TVBL divided by the number of motion segments involved in the vertebral loss. (Figure 2). Line diagram depicting calculation of Vertebral body loss. To calculate VBL, the first Vertebral body height is first divided into ten equal fractions, and VBL will be measured as the number of fractions lost. In the case of multiple vertebral involvements, the sum of each vertebral loss will be mentioned as Total Vertebral body loss (TVBL). The TVBL-segmental ratio is calculated by dividing TVBL by the number of segments involved.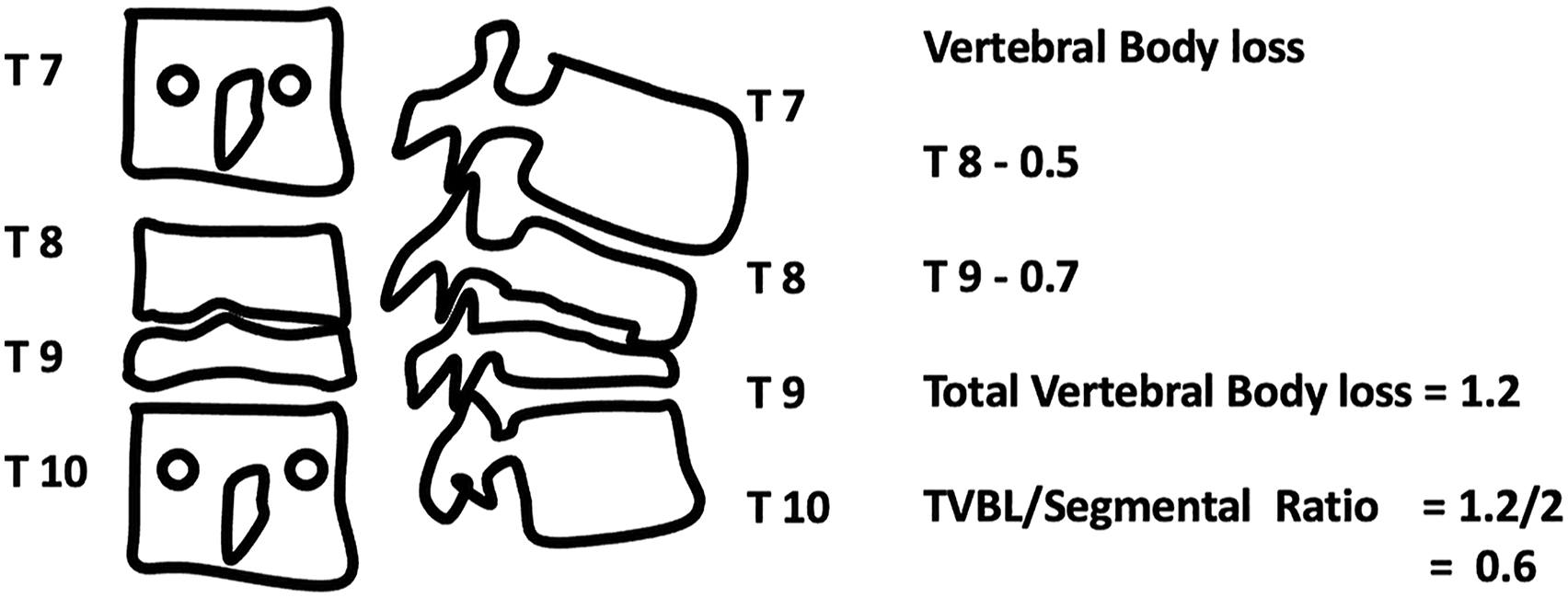
Statistical Analysis
Various factors based on expert’s opinions, knowledge, and understanding were collected to develop a scoring system for established stability of a spine. Along with regular categorical variables, the continuous variables like age, deformity angle ratio, etc., were categorized and statistically assessed for their association with unstable spines, classified as such (stable and unstable) by the experts. Chi-square and Fisher’s exact tests were used to find the variables that were significantly associated with stability. To avoid multi-collinearity between the variables, the significant variables were further filtered using inter-correlation analysis and experts’ understanding of a variable’s effect on stability. A score was given to each selected variable based on their amount of impact on the stability. A cut-off for the total score was assessed from the ROC analysis, which was later validated on a sample of test cases. All the statistical tests were considered significant at P < .05. Inter-rater, intraclass coefficient analysis assessed the reliability of the scoring system, and the reproducibility was assessed using Pearson’s correlational coefficient and Cohen Kappa coefficient.
Results
All 68 surgeons recruited in phase-II of the study answered the questionnaire to identify factors contributing to instability. (Figure 3). Ten variables considered to contribute to instability or surgical candidacy by more than 70% of the participants were considered. The presence of spine at risk signs and bowel and bladder involvement was deemed important by all (100%), followed by severity of vertebral body loss (89.56%), cervico-thoracic or thoraco-lumbar junction involvement (86.57%), young age at presentation (85.07%), intractable pain during ambulation (82.09%), kyphotic deformity >30° (80.60%), neurological deficits of grade ASIA-A/B/C (79.10%), and hyperreflexia in the presence of gait abnormality or neurological deficit (71.64%). Factors identified by only a minority, such as lumbosacral junction involvement (26.86%), skip lesions (28.36%), intraspinal abscess without neurological deficit (31.34%), osteoporosis (25.37%), and sensory disturbances (17.91%), were not considered. Histogram showing opinions of the 68 spine surgeons on various factors considered significantly contributing to instability.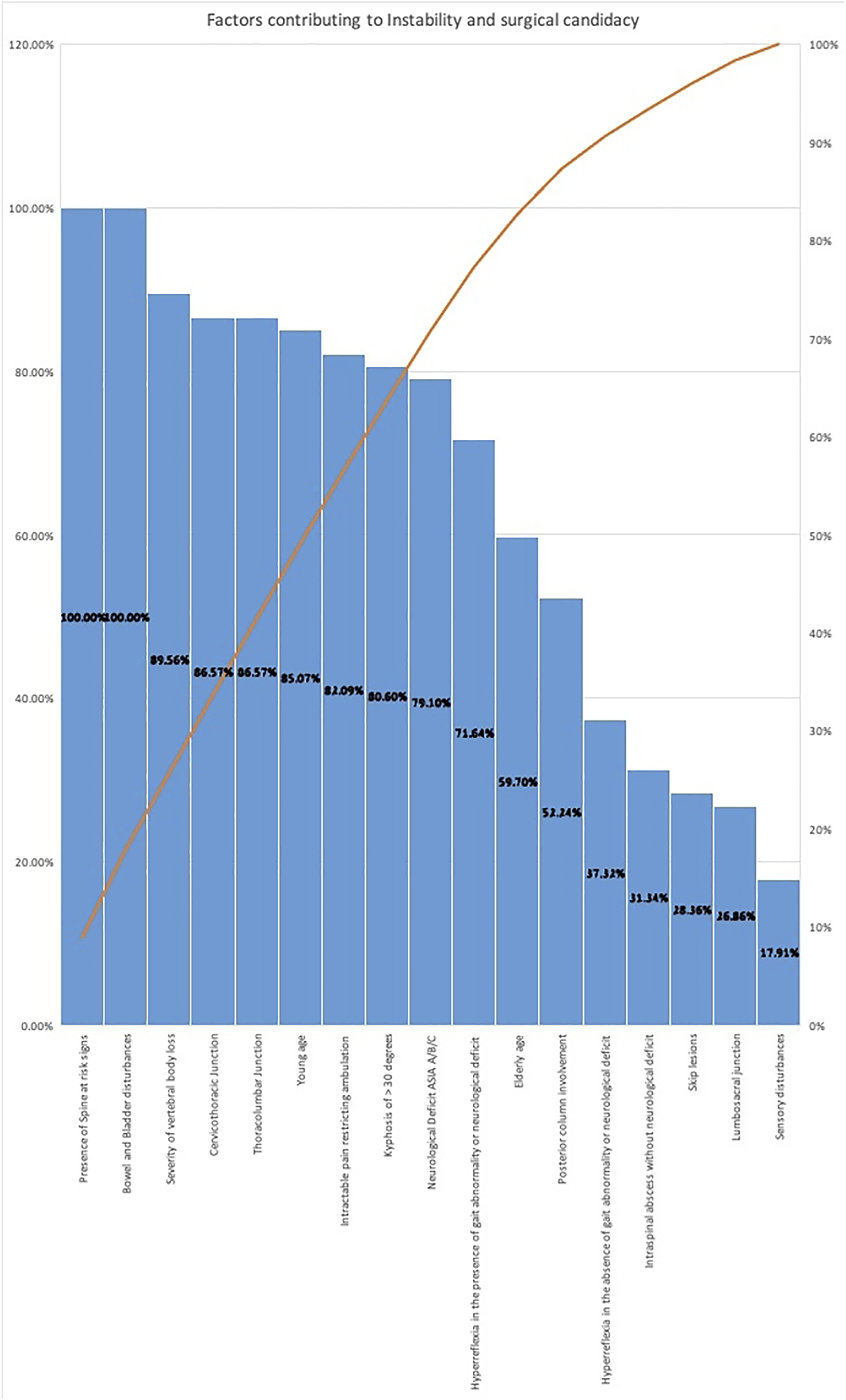
All participants were requested to identify the 5 most important factors contributing to impending or definite mechanical instability. Spine at risk signs (97.01%) and deformity angle (97.01%) were the 2 most frequently reported factors, followed by vertebral body loss (94.03%), junctional involvement (86.57%), and young age at presentation (74.63%) were the most commonly identified.
The 10-member expert panel analyzed the above results in a round table discussion, and a framework was developed for predicting mechanical stability. Among the ten factors, 4 of them; intractable pain restricting ambulation, hyperreflexia in the presence of gait abnormality or neurological deficit, bowel and bladder disturbances, and neurological deficit of grade ASIA A/B/C were discussed and found to be mainly influencers of surgical candidacy, rather than direct causes of mechanical instability. Factors directly responsible for determining deformity progression, instability or impending instability—young age at presentation, junctional involvement (Cervicothoracic/Thoracolumbar), the severity of Kyphosis, vertebral body loss, and presence of spine at risk signs were considered as the 5 main components of the scoring system, which also happen to be the 5 topmost components chosen by the 68 spine surgeons.
Content Threshold Values
To fulfill the aim of developing a simple and yet effective scoring method to evaluate instability-specific domains with defined threshold values to indicate instability were evolved rather than allocating graded scores as done in the spinal neoplastic instability score (SINS) for spinal tumors. 7
Age at Presentation
Young age implicating skeletal immaturity is a well-established risk factor for progressive deformity in children. While the majority of the spine surgeons (58.21%) considered an age <10 years as an indicator of instability, a significant number (29.85%) considered ≤15 years as the threshold. In the round table discussion, the 10-member expert panel opined that though age <10 years will result in a significant deformity progression even after healing of a disease, the skeletally immature adolescence (10–15 years) cannot be neglected, and therefore we considered an age of ≤15 years as the threshold value. A score of 1 was allotted to this content.
Junctional Involvement
This study aimed to develop a scoring system for thoracolumbar tuberculosis; therefore, cervical segments and Occipitocervical junction were not included. Both cervicothoracic (CT) and thoracolumbar (TL) junctional lesions were considered to be unstable lesions (86.57%) when compared to lumbosacral (LS) junction (26.86%). Further, a separate question was raised to find out if surgeons differentiated CT or TL junctional involvement. A variable response was obtained where 34.33% considered CT as more unstable compared to TL, 32.84% considered TL more unstable, and another 32.84% considered both as equally unstable. After reviewing these results, the expert panel had a discussion with a set of examples involving both CT and TL junctions, and a decision was made to consider both as equally unstable with a score value of 1.
Severity of Kyphosis
STB primarily involves and destroys the anterior column resulting in a progressive kyphotic deformity. A deformity of ≥30° at an initial presentation during active stages of the disease was agreed by 80.60% of a participant as a significant contributor of instability. 74.63% would consider deformity >30° unstable and (16.42%) would consider the threshold as 40°, and 8.96% considered a value beyond 50°.
The expert panel evaluated these results and also investigated the scenarios in a series of representative cases. While all of them agreed to set a threshold for 30°, they also opined that the number of levels involved to create the deformity was also substantial. A 30-degree deformity spanning over 5 or 6 motions is different compared to a deformity of 30° contributed by only single or 2 segments. To overcome this, we used Sagittal DAR. A preliminary analysis was done using DAR ≥15° in a series of 60 representative cases in the current study, also, it showed significant co-relation with instability. In the scoring system, under the severity of deformity domain, a kyphosis of 30° or sagittal DAR ≥15° for multilevel involvement was given a score of 2.
Vertebral Body Loss
Vertebral loss calculation was first proposed by Rajasekaran et al. and emphasized as a significant predictor of final deformity. A formula was derived to predict kyphotic deformity (y = a+bx) at the end of treatment. 8 Y is the final angle, “a” and “b” are constants, 5.5 and 30.5, respectively, and x is the initial loss of vertebral height in the thoracic and thoracolumbar spine. Later, it was found that the involvement of 3 or more vertebral bodies with loss of 1 to 1.5 vertebral body height in the thoracic or thoracolumbar spine will result in significant deformity and thereby need surgical intervention. 9 In the current study, we used a TVBL-segmental ratio of ≥.5 to consider instability, and a value of 2 was given for this factor.
Posterior Column Failure
Posterior column involvement in STB is rare, but pedicle or facet involvement, unlike in neoplasia/trauma per se, does not implicate instability. However, the presence of spine at risk signs is a well-documented entity representing a mechanical failure of the posterior column. 10 In this study, while 52.4% would consider posterior column involvement as a factor for instability, 100% of participants felt “spine at risk signs” as a definite sign of instability. A consensus was then reached to include only the presence of any “spine at risk signs” in the scoring system with a value of 3 as it occurs only after failure of the anterior and middle column.
Construct Validity of the Scoring System
The preliminary scoring system was then tested for construct validity by testing its ability to diagnose stable or unstable lesions in 60 representative cases. All 60 cases were presented to the expert panel, and a consensus arrived as to consider them stable or unstable. Statistical analysis was then performed to analyze the association between various possible factors determining instability. All the 5 factors considered in the scoring system were statistically found to be associated with instability: young age 15 years (P-value, .05), cervicothoracic/thoracolumbar junction involvement (P-value, .028), single-level > 30° or DAR ≥15° (P-value <.001), deformity vertebral body loss ratio ≥.5 (P-value <.001), and presence of spine at risk signs (P-value <.001). Non-significant parameters included lumbosacral junction involvement (P-value, .112), osteoporosis (P-value, .06), paraspinal abscess (P-value, .72), intraspinal epidural abscess (P-value, .091), skip lesions (P-value, .053), and multilevel involvement (P-value, .197).
Predictability and Efficacy of the Scoring System
The scoring system (Table 5) comprising 5 domains was plotted for its ability to efficiently diagnose instability. A receiver operating characteristic curve (ROC) analysis was performed to quantify the predictive ability of the scoring system. A cut-off >1, meaning a score of 2 and above, had a sensitivity of 90% and specificity of 93%. A cut-off >2, meaning a score of 3 and above, had a sensitivity of 77% but a specificity of 100%. Positive and negative predictive values and accuracy of the various threshold were also found (Table 5).
Validation of the Scoring System
The validation sample consisted of 30 cases of STB presented to the expert panel to arrive at a consensus on instability. Scoring was performed by 2 experienced spine surgeons who were blinded to the opinion of the expert panel on instability, and the score was validated. The scoring system had 100% accuracy in predicting instability. Ten spine fellows and ten orthopedic residents naïve to the scoring methods were then asked to opine on these 30 cases before and after educating them. Following education of the scoring system, the overall agreement of 72.25 ± 9.87% in predicting instability improved to 92.6 ± 9.49%. The inter-rater intraclass coefficient measured for predicting instability showed moderate reliability before using the scoring system, and it was better amongst spine fellows (.794) compared to orthopedic residents (.683). However, these values improved following the employment of a scoring system and had excellent inter-rater reliability of .971 amongst spine fellows and .957 amongst orthopedic residents. In another analysis, the total score value given to each of the 30 cases by these participants was analyzed at 2 different time points (1 month apart) to investigate the reliability and reproducibility of the scoring system. The calculation of score had excellent inter-rater intraclass coefficients amongst both spine fellows (.994) and orthopedic residents (.997). Repeatability/reproducibility assessed using Pearson’s correlation analysis showed a good agreement (.9625), and the overall Cohen's kappa coefficient was strong (.809) even after 1 month of initial measurement.
Discussion
As per WHO 2020 statistics, in 2019, an estimated 10 million people fell ill with TB worldwide, while a total of 1.4 million people died from TB in 2019. 11 Worldwide, TB is one of the top 10 causes of death and the leading cause of a single infectious agent (above HIV/AIDS). Spinal tuberculosis (STB) is the most common form of extra-pulmonary TB affecting more than 50% of those with skeletal involvement. 12 In addition, STB is still the most common cause of paraplegia and deformity across many parts of the world. 13
Multidrug chemotherapy has converted uncomplicated STB into mainly a medical disease due to its excellent healing response. 14 However, instability and neurological deficit are 2 critical scenarios where surgical intervention is required. 15 While evaluation and assessment of neurological deficit can be objective and precise, the ability to identify and estimate instability remains very subjective and generally based on individual experience. This can lead to errors in clinical judgment where a patient with spinal instability could have progressive deformity not only during the active stage of the disease but also after healing of the lesion and can perpetuate neurological weakness. 16 On the contrary, surgical intervention in stable lesions leads to a waste of resources and can also expose the patients to the risks of surgery, leading to unnecessary morbidity and mortality. Furthermore, surgical debridement and stabilization often involve the transgression of body cavities and intraspinal procedures with blood loss and possible intraoperative neurological deficits. 17 Therefore, there is an urgent need for objective assessment of instability which, apart from a neurological deficit, is the main indication for surgery. This will be a boon in deciding the management of approximately 150000 patients getting affected by STB in the world annually.
Quantifying spinal instability is a challenge given the influence of multiple clinical, radiological, and biological factors and is varied across different pathological conditions such as trauma, osteoporosis, tumor, metastasis, and infections. The Spinal Instability Neoplastic Score (SINS) used for quantifying spinal instability in metastasis has been widely used and validated for its efficacy and reliability in multiple studies. 7 It is based on 6 factors: location of the lesion, type of lesion, bone lesion, spinal alignment, vertebral body collapse, and posterior spinal involvement. A similar score but specific to factors contributing to instability in STB will be helpful not only for the surgeons in the developing world who frequently treat these cases and serve as a guide in the developed world who have no/little experience in treating STB.
Oguz et al. 18 described the GATA classification to predict instability in STB in 2008 based on a combination of various factors like disc involvement, vertebral damage, abscess formation, kyphosis, and neurological deficit. There were 3 groups 1–3, based on a combination of these factors, and corresponding treatment principles were described. However, the classification is subjective, vague, and descriptive rather than being objective and quantitative. Being far from ideal, this classification has not been validated nor used widely.
Our study has fulfilled the need for an objective spinal instability scoring system in TB, which has been developed on a robust scientific methodology, bringing in the expertise of a 10-member panel and 68 spine surgeons from 12 different nations experienced in treating STB. The whole process was evidence-based and performed logically and systematically, and verified by appropriate statistical methods. After enlisting all factors influencing STB management, a questionnaire was circulated using an online survey tool to arrive at a consensus of factors in the scoring system. Ten factors deemed important by >70% of the participants were segregated into factors contributing to actual mechanical instability and those that influence surgical candidacy.
Among the ten factors deemed important, the presence of spine at-risk signs and bladder and bowel disturbance were universally accepted to favor surgical decisions. However, bladder and bowel disturbances were not considered for instability scoring as they contribute more toward determining surgical candidacy rather than instability. Similarly, pain restricting ambulation is a subjective criterion, which could either be due to biological or mechanical reasons and again influence the surgical choice rather than actual contribution to mechanical instability.
The top 5 factors recognized by the 68 spine surgeons and the 10-member expert panel to contribute to mechanical instability included spine at risk signs (97.01%), deformity angle (97.01%), vertebral body loss (94.03%), junctional involvement (cervicothoracic/thoracolumbar) (86.57%), and young age at presentation (74.63%).
Younger Age at Presentation
Younger age at presentation has been a well-established risk factor for deformity progression as the natural history of STB in relation to deformity in children is different from that of adults. Biomechanically, pediatric spine can be compared to a long structural slender column, which leads to a “buckling collapse” when subjected to a high load or when weakened by destruction, as in the case of STB according to the biomechanical principles proposed by Euler. 9 The pediatric spine is naturally more flexible and prone to collapse owing to the higher disc-vertebral ratio. In infancy, the disc with the lowest Young’s modulus of elasticity occupies 50% of the vertebral height compared to only 25% in adulthood. 19 In addition, the lower cross-sectional area of a pediatric spine and excessive ligamentous laxity predispose the young age population to higher tensile forces when anterior structures are destroyed, as in the case of spinal TB leading to facetal subluxation, instability, and progressive deformity. Further, multilevel contiguous level involvement and significant destruction of anterior structures are more common in children, unlike the paradiscal type of involvement in adults. While an age <7 years has been an established risk factor for “buckling collapse,” a number of studies have documented an age <10 years as a risk factor for progressive deformity. 20 In the current study, a good number of participants (29.85%) considered an age between 10 and 15 as still skeletally immature in addition to the (58.21%) who considered <10 years as unstable. A round table discussion was held, and a consensus was arrived to choose an age ≤of 15 years as the threshold in the study, and a score of 1 was allotted.
Cervicothoracic and Thoracolumbar Junctional Involvement
Junctional involvement has always been considered inherently unstable due to the biomechanical transition from a mobile segment (cervical/lumbar) to a rigid segment (thoracic/sacral), rendering them to unusually high tensile forces on axial loading, especially after the destruction of anterior structures as in STB. In addition, the neural structures at the cervicothoracic junction are subjected to a higher chance of damage owing to the smaller canal size similar to the thoracolumbar junction. However, lumbosacral junctions are considered stable due to a larger spinal canal, passage of cauda equina fibers, unlike the conus medullaris at the thoracolumbar junction or the spinal cord at the cervicothoracic junction, and generally have good clinical outcomes.21,22 Further, vertical facet orientation and inclination of the vertebra at cervicothoracic and thoracolumbar junction predispose them to higher translational forces, unlike the lumbosacral joint. In the current study, while most of the participants considered lumbosacral junction as stable and less likely to influence the progression of the deformity and progressive prolapse, there was no consensus as to which of the cervicothoracic or thoracolumbar junction is highly unstable. 34.33% considered CT as more unstable compared to TL, 32.84% considered TL more unstable, and another 32.84% considered both as equally unstable. Owing to this discrepancy and biomechanical reasons, both were considered equally unstable and were allotted a score of 1.
The Severity of Deformity
A deformity of ≥30° was considered unstable based on available evidence and the expert consensus. However, on reviewing many representative cases, multilevel involvement was common in TB, and the expert panel realized that a deformity of 30° contributed by a single vertebra cannot be equated to that of 3 or 4 vertebral involvement. Such inclusion will overly diagnose instability in multilevel involvement. It should be realized that a deformity is considered an important factor of instability as it puts the posterior column at stress which is true for a significant deformity contributed by a single vertebra. A solution was proposed to calculate sagittal deformity angle ratio (DAR), where deformity angle is divided by the number of involved vertebrae in the case of multilevel involvement. A DAR ≥15° was proposed as a threshold based on a recent study that reported DAR ≥15° to have a significantly higher rate of spinal cord monitoring events during deformity correction. 5 The association between a kyphosis of ≥30° or DAR ≥15° in multivertebral involvement was given a score of 2.
Total Vertebral Loss
A TVBL of 1 to 1.5 has been identified as a risk factor for instability. However, a TVBL of 1 contributed by a loss of .25 in each vertebra across 4 segments could be stable, while a TVBL of 1 contributed by .5 in each vertebra across 2 segments is essentially unstable. Therefore, considering the biomechanical principle of loss of 50% vertebral height as unstable, a TVBL-segmental ratio (calculated as TVBL divided by the number of motion segments) ≥ .5 was considered unstable. The TVBL—segmental ratio ≥.5, which was found to be significantly associated with instability, was given a score of 2.
Spine At-Risk Signs
Rajasekaran et al. described 4 radiological signs (a) “Separation of the facet joints” (b) “Retropulsion” (c) “Lateral translation,” and (d) “Toppling” of vertebra in children, which essentially indicate failure of the posterior column due to facet subluxation or destruction. 20 In a large prospective cohort study of 61 children affected with STB, the presence of spine at risk signs was identified as independent risk factors for progressive collapse and deformity progression. Unlike anterior vertebral destruction (vertebral body loss) leading to kyphotic deformity, which stresses the posterior column with impending instability, the presence of spine at risk sign is telltale evidence for existing instability even in adults. The presence of the spine at risk signs was the only biomechanical factor agreed by 100% of participants and was also significantly associated with instability in an analysis performed across 30 stable and unstable cases of STB in the current study. We have not included posterior column involvement as it does not reflect on mechanical instability. The mere involvement of the posterior column does not indicate posterior column failure and is amenable to chemotherapy. On the other hand, since posterior column failure is an active indicator of existing instability, the presence of spine at risk signs was given the highest value of 3 amongst the 5 factors considered in the scoring system.
Efficacy, Agreement, and Validity of the Scoring System
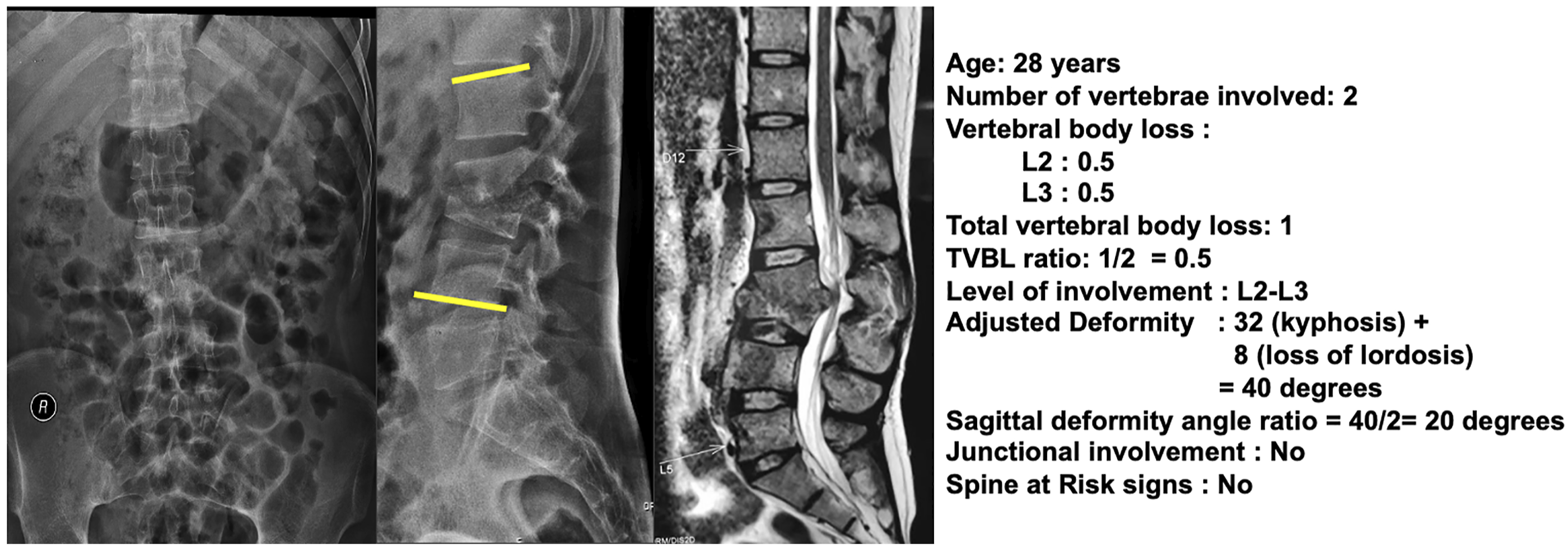
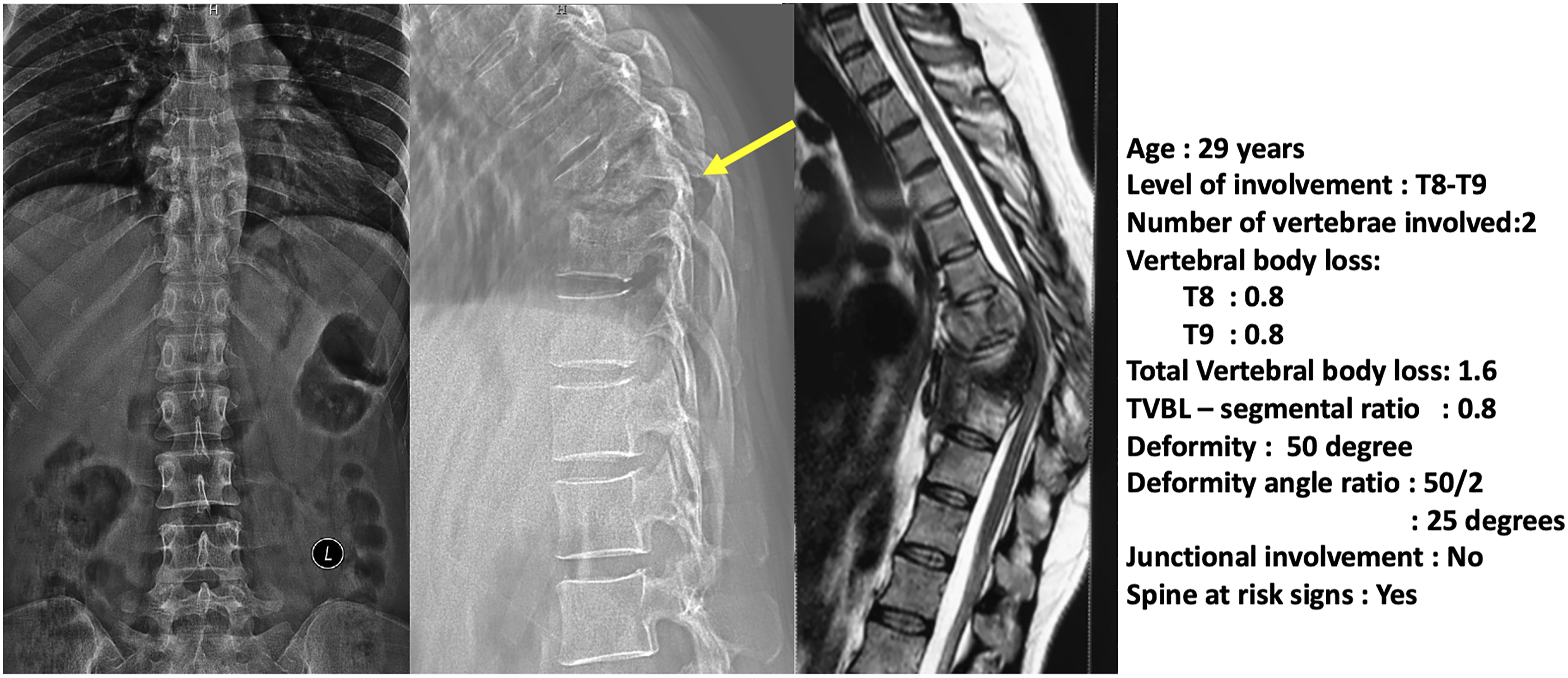
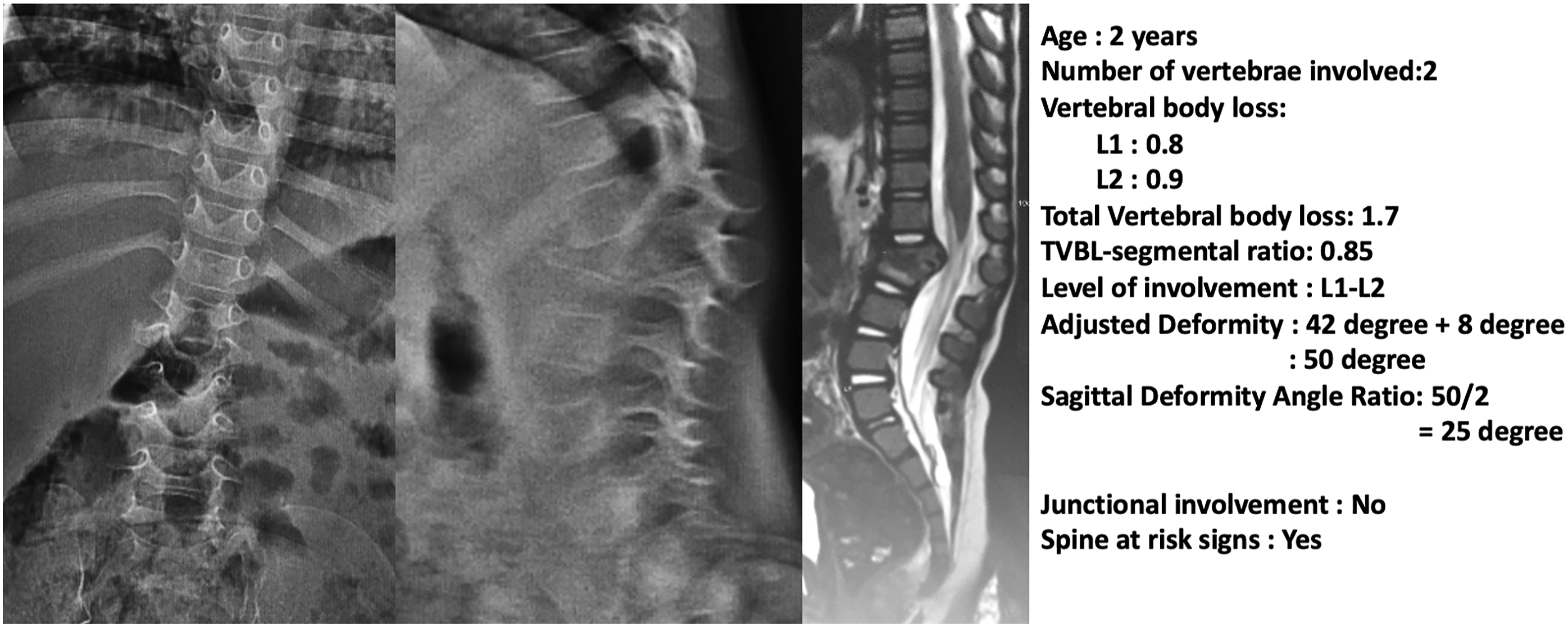
We have developed a simple yet effective scoring system to predict instability in STB using the above 5 easily measurable objective measurements (Figure 4). The total score for the 5 factors considered is 9, and a ROC analysis identified the threshold score of 3 and above to definitely predict instability with a sensitivity of 77% and specificity of 100%. The ability of the scoring system to predict instability was again validated in a fresh set of 30 STB cases and checked for agreement. The score calculation was also checked for internal consistency and reproducibility, which showed excellent inter-rater intraclass co-efficiency and a good Kappa value of .809. Figures 5–7 illustrate the application of the scoring system to predict stability or instability in STB. A 74-year-old male with intact neurology diagnosed with spinal tuberculosis presenting with occasional back pain. The scoring system application: Age (0), Junctional pathology (1), Deformity (0), VBL (0), Spine at risk signs (0) resulted in a total score of 1. Therefore, despite the involvement of the thoracolumbar junction due to the absence of severe deformity or anterior destruction, this lesion would be considered a stable lesion. A 28-year-old male was diagnosed with lumbar spinal tuberculosis. The scoring system application: Age (0), Junctional pathology (0), Deformity angle ratio (2), VBL (2), Spine at risk signs (0) resulted in a total score of 4, which indicates definite instability. The case illustrates how adjusted deformity was calculated for lumbar kyphosis and also shows the calculation of sagittal deformity angle ratio as two vertebrae are involved. A 29-year-old male was diagnosed with thoracic spinal tuberculosis following transpedicular biopsy. The scoring system application: Age (0), Junctional pathology (0), Deformity angle ratio (2), VBL (2), Spine at risk signs (3) resulted in a total score of 7, which indicates definite instability. The case illustrates the presence of spine at risk signs (arrow) which can also occur in adults and always indicate definite instability following the failure of the anterior column. A 2-year-old boy presented with deformity and was found to have spinal tuberculosis of the lumbar spine. The scoring system application: Age (1), Junctional pathology (0), Deformity angle ratio (2), VBL (2), Spine at risk signs (3) resulted in a total score of 8, which indicates definite instability. This case illustrates how age plays an important role in biomechanical instability as the child has progressed to significant deformity following massive destruction of the anterior column without obvious clinical symptoms.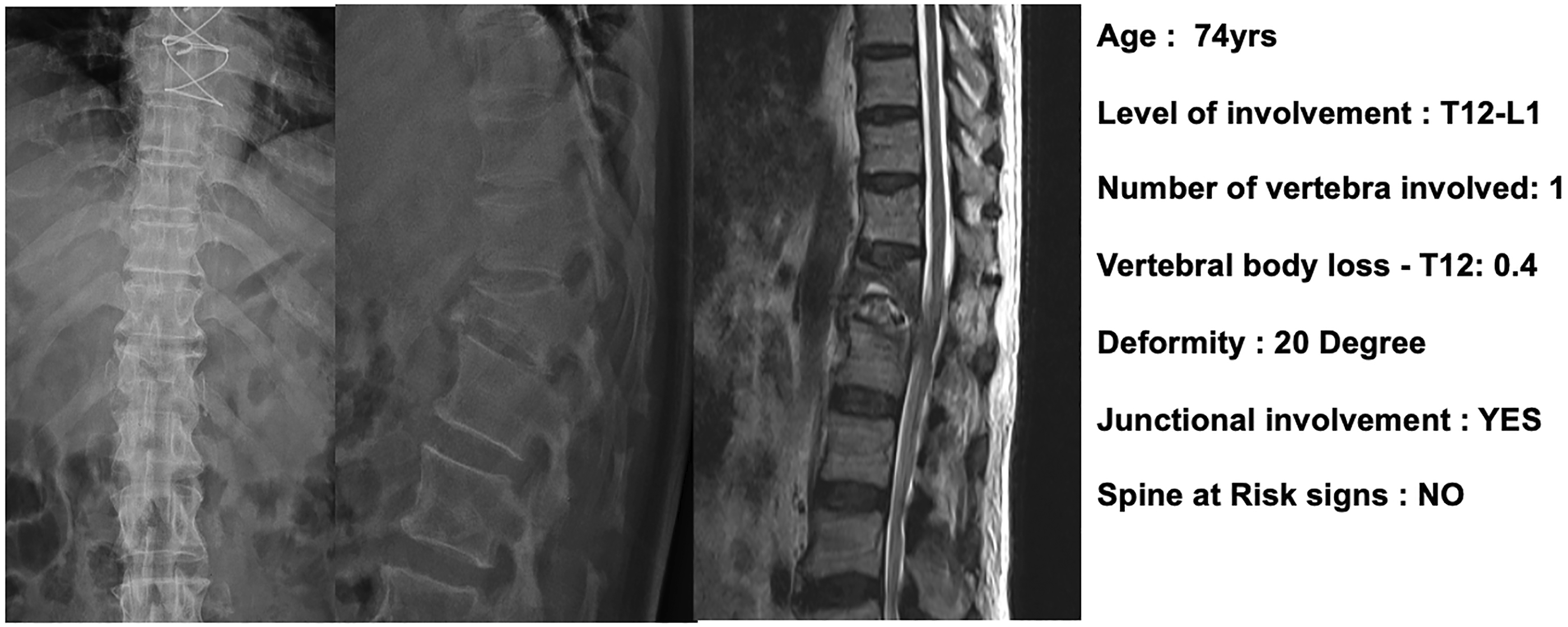
Strength and Limitations of the Study
We have adopted a systematic way of including only factors which have a direct association with mechanical instability in STB based on sound biomechanical evidence and consensus made by a 10-member expert panel over the opinions of 68 experienced spine surgeons. The factors were also found to be statistically relevant, and the scoring system proved to have excellent efficacy, reliability, and reproducibility (Figure 8). The limitation of the study being representative cases for analyzing TB was done from a single institution for the want of making appropriate measurements, and though 68 spine surgeons from 12 different nations were involved in the development of the scoring system, the validation was done amongst spine fellows and orthopedic residents belonging to the lead authors institution. Future studies involving multiple centers contributing representative cases might add much more validity to the classification system. The current scoring system only identifies spinal instability and defines a threshold for surgical management. However, it does not help in deciding levels of fusion or approach/need for reconstruction. Also, this score needs to be evaluated prospectively at every follow-up to identify instability at an earlier stage. The systematic methodology used in the current study to frame a scoring system for spinal instability in spinal tuberculosis has been depicted.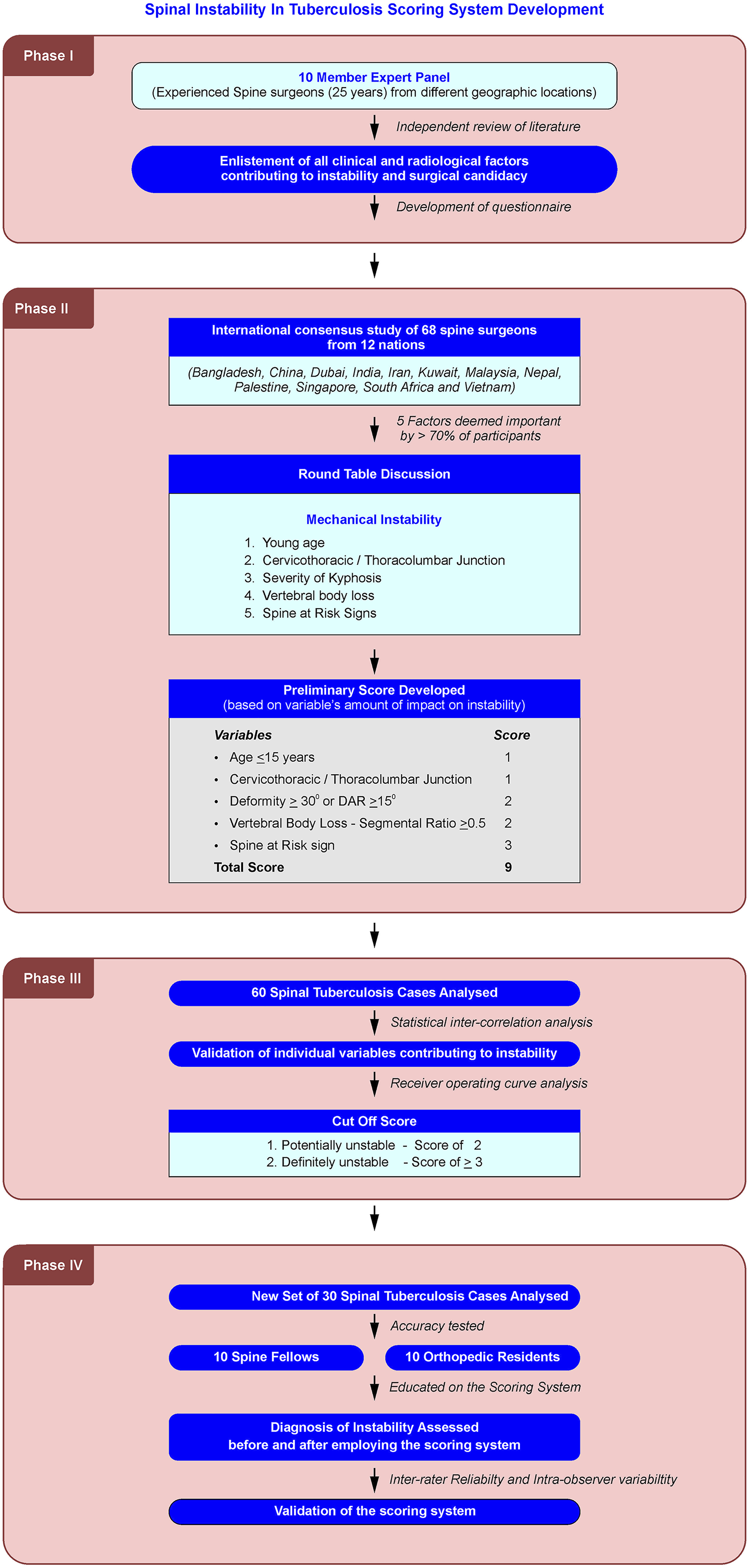
Application of the Score
In the final form, the evolved score had a total possible score of 9 from 5 factors. Each of these factors was given a value of 1–3 depending upon how severely they contributed to instability. The lowest score of 1 was given to age and the presence of cervicothoracic or thoracolumbar junctional lesions. This is because, while both these factors were important, the severity of the lesion and the ex1t of destruction was important irrespective of their region or age and time of involvement. A score of 2 was allotted to the severity of deformity because it directly influenced instability and also the chances for a functional posterior column failure. This was the same with total vertebral body loss, which has documented evidence for progression in kyphosis. The highest score of 3 was given for spine at risk signs as it represented an already unstable and displaced spine.
Application of this score in 60 cases showed that patients with a score of zero or 1 were stable; 2 were potentially unstable and required careful monitoring, and 3 and above were definitely unstable and required surgical stabilization.
Conclusion
We have developed a simple objective method of scoring instability in spinal tuberculosis based on a robust scientific and logical methodology bringing together both evidence and expert consensus of 68 spine surgeons from all over the world. The scoring system formed on a sound biomechanical basis was validated for its efficacy in predicting instability and documented to have excellent reliability and reproducibility. This novel scoring system employs 5 factors that can be objectively assessed and therefore has global application in the assessment of instability in STB.
Footnotes
Acknowledgments
All authors contributed equally towards the preparation of this manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by Ganga Orthopaedic Research and Education Foundation (GOREF 2020-09)
IRB Approval
The study was approved by Instituional review board of Ganga Medical centre and hospitals, Coimbatore. (Registered with CDSCO, Regn No: ECR/1146/Inst/TN/2018, NECRBHR Regn No: EC/NEW/INST/2020/1146.). IRB approval no of study: 2020/03/09.