
Abstract
Study Design:
Prospective Observational Study.
Objectives:
To assess the feasibility of utilizing SINS score, originally suggested for neoplastic conditions, to assess structural instability in spinal tuberculosis.
Methods:
Patients with an established diagnosis of spinal tuberculosis were included in the study. Based on SINS scoring, patients classified as those with “indeterminate stability” were managed with or without surgery based on other parameters including neurological status, severity of pain, medical comorbidities, etc.
Results:
Eighty [39 males, 41 females] patients prospectively evaluated with mean age 46.74 ± 17.3 years. Classification done into stable [n = 7], indeterminate [n = 45] and unstable [n = 28] groups based on SINS scoring. All the patients in unstable group were treated with surgical stabilization whereas none in the stable group required surgical stabilization. In the indeterminate group, 26 patients underwent surgical stabilization, while 19 treated non-operatively. Major determinants predisposing to surgical intervention in “indeterminate group” were pain [14 of 26 patients] and neurological status [11 of 26 patients]. Mean follow-up 38.5 ± 22.61 months with minimum follow-up being 24 months. Preoperative VAS score for pain improved from median of 9/10 to 1/10 following surgery [P < .0001]. In the non-operative group, the improvement was from median score of 6/10 to 1/10 [P < .0001]. Preoperative ODI improved in non-operative and operative group from median of 42% and 70%, respectively to 10% and 12%, respectively in the postoperative period [P < .0001 for both groups].
Conclusions:
SINS scoring can be a helpful tool in surgical decision-making even in spinal tuberculosis. Further refinement of the score can be done with a larger, multicenter study.
Keywords
Introduction
In a review article on trends of surgery in spinal tuberculosis, Fisahn et al identified instability as a common indication for surgery. 1 There is reasonably unequivocal literature to identify instability in pediatric spinal tuberculosis. 2 Unfortunately, however, there are no universally uniform objective criteria to define instability in the adult spinal tuberculosis. Lee et al labeled tuberculous spines as unstable in the presence of “instability catch,” i.e. a sudden painful “snap” that occurs when one extends from a forward bent to an upright position. 3 On the other hand, Mehta and Bhojraj considered kyphosis more than 30 degrees to be a potential indicator of instability and hence, an indication for surgery. 4 Mak and Cheung however, quoted kyphosis more than 60 degrees as an indication for surgery. 5 In a review article by Jain AK and Jain S, the authors advised surgical stabilization on patients with absent pedicle shadow or those with minimal scoliosis on anteroposterior radiographs or those with kyphosis. 6 They however, did not quantify the degree of kyphosis in their literature. This review of literature amply demonstrates lack of unequivocal guidelines to stabilize the tuberculous spine, particularly in adulthood.
SINS score was proposed as an objective scoring system to identify structural instability in spine affected by neoplastic process. 7 Since the process of bone destruction in infection is more akin to that in neoplastic pathology than to that in trauma, the authors hypothesized that this scoring system might be fruitfully utilized to evaluate instability in spinal tuberculosis across all age groups.
Materials and Methods
This was a prospective observational study, carried out after IRB approval [HOSMAT Hospital Institutional Review Board, approval number 02/ 20-21] at a tertiary referral center for spine surgery. Consecutive patients with established or suspected diagnosis of spinal tuberculosis were included. Informed consent was taken from all the patients. Patients with spinal tuberculosis subjected to laminectomy in the past; those with pyogenic infection and those with incomplete radiological investigations were excluded.
Preoperative radiographs, MRI and CT scanning were routinely carried out in these patients. Based on radiological criteria derived from these investigations along with clinical criteria, SINS scoring was done 7 [Table 1]. Status of posterior column integrity was assessed in the form of facetal disruption on plain lateral radiographs; or in the form of fractures at the junction of pedicle and vertebral body on CT scans or in the form of disease process causing osteolysis of the entire pedicle[s] on axial images of CT [Figure 1A, B and C]. For the purpose of assigning scores for the location component of SINS, majority of tuberculous lesions being paradiscal, involvement of endplates was an important determinant. As an illustration, a patient with paradiscal involvement at L4-5 with intact inferior endplate of L5 was assigned location as “mobile spine” rather than “junctional”. For purposes of identifying radiographic spinal alignment, loss of normal lordosis in the lumbar or cervical spine too, was assigned a score of “2”. For assessment of vertebral body collapse in patients with multiple contiguous vertebral body involvement, collapse of each of those individual vertebral bodies was assessed and then summed up so as to as to assess for >50% or <50% collapse. Contiguous lesions were marked in total whereas skip lesions were scored individually. As an illustration, if a patient had a lesion involving T10, 11 and 12; a single SINS score was calculated for this lesion spread over 3 vertebrae. On the other hand, if a patient had a lesion at L2 and another at T6, 2 SINS scores were calculated for each of these 2 lesions.
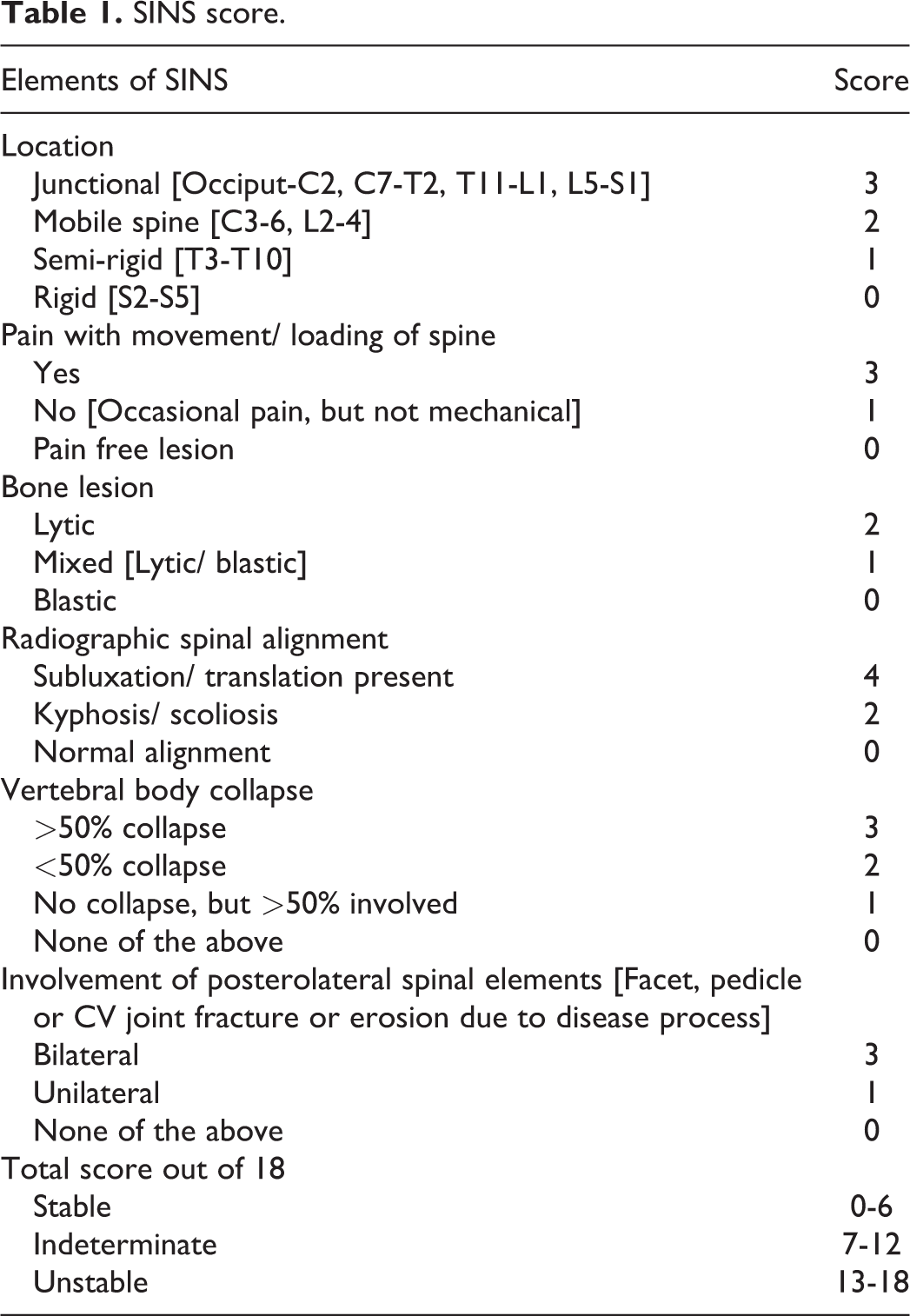
SINS score.
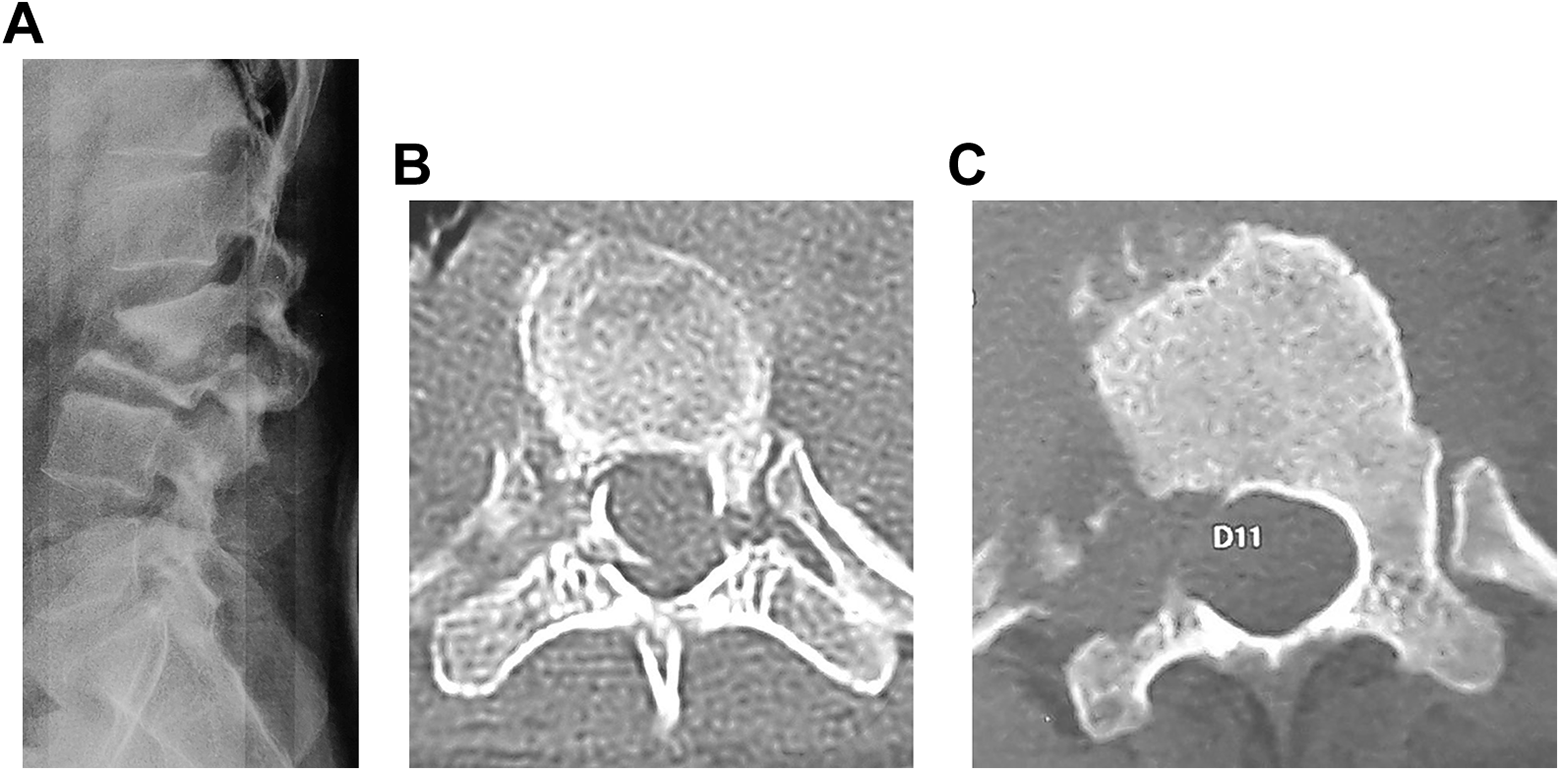
Assessment of involvement of posterolateral spinal elements for SINS scoring. A, Subluxation of facets seen on lateral plain radiographs. B, Fracture at the junction of pedicle with vertebral body on axial CT scan. C, Osteolysis of pedicle see on axial CT scan.
Inter and intra observer variability for the SINS scoring in the specific context of spinal tuberculosis was done for various components of the scoring system. Two sets of values were obtained for the same set of radiological investigations and clinical findings from a single observer [VSR] at an interval of 1 week. These were used to assess intra-observer variability. First measurement by the first observer [VSR] was compared with a single measurement made by another observer [YKP]. This was used to generate inter observer variability.
Patients classified as those with “indeterminate stability” as per the SINS criteria, were managed with or without surgery based on other parameters. Detailed counseling was done by the senior author [YKP] with these patients as regard risks and benefits for non-surgical and surgical interventions and an informed decision for further treatment plan was taken. Factors considered to decide for or against surgery in the indeterminate group included neurological status, severity of pain, failure to respond to non-operative treatment, medical comorbidities and consequent fitness for surgery, drug resistance, ambiguous percutaneous biopsy report and lastly, financial constraints, which can be a strong influencing factor in developing and under-developed countries.
Statistical analysis was done using software: Graphpad Instat, version 3.10. Power was calculated using an R package “pwr” in R 4.0.5 version. Data following Gaussian distribution was presented as mean with standard deviation and analyzed by parametric tests. Data following non-Gaussian distribution was presented as median with range in parentheses and analyzed by nonparametric tests [Wilcoxon matched-pairs signed-ranks test]. Significance was set at 2-tailed P < .05. Inter and inter-observer variability was assessed using Cohen’s kappa coefficients.
Results
Eighty [39 males, 41 females] patients with mean age 46.74 ± 17.3 years were prospectively evaluated. Diagnosis of tuberculosis was confirmed on the basis of molecular diagnostics [GenExpert] and histopathology. 8 In 7 patients in whom diagnosis could not be established on this basis, it was presumed to be tuberculosis on the basis of corroboration of clinical and radiological features along with positive response to anti-tuberculous chemotherapy as well as the fact that no other causative factor could be detected in the tests conducted. 8 All patients received anti-tuberculous chemotherapy as per WHO guidelines. 9 There were no drug-resistant cases in the present series.
With the mean SINS score of these 80 patients being 11.2375 and the standard deviation of the group being 3.3762, the sample size had a statistical power of 99.3% with the significance level set at P < .05.
Classification was done into stable [n = 7], indeterminate [n = 45] and unstable [n = 28] groups based on total SINS score [Table 1]. SINS scoring system had intra and inter-observer correlation coefficients of 0.980 and 0.949, respectively, determining the close association of the 2 sets of observations. None of the 7 patients in stable group were treated with surgical stabilization. However, 1 patient with L2-3 paradiscal lesion presenting with severe radiculopathy was operated upon with just a decompression surgery to alleviate the same [Figure 2]. Another patient with C2 lesion had a large retropharyngeal abscess without any structural instability [Figure 3]. Since the retropharyngeal abscess was causing pressure symptoms, it was drained appropriately. All patients in the unstable group underwent surgical stabilization. Transpedicular decompression was carried out in the patients with neurological deficits.

Patient with L2-3 lesion, classified as “stable” on SINS score, but was operated upon for decompression in view of severe radicular pain.

Patient with C2 lesion, classified as “stable” on SINS score, but was operated upon for drainage of retropharyngeal abscess due to mass effect.
Among the 45 patients classified in the indeterminate group, 26 patients underwent surgery while the other 19 were managed non-operatively. Of the 26 patients undergoing surgery in this indeterminate group, 14 patients opted for surgical intervention in view of severe activity-related pains while 11 patients underwent surgery for neurological reasons; either significant neurological deficit at the time of initial presentation itself or neurological deterioration while on non-operative treatment. One patient underwent surgery in this group as his percutaneous biopsy report was inconclusive and the morphology of his MRI was atypical, resembling neoplasm and hence, decision for surgical intervention was taken [Figure 4]. Among the 19 patients in this indeterminate group that were managed non-operatively, 1 patient had evidence of lateral listhesis on presentation radiographs. However, she did not have significant activity-related pains and her total SINS score was 12. In view of this, surgical stabilization was considered as a relative and not an absolute indication in her case. In view of financial constraints, a decision for non-operative treatment was taken and was found to be fruitful [Figure 5].

Patient with thoracic tuberculous lesion, classified as “indeterminate” on SINS score, but had an inconclusive report on percutaneous biopsy. Hence, was operated upon with open biopsy and surgical stabilization as the MRI picture looked more like that of neoplasm than that of tuberculosis.
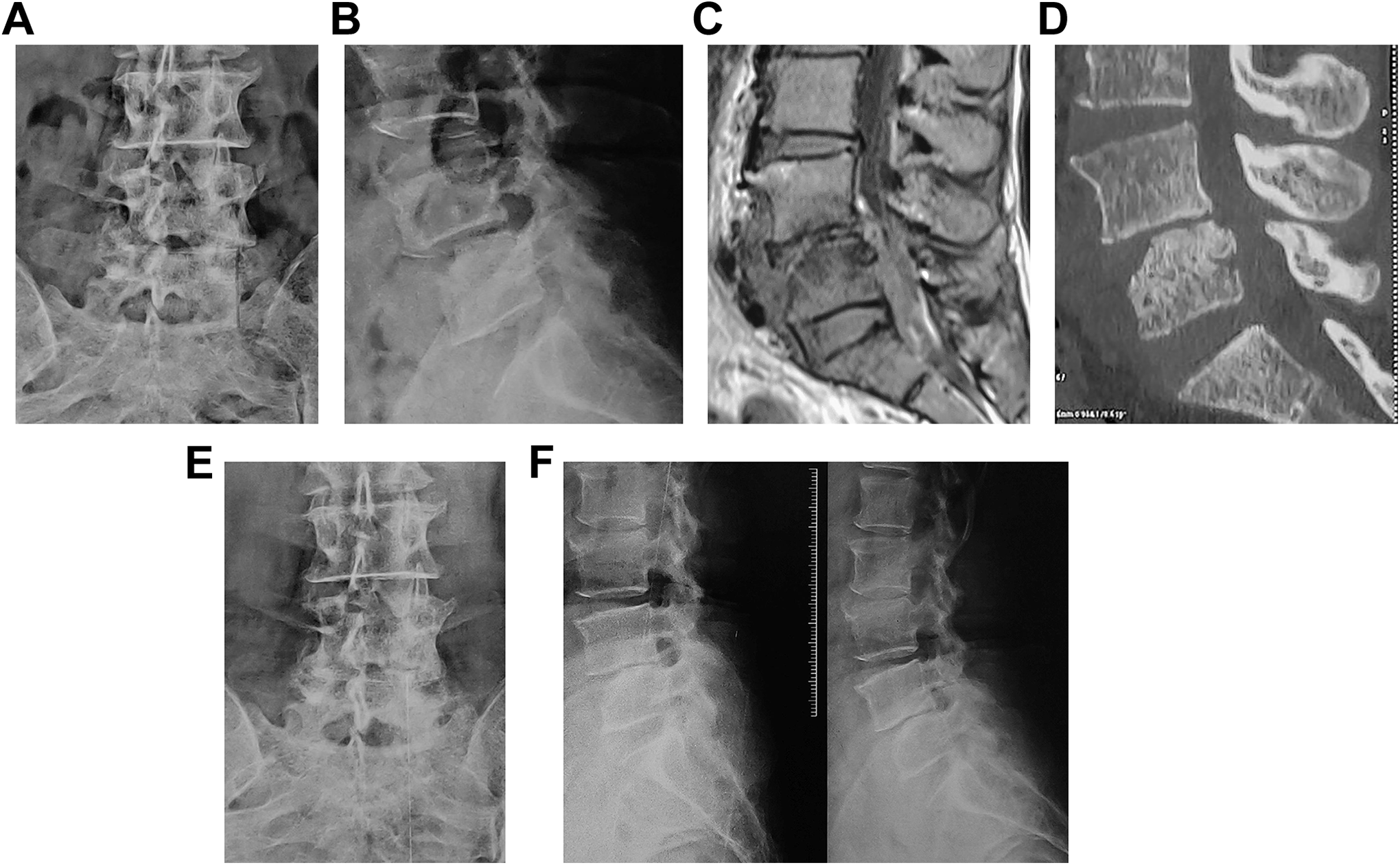
Patient with L4-5 tuberculous lesion, classified as “indeterminate” on SINS score, with financial constraints, managed with non-operative treatment. A, Anteroposterior radiograph at presentation demonstrating lateral listhesis. B, Lateral radiograph at presentation demonstrating anteroposterior listhesis. C, MRI showing paradiscal tuberculous lesion. D, CT scan showing absence of significant osteolysis. E, Post-treatment anteroposterior radiograph showing absence of any further deterioration of the lateral listhesis. F, Post-treatment flexion-extension radiographs showing absence of any instability.
Patients were followed up for 38.5 ± 22.61 months with minimum follow-up being 24 months. One patient expired on fifth postoperative day due to cardiac arrest due to pre-existing morbidities. Preoperative VAS score for pain improved from median of 9/10 to 1/10 post-surgery [P < .0001, Wilcoxon matched-pairs signed-ranks test]. In non-operative group, improvement was from median score of 6/10 to 1/10 [P < .0001, Wilcoxon matched-pairs signed-ranks test]. Preoperative ODI improved in non-operative and operative group from median of 42% and 70%, respectively to 10% and 12%, respectively in postoperative period [P < .0001 for both groups, Wilcoxon matched-pairs signed-ranks test]. As per Macnab’s criteria, 26 patients had excellent while 53 had good outcomes.
Discussion
The global tuberculosis report published by WHO in 2020 states that 88% of people who developed tuberculosis in 2019 were people aged more than 15 years. 10 This clearly demonstrates that spinal tuberculosis has become more of an adult disease. However, as already mentioned at the outset, there is a glaring deficiency in literature on unequivocal guidelines to objectively define instability in adult spinal tuberculosis. Oguz et al classified a patient as unstable only on the basis of kyphosis [sagittal index ≥200]. 11 As a result, they offered surgery to 71 out of 76 patients with spinal tuberculosis presenting to them. On the other hand, Nene A and Bhojraj S published their series of 70 patients with thoracic spinal tuberculosis out of which they successfully treated 69 patients without surgery. 12 This wide variability in surgical indications is to a great extent contributed by lack of clarity in defining instability in adult spinal tuberculosis.
In the past, attempts have been made to identify instability in spinal tuberculosis using various criteria. Mehta and Bhojraj attempted to classify surgical strategies based on MRI assessment. 4 However, there is a risk of over-estimation of the problem on MRI. 13 Spinal instability features can be assessed on a common platform for both neoplasm and infection as both tend to develop over a period of time as compared to the instantaneous disruption of spinal stability in trauma6. Hence, the authors extrapolated the use of SINS score, originally contemplated to define instability in neoplasm, as an option to evaluate instability in spinal tuberculosis as well.
The present study involved application of SINS score toward decision-making for surgical stabilization in 80 patients. It allowed unequivocal guideline in 35 of these patients in terms of whether surgical stabilization is mandatory. Appropriate management along these principles led to satisfactory outcomes in these patients. For the 45 patients in the indeterminate group, decision-making for or against surgical stabilization involved incorporation of other factors such as severe neurological deficit on initial presentation or deterioration of neurological status while on treatment. 8 Severity of pain was another important determinant to decide for or against surgery. Mechanical pains related to activity, particularly posture change, significantly influenced the decision for surgery in as many as 14 out of the 26 patients opting for surgery in the indeterminate group. Hence, pain was the single most important subjective factor from patient’s perspective to determine the need for surgery in the indeterminate group. This finding is commensurate with the original definition of instability by White and Panjabi which defined instability as a condition causing incapacitating pain during posture change. 14 Failure to respond to non-operative treatment was another obvious parameter that swung the decision toward surgical intervention in this indeterminate group. Though the present study did not involve any patients with drug resistance, the authors contemplate that a patient in the indeterminate group with proven drug resistance should preferably be operated upon so as to reduce the bacterial load and improve vascularity in the area by debriding the necrotic tissues. 15 Patients with ambiguous percutaneous biopsy report [Figure 4] in the indeterminate group, would also qualify for surgical intervention so as to allow for a proper open biopsy and appropriate surgical stabilization. Presence of medical comorbidities affecting fitness to undergo surgery, and lastly, financial constraints, which can be a strong influencing factor in developing and under-developed countries were the other additional factors considered by the authors to decide for or against surgery in the indeterminate group. As evinced by the results of case no. 39 [Figure 5], this approach led to a satisfactory outcome. A pragmatic approach to decision-making in this indeterminate group involving discussions with the patients allowed for optimal outcome in the present study.
Though the authors found extrapolation of SINS score toward evaluation of instability in spinal tuberculosis to be quite fruitful, there exist some differences between the 2 entities in the application of this score. Majority of neoplastic lesions originate in the vertebral body while majority of tuberculous lesions are paradiscal. Hence, particular attention has to be paid while assigning scores for the location. L4-5 paradiscal lesion would be labeled as a lesion in mobile spine while L5-S1 paradiscal lesion would be labeled as that in a junctional area. It also needs to be noted that there is scope for further refinement of the SINS score for its extrapolation to use in spinal tuberculosis. The fact that patients with spinal tuberculosis often present with vertebral body collapse involving multiple levels makes it necessary to have an option for increasing the options for scoring under the category of vertebral body collapse from >50% to more than one or two vertebral bodies and obviously, correspondingly increase the points assigned to this parameter. Also, it is interesting to note that the majority of patients [14 of 26] in the indeterminate group opted for surgery purely on the basis of mechanical pains. In fact, even for neoplastic lesions, de Andrade et al noted that pain was the most important determinant for surgery in their analysis of 40 patients. 16 Hence, further refinement of this score may be done by ascribing more points to the pain parameter so as to ultimately shrink the number of patients falling in indeterminate group and have a more objective unambiguous classification into stable or unstable groups.
To conclude, the authors found SINS score to be a useful objective decision-making tool in assessing the need for surgical intervention in patients with spinal tuberculosis. Decision for surgery in the indeterminate group defined by SINS score was taken on the basis of multiple factors; neurological status and pain being the most prominent ones. Further refinement of this score for the purpose of spinal tuberculosis may incorporate widening of options in the domain of vertebral collapse and ascribing more points to mechanical pains.
Footnotes
Authors’ Note
Institute where the scientific study was carried out: HOSMAT Hospital, Bengaluru, India.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.