
Abstract
Study Design
Retrospective cohort study.
Objectives
To investigate the influence of spontaneous C2-3 interlaminar bony fusion on the long-term progression of ossification of the posterior longitudinal ligament (OPLL), and to assess its associated clinical and radiologic consequences following cervical laminoplasty.
Methods
Patients who underwent cervical laminoplasty for myelopathy due to multilevel OPLL involving the C2-3 level and were followed for ≥5 years were analyzed. Patients were classified according to the presence of C2-3 interlaminar fusion. OPLL progression (anteroposterior [AP] and sagittal diameters), cervical range of motion (ROM), and patient-reported outcomes were compared. Multivariable linear regression and linear mixed-effects modeling assessed the adjusted association between fusion status and OPLL progression over time, controlling for key covariates.
Results
Forty-nine patients met inclusion criteria. C2-3 interlaminar fusion independently predicted reduced AP (β = −1.439, P = .0031) and sagittal (β = −8.725, P = .0007) progression after adjustment for all confounders. Mixed-effects modeling confirmed a significantly flatter long-term progression trajectory in patients with interlaminar fusion. C2-7 ROM and patient-reported outcomes were comparable between groups.
Conclusions
Spontaneous C2-3 interlaminar fusion is associated with attenuation of postoperative OPLL progression without compromising overall cervical motion or clinical outcomes. These findings suggest that C2-3 interlaminar fusion may function as a stabilizing postoperative phenomenon rather than an unfavorable radiologic change following cervical laminoplasty in multilevel OPLL patients.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a progressive disorder that causes cervical myelopathy through ectopic bone formation within the spinal canal.1,2 Cervical laminoplasty provides effective multilevel decompression while preserving motion and posterior elements. 3 However, because the ossified mass is not directly removed, residual OPLL often continues to enlarge postoperatively, sometimes resulting in delayed neurologic deterioration.4–6 Excessive cervical range of motion (ROM) has been consistently associated with postoperative OPLL progression.7–10
Interlaminar bony fusion commonly develops after laminoplasty, most often at C2-3 level.11,12 Although conventionally viewed as a complication due to reduced segmental motion or alignment changes, its biomechanical significance remains uncertain. Experimental studies suggest that mechanical stress promotes ossification through osteogenic signaling pathways 13 ; therefore, spontaneous C2-3 interlaminar fusion could plausibly exert a stabilizing effect that limits postoperative OPLL progression. However, this potential relationship has not been systematically investigated.
We evaluated whether spontaneous C2-3 interlaminar bony fusion following cervical laminoplasty is associated with reduced OPLL progression and examined its influence on long-term radiologic and clinical outcomes.
Materials and Methods
Study Design and Population
Following institutional review board approval, a retrospective cohort study was conducted of consecutive patients who underwent cervical laminoplasty for cervical myelopathy caused by multilevel OPLL extending to the C2 level between 2014 and 2020. Eligible patients had complete radiologic and clinical data at baseline and at 1-, 2-, and ≥5-year follow-up. Exclusion criteria included surgery for non-OPLL pathology and cases in which OPLL did not involve the C2-3 level (Figure 1). The requirement for informed consent was waived owing to the retrospective study design. Flow diagram of patient selection for this study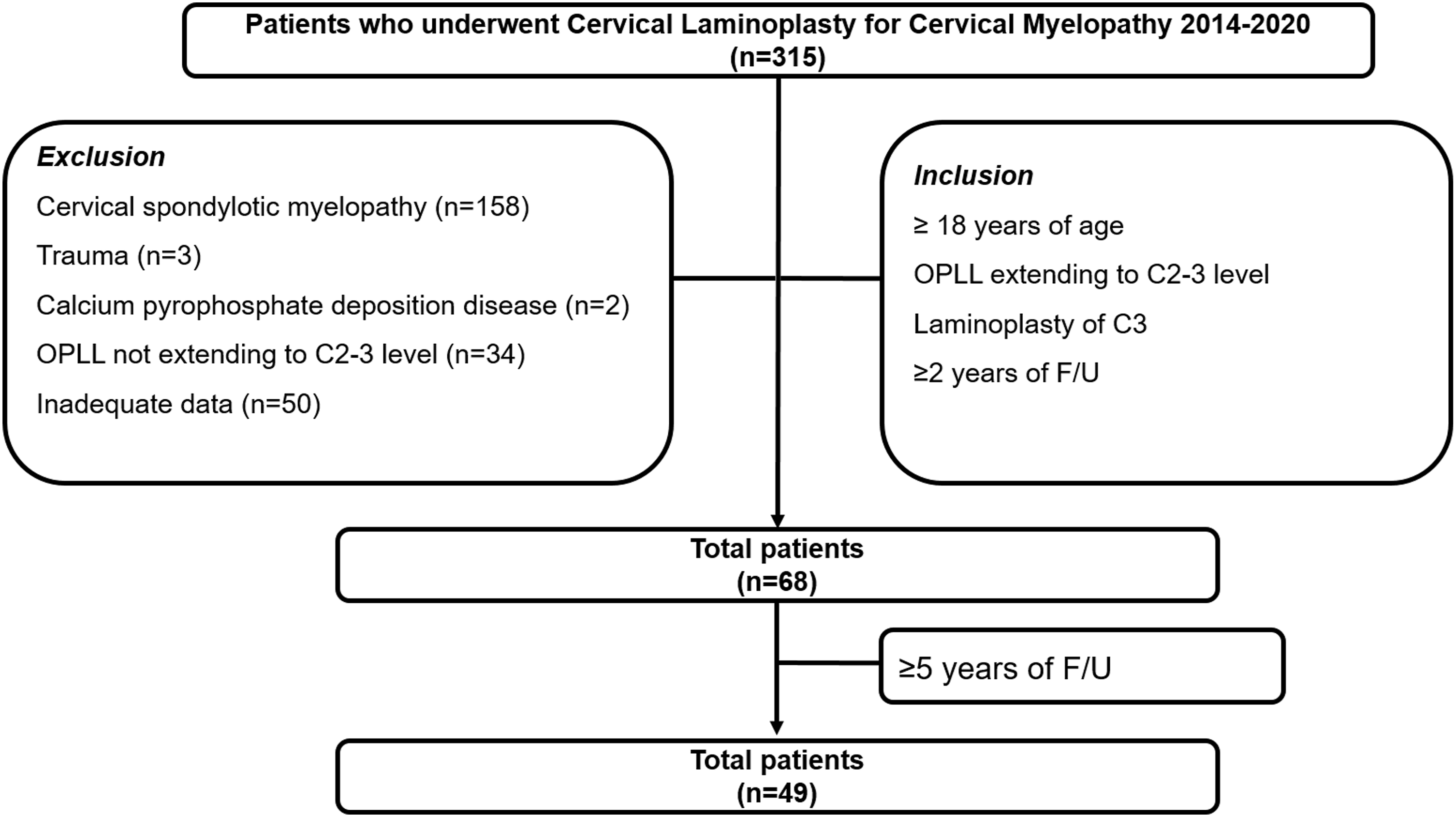
Surgical Technique
All patients underwent conventional open-door laminoplasty using mini-plates and screws. The decompression levels were selected according to the extent of the ossified lesion. The semispinalis cervicis attachment to C2 was preserved whenever possible. At the C2-3 level, either the C2 lamina was preserved or a dome-like expansive laminoplasty was performed at C2, followed by open-door laminoplasty at C3. No fixation or fusion procedures were intentionally performed. All patients wore a cervical collar for 6 weeks postoperatively.
Radiologic Assessments
Dynamic lateral cervical radiographs and computed tomography (CT) scans were obtained at baseline and at 1, 2, and ≥5 years postoperatively. C2-3 interlaminar bony fusion was defined as the presence of bony bridging with <1 mm interspinous motion on dynamic radiographs.
14
OPLL diameters were measured in both the anteroposterior (AP) and sagittal dimensions on sagittal CT images. The AP diameter was defined as the distance from the posterior cortex of the C3 vertebral body to the posterior margin of the ossified mass, and the sagittal diameter as the vertical distance from the C3 upper endplate to the OPLL apex (Figure 2). OPLL progression was defined as an increase in each diameter from baseline. Segmental motion at C2-3 and global C2-7 ROM were assessed on flexion-extension radiographs. Two blinded observers independently performed all measurements, and the mean of their values was used for analysis. Interobserver reliability for OPLL progression measurements was evaluated using intraclass correlation coefficients (ICC). Measurement of ossification of the posterior longitudinal ligament (OPLL) diameters on sagittal CT images.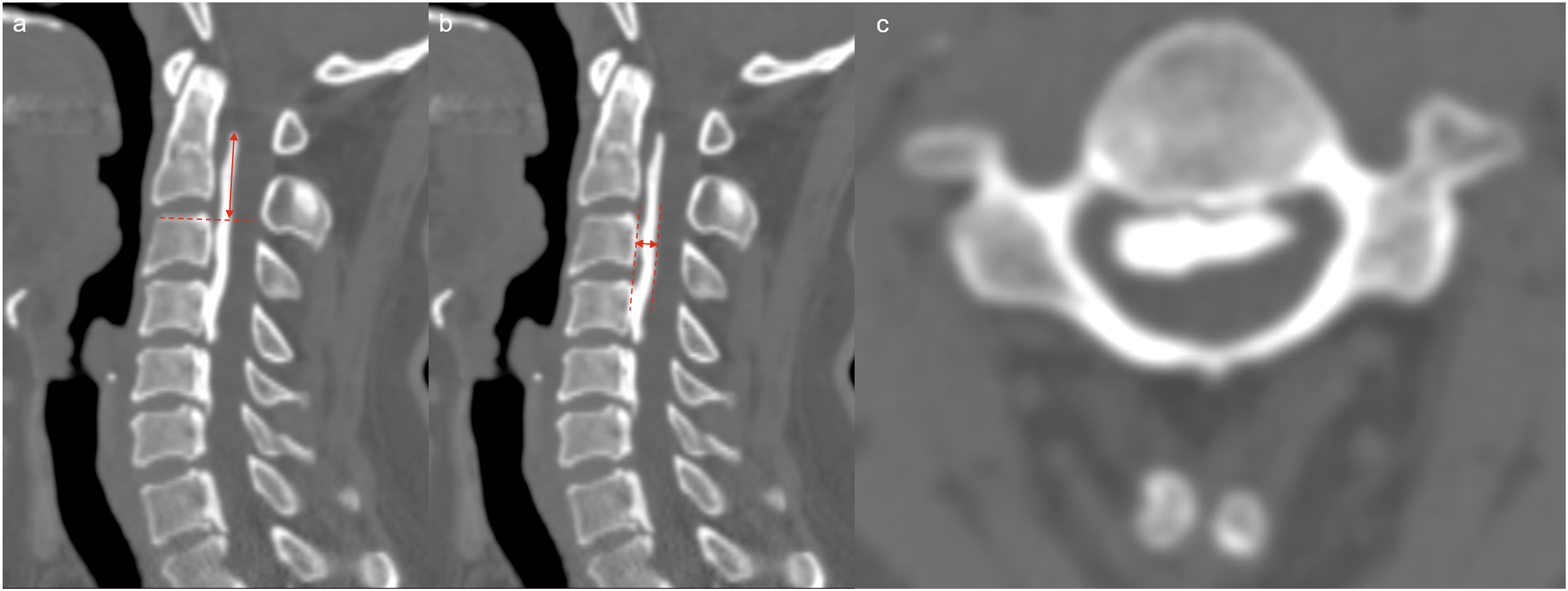
Clinical Outcomes
Patient-reported outcomes included visual analog scale (VAS) scores for neck and arm pain, Neck Disability Index (NDI), Japanese Orthopaedic Association (JOA) score, JOA recovery rate (as described by Hirabayashi et al 15 ), and EuroQol 5-Dimension visual analog scale (EQ-5D VAS). The NDI score was converted into a percentage to accommodate non-drivers. All assessments were performed at each follow-up time point.
Statistical Analysis
Patients were classified according to the presence or absence of C2-3 interlaminar fusion at each follow-up interval. Baseline characteristics were compared using chi-square or Fisher’s exact tests for categorical variables and t-tests or Wilcoxon rank-sum tests for continuous variables, as appropriate.
Longitudinal comparisons of OPLL progression, ROM, and clinical outcomes at 1, 2, and ≥5 years were performed. Multivariable linear regression analyses evaluated the association between C2-3 interlaminar fusion and OPLL progression, adjusting for demographic, surgical, and radiologic covariates, including age, sex, body mass index (BMI), smoking status, OPLL type at the C2-3 level, presence of ossification of anterior longitudinal ligament (OALL) at C2-3, immediate postoperative C2-3 contact, C2 dome laminoplasty, number of laminoplasty levels, baseline OPLL size (AP and sagittal), preoperative C2-3 and C2-7 ROM, and fusion other than interlaminar fusion (including fusion caused by OALL and direct OPLL bridging) at each follow-up. OPLL type was assessed at the C2-3 level because the primary objective of the study was to evaluate the association between C2-3 interlaminar fusion and OPLL progression at the same segment.
Linear mixed-effects models were fitted with random intercepts for patients and fixed effects for time (1, 2, and ≥5 years), interlaminar fusion status (fusion vs no fusion), and their interaction. Models were adjusted for the same covariates used in regression analyses, including baseline OPLL size as an ANCOVA covariate. Estimated marginal means were obtained, and within-time contrasts between fusion groups were tested using appropriate degrees-of-freedom approximations.
All analyses were performed using R (version 4.5.0; R Foundation for Statistical Computing, Vienna, Austria), with statistical significance defined as P < .05.
Results
Baseline Characteristics
Baseline Characteristics According to Interlaminar Fusion at Postoperative ≥5 years
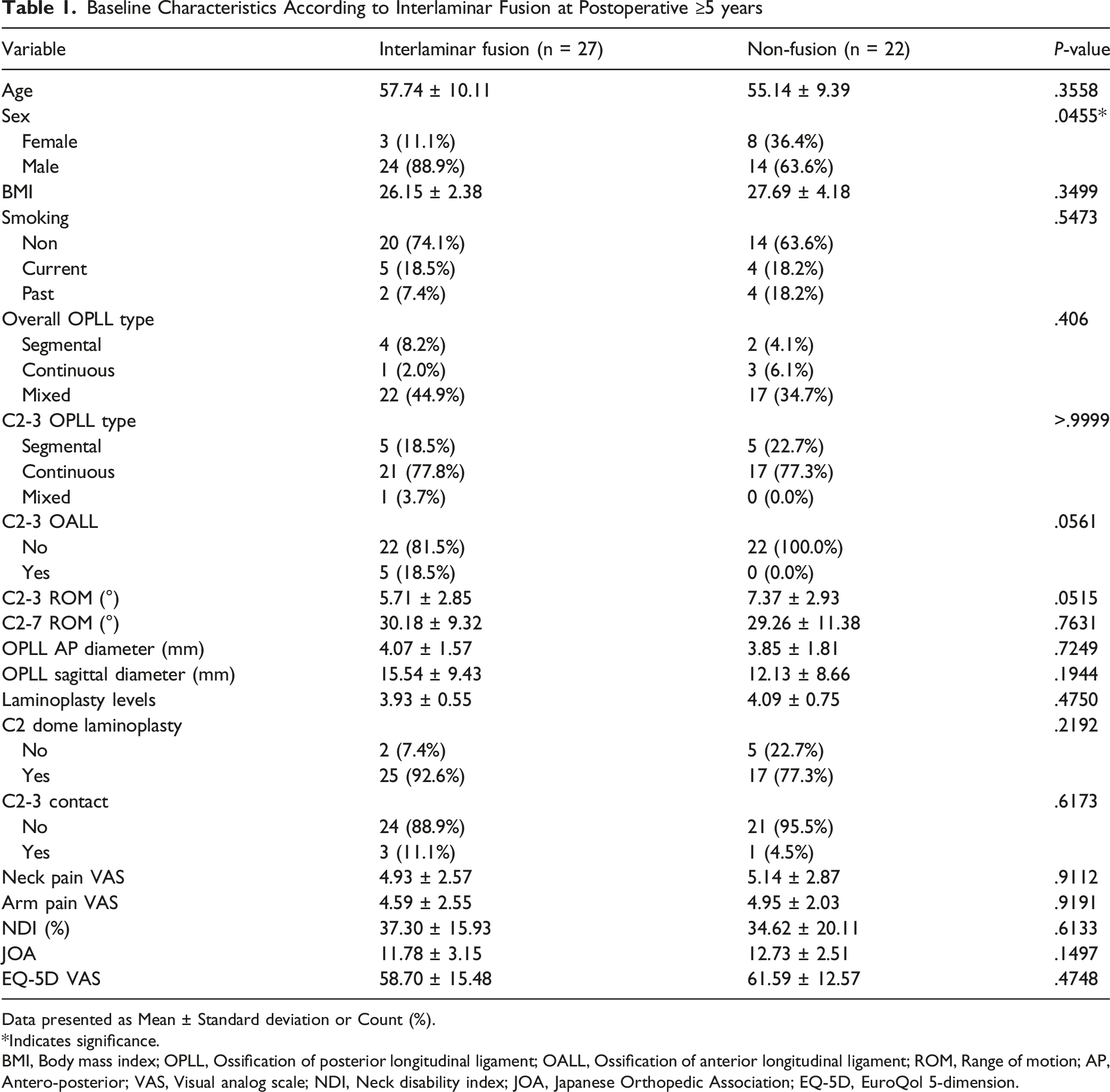
Data presented as Mean ± Standard deviation or Count (%).
*Indicates significance.
BMI, Body mass index; OPLL, Ossification of posterior longitudinal ligament; OALL, Ossification of anterior longitudinal ligament; ROM, Range of motion; AP, Antero-posterior; VAS, Visual analog scale; NDI, Neck disability index; JOA, Japanese Orthopedic Association; EQ-5D, EuroQol 5-dimension.
Radiologic and Clinical Outcomes
Comparison of OPLL Progression, Radiologic, and Clinical Outcome at Postoperative 1 year
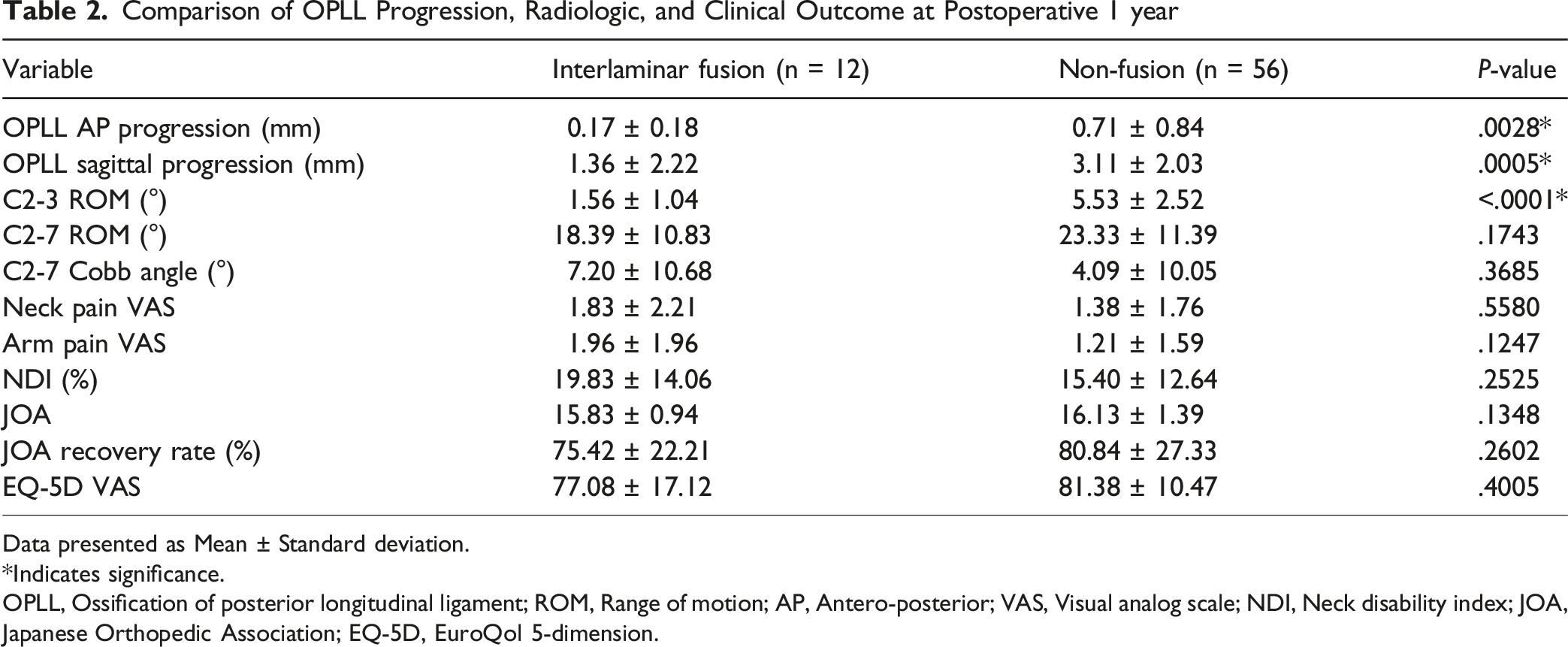
Data presented as Mean ± Standard deviation.
*Indicates significance.
OPLL, Ossification of posterior longitudinal ligament; ROM, Range of motion; AP, Antero-posterior; VAS, Visual analog scale; NDI, Neck disability index; JOA, Japanese Orthopedic Association; EQ-5D, EuroQol 5-dimension.
Comparison of OPLL Progression, Radiologic, and Clinical Outcome at Postoperative 2 years
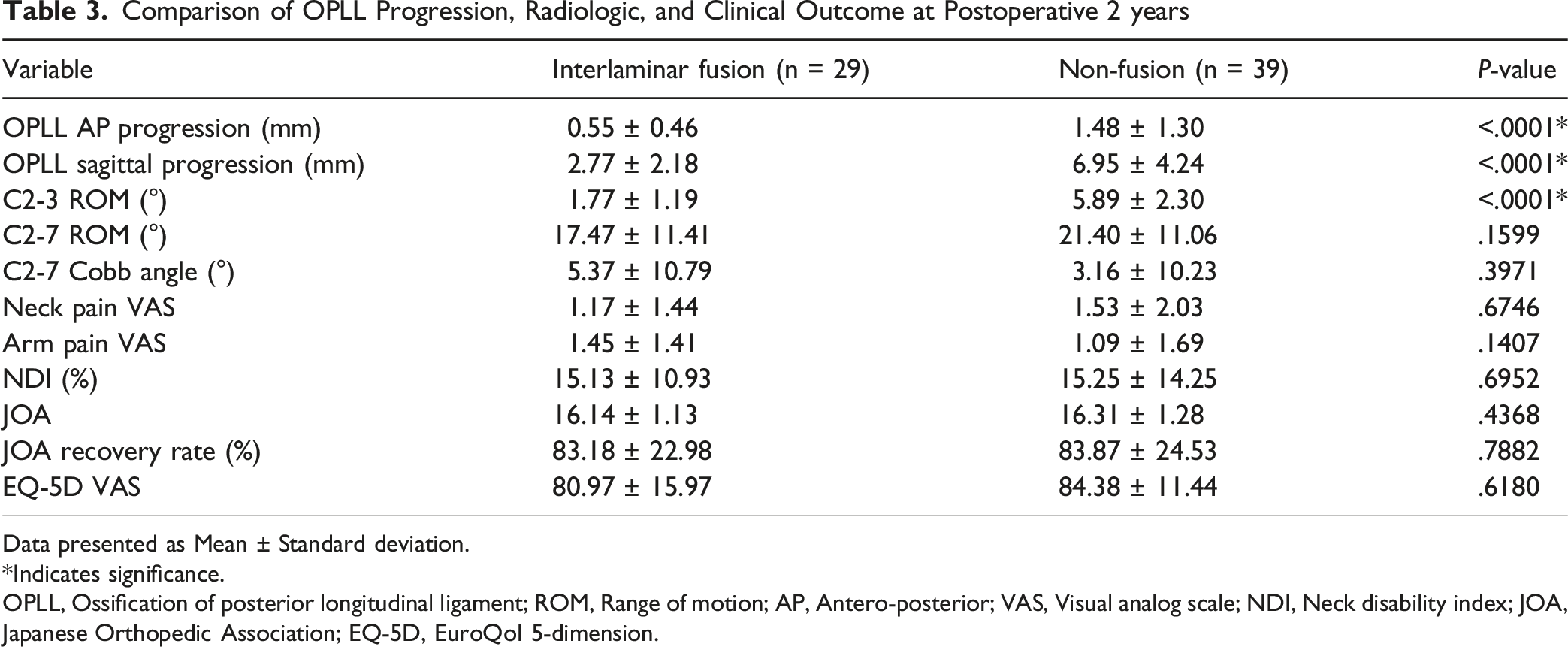
Data presented as Mean ± Standard deviation.
*Indicates significance.
OPLL, Ossification of posterior longitudinal ligament; ROM, Range of motion; AP, Antero-posterior; VAS, Visual analog scale; NDI, Neck disability index; JOA, Japanese Orthopedic Association; EQ-5D, EuroQol 5-dimension.
Comparison of OPLL Progression, Radiologic, and Clinical Outcome at Postoperative ≥5 years
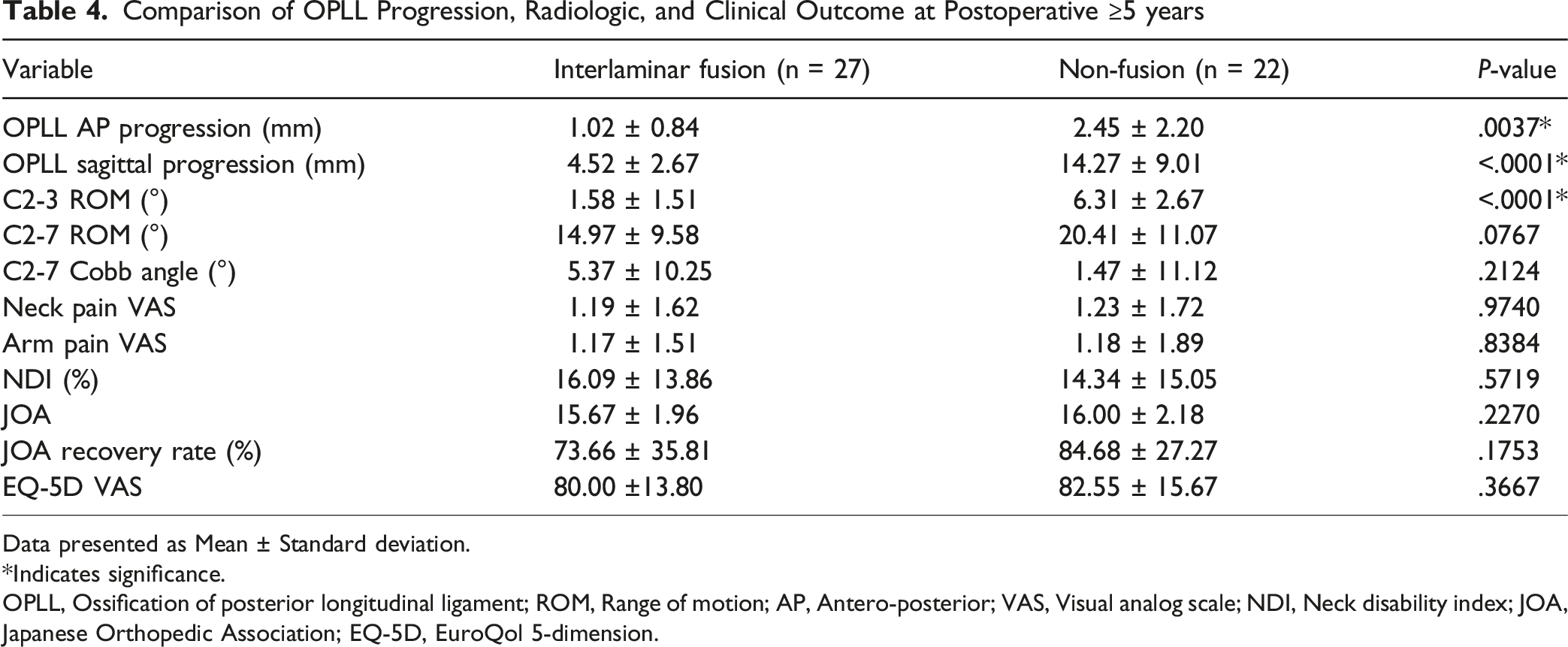
Data presented as Mean ± Standard deviation.
*Indicates significance.
OPLL, Ossification of posterior longitudinal ligament; ROM, Range of motion; AP, Antero-posterior; VAS, Visual analog scale; NDI, Neck disability index; JOA, Japanese Orthopedic Association; EQ-5D, EuroQol 5-dimension.
Multivariable Regression Analysis
After adjustment for demographic, surgical, and radiologic variables, C2-3 interlaminar fusion remained an independent predictor of reduced OPLL progression across all follow-up periods.
Predictors Affecting OPLL Progression
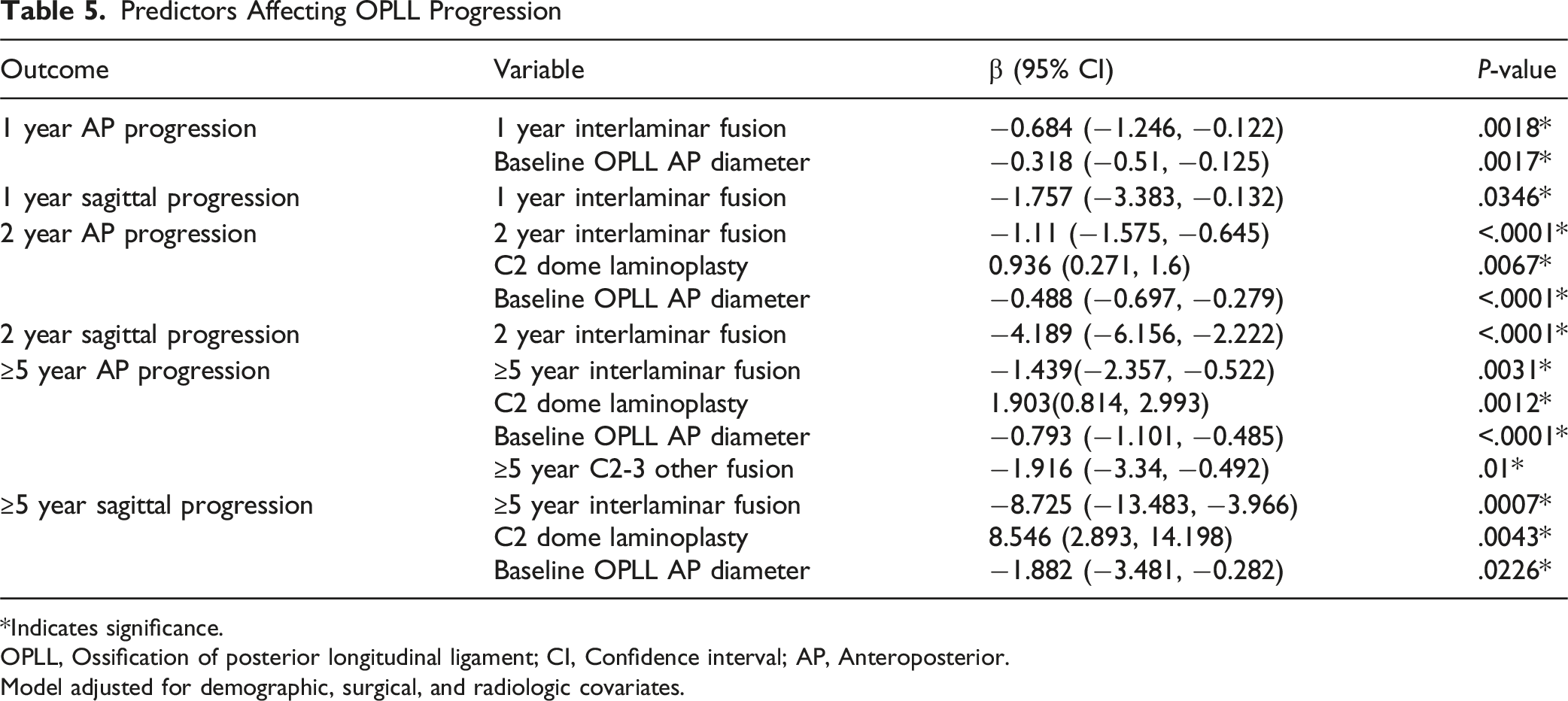
*Indicates significance.
OPLL, Ossification of posterior longitudinal ligament; CI, Confidence interval; AP, Anteroposterior.
Model adjusted for demographic, surgical, and radiologic covariates.
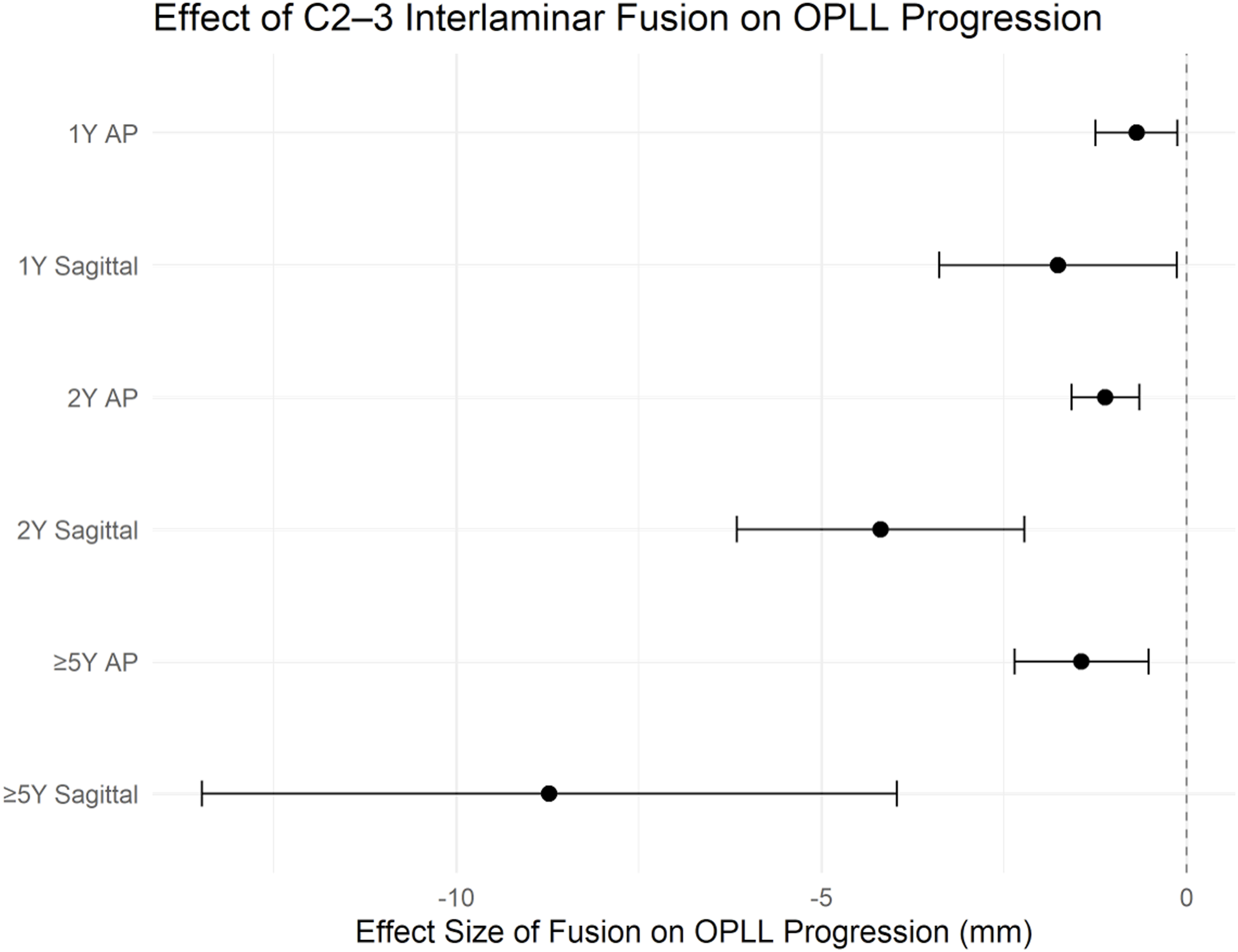
Forest plot illustrating the adjusted effect of C2-3 interlaminar bony fusion on OPLL progression in AP and sagittal dimensions at 1, 2, and ≥5 years. Values represent regression coefficients with 95% confidence intervals
C2 dome laminoplasty was associated with greater AP progression at 2 years (β = 0.936, 95% CI: 0.271 to 1.600, P = .0067) and with increased AP (β = 1.903, 95% CI: 0.814 to 2.993, P = .0012) and sagittal (β = 8.546, 95% CI: 2.893 to 14.198, P = .0043) progression at ≥5 years. Baseline OPLL AP diameter was an independent inverse predictor of AP progression across all time points (1 year: β = −0.318, 95% CI: −0.510 to −0.125, P = .0017; 2 years: β = −0.488, 95% CI: −0.697 to −0.279, P < .0001; ≥5 years: β = −0.793, 95% CI: −1.101 to −0.485, P < .0001) and of sagittal progression at ≥5 years (β = −1.882, 95% CI: −3.481 to −0.282, P = .0226). Fusion other than interlaminar fusion at ≥5 years was also associated with reduced AP progression (β = −1.916, 95% CI: −3.340 to −0.492, P = .010) (Table 5).
Full model coefficients and confidence intervals are provided in the Supplementary Materials.
Mixed-Effects Model
Adjusted trajectories (Figure 4) showed that OPLL progression occurred over time in both groups but with a markedly flatter slope in patients with interlaminar fusion. In the AP dimension, the difference between fusion and non-fusion groups was not significant at 1 year but became significant at 2 years and remained so at ≥5 years. In the sagittal dimension, divergence was greater, with significant between-group differences evident from 2 years onward. Numerical estimated marginal means and within-time contrasts are presented in the Supplementary Materials. Adjusted C2-3 OPLL diameters by time and fusion status. Error bars: 95% confidence intervals. The bottom strip shows the number of patients per time × group. Baseline is not plotted because it is included as a covariate, and no patient was fused at baseline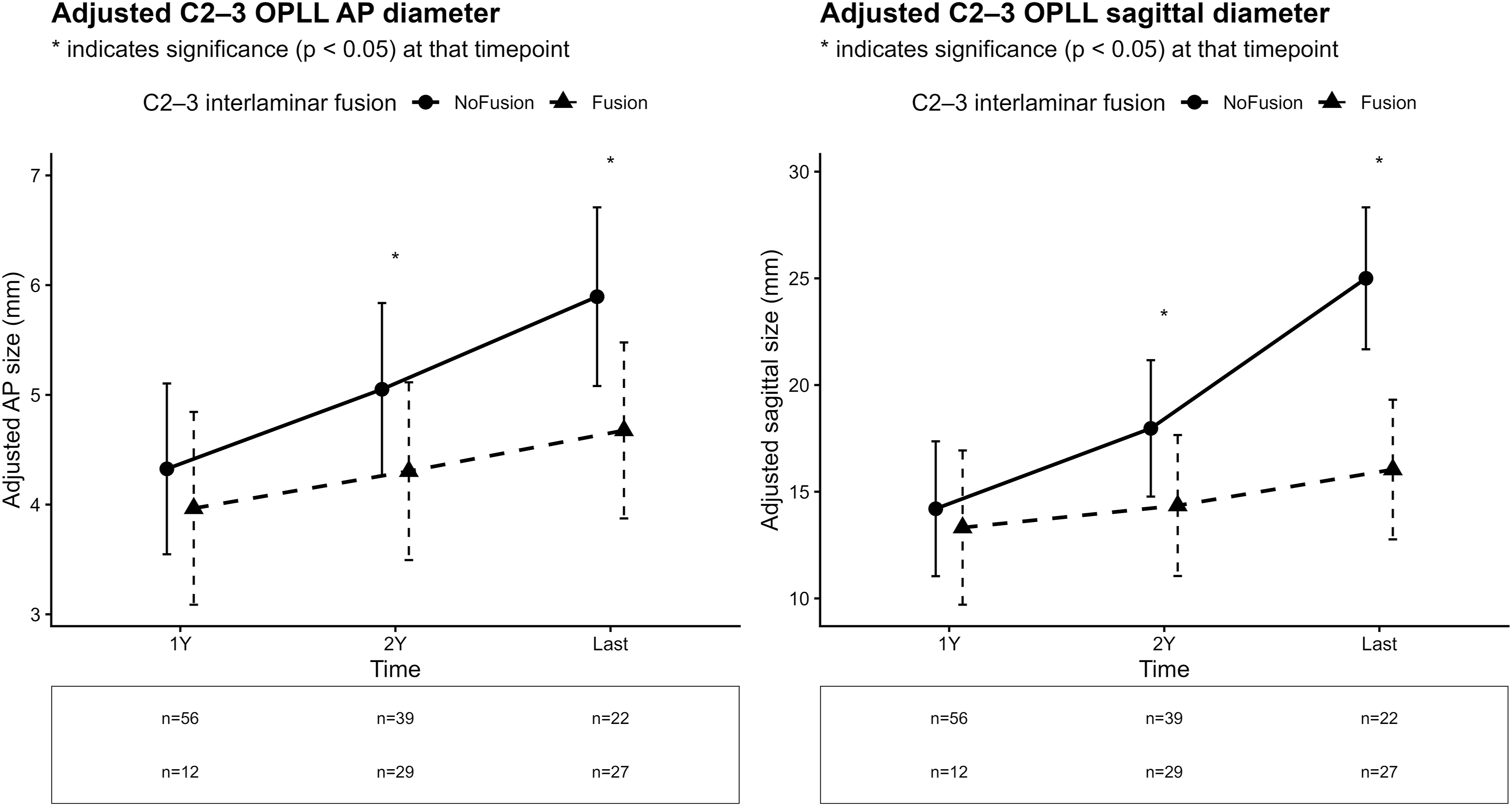
Illustrative Case
An illustrative case demonstrating C2-3 interlaminar fusion with minimal OPLL progression is shown in Figure 5. Illustrative case demonstrating differences in OPLL progression (A, B) Sagittal CT images of a patient without C2-3 interlaminar fusion, showing marked OPLL progression over time. (C, D) Sagittal CT images of a patient with C2-3 interlaminar bony fusion (white arrow), demonstrating minimal progression during the same follow-up period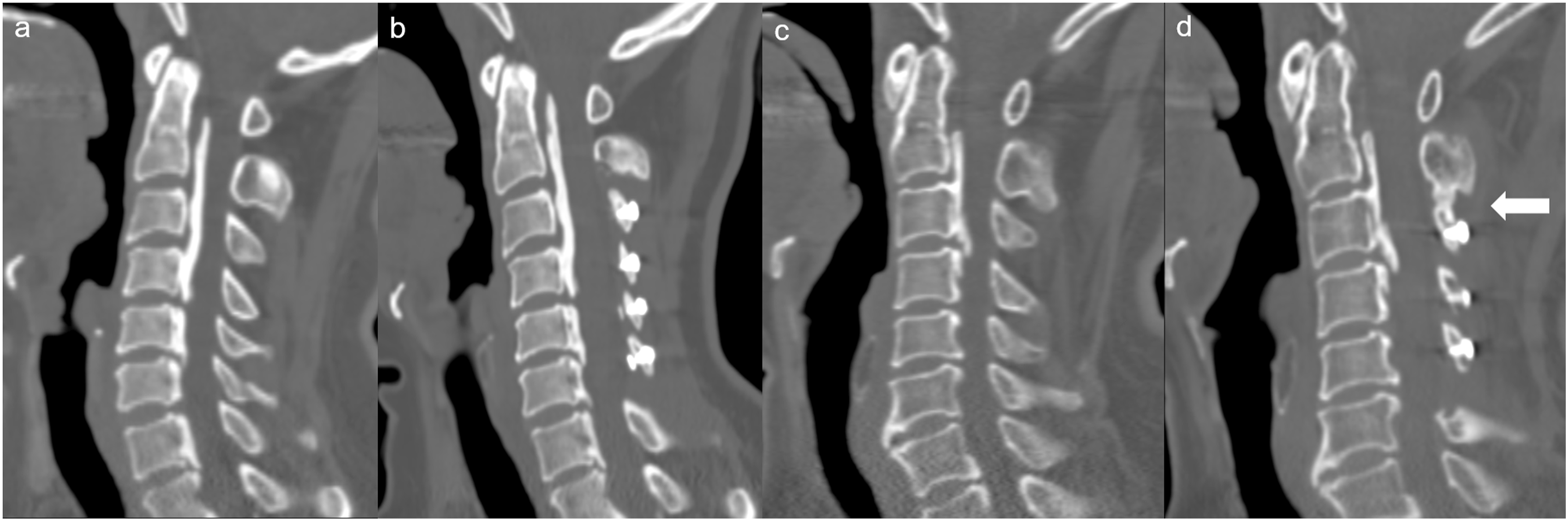
Discussion
This study demonstrated that spontaneous C2-3 interlaminar bony fusion following cervical laminoplasty independently mitigates postoperative OPLL progression over long-term follow-up, without compromising overall cervical motion or clinical outcomes. The protective association was consistent across all postoperative time points and remained robust after multivariable adjustment and longitudinal mixed-effects modeling.
Cervical OPLL has been reported to progress both during the natural course and after surgery. 10 Posterior surgeries, including laminoplasty and laminectomy with fusion are the preferred treatments for multilevel OPLL involving three or more levels. Because these procedures do not directly remove the ossified mass, residual lesions remain susceptible to further progression and potential neurological deterioration.4,6 Previous studies have identified several risk factors for OPLL progression, including younger age, multilevel involvement, and mixed or continuous OPLL types.10,16,17 Segmental motion is another well-established contributor, with progression reported to be more prominent after laminoplasty than after laminectomy and fusion.7,18 Mechanical stress is believed to promote OPLL progression by inducing osteogenic differentiation in spinal ligament cells and stimulating the expression of bone morphogenic proteins. 13 Conversely, mechanical stabilization appears to suppress this ossification process.8,19
Interlaminar bony fusion following cervical laminoplasty has been reported to occur in 28% to 88% of patients, most commonly at the C2-3 level.11,20 Traditionally it has been regarded as a postoperative complication due to its association with adverse radiologic changes including reduced ROM and loss of cervical lordosis.21,22 To minimize its occurrence, several technical modifications have been proposed, including fat grafting at the interlaminar space, early cervical collar removal after surgery, and performing C3 laminectomy instead of C3 laminoplasty.22–24 However, the present results suggest an alternative interpretation: although interlaminar fusion limits segmental motion at the C2-3 level, it may also confer local mechanical stability that mitigates the dynamic stress contributing to OPLL progression. This interpretation is consistent with prior studies implicating motion as a key driver of OPLL progression.7,8,19 Interlaminar fusion likely restricts motion between adjacent laminae, potentially reducing the biomechanical triggers responsible for further ossification. Notably, the interlaminar fusion and non-fusion groups in our cohort did not differ significantly in age, OPLL type, or extent of involvement, reducing the likelihood of confounding by these established risk factors. At the same time, interlaminar fusion at C2-3 may theoretically influence load distribution or motion at adjacent cervical segments. Because the present analysis focused on OPLL progression at the C2-3 level, such adjacent-segment effects could not be evaluated and warrant further investigation.
An important distinction is that studies reporting reduced ROM after C3 laminoplasty have primarily involved patients with cervical spondylotic myelopathy, rather than those with OPLL.11,22,25 In contrast, investigations that included OPLL patients—either within mixed cohorts or as subgroup analyses focused on OPLL—generally found no significant differences in postoperative ROM.26,27 Our findings are consistent with these observations: although segmental motion at C2-3 was significantly reduced in the interlaminar fusion group, overall C2-7 ROM did not differ between groups. This likely reflects the altered baseline biomechanics in multilevel OPLL, where preexisting ossification already limits mobility.
Clinical outcomes also remained comparable regardless of interlaminar fusion status, consistent with previous reports in OPLL-specific populations.26,27 In our cohort, there were no significant between-group differences in neck or arm pain, NDI, JOA score, JOA recovery rate, or EQ-5D. Collectively, these results indicate that in patients with extensive OPLL, reduction in segmental motion due to interlaminar fusion does not lead to measurable functional impairment.
Given that interlaminar fusion was associated with reduced C2-3 OPLL progression without adverse effects on clinical or radiologic outcomes, it may offer a biomechanical benefit at the C2-3 segment in patients with multilevel OPLL. This observation challenges the rationale behind preventive measures aimed at avoiding interlaminar fusion, such as C3 laminectomy, which may provide limited benefit and could even be counterproductive in this population. Although our study did not directly compare surgical techniques, previous work by Kim et al2 28 reported less favorable outcomes following C3 laminectomy, further supporting the rationale for preserving posterior structures when feasible.
Interestingly, our analysis showed that C2 dome laminoplasty was independently associated with increased OPLL progression. However, there is no clear evidence linking dome-like laminoplasty to postoperative instability or excessive motion. On the contrary, this technique has been widely regarded as beneficial for preserving semispinalis muscle attachments and reducing postoperative neck pain.29,30 Biomechanical studies have demonstrated that the C2 spinous process and its attached extensor musculature play an important role in maintaining cervical alignment and stability, and that excessive disruption of these posterior structures, such as in conventional C2 open-door laminoplasty, may adversely affect postoperative biomechanics.29,31 The observed association in our study is therefore more likely attributable to baseline disease severity, as patients requiring dome laminoplasty typically had more extensive cranial OPLL. Moreover, since the majority of our cohort (42 of 49; 85.7%) underwent dome laminoplasty, this finding may also reflect sampling bias. Accordingly, this result should not discourage the use of dome laminoplasty when indicated, as adequate decompression remains the cornerstone of surgical management in cervical myelopathy.
We also found that larger baseline OPLL AP diameter was inversely associated with subsequent progression. Several long-term studies have similarly reported that OPLL tends to progress more in the sagittal dimension than in transverse dimension, consistent with our findings.17,32–34 This inverse relationship may represent a “ceiling effect” in the biological capacity for additional ossification once the AP dimension reaches a critical thickness. This interpretation aligns with prior clinical and biomechanical observations suggesting that OPLL growth decelerates after achieving a certain extent.16,35 Another possible explanation is that increased cerebrospinal fluid pressure, especially after decompression, may exert an inhibitory effect on the AP progression. Limited AP progression could, in part, explain the relatively low incidence of neurological deterioration despite radiologic progression,9,10,33,34 as observed in our cohort, where no patient required reoperation.
Taken together, our findings suggest that C2-3 interlaminar fusion should not be regarded as an undesirable consequence of cervical laminoplasty in patients with OPLL. Rather, its occurrence may reflect a more stable postoperative biomechanical environment that contributes to reduced OPLL progression without compromising functional outcomes. Although our results do not advocate for the intentional induction of interlaminar fusion, its presence in patients with multilevel OPLL should not be considered problematic.
This study has several limitations. First, it was a retrospective, single-center analysis. Although this design ensured consistency in surgical technique and follow-up, it limits the generalizability of our findings. Future prospective, multicenter studies are warranted to validate these results and to further clarify the relationship between surgical technique and OPLL progression. Second, OPLL progression was assessed using linear measurements on sagittal CT rather than volumetric analysis or MRI-based evaluation, which may underestimate the three-dimensional extent of ossification and its impact on the spinal cord. Third, the recently proposed concept of the “true continuous segment” in OPLL 35 was not applied, as we used conventional radiologic OPLL typing. As a result, certain dynamic or segmental characteristics may have been overlooked. Fourth, a relatively higher loss to follow-up was observed in the non-fusion group between the 2-year and ≥5-year follow-up periods, raising the possibility of attrition bias. As a result, findings from the ≥5-year analyses should be interpreted with caution, particularly with respect to between-group comparisons. Finally, fusion occurring at cervical levels other than C2-3 was not systematically evaluated, and potential adjacent-segment effects were therefore not analyzed.
Despite these limitations, this study has important strengths. It is, to our knowledge, the first to examine the influence of interlaminar bony fusion on OPLL progression after cervical laminoplasty with long-term radiologic and clinical follow-up.
Conclusion
Spontaneous C2-3 interlaminar bony fusion following cervical laminoplasty was independently associated with reduced C2-3 level OPLL progression without adverse effects on cervical motion or clinical outcomes. These results suggest that interlaminar fusion may serve as a stabilizing factor rather than an unfavorable postoperative change in patients with multilevel OPLL.
Supplemental Material
Supplemental Material - C2–3 Interlaminar Bony Fusion Mitigates Long-Term Progression of Ossification of the Posterior Longitudinal Ligament Following Cervical Laminoplasty
Supplemental Material for C2–3 Interlaminar Bony Fusion Mitigates Long-Term Progression of Ossification of the Posterior Longitudinal Ligament Following Cervical Laminoplasty by Namhoo Kim, Kyung-Soo Suk, Junseok Hong, Jaenam Lee, Sub-Ri Park, Jae Won Shin, Ji-Won Kwon, Byung Ho Lee, Si-Young Park, Jin-Oh Park, Seong-Hwan Moon, Hak-Sun Kim in Global Spine Journal
Footnotes
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of Yonsei University Gangnam Severance Hospital, and the study was registered under No. 3-2024-0070.
Consent to Participate
The need for informed consent was waived due to the retrospective design of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.