
Abstract
Study Design
Systematic review.
Objective
To compare laminoplasty versus laminectomy and fusion in patients with cervical myelopathy caused by OPLL.
Methods
A systematic review was conducted using PubMed/Medline, Cochrane database, and Google scholar of articles. Only comparative studies in humans were included. Studies involving cervical trauma/fracture, infection, and tumor were excluded.
Results
Of 157 citations initially analyzed, 4 studies ultimately met our inclusion criteria: one class of evidence (CoE) II prospective cohort study and three CoE III retrospective cohort studies. The prospective cohort study found no significant difference between laminoplasty and laminectomy and fusion in the recovery rate from myelopathy. One CoE III retrospective cohort study reported a significantly higher recovery rate following laminoplasty. Another CoE III retrospective cohort study reported a significantly higher recovery rate in the laminectomy and fusion group. One CoE II prospective cohort study and one CoE III retrospective cohort study found no significant difference in pain improvement between patients treated with laminoplasty versus patients treated with laminectomy and fusion. All four studies reported a higher incidence of C5 palsy following laminectomy and fusion than laminoplasty. One CoE II prospective cohort and one CoE III retrospective cohort reported that there was no significant difference in axial neck pain between the two procedures. One CoE III retrospective cohort study suggested that there was no significant difference between groups in OPLL progression.
Conclusion
Data from four comparative studies was not sufficient to support the superiority of laminoplasty or laminectomy and fusion in treating cervical myelopathy caused by OPLL.
Keywords
Introduction
Currently there is no standard surgical algorithm for treating cervical myelopathy caused by ossification of the posterior longitudinal ligament (OPLL). Surgical options include anterior corpectomy and fusion, laminoplasty, and laminectomy and fusion. 1 The literature has demonstrated a significant complication rate associated with anterior corpectomy and fusion, 2 which has led to the investigation of posterior-based procedures, including both laminoplasty and laminectomy and fusion. Laminoplasty has been advocated because of its preservation of neck range of motion (ROM) compared with laminectomy and fusion. However, OPLL is unique when compared with other inciting etiologies of myelopathy, in that neck ROM may incite further progression of OPLL. 3
The current literature is laden with studies of laminoplasty and laminectomy and fusion, with the majority of studies lacking comparative groups or long-term follow-up. In this study, we performed a systematic review to assess the clinical results and complications of laminoplasty compared with that of laminectomy and fusion for the treatment of cervical myelopathy caused by OPLL.
To compare laminoplasty to laminectomy and fusion, three key questions were devised: (1) In patients with cervical myelopathy caused by OPLL, what is the effectiveness of laminoplasty compared with laminectomy and fusion? (2) In patients with cervical myelopathy caused by OPLL, what is the safety of laminoplasty compared with laminectomy and fusion? (3) In patients with cervical myelopathy caused by OPLL, does OPLL progress after laminoplasty more than laminectomy and fusion?
Materials and Methods
No approval from the Institutional Review Board was needed.
Results
One hundred fifty-seven citations were initially reviewed. After application of the inclusion criteria, seven studies were evaluated for review. Three studies were excluded because they had fewer than five patients per group or they did not directly compare laminoplasty to laminectomy and fusion. 6 , 7 , 8 Four studies were included in the final analysis in this study (Fig. 1, Table 1). Yuan et al, the single prospective cohort study reviewed (CoE II), compared laminoplasty with laminectomy and fusion. 9 Lee et al, a retrospective cohort study (CoE III), compared laminoplasty, laminectomy alone, and laminectomy and fusion. 10 The final two articles, each retrospective cohort studies (CoE III), were authored by Chen et al and compared laminoplasty, corpectomy, and fusion with laminectomy and fusion. 11 , 12 Each study included a mixture of continuous, segmental, and mixed types of OPLL. The populations in the studies were predominantly middle-aged men, and the follow-up was greater than 12 months in each study (range 12 to 72 months).
Studies comparing laminoplasty with laminectomy and fusion: characteristic of included studies
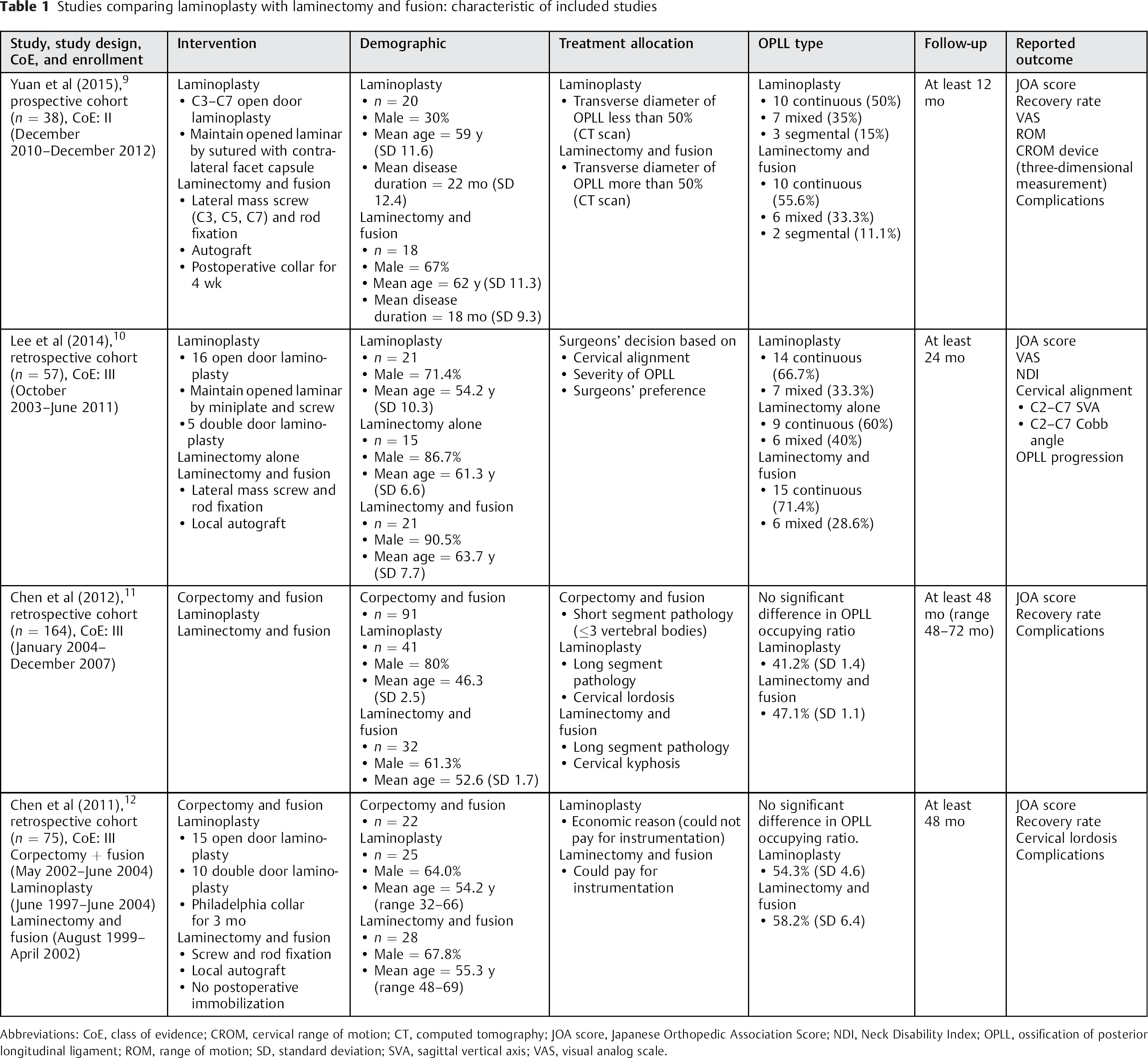
Abbreviations: CoE, class of evidence; CROM, cervical range of motion; CT, computed tomography; JOA score, Japanese Orthopedic Association Score; NDI, Neck Disability Index; OPLL, ossification of posterior longitudinal ligament; ROM, range of motion; SD, standard deviation; SVA, sagittal vertical axis; VAS, visual analog scale.
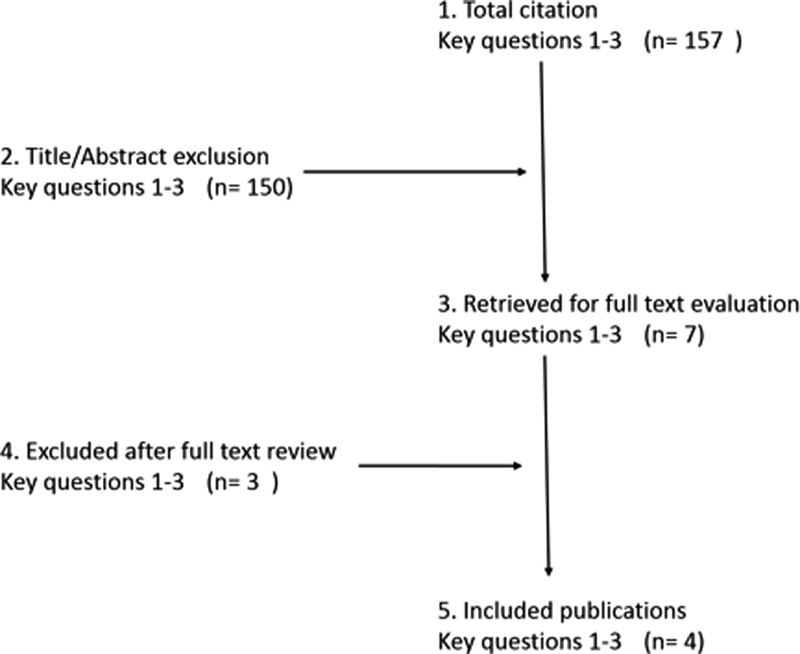
Flowchart showing result of literature search.
Comparison of Clinical Results
Myelopathy
The recovery rate as defined by Hirabayashi et al is based on the equation: [(postoperative JOA score − preoperative JOA score)/(17 − preoperative JOA score)] × 100%. 13 Yuan et al evaluated neurologic improvement using JOA score and recovery rate (Table 2). 9 The study found no significant difference between treatments groups at 1-year follow-up. The mean recovery rate was 43.7% in the laminoplasty group and 50.8% in the laminectomy and fusion group. In agreement, Lee et al did not find any significant difference in recovery between treatment groups. 10 Chen et al additionally assessed the neurologic improvement using the JOA score and recovery rate. 11 This study reported a significantly higher recovery following laminoplasty compared with laminectomy and fusion (65.2 versus 50.8%). However, all patients who underwent laminectomy and fusion had preoperative cervical kyphosis and a more severe neurologic deficit preoperatively, which might explain the lower recovery rate in the laminectomy and fusion group of this study. In contrast, Chen et al found that the recovery rate after laminoplasty was significant lower than after laminectomy and fusion (21.1 versus 43.5%). 12 In this study, the preoperative cervical alignment and neurologic status were comparable between groups.
Studies comparing laminoplasty with laminectomy and fusion: comparison of clinical results
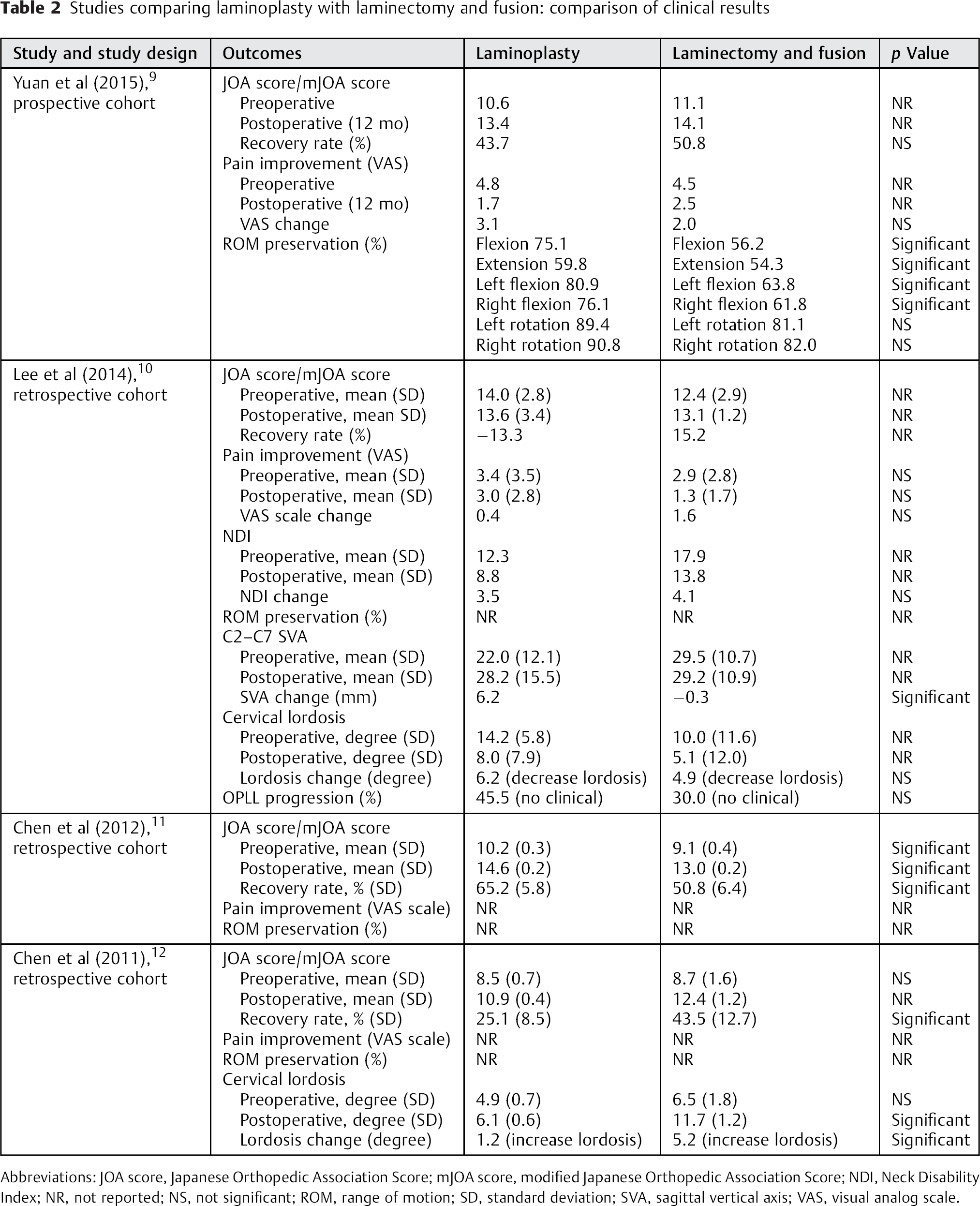
Abbreviations: JOA score, Japanese Orthopedic Association Score; mJOA score, modified Japanese Orthopedic Association Score; NDI, Neck Disability Index; NR, not reported; NS, not significant; ROM, range of motion; SD, standard deviation; SVA, sagittal vertical axis; VAS, visual analog scale.
Neck Pain
Yuan et al reported VAS following both laminoplasty and laminectomy and fusion (Table 2). 9 The mean VAS of the laminoplasty group decreased from 4.8 to 1.7, and the mean VAS of the laminectomy and fusion group decreased from 4.5 to 2.5. There was no significant difference in the improvement of VAS between these groups. In accordance with these results, Lee et al reported improvements in VAS of neck pain after surgery in both treatments groups, laminoplasty (3.4 to 3) and laminectomy and fusion (2.9 to 1.3), with no significant difference between operative groups. 10
Neck Disability Index
Lee et al accessed functional improvements using the Neck Disability Index (NDI) score (Table 2). 10 The mean NDI score following laminoplasty decreased from 12.3 to 8.8, and the mean NDI score following laminectomy and fusion decreased from 17.9 to 13.8. Improvement in the NDI score was not significantly different between the two treatment groups.
Cervical Range of Motion Preservation
Yuan et al was the only study to compare ROM between the different surgical interventions (Table 2). 9 This study reported significantly greater ROM in flexion, extension, and side bending in the individuals who underwent laminoplasty compared with those who underwent laminectomy and fusion. The greatest loss in ROM seen in both surgical groups was in extension, 59.8 and 54.3% of preoperative values for laminoplasty and laminectomy and fusion groups, respectively. The greatest preservation in ROM was seen in rotation, wherein 90% of preoperative ROM was seen following laminoplasty and 80% following laminectomy and fusion.
Cervical Alignment
Lee et al found a significant loss of cervical lordosis over time following both laminoplasty and laminectomy and fusion: laminoplasty, change from −14.2 degrees to −8.0 degrees; laminectomy and fusion, change from −10.0 degrees to −5.1 degrees (Table 2). 10 Additionally, this study showed that the mean C2–C7 sagittal vertical axis of patients in the laminoplasty group increased gradually from preoperative to 24 months (change from 22.0 to 28.2 mm). In contrast, there was no change in the laminectomy and fusion group for 24 months (change from 29.5 to 29.2 mm). Subgroup analysis showed that a high sagittal vertical axis (>40 mm) was correlated with significant neck pain in the laminoplasty group. Chen et al reported significantly greater lordosis following laminectomy and fusion than laminoplasty. 12
Complications
Fifth Cervical Nerve Root Palsy
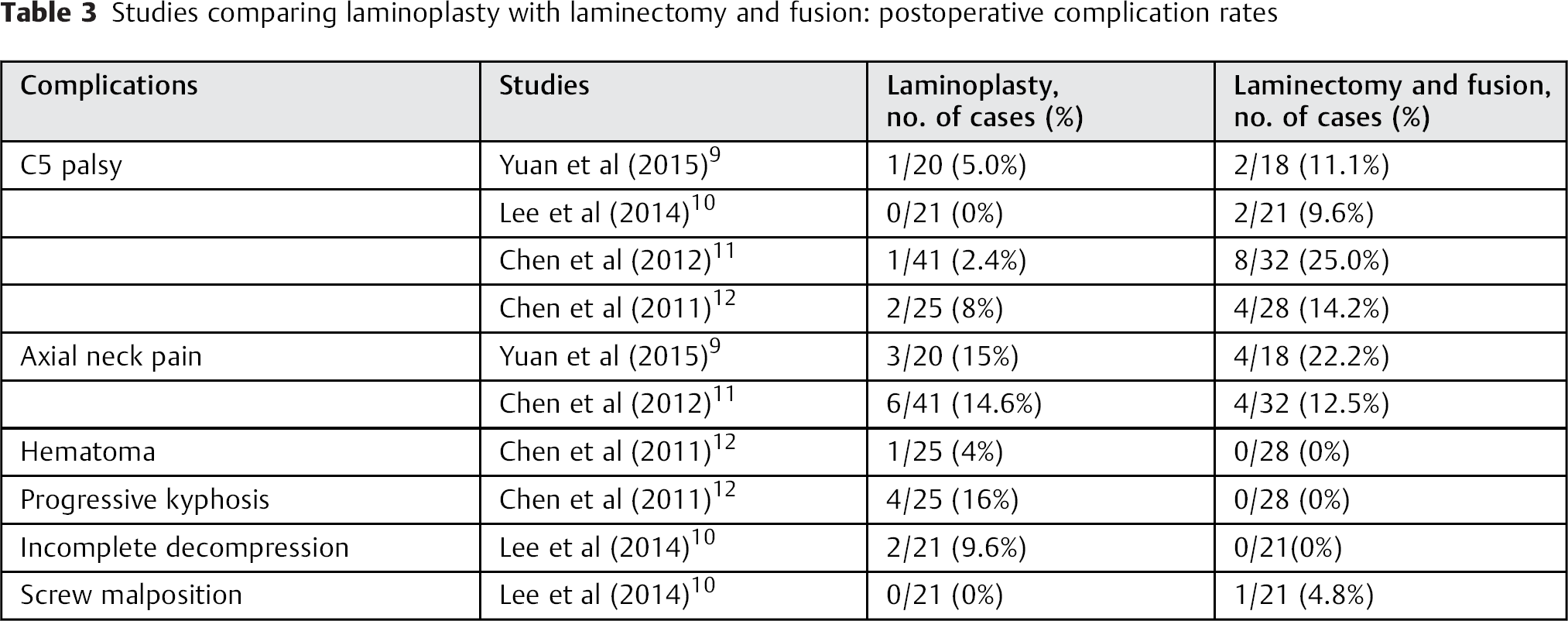
All four studies reported that the incidence of cervical nerve root five (C5) palsy was higher following laminectomy and fusion (range, 9.6 to 25%) than laminoplasty (range, 0 to 8%). The majority of C5 palsy fully recovered at 12 months’ follow-up (Table 3).
Studies comparing laminoplasty with laminectomy and fusion: postoperative complication rates
Other Complications
Miscellaneous complications were reported following laminoplasty including hematoma (4%), 12 progressive kyphosis (20%), 12 and incomplete decompression (9.6%). 10 Lee et al reported a 4.8% rate of screw malposition following laminectomy and fusion. 10
OPLL Progression
Lee et al reported that the progression rate of OPLL was 45.5, 52.5, and 30.0% in laminoplasty, laminectomy alone, and laminectomy and fusion groups, respectively (Table 2). 10 This study found no significant difference following laminoplasty compared with laminectomy and fusion. Additionally, no neurologic deterioration was found as a result of OPLL progression in any of the groups.
Evidence Summary
The evidence presented does not establish the superiority of laminoplasty or laminectomy and fusion (Table 4). The evidence regarding improvements in myelopathy and NDI following laminoplasty or laminectomy and fusion is insufficient. The strength of evidence regarding pain and ROM following either procedure is low. Additionally, the strength of evidence evaluating the safety of either procedure is insufficient. Finally, the overall strength of evidence evaluating the incidence of OPLL progression following laminoplasty or laminectomy and fusion does not establish the beneficence of one procedure over the other.
Evidence summary
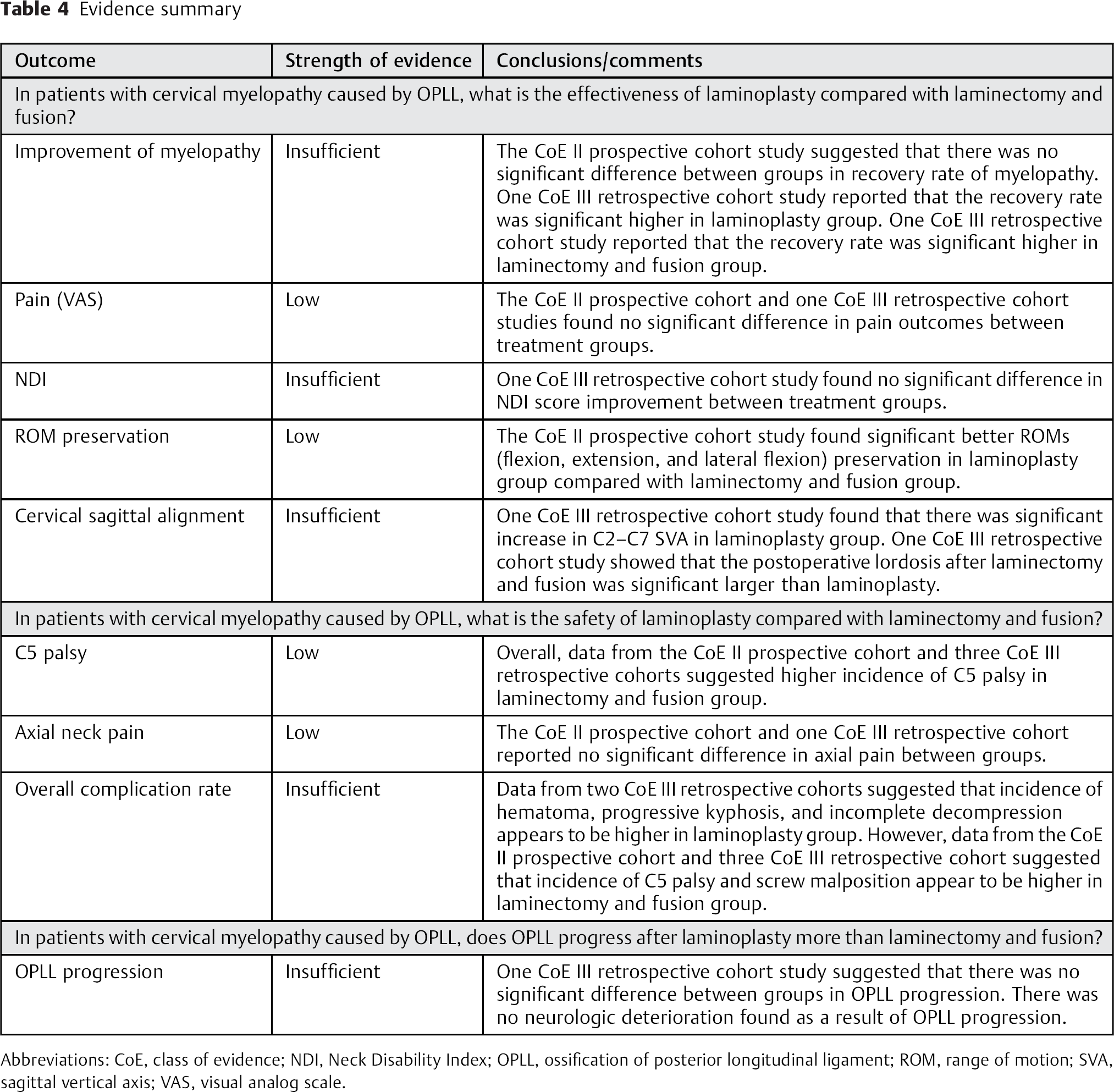
Abbreviations: CoE, class of evidence; NDI, Neck Disability Index; OPLL, ossification of posterior longitudinal ligament; ROM, range of motion; SVA, sagittal vertical axis; VAS, visual analog scale.
Discussion
The gold standard surgical treatment for cervical myelopathy caused by OPLL remains controversial. Anterior corpectomy and fusion surgery, which directly decompresses the spinal cord, is technically demanding and associated with high complication rates, causing surgeons to opt for the posterior approach to address this cervical pathology. In this study, we evaluated the evidence regarding laminoplasty or laminectomy and fusion by analyzing data obtained from PubMed/Medline, Cochrane, and Google scholar. Despite many studies on the surgical treatment of OPLL, few had comparative groups. After application of inclusion criteria, four studies were included for analysis: one prospective cohort and three retrospective cohort studies. Due to the heterogeneity of these studies, we were unable to perform a meta-analysis of the data. Therefore, we performed a systematic review regarding the surgical effectiveness, safety, and risk of OPLL progression comparing laminoplasty and laminectomy and fusion.
Each of the studies reported a JOA score and an individual recovery rate; however, the results diverged. Yuan et al suggested no significant difference in recovery rate between the treatment groups. 9 Insignificance between the two groups was similarly seen in the study by Lee et al. 10 In contrast, Chen et al reported that laminoplasty was superior. However, all patients who underwent laminectomy and fusion had preoperative cervical kyphosis and more severe neurologic deficits. 11 In another study, Chen et al reported conflicting conclusions that favored laminectomy and fusion. 12 Although each study was comparative, each also has significant limitations. All four studies were nonrandomized controlled studies. Additionally, the surgeons chose either laminoplasty or laminectomy and fusion with different criteria; therefore, there were significant differences in the populations compared. In conclusion, the current literature does not demonstrate greater effectiveness of laminoplasty or laminectomy and fusion in treating cervical myelopathy caused by OPLL.
There was no one procedure that was found to be superior regarding complications. There was a higher incidence of C5 palsy following laminectomy and fusion. On the other hand, the incidence of postoperative hematoma, progressive kyphosis, and incomplete decompression were higher following laminoplasty. Additionally, OPLL progression was 45.5% following laminoplasty and 30.0% after laminectomy and fusion. However, this result was not statistically significant, and there was no neurologic deterioration found as a result of OPLL progression. Finally, the incidence of axial neck pain was comparable between groups.
The greatest limitation to this current study is that few comparative studies are available, and there were no randomized controlled studies for evaluation. Additionally, the NDI score and ROM preservation were reported in only one study. Data from these four comparative studies is not sufficient to establish the superiority of laminoplasty or laminectomy and fusion in treating cervical myelopathy caused by OPLL. The overall strength of evidence to support any conclusion is low or insufficient. Often, the value of a systematic review is to identify the absence of clear-cut evidence. For example, some surgeons believe that one procedure is superior to the other and cite the few articles on the topic. Our analysis suggests that the evidence for superiority of one over the other is not strong. However, because outcomes of both procedures appear to be equivalent, one might consider the less-invasive nature and lower cost of laminoplasty. Although there is insufficient evidence to make the recommendation based upon the available literature, surgeons and patients might consider cost and invasiveness when choosing between the two options. Nonetheless, it is a reflection of the state of the literature, and at minimum, this review can be a springboard for future research to fill in the gaps. Well-designed randomized studies are required to answer this question.
Conclusion
The data from four comparative studies is not sufficient to support the superiority of laminoplasty or laminectomy and fusion in treating cervical myelopathy caused by OPLL. The overall strength of evidence to support any conclusion is low or insufficient.
Disclosures
Weerasak Singhatanadgige: none
Worawat Limthongkul: none
Frank Valone III: none
Wicharn Yingsakmongkol: none
K. Daniel Riew: Board member (AOSpine International); Editorial board (Global Spine Journal, Spine Journal, Neurosurgery); Grant (AOSpine, Cerapedics, Medtronic); Honorarium (AOSpine, NASS); Royalties (Medtronic, Biomet); Travel expenses (Broadwater)
Funding
None