
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To compare postoperative changes of cervical sagittal alignment (CSA) and cervical sagittal balance (CSB) after laminoplasty between cervical spondylotic myelopathy (CSM) and ossification of the posterior longitudinal ligament (OPLL) and to examine impacts of these radiologic changes on neurologic outcomes.
Methods:
A total of 168 consecutive patients with CSM (CSM group) and 51 consecutive patients with OPLL (OPLL group) were included. As indicators of CSA and CSB, the C2-7 angle and C1-C7 sagittal vertical axis (SVA) were, respectively, measured before surgery and at 2-year follow-up. Neurologic status was assessed using the Japanese Orthopaedic Association score before surgery and at 2-year follow-up.
Results:
Whereas both postoperative loss of C2-7 angle and increase of C1-C7 SVA were significantly greater in the elderly subgroup of the CSM group, patient age did not significantly affect these changes in the OPLL group. Preservation of C7 maintained C1-C7 SVA at postoperative 2 years only in the CSM group. Postoperative cervical kyphosis and sagittal imbalance significantly decreased neurologic improvement in the CSM group but not in the OPLL group.
Conclusions:
Elderly patients with CSM have significantly greater postoperative loss of lordosis and increase in C1-C7 SVA than nonelderly patients, and both postoperative kyphotic deformity and sagittal imbalance significantly deteriorate neurologic recovery. On the other hand, although patients with OPLL, irrespective of patient age and preservation of C7, have significantly more loss of lordosis and increase in C1-C7 SVA than CSM patients, neither postoperative kyphotic deformity nor sagittal imbalance significantly deteriorates neurologic recovery in OPLL patients.
Keywords
Introduction
Cervical laminoplasty has been one of the widely accepted surgical procedures for cervical compression myelopathy, such as cervical spondylotic myelopathy (CSM) and cervical ossification of the posterior longitudinal ligament (OPLL). Kyphotic deformity, an unfavorable change of cervical sagittal alignment (CSA) after laminoplasty, is one of the well-known complications affecting surgical outcomes following surgery for CSM and OPLL. 1 -3 In addition to cervical sagittal malalignment, cervical sagittal balance (CSB) defined on the cervical sagittal vertical axis (SVA) has recently been recognized as one of the important factors affecting the outcomes of cervical spine surgery. 4 CSM and OPLL have substantially different etiologies and pathological conditions. However, no studies have reported on the differences in the postoperative changes of CSA and CSB after laminoplasty between CSM and OPLL. The purposes of this study were thus to compare the postoperative changes of CSA and CSB after laminoplasty between CSM and OPLL, focusing primarily on the impacts of patient age and preservation of C7 on these changes, and to examine impacts of these radiologic changes on neurologic recovery after surgery.
Materials and Methods
Patients
All patients with cervical myelopathy at our institute are treated using cervical laminoplasty, with the exception of those with cervical kyphosis ≥15° and a single-level anterior lesion without a narrow spinal canal who are good candidates for anterior decompression and fusion. Based on our criteria, 168 consecutive patients who underwent laminoplasty for CSM between June 2010 and April 2015 and were followed for >24 months were included in this study (CSM group). A total of 51 consecutive patients who underwent laminoplasty for OPLL during the same period as the CSM group and were followed for >24 months were also included (OPLL group). The mean age of the patients at the time of surgery was 70.1 years (range = 32-89 years) in the CSM group and 67.9 years (range = 40-89 years) in the OPLL group. No statistically significant difference in age at the time of surgery was seen between the CSM and OPLL groups (Table 1). For the first 2 weeks after surgery, all patients wore a soft collar to alleviate surgical wound pain. The protocol was approved by Kansai Rosai Hospital Ethics Committee, and written informed consent was obtained from all participants.
Demographic Data and Radiological Outcomes in the 2 Groups.a
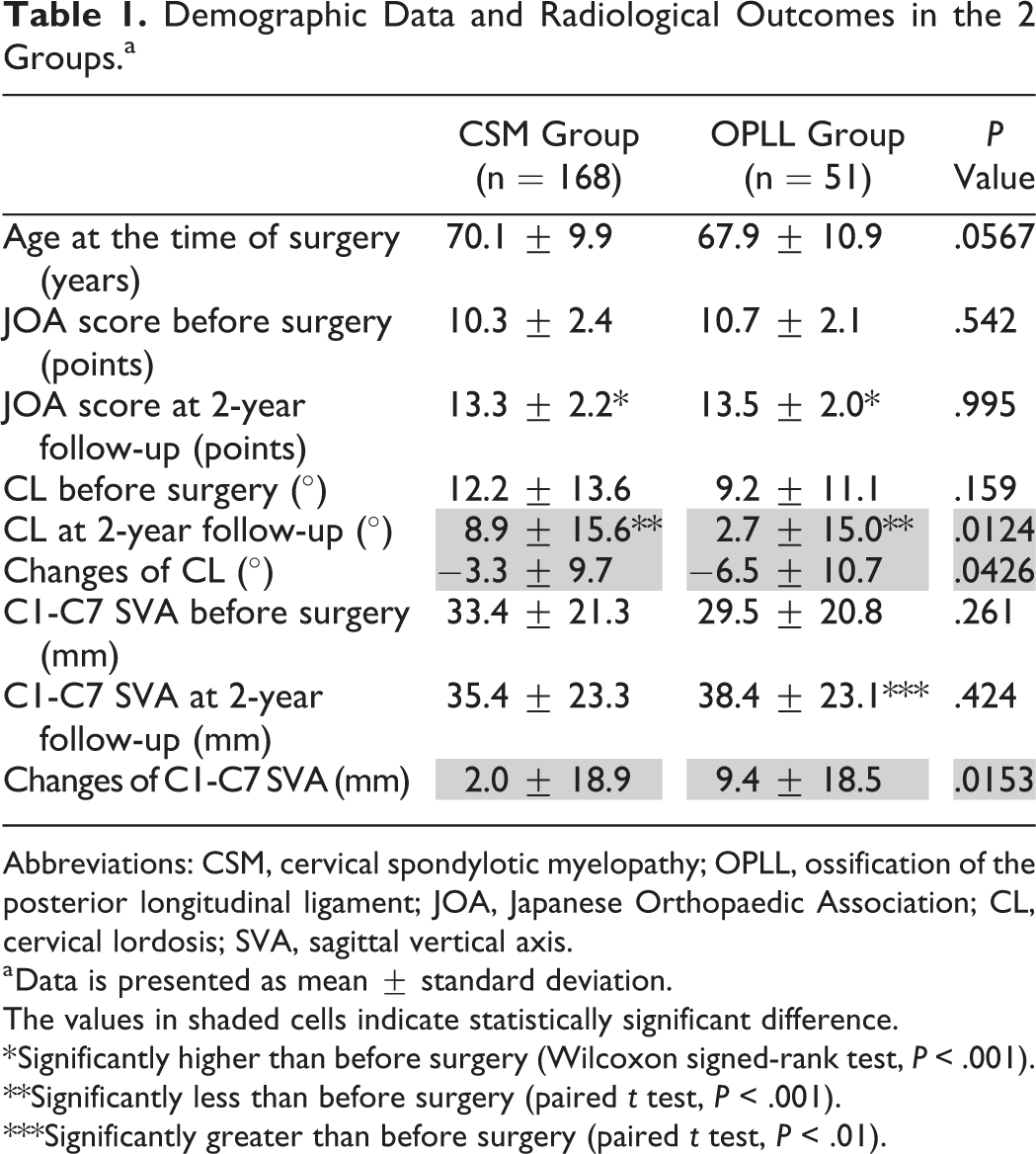
Abbreviations: CSM, cervical spondylotic myelopathy; OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association; CL, cervical lordosis; SVA, sagittal vertical axis.
a Data is presented as mean ± standard deviation.
The values in shaded cells indicate statistically significant difference.
* Significantly higher than before surgery (Wilcoxon signed-rank test, P < .001). **Significantly less than before surgery (paired t test, P < .001). ***Significantly greater than before surgery (paired t test, P < .01).
Radiologic Evaluations
Using lateral radiographs of the cervical spine in the standing position taken before surgery and at 2 years postoperatively, as indicators of CSA and CSB, cervical lordosis (CL = C2-7 Cobb angle) and C1-C7 SVA were measured, respectively. CL indicates the angle formed by 2 lines drawn parallel to the inferior endplates of the C2 and C7 vertebral bodies (Figure 1). C1-C7 SVA was defined as the distance between a plumb line dropped from the center of the C1 anterior arch and the center of the C7 vertebral body (Figure 1). In both groups, the patients were divided into 2 subgroups according to patient age (≥75 years old [E subgroup = elderly subgroup] and <75 years old [NE subgroup = nonelderly subgroup]), and they were also divided into 2 other subgroups according to the most caudal level of laminoplasty (C6 subgroup and C7 subgroup).
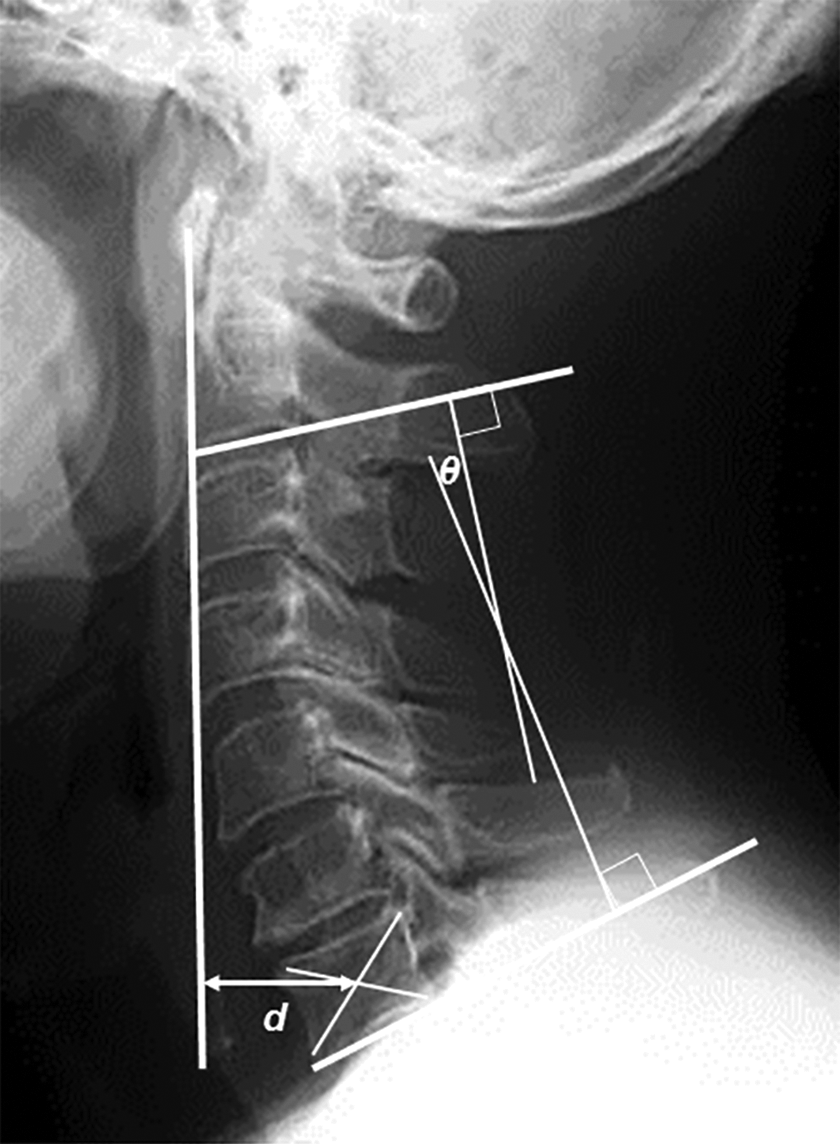
Radiographic measurements. Cervical lordosis (θ) indicates the angle formed by 2 lines drawn parallel to the inferior endplates of the C2 and C7 vertebral bodies. C1-C7 SVA (d) is defined as the distance between a plumb line dropped from the center of the C1 anterior arch and the center of the C7 vertebral body.
Neurologic Evaluations
The neurologic status of cervical myelopathy was assessed using the Japanese Orthopaedic Association (JOA) scoring system for cervical myelopathy (JOA score) 5 before surgery and at 2-year follow-up. The recovery rate of the JOA score was calculated by the following formula: Postoperative recovery rate (%) = (postoperative score − preoperative score)/(17 − preoperative score) × 100. 6 In both groups, the patients were divided into 2 subgroups according to postoperative CL (≥0° [Lordosis subgroup] and <0° [Kyphosis subgroup]), and they were also divided into 2 other subgroups according to postoperative C1-C7 SVA (≥30 mm [Imbalance subgroup] and <30 mm [Balance subgroup]).
Statistical Analysis
Statistical analysis was performed using JMP 5.0.1 software (SAS Institute, Cary, NC). The unpaired t test, paired t test, Mann-Whitney U test, and Wilcoxon signed-rank test were used, as appropriate. Values of P < .05 were considered significant.
Results
Cervical Sagittal Alignment
Preoperative CL was not significantly different between the CSM and OPLL groups (Table 1), between the Elderly (E) and Nonelderly (NE) subgroups (Tables 2 and 3), and between the C6 and C7 subgroups (Tables 4 and 5). In both the CSM and OPLL groups, CL decreased significantly after laminoplasty, and loss of CL was significantly greater in the OPLL group than in the CSM group (Table 1). Postoperative loss of CL was significantly greater in the E subgroup than in the NE subgroup of the CSM group (Table 2), whereas postoperative loss of CL was statistically significant and equal in both the E and NE subgroups of the OPLL group (Table 3). Age at the time of surgery was not significantly different between the C6 and C7 subgroups (Tables 4 and 5). Postoperative loss of CL was statistically significant and equal between the C6 and C7 subgroups (Tables 4 and 5).
Radiological Outcomes in the E and NE Subgroups of the CSM Group.a
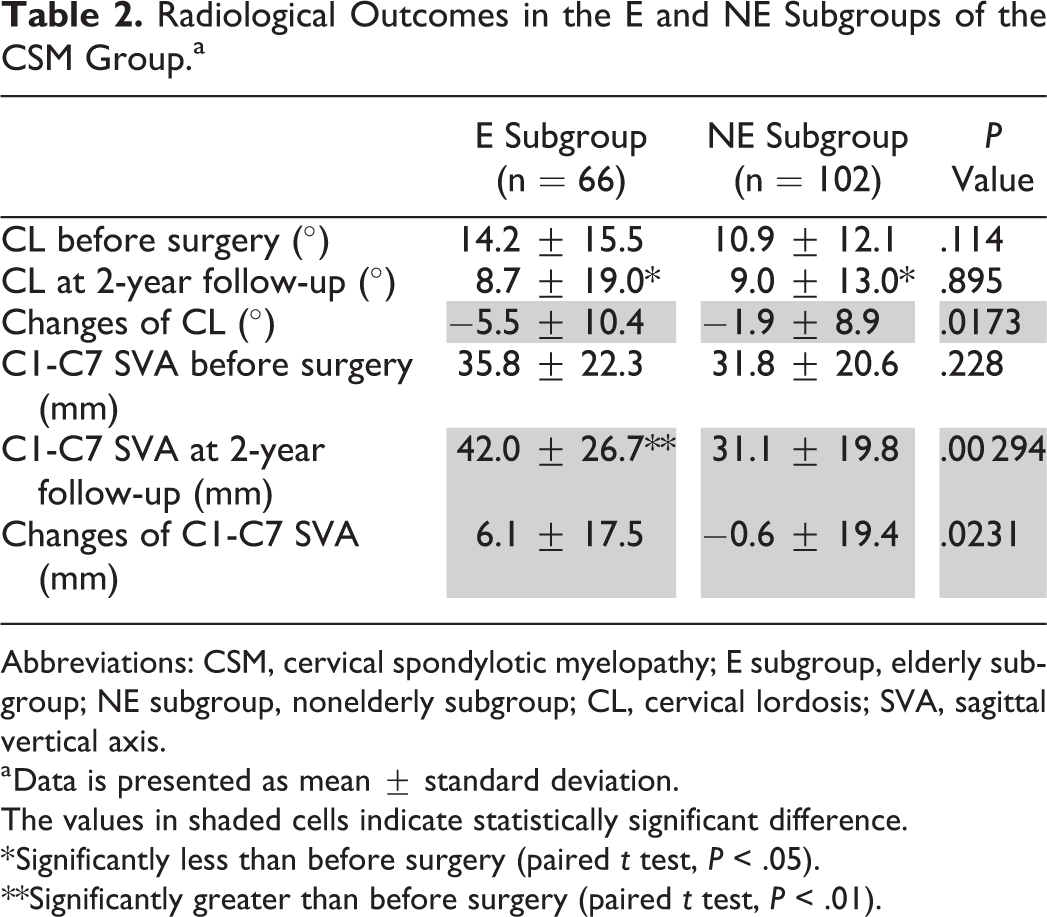
Abbreviations: CSM, cervical spondylotic myelopathy; E subgroup, elderly subgroup; NE subgroup, nonelderly subgroup; CL, cervical lordosis; SVA, sagittal vertical axis.
a Data is presented as mean ± standard deviation.
The values in shaded cells indicate statistically significant difference.
* Significantly less than before surgery (paired t test, P < .05). **Significantly greater than before surgery (paired t test, P < .01).
Radiological Outcomes in the E and NE Subgroups of the OPLL Group.a
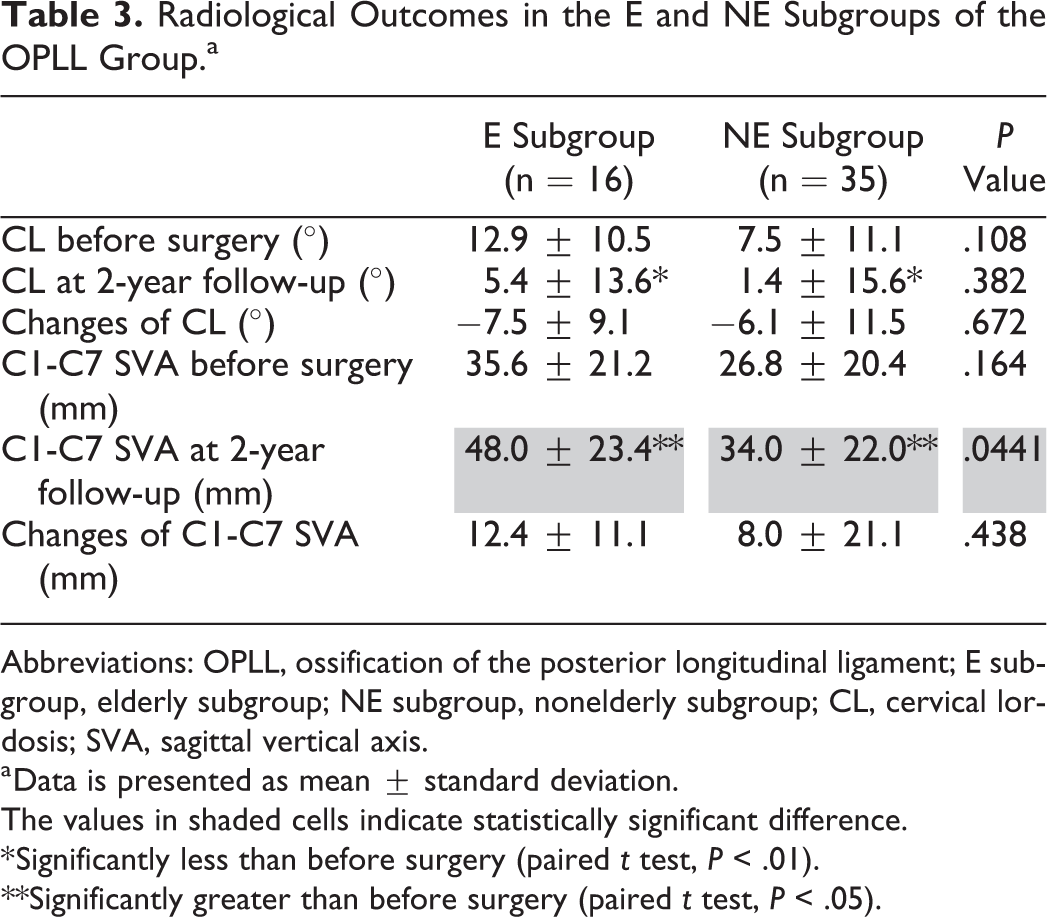
Abbreviations: OPLL, ossification of the posterior longitudinal ligament; E subgroup, elderly subgroup; NE subgroup, nonelderly subgroup; CL, cervical lordosis; SVA, sagittal vertical axis.
a Data is presented as mean ± standard deviation.
The values in shaded cells indicate statistically significant difference.
* Significantly less than before surgery (paired t test, P < .01). **Significantly greater than before surgery (paired t test, P < .05).
Patients’ Age and Radiological Outcomes in the C6 and C7 Subgroups of the CSM Group.a
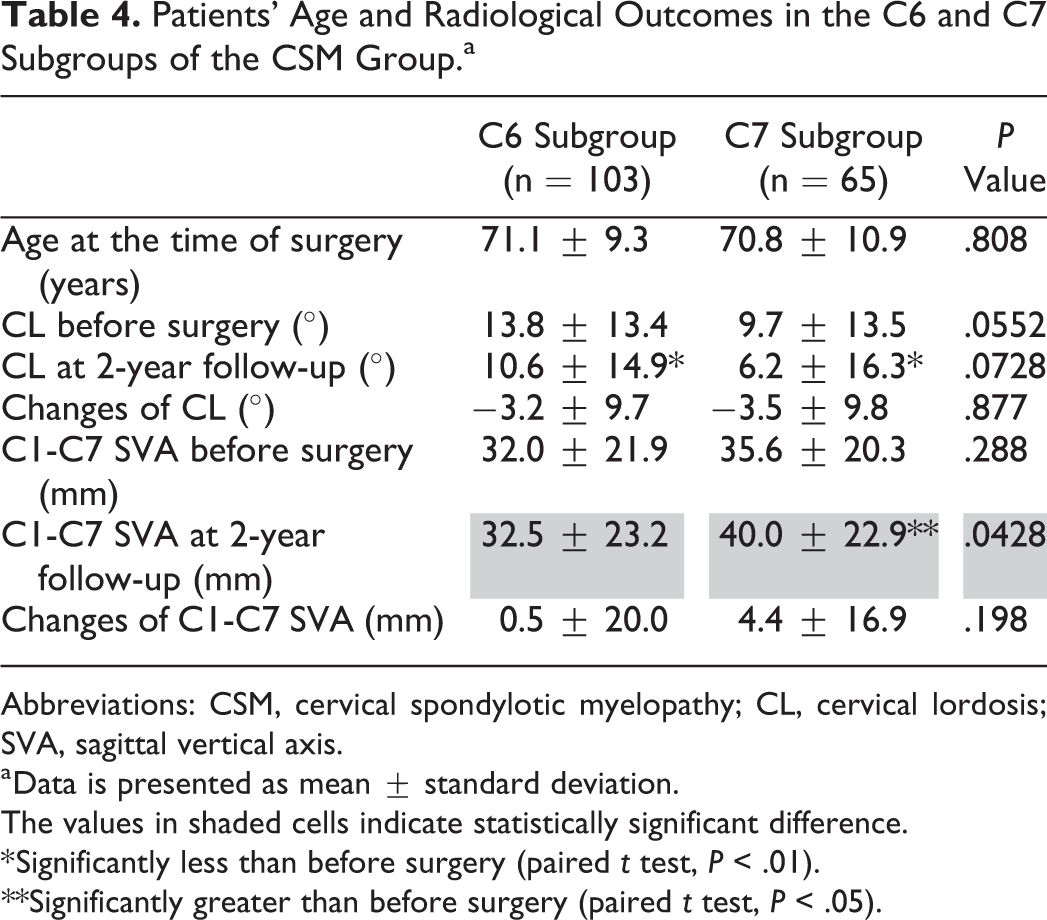
Abbreviations: CSM, cervical spondylotic myelopathy; CL, cervical lordosis; SVA, sagittal vertical axis.
a Data is presented as mean ± standard deviation.
The values in shaded cells indicate statistically significant difference.
* Significantly less than before surgery (paired t test, P < .01). **Significantly greater than before surgery (paired t test, P < .05).
Patients’ Age and Radiological Outcomes in the C6 and C7 Subgroups of the OPLL Groupa.
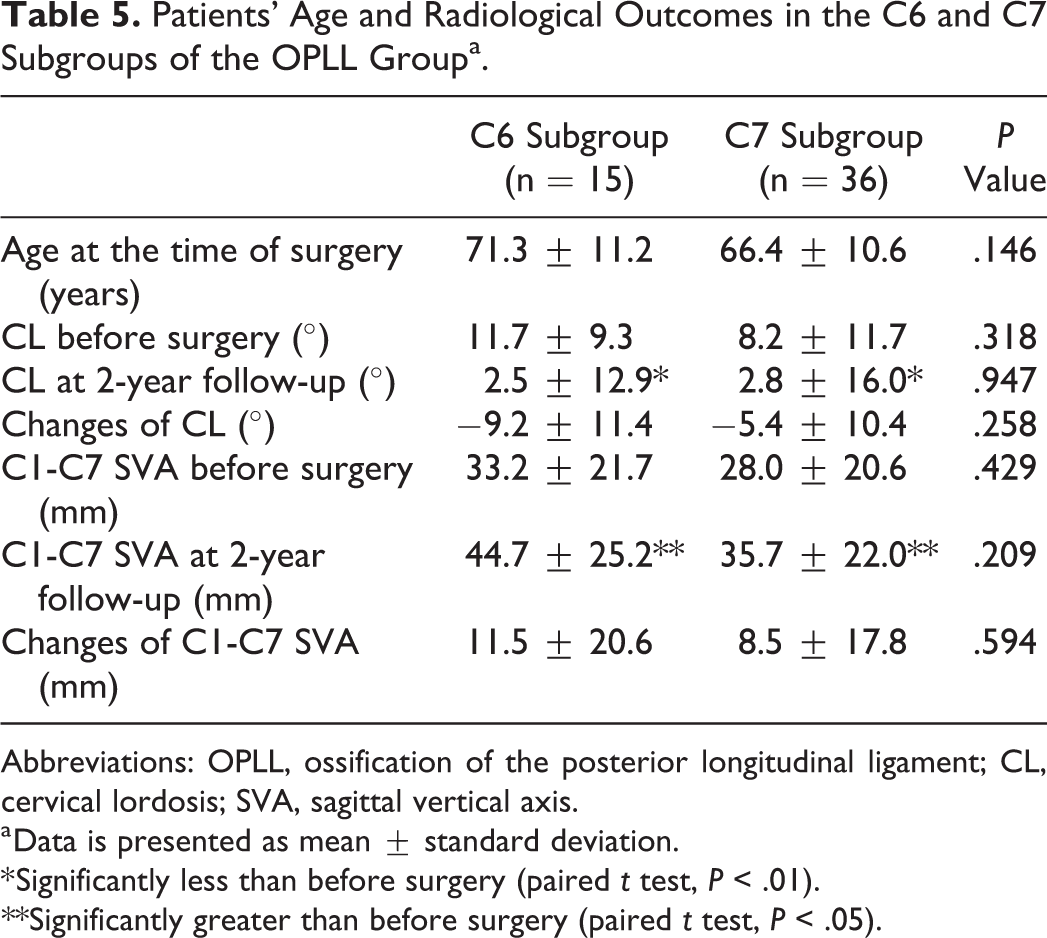
Abbreviations: OPLL, ossification of the posterior longitudinal ligament; CL, cervical lordosis; SVA, sagittal vertical axis.
a Data is presented as mean ± standard deviation.
* Significantly less than before surgery (paired t test, P < .01). **Significantly greater than before surgery (paired t test, P < .05).
Cervical Sagittal Balance
Preoperative C1-C7 SVA was not significantly different between the CSM and OPLL groups (Table 1), between the E and NE subgroups (Tables 2 and 3), and between the C6 and C7 subgroups (Tables 4 and 5). C1-C7 SVA was maintained at 2 years after surgery in the CSM group, while it increased significantly in the OPLL group (Table 1). Postoperative deterioration of C1-C7 SVA was statistically significant only in the E subgroup of the CSM group (Table 2). Whereas C1-C7 SVA was maintained at postoperative 2 years in the C6 subgroup of the CSM group, it increased significantly in the C7 subgroup (Table 4). On the other hand, the postoperative increase of C1-C7 SVA was statistically significant and equal between the E and NE subgroups of the OPLL group (Table 3), and between the C6 and C7 subgroups of the OPLL group (Table 5).
Neurologic Outcomes
The JOA score improved significantly after laminoplasty in both the CSM and OPLL groups, and neither the JOA score before surgery nor at 2 years after surgery showed statistically significant difference between the 2 groups (Table 1). In the CSM group, the recovery rate of the JOA score was significantly lower in the Kyphosis subgroup than in the Lordosis subgroup, and it was also significantly worse in the Imbalance subgroup than in the Balance subgroup (Table 6). On the other hand, in the OPLL group, neither postoperative CSA nor CSB significantly affected the recovery rate of the JOA score (Table 7).
Impacts of Postoperative Cervical Sagittal Alignment and Balance on Neurologic Recovery in the CSM Groupa.

Abbreviations: CSM, cervical spondylotic myelopathy; JOA, Japanese Orthopaedic Association.
a Data is presented as mean ± standard deviation.
Impacts of Postoperative Cervical Sagittal Alignment and Balance on Neurologic Recovery in the OPLL Groupa.

Abbreviations: OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association.
a Data is presented as mean ± standard deviation.
Discussion
In the present study, elderly patients with CSM had significantly greater postoperative loss of lordosis and increase in C1-C7 SVA than nonelderly CSM patients, although preservation of C7 maintained C1-C7 SVA at postoperative 2 years in the CSM group. Both postoperative kyphotic deformity and sagittal imbalance significantly deteriorated neurologic recovery in the CSM group. On the other hand, although patients with OPLL, irrespective of patient age and preservation of C7, had significantly more loss of lordosis and increase in C1-C7 SVA than CSM patients, neither postoperative kyphotic deformity nor sagittal imbalance significantly deteriorated neurologic recovery in the OPLL group.
The cutoff value for predicting kyphotic deformity after laminoplasty in CSM patients was reportedly an age of 75 years. 3 Patients in both the CSM and OPLL groups were thus divided into 2 subgroups by patient age (≥75 years old [E subgroup] and <75 years old [NE subgroup]). Clinical and biomechanical studies have proven that the nuchal ligament represents a significant restraint on cervical flexion, 7,8 and the funicular section of the nuchal ligament is tightly attached to the C7 spinous process. Based on these results, patients in both groups were also divided into 2 other subgroups according to the most caudal level of laminoplasty (C6 subgroup and C7 subgroup).
As an index of CSB, C1-C7 SVA was measured in the present study instead of the center of gravity of the head (CGH)-C7 SVA and C2-C7 SVA. CGH, the anterior margin of the external auditory canal, was reported to be not observed in 11.8% of the patients on lateral radiographs of the cervical spine, and CGH-C7 SVA was proven to have relatively low reproducibility. 9 C2-C7 SVA was reported to be influenced by anterior inclination of the dens. 9 On the other hand, C1-C7 SVA has reportedly relatively high reproducibility. 9 Based on these results, C1-C7 SVA was measured as the best index of CSB in the present study.
Regarding the postoperative changes of CL and cervical regional SVA, Sakai et al reported that both CL and cervical regional SVA worsened after laminoplasty for CSM. 10 Lee et al also reported that both CL and cervical regional SVA deteriorated following laminoplasty for OPLL. 11 On the other hand, Kato et al reported that postoperative changes of CL and cervical regional SVA were not statistically significant after laminoplasty for CSM and segmental OPLL. 12 As previously reported, 3 postoperative loss of CL was significantly greater in ≥75-year-old patients of the CSM group than in <75-year-old patients in this comparative study. Moreover, postoperative deterioration of C1-C7 SVA was also statistically significant only in ≥75-year-old patients of the CSM group in the present study. In general, a decrease of lumbar lordosis and an increase of thoracic kyphosis with increasing age result in an increase of cervical lordosis due to the compensation for balance. 13 In fact, in the present study, preoperative CL was greater in the Elderly subgroup than in the Nonelderly subgroup of the CSM group, though there was no statistically significant difference (Table 2). As Sakai et al suggested, 3 although preservation of C7 prevented postoperative deterioration of C1-C7 SVA in the CSM group, loss of compensatory force to maintain cervical lordosis due to surgical invasion in the posterior extensor mechanism during the laminoplasty procedure may lead to statically significant postoperative loss of CL and increase of C1-C7 SVA in the Elderly subgroup of the CSM group. On the other hand, most OPLL patients included in the present study had a mixed-type OPLL. After laminoplasty, which causes the destruction of the posterior extensor mechanism, the ankylosed area of the cervical spine due to a continuous portion of OPLL, as a long lever arm, could have stronger force acting on forward inclination of the craniocervical region than the cervical spine of CSM. We thus speculate that this mechanism may result in statistically significant postoperative deterioration of CL and C1-C7 SVA in the OPLL group, irrespective of patient age and preservation of C7.
Regarding neurologic recovery after laminoplasty for CSM, the recovery rate of the JOA score has been reported to be lower in patients with kyphotic deformity than in those without cervical kyphosis. 1,3 Since laminoplasty is a posterior indirect decompression procedure, sufficient decompression cannot be obtained in patients with cervical kyphosis that do not allow sufficient posterior shift of the spinal cord. This is thought to be the most likely cause of poor recovery rate of the JOA score in patients with kyphotic deformity after laminoplasty. Moreover, in CSM patients, the JOA score was reported to be negatively correlated with C2-C7 SVA. 14 As one of the possible mechanisms leading to this result, an in vitro study showed that increased intramedullary pressure was correlated with high SVA in the straight cervical spine. 15 The results in the present study were similar to these previously reported results. On the other hand, Iwasaki et al reported that, although postoperative progression of kyphotic deformity was observed in 8% of the OPLL patients after laminoplasty, it did not cause neurological deterioration. 16 Moreover, Lee et al recently reported that CL, C2-C7 SVA, and their changes after laminoplasty for OPLL were not significantly correlated with postoperative JOA scores. 17 Furthermore, in the present study, neither postoperative CSA nor CSB significantly affected the recovery rate of the JOA score in the OPLL group. Considering these results, variables other than postoperative CL and C1-C7 SVA, such as type of OPLL, occupation ratio of OPLL, patient age, duration of myelopathic symptoms, or preoperative severity of cervical myelopathy could affect the recovery rate of the JOA score after laminoplasty.
The present study has the following limitations: (1) since this study was retrospective in nature, the effects of thoracolumbar and spinopelvic parameters on postoperative changes of CSA and CSB were not examined using radiographs of the whole spine, and neither health-related quality of life (HRQOL), such as the Short Form-36, nor the visual analog scale (VAS) for axial neck pain were examined; (2) the follow-up period of 2 years was relatively short; and (3) the number of patients was much smaller in the OPLL group than in the CSM group. A further long-term study with larger patient populations including evaluation of whole spine radiographs, HRQOL, and VAS for axial neck pain is needed to make our findings in the present study more generalized and informative to those who are engaged in spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.