
Abstract
Study Design
A retrospective observational study.
Objective
To describe a novel outcome indication system, the posterior compression score (PCS), and investigate its clinical value in cervical ossification of the posterior longitudinal ligament (OPLL) patients treated with laminoplasty.
Methods
A total of 282 OPLL patients who underwent laminoplasty from January 2013 to December 2018 were reviewed. The patients were divided into high-score (HS) or low-score (LS) groups based on whether the PCS was over 8. Propensity score matching analysis with a caliper of .1 was used to attenuate the potential selection bias. Clinical measurements, including the Japanese Orthopedic Association (JOA) score, visual analog scale (VAS), neck disability index (NDI), and radiological measurements, including C2–C7 lordotic angle and range of motion (ROM), were compared between the groups.
Results
The mean follow-up period was 29.87 ± 9.17 months. There were no significant differences between the two groups regarding patients’ baseline demographical and clinical characteristics after propensity score matching. No significant differences were found in the operative time, blood loss, postoperative VAS score for neck and arm pain, postoperative C2–C7 lordotic angle, or postoperative ROM (P > .05). However, the postoperative JOA score and recovery rate were significantly higher in the HS group than in the LS group, while the postoperative NDI was significantly lower in the HS group (P < .05).
Conclusion
OPLL patients with higher PCS scores displayed better clinical outcomes. The novel PCS system is suggested to be a reliable scoring system for surgical outcome evaluation in patients with cervical OPLL.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a major cause of cervical myelopathy, which commonly occurs in the Asian male population.1-3 Laminoplasty (LAMP) has been widely accepted as an effective and safe method for OPLL.4,5 However, the surgical outcome of LAMP largely depends on the backward shifting of the spinal cord, so the clinical outcome is not always satisfying in some OPLL patients. Therefore, finding the risk factors that affect the outcome of LAMP is important for OPLL treatment.
The K-line was first introduced by Fujiyoshi et al 6 which helped to predict the prognosis of LAMP-treated OPLL patients and further contributed to the surgical approach decision-making for OPLL patients by using preoperative measurements. The K-line connects the midpoints of the anteroposterior spinal canal at both the C2 and C7 levels. When the foci of the ossified ligament exceed the K-line, it is denoted as K-line (-), while if the foci do not exceed the K-line, it is denoted as K-line (+). The K-line results reflect the alignment of the cervical spine, which influences the indirect decompression effect of LAMP and indicates the severity and thickness of ossified foci of OPLL.
Although better neurologic improvement was indicated by K-line (+) status in LAMP-treated OPLL patients, recent studies found few differences between K-line (+) and K-line (-) OPLL patients in clinical outcome by comparing the postoperative recovery rate of JOA score after LAMP.7,8 Thus, we suspect that the K-line might not be sufficient for predicting prognosis in all OPLL patients. A better indicator could be developed to predict the prognosis and help decide surgical approaches for LAMP-treated OPLL patients.
Since the K-line is used to assess the severity of ventral compression of the OPLL, we proposed a novel dorsal compression evaluation method called the posterior compression score (PCS) that may help to predict the prognosis of LAMP-treated OPLL patients by simply counting the PCS score of each region of the spinal cord dorsally. We further verified its clinical value by retrospectively reviewing LAMP-treated OPLL patients.
Materials and Methods
Patients
All study procedures were approved by the institute chancellor’s Human Research Committee in accordance with institute’s protocol. Ethical approval of this retrospective study was given by the Shanghai Changzheng Hospital ethics committee review board. This research was conducted in regard of the Declaration of Helsinki. We retrospectively studied patients with cervical OPLL who underwent LAMP between January 2013 and December 2018. OPLL was diagnosed using the following criteria: typical clinical symptoms of cervical myelopathy, accompanied by OPLL-featuring radiological evidence on X-ray, three-dimensional reconstructed computed tomography, and magnetic resonance imaging (MRI). A total of 326 patients were initially reviewed, and patients were excluded if they had incomplete radiological data, a previous cervical surgery history, were subjected to revision surgery, or were lost to follow-up. Based on the exclusion criteria, 282 patients passed, and all included patients were divided into two groups according to the PCS system (Figure 1). Patients in our study did not have severe kyphosis (cervical kyphosis angle >13°), which is not suitable for LAMP. The anesthesia protocol, surgical protocol, and perioperative management were standardized for all patients as previously described.
9
All patients were followed-up for at least 2 years, and informed consents were obtained from the participated patients. Flowchart of patients in the study.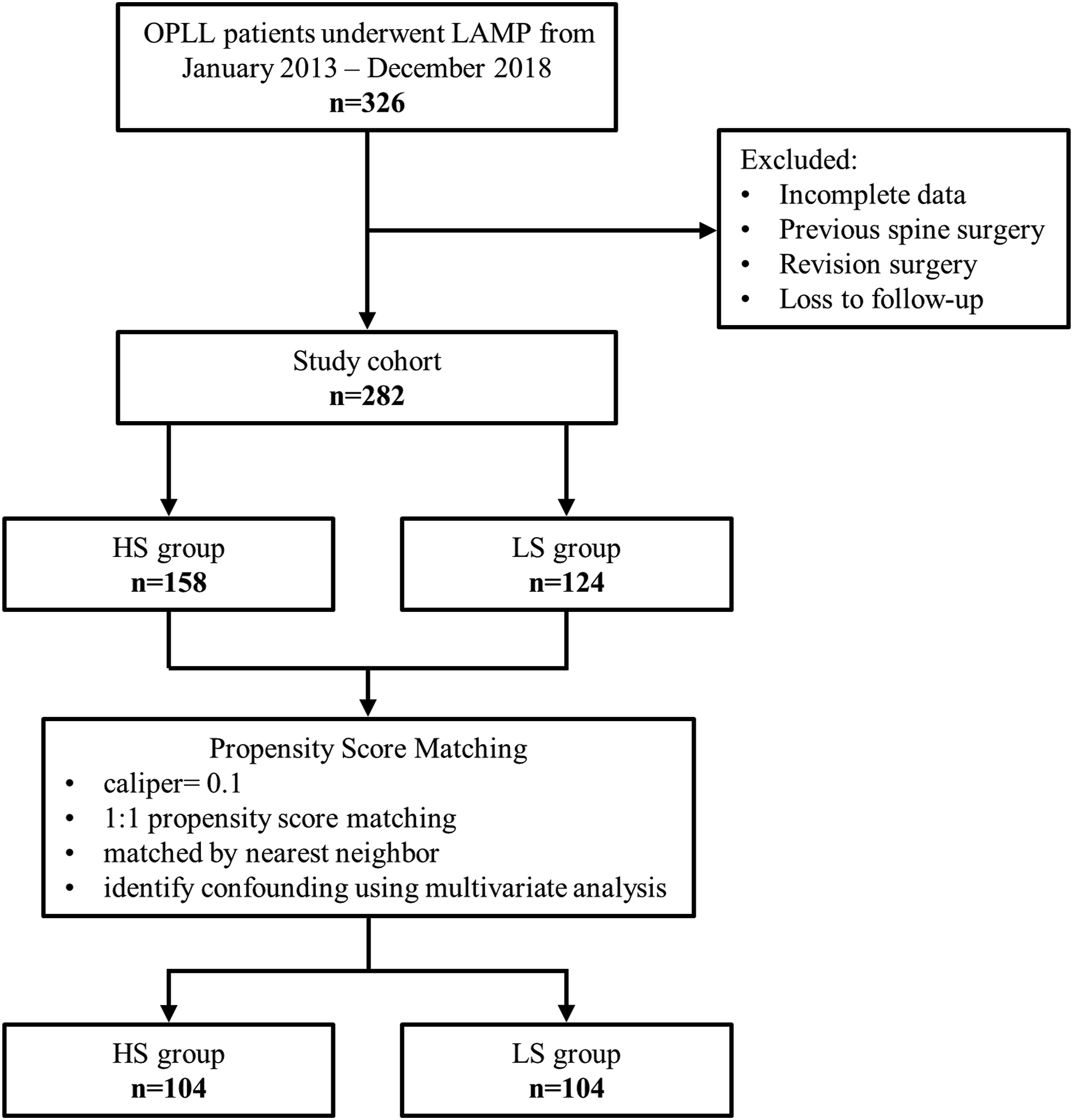
Clinical Assessments
The clinical outcomes were evaluated using the Japanese Orthopedic Association (JOA) score, neck disability index (NDI), and visual analog scale (VAS) for neck pain and arm pain. Neurological recovery was calculated by using the following formula: recovery rate (RR) of JOA score (%) = (postoperative JOA score – preoperative JOA score)/(17 – preoperative JOA score) × 100%.
Radiological Assessments
The radiological measurements were assessed by the C2–C7 lordotic Cobb angle and range of motion (ROM). The C2–C7 lordotic Cobb angle was defined as the angle from the inferior endplate of C2 to the superior endplate of C7 on lateral X-ray radiographs. The total cervical ROM was defined as the maximum movement angle of flexion to extension of the cervical spine in lateral radiographs.
The OPLL type was classified as segmental, continuous, and mixed. The K-line was defined as the line connecting the midpoint of the spinal canal at the C2 and C7 levels. K-line (+) was defined as OPLL that does not exceed the K-line, while K-line (-) was OPLL that exceeds the K-line. The OPLL occupation ratio (length of OPLL/length of the spinal canal) was measured at the most stenotic level of the spinal canal on a CT sagittal view. The formula for occupation ratio was as follows: occupation ratio (%) = (thinness of OPLL at most stenotic level/anteroposterior diameter of bony canal) × 100%.
MRI showed both the degree of spinal cord compression and the signal change of the spinal cord. The increased signal intensity (ISI) on T2-weighted MRI was classified into three grades: grade 0, none; grade 1, light or obscure; and grade 2, intense or bright. We also used this three-grade classification of ISI in this study.
Definition of PCS
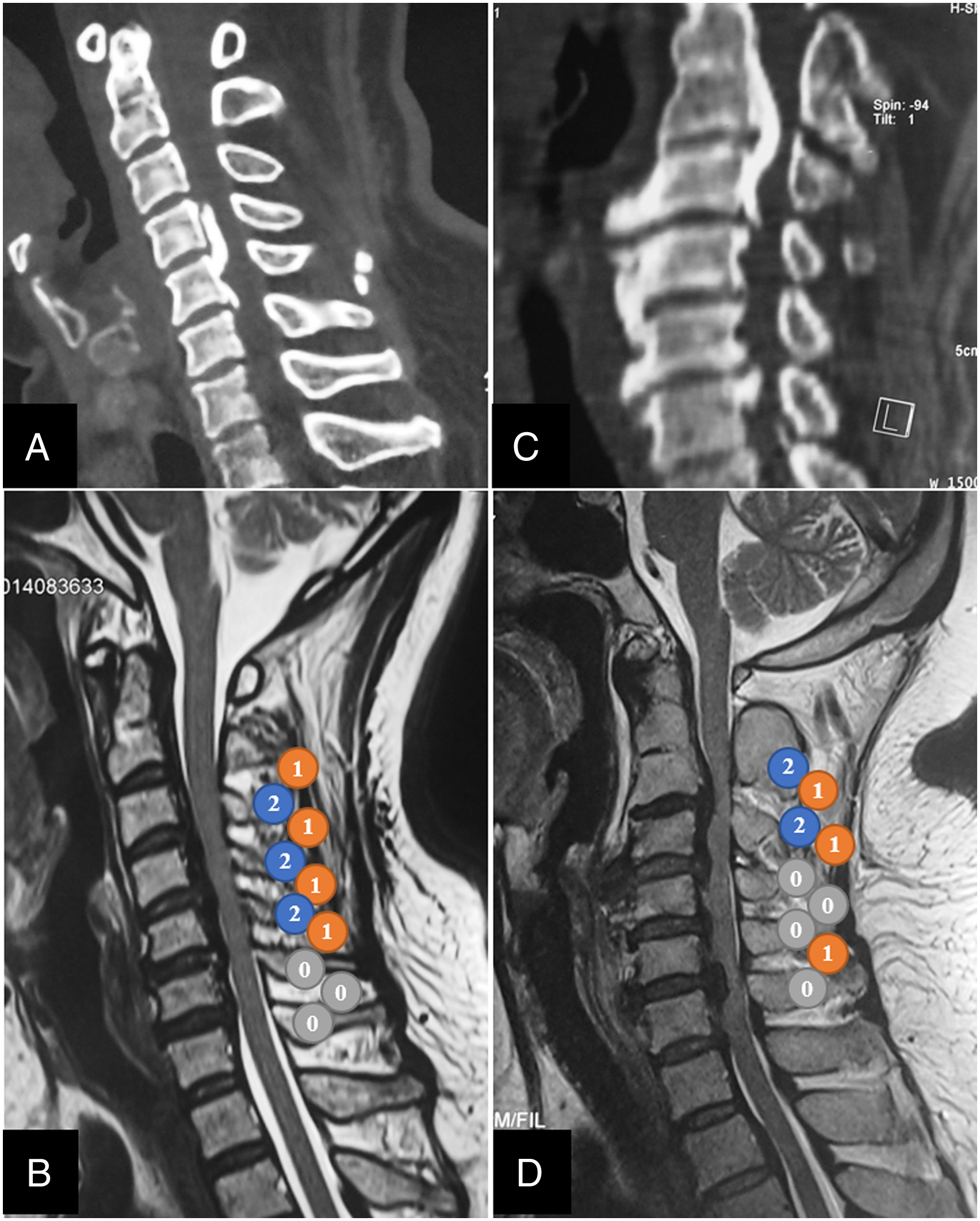
The PCS is a novel scoring system for evaluating posterior compression of the cervical spinal cord, which is measured on sagittal T2-weighted images of cervical MRI in patients with OPLL. There exists posterior compression when the dorsal CSF signal disappears. PCS is defined as the sum of compression at each cervical interlaminar and laminar level. The compression of the spinal cord at the laminar level was mainly the posterior bony structure (rigid), while the compression of the spinal cord at the interlaminar level was mainly ligamentous hypertrophy (soft). Therefore, we presumed that the compression at the laminar level was more severe than that at the interlaminar level. For each level, the PCS will be defined as 0 points if no compression was found, 1 point if the compression is at the interlaminar level, and 2 points if compression is at the laminar level (Figure 2). PCS was evaluated by two independent experienced surgeons in the spine imaging. The concordance between the two observers in calculating PCS on sagittal T2-weighted images was Kappa = .928 (P < .001). The two observers confirmed the final PCS by consensus. The average PCS of 282 patients in this study was 7.59. And we investigated the postoperative outcomes with a cutoff value of either 7 or 8 points. We found that there were no significant differences in postoperative clinical and radiological outcomes after propensity score matching with a cutoff value of 7. While, the postoperative outcomes showed statistical difference with a cutoff value of 8 (Supplementary Table 1). So, the patients were divided into two groups, the high-score (HS) group with PCS ≥ 8 (Figure 3A, B) and the low-score (LS) group with PCS < 8 (Figure 3C, D). Schematic drawings of the posterior compression score of the spinal cord (PCS). PCS is measured on sagittal T2-weighted images of cervical MRI in patients with OPLL. PCS will be defined as 1 point if the compression is at the interlaminar level; and PCS will be defined as 2 points if compression is at the laminar level. Representative computed tomography and magnetic resonance imaging (MRI) images of the patients with high posterior compression score of the spinal cord (PCS) and low PCS. (A, B) Representative cervical CT and MRI images of a 44-year-old female in the HS group. The PCS was calculated as 10 points as shown in the sagittal view of MRI image (B). (C, D) Representative cervical CT and MRI scans of a 42-year-old female in the LS group. The PCS was calculated as 7 points as shown in the sagittal view of MRI image (D).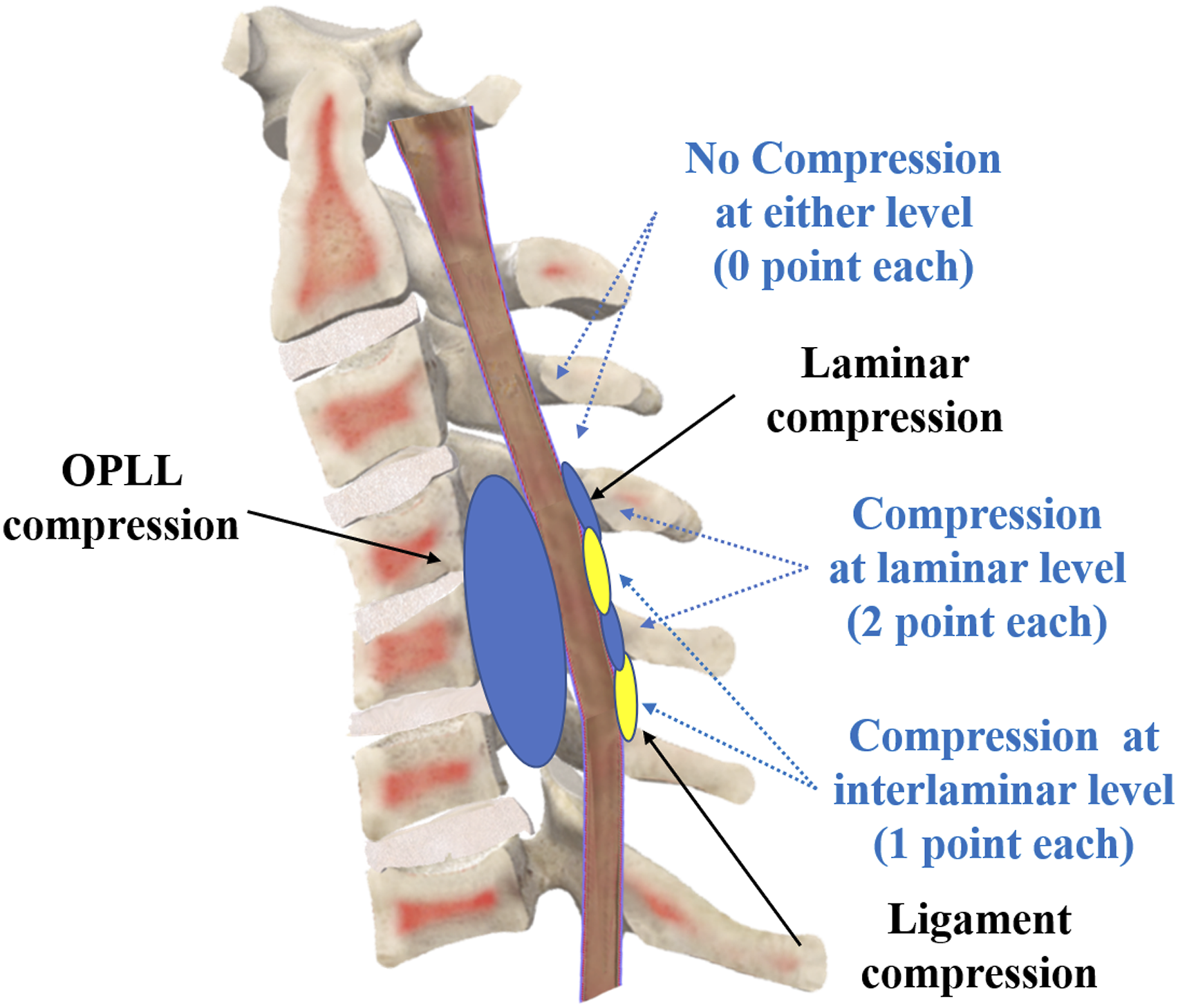
Propensity Score Matching
Baseline Demographical and Clinical Characteristics of All Patients Before and After Propensity Score Matching.
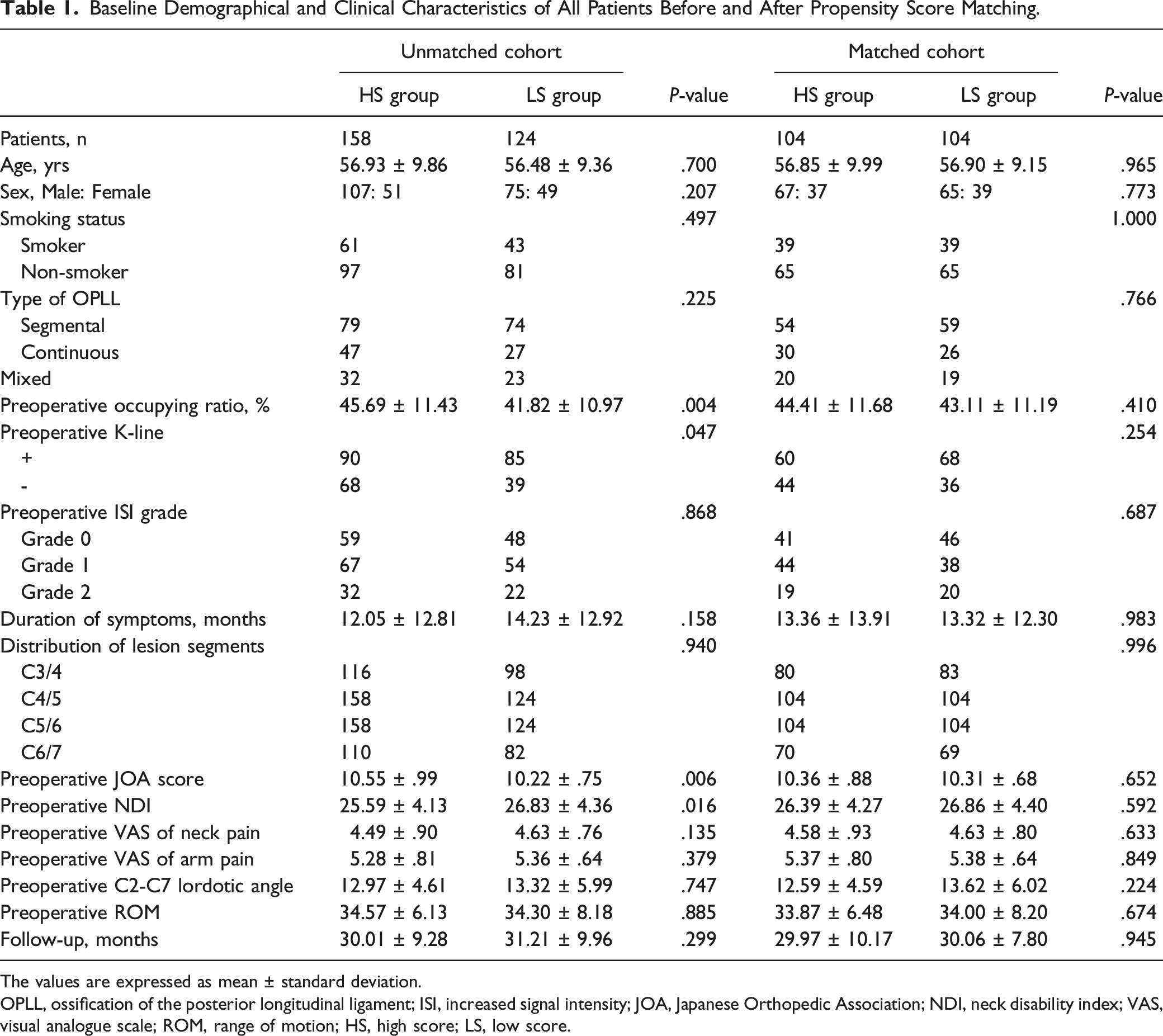
The values are expressed as mean ± standard deviation.
OPLL, ossification of the posterior longitudinal ligament; ISI, increased signal intensity; JOA, Japanese Orthopedic Association; NDI, neck disability index; VAS, visual analogue scale; ROM, range of motion; HS, high score; LS, low score.
Clinical and Radiological Outcomes of Patients After Propensity Score Matching.
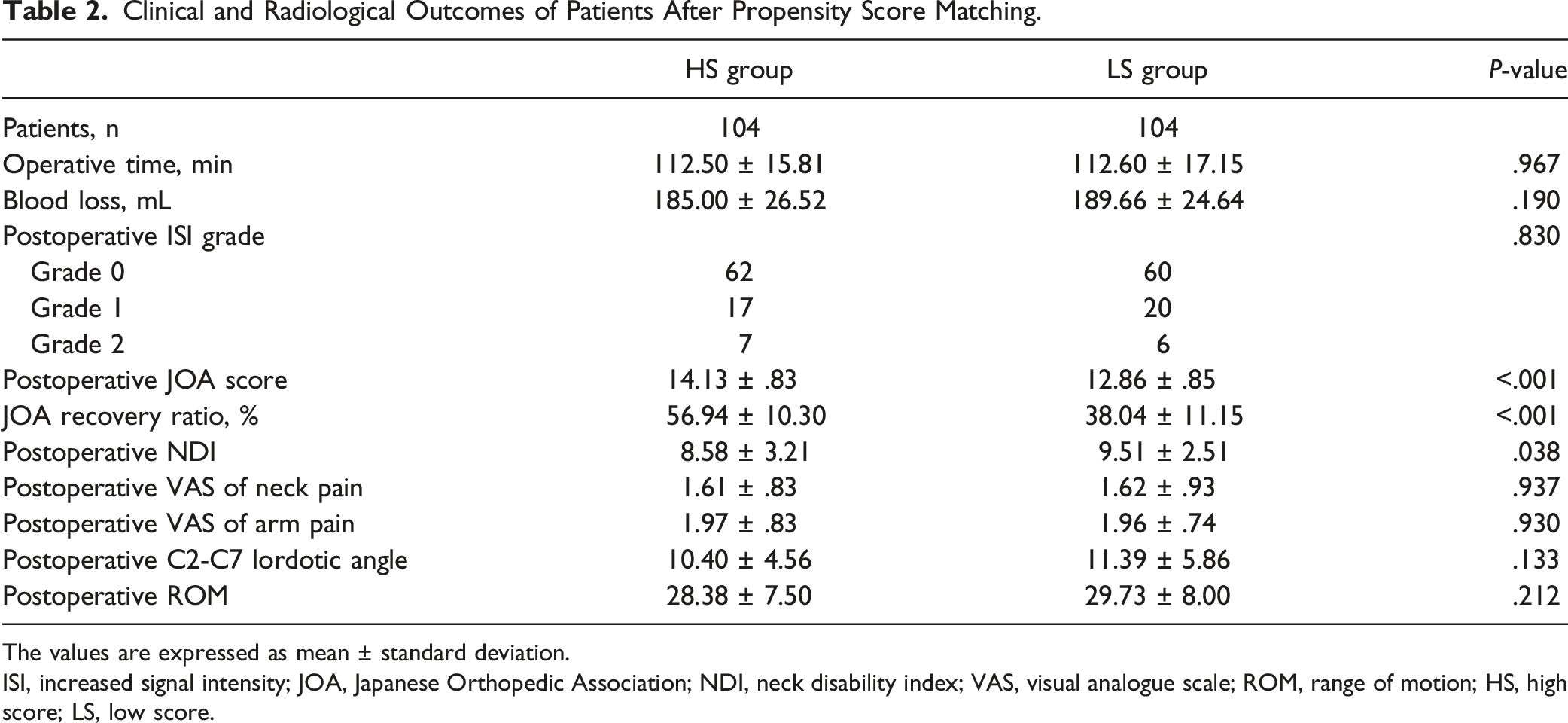
The values are expressed as mean ± standard deviation.
ISI, increased signal intensity; JOA, Japanese Orthopedic Association; NDI, neck disability index; VAS, visual analogue scale; ROM, range of motion; HS, high score; LS, low score.
Statistical Analysis
All the data were analyzed by using SPSS, version 25 (IBM Statistics, New York, USA). Means and standard deviations are presented for continuous variables, while frequencies and percentages were calculated for categorical variables. Independent-samples Student's t test or the Mann–Whitney U test was used to compare differences in continuous variables between the HS group and LS group, and the chi-square test or Fisher’s exact test was used to investigate differences between the two groups in categorical variables. Cohen’s Kappa was used to evaluate interobserver reliability for PCS. Kappa values of .81-1.00 were considered perfect agreement. P values of ≤ .05 were regarded as statistically significant.
Results
A total of 282 patients with cervical OPLL were included in this cohort study (Figure 1). Their mean age was 56.73 years (30-78); 182 were male (64.50%), and 100 were female (35.50%). A total of 158 (56.03%) patients had a high PCS of ≥8, and 124 (43.97%) patients had a low PCS of <8. PCS was evaluated by two independent experienced surgeons in spine imaging, and the concordance between the observers in calculating PCS on sagittal T2-weighted images was Kappa = .928 (P < .001), which showed good interobserver reliability for the PCS method. There were significant differences between the two groups regarding the preoperative occupying ratio (P = .004), preoperative K-line (P = .047), preoperative JOA score (P = .006), and preoperative NDI (P = .016) (Table 1). After propensity score matching, 208 patients (73.76%) were matched with 104 patients in each group. There were no significant differences between the two groups with regard to preoperative occupying ratio, K-line, JOA score, and NDI (Table 1). This showed that propensity score matching attenuated the confounding factors and that the two groups were comparable.
After matching, there were no significant differences in the intraoperative data between the HS and LS groups. The operative time was 112.50 ± 15.81 minutes in the HS group and 112.60 ± 17.15 minutes in the LS group (P > .05). The blood loss was 185.00 ± 26.52 mL in the HS group and 189.66 ± 24.64 mL in the LS group (P > .05). The postoperative ISI grade was similar in both groups. In the HS group, the postoperative MRI showed 62 patients in Grade 0, 17 patients in Grade 1, and 7 patients in Grade 2. In the LS groups, the postoperative MRI showed 60 patients in Grade 0, 20 patients in Grade 1, and 6 patients in Grade 2 (Table 2).
There were significant differences in the clinical outcomes between the HS and LS groups, except for postoperative VAS scores for neck and arm pain. The postoperative JOA score and its recovery rate were both significantly higher in the HS group (P < .001), while the postoperative NDI was significantly lower in the HS group (P = .038). In addition, there were no significant differences in the postoperative C2-C7 lordotic angle or ROM between the groups.
Subgroup Analysis of Clinical and Radiological Outcomes of Patients After Propensity Score Matching by Gender.
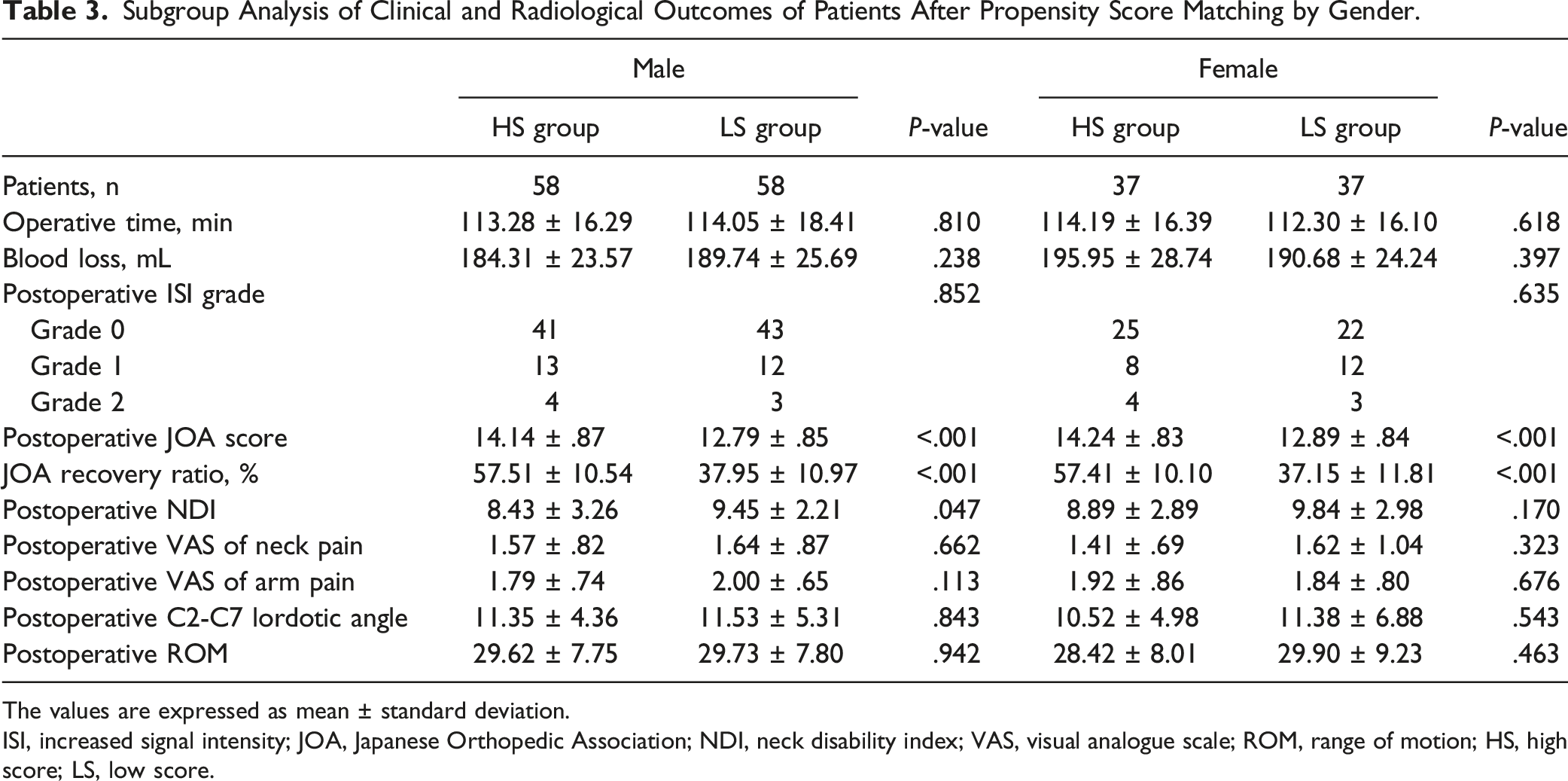
The values are expressed as mean ± standard deviation.
ISI, increased signal intensity; JOA, Japanese Orthopedic Association; NDI, neck disability index; VAS, visual analogue scale; ROM, range of motion; HS, high score; LS, low score.
Discussion
In this study, we described a novel evaluation method, the PCS, to evaluate the surgical outcome of LAMP-treated OPLL. The idea of establishing this scoring system originates from the indirect decompression nature of open-door LAMP. Since open-door LAMP relieves spinal cord compression by backshifting the spinal cord, whether the dorsal part of the spinal cord is compressed or whether the compressed dorsal cord is against laminar (hard bone tissue) or interlaminar tissue (ligament and other soft tissue) may be important to the severity of spinal cord impairment and the extent of backshifting after surgical treatment. In comparison, the K-line mainly assesses whether anterior compression is severe while considering the alignment. Here, we evaluated the PCS system and showed that the postoperative neurological outcomes, including the JOA score, recovery rate, and NDI, were significantly better after LAMP in the HS group than in the LS group. Further subgroup analysis found that the postoperative NDI was significantly lower in the HS group for the male patients, but not female patients. Therefore, PCS is a simple and fast scoring system for prognostic prediction for patients with cervical OPLL, especially for males.
LAMP is a common surgical technique for OPLL, which has the advantages of maintaining segmental motion without sacrificing cervical stability. However, the surgical outcomes after LAMP vary from poor to better neurological recovery for OPLL patients.10,11 Fujiyoshi et al 6 reported that the K-line was a practical index for making surgical decisions for OPLL patients. They found that an insufficient posterior shift of the spinal cord was the reason for the poor neurological improvement in the K-line (-) OPLL patients. The K-line has been widely used as an indicator for surgical outcomes in OPLL patients. Nevertheless, Tsujimoto et al 12 recently found that 10 patients classified as K-line (-) achieved favorable neurological outcomes (JOA recovery rate ≥50%) after LAMP. The portion of these exceptional K-line (-) patients was nearly 1/3 (10 of 31 patients). Furthermore, two other recent studies reported that the postoperative JOA recovery rate was similar between the K-line (+) and K-line (-) groups after posterior surgeries.7,8 These findings revealed that the K-line might be unable to predict surgical outcomes for OPLL patients. The K-line is focused on evaluating the ventral compression of the cervical spinal cord, neglecting the dorsal compression of the cervical spinal cord. Thus, we proposed a new evaluation method, the PCS, to evaluate the posterior compression of the cervical spinal cord. Our results showed that patients with high PCS scores achieved better neurological recovery than patients with low PCS scores. One possible explanation for better neurological outcomes after LAMP in patients with high PCS is that patients with more severe preoperative dorsal compression can achieve an adequate posterior shift of the cervical spinal cord after LAMP, regardless of the K-line. However, patients with less preoperative dorsal compression have spinal compression mainly on the ventral side. In these cases, LAMP may not provide sufficient ventral decompression of the spinal cord.
A previous study reported that the incidence of OPLL is more frequent in males than females, with a ratio of 2:1. 13 In our study, there were 182 males (64.50%) and 100 females (35.50%), the ratio is consistent with the previous report. During the study, we performed a subgroup analysis of surgical results by sex. We found that patients with high PCS scores and low PCS scores had significantly different postoperative JOA scores and recovery rates, regardless of sex. However, in contrast to males, there was no significant difference in postoperative NDI between the HS group and LS group in the female patients. Therefore, the PCS was a more useful predictor for male patients. The possible reason for the sex difference is that male patients tend to have a larger spinal canal diameter and more symptomatic tolerance for disease progression than female patients, which means that male patients may have more severe conditions of OPLL when symptoms occur.14,15
Currently, surgical decompression for OPLL can be achieved by using anterior or posterior approaches.16,17 Anterior approaches include anterior cervical corpectomy with fusion (ACCF), anterior controllable ante-displacement and fusion (ACAF), and vertebral body sliding osteotomy (VBSO).18-20 Posterior approaches include LAMP, laminectomy, and posterior decompression with instrumented fusion.8,21,22 However, the optimal surgical approach for OPLL remains unclear and controversial. 23 In our results, patients with high PCS can gain favorable neurological recoveries after LAMP. Instead, patients with low PCS might have satisfactory neurological outcomes using anterior approaches.
There were some limitations in our study. First, this study was a retrospective study, although we used propensity score matching analysis to reduce selection bias. Second, the sample size of our study was relatively small. Further prospective studies are required to confirm the efficacy of this novel index.
Conclusion
This study demonstrated that patients with high PCS scores showed better clinical outcomes than patients with low PCS scores, including neurological recovery and disability, especially in male patients. The novel PCS is a simple and fast scoring system for surgical decision-making for patients with cervical OPLL.
Key Points
1. We proposed a novel index, PCS, which evaluates the dorsal compression of the cervical spinal cord, regardless of the K-line. 2. Cervical OPLL patients were classified into the high PCS (HS) group and low PCS (LS) group. 3. Patients with high PCS can achieve favorable clinical outcomes, including neurological recovery and disability, especially for male patients. 4. The novel PCS is a simple and fast score system for surgical decision-making for patients with cervical OPLL.
Supplemental Material
Supplemental Material - A Novel Posterior Compression Score System for Outcome Prediction in Laminoplasty Treated OPLL Patients: A Propensity-Matched Analysis
Supplemental Material for A Novel Posterior Compression Score System for Outcome Prediction in Laminoplasty Treated OPLL Patients: A Propensity-Matched Analysis by Leixin Wei, Peng Cao, Chen Xu, Bo Hu, Huiqiao Wu, Ye Tian, Huajiang Chen, Xiaolong Shen, and Wen Yuan in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82002335, 81972088, 82172470, 81902234, 81871802, 82072469, 81772376, 82072471), Shanghai Shenkang hospital development center clinical innovation project (SHDC2020CR6018), Shanghai Science & Technology Commission Rising-Star Program (20QA1409200), Excellent academic leader project (21XD1404800) and Shanghai Changzheng Hospital Clinical Innovation Project (2020YLCYJ-Z04).
Ethical Approval
This study was approved by ethics committee (Shanghai Changzheng Hospital, IRB number: 2021SL044). Each author certifies that the institution approved the human protocol for this investigation and that all written informed consent was obtained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.