
Abstract
Study Design:
Retrospective clinical study.
Objective:
We evaluated the relationship between cervical sagittal alignment parameters and clinical status in patients with cervical myelopathy and analyzed the effect of cervical sagittal balance on cervical laminoplasty.
Methods:
Patients with cervical myelopathy (n = 110) who underwent laminoplasty were included in this study. The relationship between cervical sagittal alignment parameters and clinical status was evaluated. The changes in radiographic cervical sagittal parameters and clinical status 2 years after surgery were compared between patients with preoperative C2-7 SVA ≥35 mm (group A) and those with preoperative C2-7 SVA <35 mm (group B).
Results:
Preoperatively, C2-7 SVA had no correlation with defined health-related quality of life evaluation scores. At 2-year follow-up, the improvement in SF-36 physical component summary was significantly lower in group A than in group B. The postoperative change of C2-7 SVA did not significantly differ in 2 groups. Patients in group A maintained cervical regional balance after laminoplasty but experienced extensive postoperative neck pain.
Conclusions:
Our patients with a C2-7 SVA of ≥35 mm maintained cervical regional balance after laminoplasty and their improvement in myelopathy was equivalent to that in patients with a C2-7 SVA of <35 mm. However, the patents with a C2-7 SVA of ≥35 mm experienced severe postoperative neck pain. C2-7 SVA is a parameter worth considering because it can lead to poor QOL and axial neck pain after laminoplasty.
Keywords
Introduction
The importance of normative global spinal and pelvic parameters for quality of life (QOL) has been established. Proper sagittal balance of the physiologically upright spine maintains alignment with minimum energy expenditure against the global axis of gravity. Global spinal imbalance in the sagittal plane may lead to development of clinical symptoms and degenerative disease, which could require additional perioperative care of treated patients. 1 –3 However, relatively few publications have defined normative values for cervical or thoracic sagittal balance, and even fewer have directly evaluated the influence of cervical segmental and regional balance on outcomes in cervical surgery. 4 –7 Scheer et al provided a definition of the cervical sagittal vertical axis (C2-7 SVA) that refers to the distance between a plumb line dropped from the centroid of C2 (or dens) and the posterosuperior aspect of C7. 7 This parameter is expected to provide a measure of cervical regional balance. However, there are few reports on the relationship between C2-7 SVA and lumbar-pelvic sagittal alignment parameters, and it is unclear if C2-7 SVA influences clinically defined health-related QOL (HRQOL).
Cervical myelopathy frequently requires surgical treatment because its natural course results in poor clinical outcomes. Laminoplasty is a posterior method, and maintenance of both preoperative and postoperative lordotic alignment is a prerequisite for successful surgery in patients with cervical myelopathy. Unfortunately, patients who undergo laminoplasty tend to experience kyphotic alignment changes postoperatively despite sufficient preoperative lordosis, and such changes can adversely affect surgical outcomes and require additional surgery. 8 –10 Therefore, it is important to understand the factors predisposing postoperative cervical malalignment changes. Some authors have reported that cervical sagittal imbalance defined on the C2-7 SVA will adversely affect surgical outcome for cervical myelopathy. 11,12 However, it is unclear whether this cervical regional balance affects the cervical alignment and surgical outcomes of laminoplasty for cervical degenerative diseases, including cervical myelopathy. The purpose of this study was to evaluate the relationship between cervical sagittal parameters, including C2-7 SVA, and clinical status in patients with cervical myelopathy and analyze the effect of cervical sagittal balance on cervical posterior decompression (laminoplasty).
Methods
The study protocol was approved by the Institutional Review Board of Osaka City General Hospital. Written informed consent was obtained from the patients for publication of current research and any accompanying images.
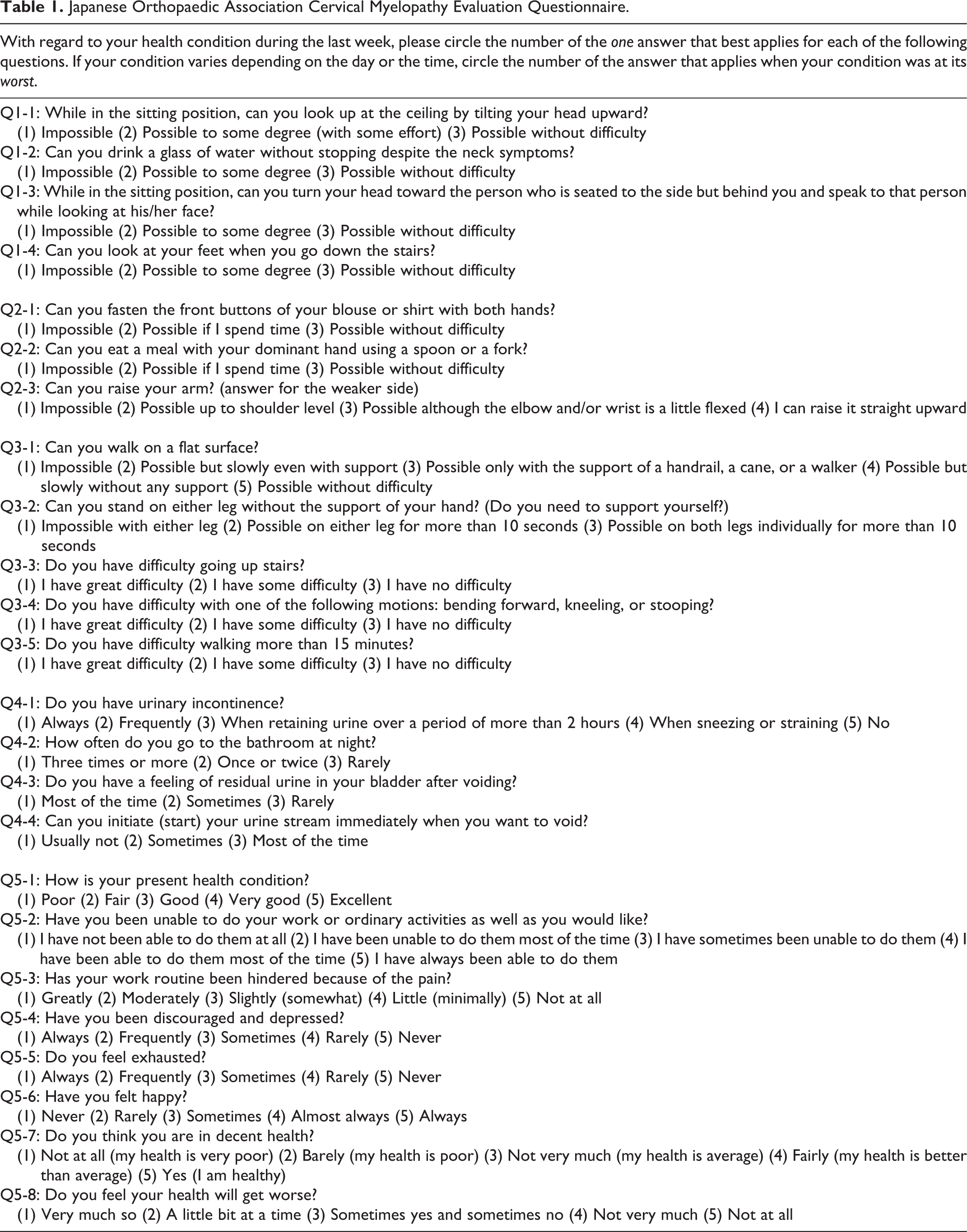
One hundred and ten patients with cervical myelopathy who underwent laminoplasty using the open-door technique at our institution between 2008 and 2012 were included in this study (39 women, 71 men; mean age, 66.7 years; follow-up, 2 years). The underlying pathologies comprised cervical spondylotic myelopathy (n = 94) and segmental posterior longitudinal ligament ossification (n = 16). Patients with complications of thoracolumbar spine or lumbar spine lesions were excluded. The laminoplasty involved C3-C7 in 37 cases and C3-C6 in 73 cases. Patients wore a collar for 10 days after surgery, and isometric cervical muscle exercises were started after collar removal. We checked clinical status and performed radiographic evaluation of the patients before surgery and 2 years postoperatively. Clinical outcomes were evaluated by using the Japanese Orthopaedic Association (JOA) score, and the recovery was calculated by using Hirabayashi’s method. 13 Patient HRQOL was assessed by using the visual analogue scale for neck pain and shoulder stiffness (VAS; 0-100), the JOA Cervical Myelopathy Evaluation Questionnaire (JOACMEQ), and the Short Form-36 (SF-36). 14,15 The JOACMEQ is a self-reported questionnaire to be completed by the patient, with the major criterion for evaluation being patient-oriented outcomes (Table 1). The JOACMEQ comprises 5 subscales: neck function (Q-1 part), upper extremity function (Q-2 part), lower extremity function (Q-3 part), bladder disturbance (Q-4 part), and QOL (Q-5 part). Each subscale is calculated from 0 to 100 points, and a higher value reflects better function. On SF-36, the physical component summary (PCS), mental component summary, physical functioning domain, and bodily pain domain were checked. The sagittal alignment was investigated by using lateral view roentgenograms of the standing total spine to evaluate C2-7 SVA, cervical lordosis (CL) defined by C2-7 angle, T1 slope, thoracic kyphosis (TK) defined by T1-T12 angle, lumbar lordosis (LL) defined by T12-S1 angle, sacral slope (SS), and SVA (Figure 1). Pelvic incidence (PI) was evaluated preoperatively. We investigated the relationship between cervical sagittal parameters and clinical status/HRQOL in patients with myelopathy preoperatively and 2 years postoperatively. In addition, the patients were allocated to 2 groups: patients with preoperative C2-7 SVA ≥35 mm (group A, n = 14) and those with preoperative C2-7 SVA <35 mm (group B, n = 96). The changes in radiographic cervical sagittal parameters, including C2-7 SVA, and clinical status/HRQOL at 2 years postoperatively were compared.
Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire.
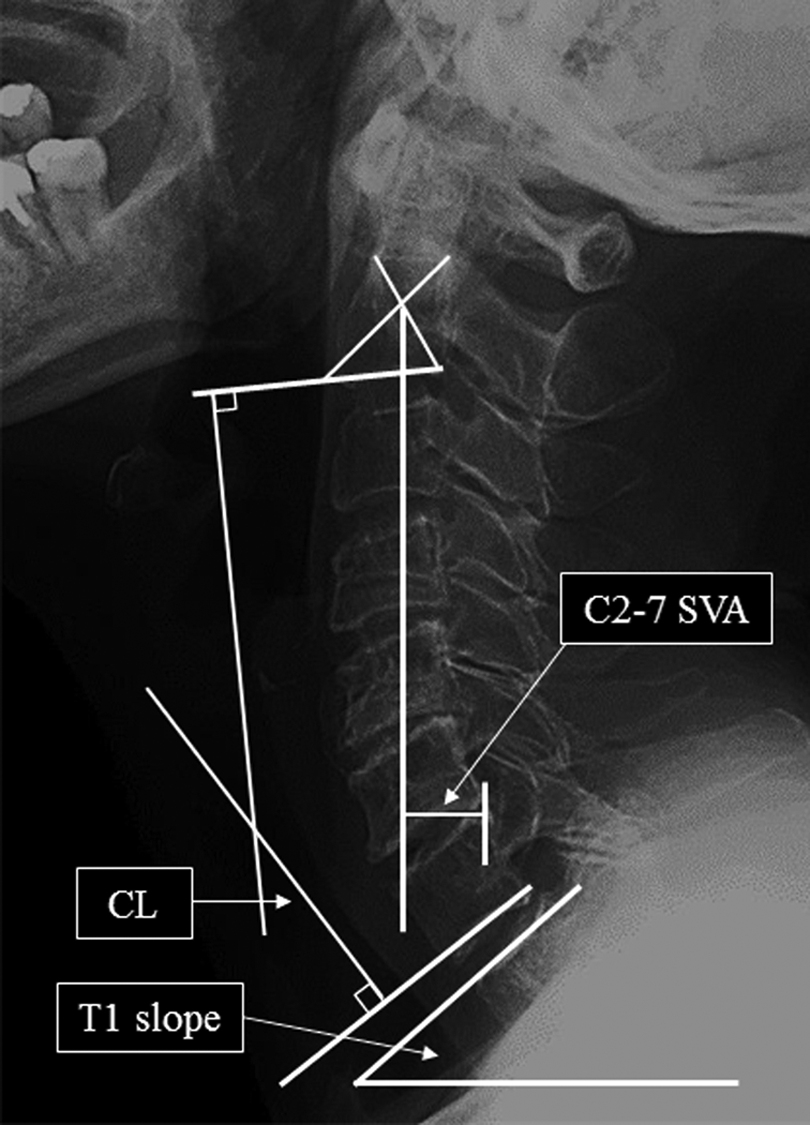
C2-7 sagittal vertical axis (C2-7 SVA), cervical lordosis (CL), and T1 slope were measured on whole-spine standing lateral radiographs. C2-7 SVA is defined as the distance from a plumb line drawn at the midpoint of the base of C2 to the plumb line drawn at the point of the superior dorsal aspect of the C7 vertebral body measured on a standing lateral cervical spine radiograph.
Statistical Analysis
Statistical analyses were performed by using the Mann-Whitney U test, paired t test, or Pearson product-moment correlation coefficient, as appropriate. All analyses were performed by using JMP 7.0 software (SAS Institute, Inc, Cary, NC). A P value <.05 was defined as indicating statistical significance.
Results
Relationship Between Cervical SVA and Other Sagittal Parameters, Clinical Status, and HRQOL
None of the studied patients presented with neurological deficits postoperatively required a second surgery because of worsening symptoms. Patients’ demographics and preoperative sagittal alignment parameters are shown in Table 2. The mean C2-7 SVA of all patients was 19.9 mm. The mean T1 slope was 22.4°. The relationship among the preoperative sagittal parameters are shown in Table 3. C2-7 SVA significantly correlated with CL (coefficient, −0.28), T1 slope (coefficient, 0.51), and TK (coefficient, 0.4). The T1 slope significantly correlated with CL (coefficient, 0.41) and TK (coefficient, 0.74). Cervical sagittal parameters were closely related to each other. C2-7 SVA was not related to lumbar and pelvic sagittal parameters (LL, SS, PI) and global sagittal balance (SVA).
Preoperative Demographic Data and Sagittal Alignment Parameter (N = 110).
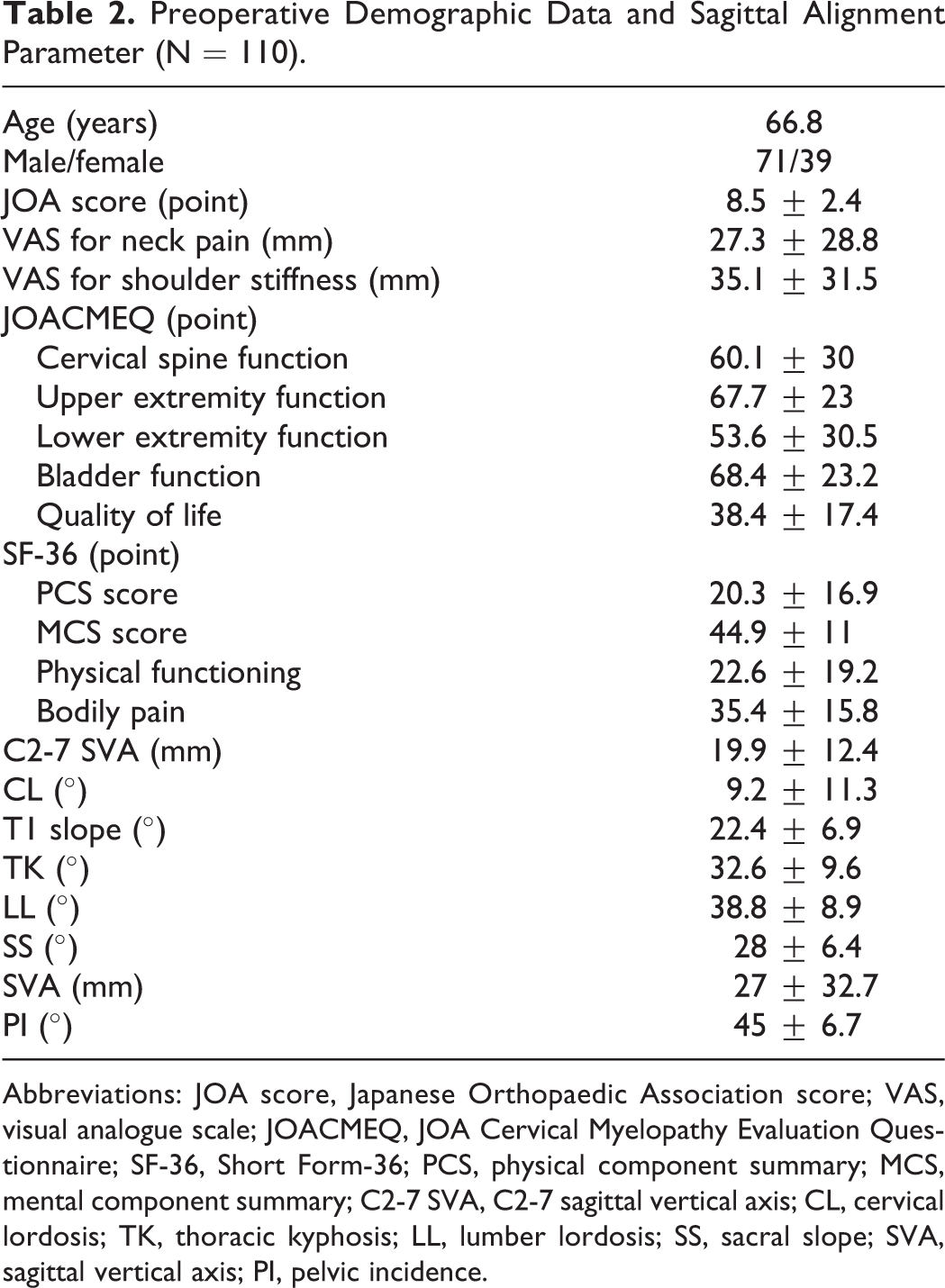
Abbreviations: JOA score, Japanese Orthopaedic Association score; VAS, visual analogue scale; JOACMEQ, JOA Cervical Myelopathy Evaluation Questionnaire; SF-36, Short Form-36; PCS, physical component summary; MCS, mental component summary; C2-7 SVA, C2-7 sagittal vertical axis; CL, cervical lordosis; TK, thoracic kyphosis; LL, lumber lordosis; SS, sacral slope; SVA, sagittal vertical axis; PI, pelvic incidence.
Relationship Among the Preoperative Sagittal Alignment Parametersa.
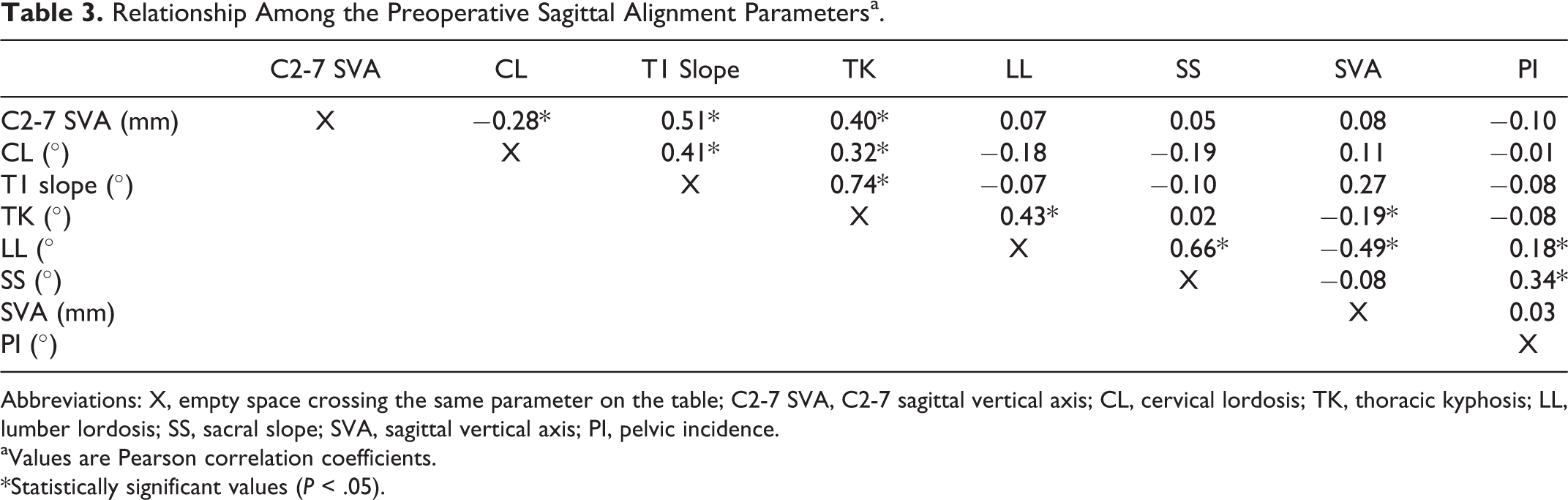
Abbreviations: X, empty space crossing the same parameter on the table; C2-7 SVA, C2-7 sagittal vertical axis; CL, cervical lordosis; TK, thoracic kyphosis; LL, lumber lordosis; SS, sacral slope; SVA, sagittal vertical axis; PI, pelvic incidence.
aValues are Pearson correlation coefficients.
*Statistically significant values (P < .05).
Preoperatively, C2-7 SVA had no correlation with clinical status/HRQOL evaluation scores (JOA score, VAS, JOACMEQ, and SF-36; Table 4). On the other hand, CL showed a slight significant correlation with upper extremity function and lower extremity function on the JOACMEQ, and there was a significant relationship between SVA and SF-36 PCS score (coefficient, −0.43).
Relationship Between Preoperative Sagittal Alignment Parameters and Clinical Status and HRQOLa.
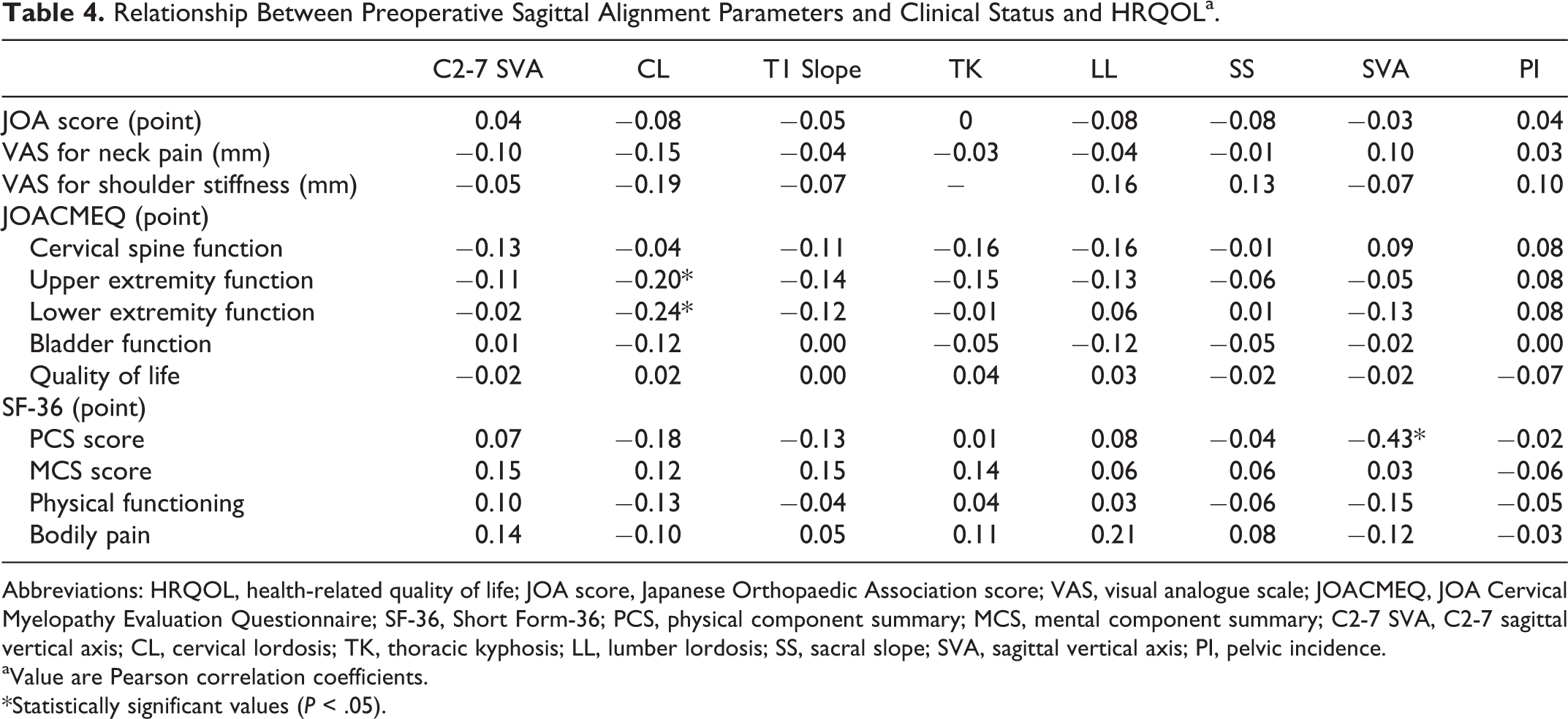
Abbreviations: HRQOL, health-related quality of life; JOA score, Japanese Orthopaedic Association score; VAS, visual analogue scale; JOACMEQ, JOA Cervical Myelopathy Evaluation Questionnaire; SF-36, Short Form-36; PCS, physical component summary; MCS, mental component summary; C2-7 SVA, C2-7 sagittal vertical axis; CL, cervical lordosis; TK, thoracic kyphosis; LL, lumber lordosis; SS, sacral slope; SVA, sagittal vertical axis; PI, pelvic incidence.
aValue are Pearson correlation coefficients.
*Statistically significant values (P < .05).
Effect of Cervical Sagittal Balance on Laminoplasty
Regarding the 2-year postoperative relationship between sagittal alignment parameters and clinical status/HRQOL, cervical sagittal parameters except CL had no correlation with clinical scores (JOA score, VAS, JOACMEQ, and SF-36). CL showed a slightly significant correlation just with the upper extremity function of the JOACMEQ (coefficient, −0.19). On the other hand, SVA significantly correlated with the upper/lower extremity function of the JOACMEQ (coefficient, −0.21/−0.28), SF-36 PCS (coefficient, −0.41), and physical functioning (coefficient, −0.35) at the 2-year follow-up after laminoplasty. Other pelvic sagittal parameters were not significantly related to clinical scores.
Regarding postoperative radiographic changes in the sagittal parameters of total materials, C2-7 SVA changed from 19.9 mm preoperatively to 23.8 mm at the 2-year follow-up; however, the postoperative change was not statistically significant. CL/T1 slope/TK changed from 9.2°/22.4°/32° to 6.2°/20.2°/31.2°. LL/SS/SVA changed from 38.8°/28°/27 mm preoperatively to 38°/26.9°/20.8 mm at the 2-year follow-up. These radiographic changes were not statistically significant.
In comparison of clinical outcome after laminoplasty between the 2 groups (Table 5), there was no significant difference of JOA score recovery rate between group A (47.3%) and group B (53.8%), and there was a trend toward larger increases in VAS scores for neck pain in group A (16.2 mm) than in group B (6.1 mm). The improvements to JOACMEQ cervical spinal function scores were −4.9 points and 5.7 points in groups A and B, respectively, and the difference of the improvement significantly differed in 2 groups. These results showed that refractory neck pain occurred after laminoplasty in group A. The improvement in SF-36 PCS was significantly lower in group A than in group B. The changes in the pre- and postoperative C2-7 SVA values were 0.6 mm and 4.3 mm in groups A and B, respectively (Table 6), but the difference was not significant. There was a significant difference in the CL change between the groups. There were no significant differences in the T1 slope, TK, LL, SS, or SVA changes between the groups. A representative case in group A is shown in Figure 2.
Change in Clinical Status/HRQOL in Patients After Laminoplasty.
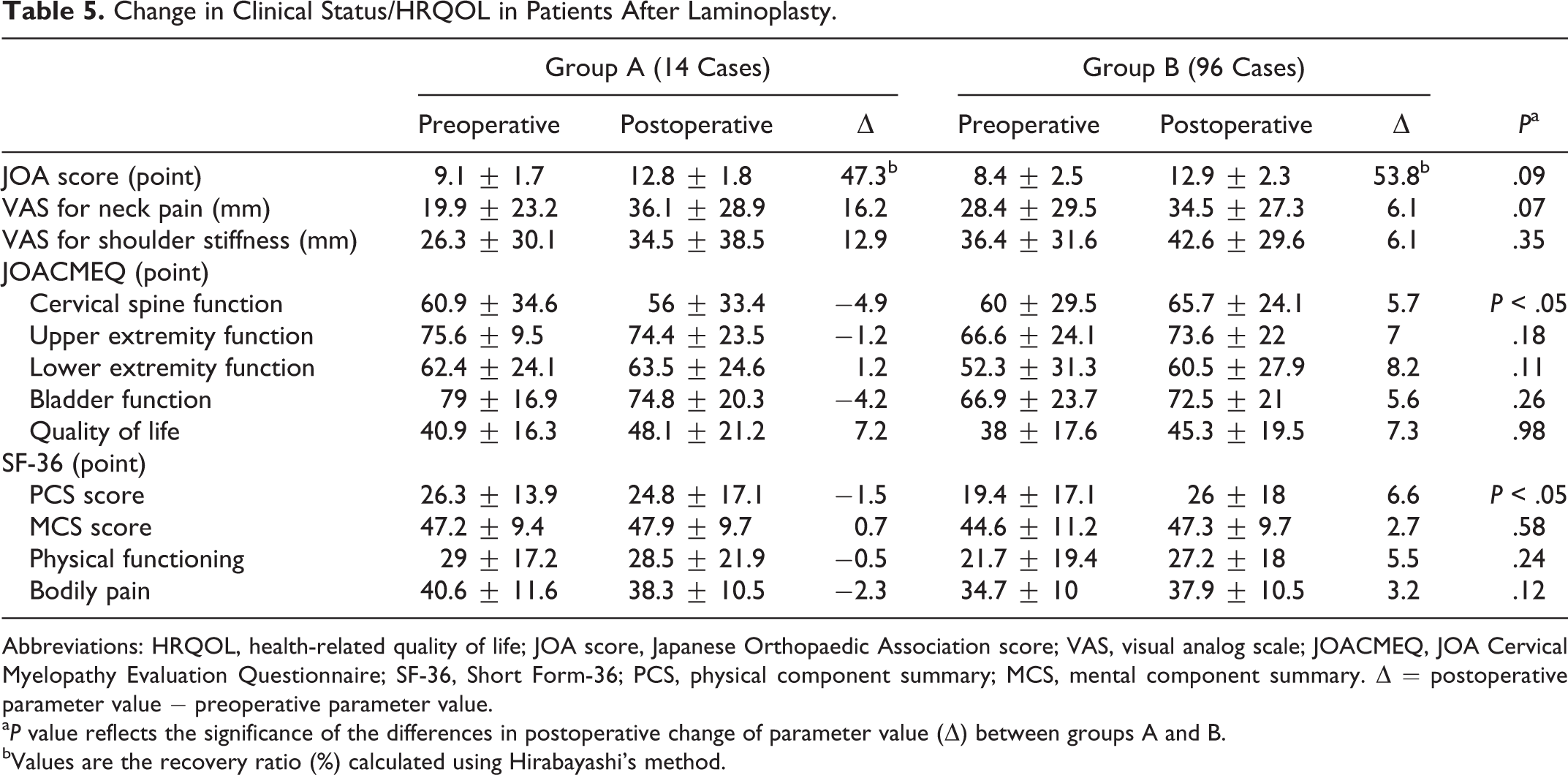
Abbreviations: HRQOL, health-related quality of life; JOA score, Japanese Orthopaedic Association score; VAS, visual analog scale; JOACMEQ, JOA Cervical Myelopathy Evaluation Questionnaire; SF-36, Short Form-36; PCS, physical component summary; MCS, mental component summary. ▵ = postoperative parameter value − preoperative parameter value.
a P value reflects the significance of the differences in postoperative change of parameter value (▵) between groups A and B.
bValues are the recovery ratio (%) calculated using Hirabayashi’s method.
Change in Sagittal Alignment Parameters in Patients After Laminoplasty.
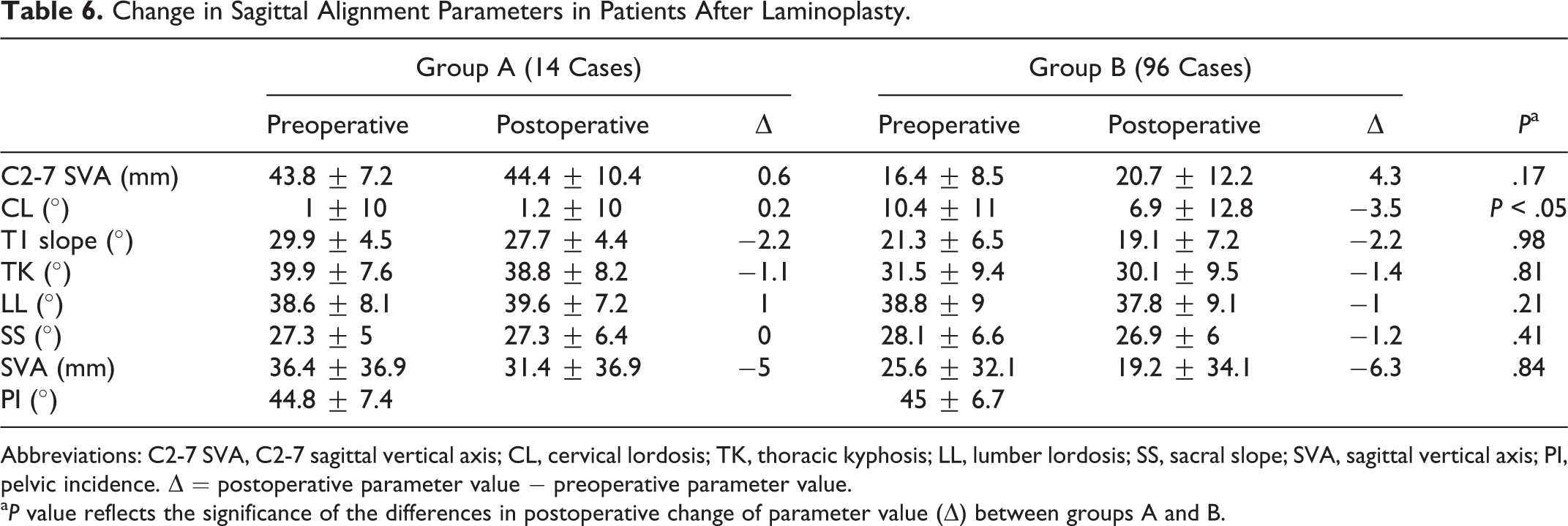
Abbreviations: C2-7 SVA, C2-7 sagittal vertical axis; CL, cervical lordosis; TK, thoracic kyphosis; LL, lumber lordosis; SS, sacral slope; SVA, sagittal vertical axis; PI, pelvic incidence. ▵ = postoperative parameter value − preoperative parameter value.
a P value reflects the significance of the differences in postoperative change of parameter value (▵) between groups A and B.
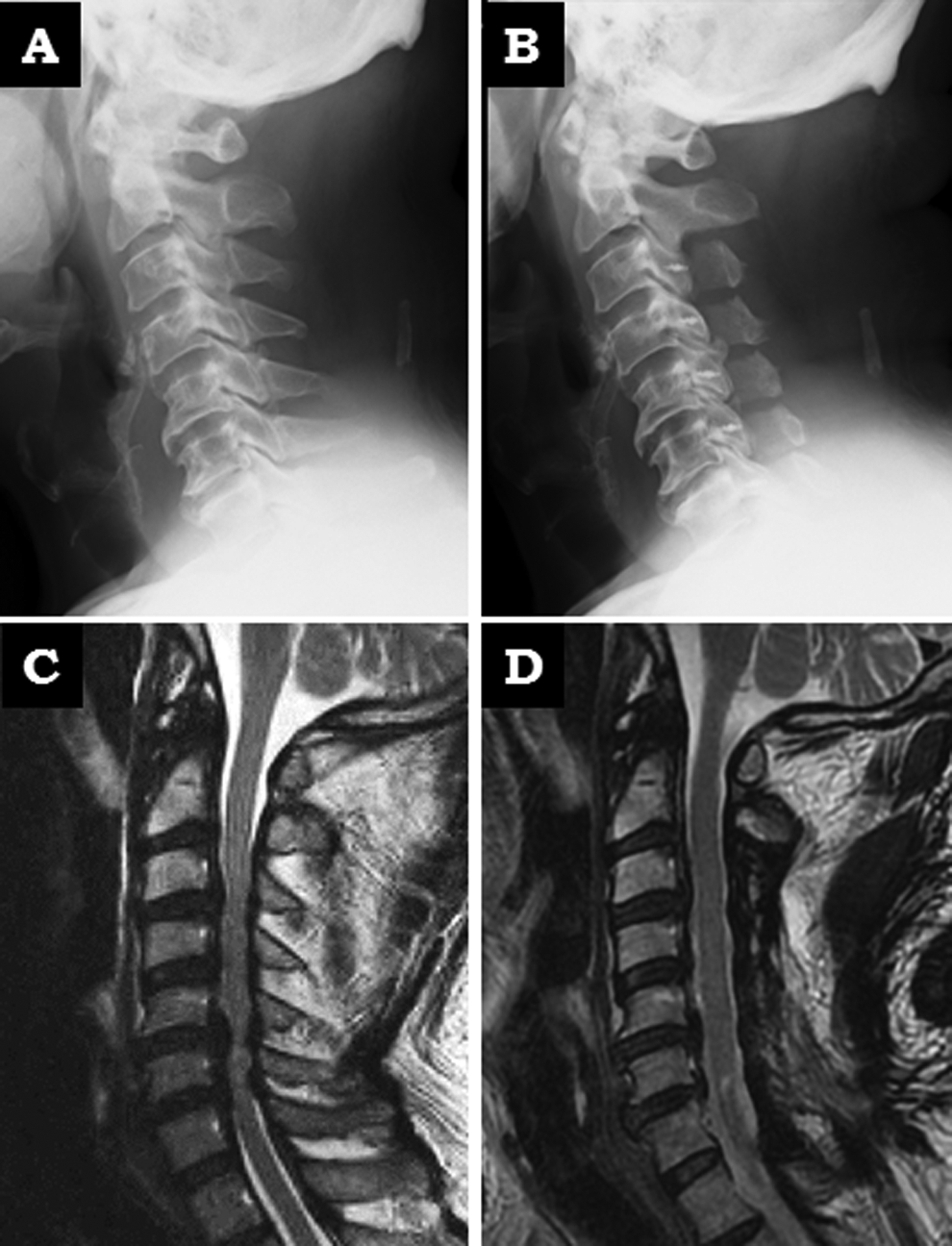
Representative case. A 70-year-old man with segmental posterior longitudinal ligament ossification reported hand clumsiness and gait disturbance with spasticity (JOA score of 8 points). After C3-7 laminoplasty, the patient’s hand clumsiness and gait disturbance improved, and his large C2-7 SVA (37 mm) was maintained at the 2-year follow-up after laminoplasty. The 2-year postoperative JOA score was 13 points (recovery ratio: 55.6%). However, he developed severe neck pain that resisted conservative treatment. The 2-year postoperative VAS for neck pain was 58 mm. The change of SF-36 PCS/neck function domain of the JOACMEQ was −3 points/−5 points postoperatively at 2 years. (A, B) Radiograph on lateral view of cervical spine (neutral position). A, preoperatively; B, at 2-year follow-up. (C, D) Sagittal T2-weighted magnetic resonance imaging of cervical spine. C, preoperatively; D, at 2-year follow-up.
Discussion
No advanced research has been conducted on cervical alignment or balance to characterize the global relationships in the spine. The reasons for this are that cervical spinal curvature varies, the motion of the cervical spine associated with the range is large, the connection between cervical alignment and thoracic kyphosis is weaker than that between the lumbar and pelvic regions, and the cervical region segments are often afflicted with myelopathy. 16 –18 Our preoperative results showed that the C2-7 SVA was strongly correlated with other cervical and thoracic sagittal parameters (CL, T1 slope, TK) but not with lumbar and pelvic sagittal parameters (LL, SS, PI) or global sagittal balance (SVA). Few reports have described the relationship between cervical and global sagittal alignment. 19 –21 Lee et al reported that there were significant relationships among the thoracic inlet angle, T1 slope, and C2-7 angle in asymptomatic volunteers. 21 Similarly, our data in patients with cervical myelopathy suggests that the C2-7 SVA has a significant relationship with other cervical and thoracic alignment parameters. Our data could provide a baseline for various clinical studies on myelopathy patients with cervical sagittal parameters.
Smith et al investigated how newer sagittal parameters, including C2-7 SVA or T1 slope, affect HRQOL and surgical outcomes in 56 patients with myelopathy. They determined the severity of C2-7 SVA with myelopathy by using modified JOA scores and stated that cervical sagittal balance, but not kyphosis, was associated with the myelopathy score. 4 However, in the present study, the C2-7 SVA did not correlate with preoperative JOA score and HRQOL score. The reason for that might be racial differences. Our average C2-7 SVA (19.9 ± 12.4 mm) in Japanese myelopathy patients was smaller than Smith’s (32.3 ± 14.5 mm) in North American myelopathy patients even though both were determined in myelopathy patients. 4 It should be noted that the small C2-7 SVA will hardly cause a difference in clinical status. SVA was the only sagittal parameter that related to SF-36 PCS scores in the myelopathy patients, preoperatively and postoperatively. We guess that it is difficult for myelopathy patients with spinal global imbalance to maintain their daily lives. The extent of the myelopathy influences the clinical status more than does cervical regional balance because the SF-36 questionnaires, which are based on activities of daily living and locomotion, relate much more to myelopathy than to cervical balance. It has not yet been established whether the context of cervical regional balance and global balance affect HRQOL in myelopathy patients, so further research is needed.
Whether sagittal imbalance of the cervical spine affects the clinical outcomes of cervical myelopathy operations is controversial. Some studies have shown that large C2-7 SVA negatively affects outcomes after operation for myelopathy. 11,12 Tang et al reported that the C2-7 SVA correlated significantly with SF-36 PCS and NDI scores, and the severity of disability increased with positive cervical sagittal malalignment following surgical reconstruction in 113 patients who received multilevel posterior cervical fusion. 11 This study examined the effect of cervical SVA on the changes in sagittal alignment parameters following laminoplasty. Laminoplasty is popular in patients with myelopathy in whom the cord is compressed at multiple levels. Our results showed that the JOA recovery ratio of patients in group A (with a C2-7 SVA of ≥35 mm) was improved in a manner similar to that of patients in group B (with a C2-7 SVA of <35 mm). However, although large C2-7 SVA had not deteriorated to the point of cervical regional balance after laminoplasty, patients in group A had significantly lower improvement scores in SF-36 PCS than patients in group B. In addition, patients in group A experienced extensive postoperative neck pain (axial pain) based by VAS for neck pain or neck functional domain of the JOACMEQ. The JOA scoring system focuses on the severity of myelopathy, as evaluated from an objective medical viewpoint, and has displayed problems of not sufficiently reflecting levels of patient satisfaction regarding QOL and treatment. Furthermore, other HRQOL evaluation scores are based on a self-reported questionnaire. Therefore, although the myelopathy of patients in group A improved by laminoplasty, these patients did not achieve an improvement in some HRQOL scores because of the potential impact of the postoperative neck pain on patient satisfaction and daily activities. A possible reason for postoperative axial pain after the cervical posterior approach is that it could damage cervical posterior elements, such as the lamina, nuchal ligaments, facet joints, and posterior neck muscles. 22 A cervical spine with large C2-7 SVA may be vulnerable of damage to the posterior elements because the posterior elements of the cervical spine could prevent the kyphotic alignment of structures that have been exposed to mechanical stress-induced sagittal imbalance. 12,23 Some cervical parameters, such as T1 slope, cervical regional kyphosis, and K-line, have been reported as important factors related to laminoplasty outcomes. 5,10,24 C2-7 SVA is a parameter worth considering because it can cause poor QOL and axial neck pain after laminoplasty.
Decompression (laminoplasty) is less invasive than fusion surgery as a surgical treatment for patients with degenerative cervical spine disease. However, our results indicated that laminoplasty alone might be not a good option for patients with large C2-7 SVA. Mitigation of postoperative axial pain in myelopathy patients with this condition is an important goal. Some authors have recommended realignment of imbalanced cervical spines by using an anterior approach with reconstruction and lordotic interbody spacers to restore the natural lordotic curve of the cervical spine. 12 However, anterior reconstruction surgery to realign the cervical spine might require a long fusion, which requires invasive surgery with high risks (ie, pseudoarthrosis, proximal junctional kyphosis, and instrument failure). The posterior approach procedure with spinal instrumentation, such as a lateral mass screw or a pedicle screw, has been reported to be favorable in patients with cervical kyphosis. 25 Posterior decompression and realignment fusion might reduce postoperative neck pain and be better for patients with C2-7 SVA ≥35 mm. Further research is needed to identify clearly suitable operations for these patients.
Our study had a number of limitations. First, this was a retrospective study, and the short follow-up period of 24 months was another limitation because cervical sagittal balance may have worsened over a longer follow-up. In addition, this study did not evaluate the effect of myelopathy severity on cervical balance, but this is important given the impact of myelopathy on patient function and HRQOL. Further studies with longer follow-up periods should be conducted to confirm the results of the present study. However, our results could provide valuable data for further studies on the effect of cervical sagittal parameters on myelopathy patients and surgical treatment. Future studies on the effect of cervical sagittal balance on laminoplasty should be conducted prospectively and consider a wide variety of factors.
Conclusions
In patients with cervical myelopathy, the C2-7 SVA was strongly associated with cervical and thoracic sagittal alignment parameters, including the CL, T1-slope, and TK, but not with lumbar and pelvic sagittal parameters (LL, SS, and PI) or global sagittal balance (SVA). Cervical SVA had no effect on daily life disabilities. SVA did affect the daily activities of myelopathy patients, such as asymptomatic volunteers or adult spinal deformity patients. Our patients with a C2-7 SVA of ≥35 mm maintained cervical regional balance after laminoplasty and their improvement in myelopathy was equivalent to that in patients with a C2-7 SVA of <35 mm. However, the patents with a C2-7 SVA of ≥35 mm experienced severe postoperative neck pain (axial pain). C2-7 SVA is a parameter worth considering because it can lead to poor QOL and axial neck pain after laminoplasty. Further discussion is needed in future for determining of the impact of cervical SVA on myelopathy in patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.