
Abstract
Study Design
Retrospective Single-center propensity score–matched cohort study.
Objective
Adjacent segment disease remains a major cause of revision surgery after multilevel lumbosacral fusion, and muscle-preserving approaches may help reduce this risk. This study compared clinical and radiographic outcomes between a muscle-preserving fusion combining standalone anterior plus lateral lumbar interbody fusion (A + LLIF) vs circumferential lateral plus posterior lumbar interbody fusion (L + PLIF).
Methods
Patients who underwent multilevel lumbosacral fusion (2016-2023) with either A + LLIF or L + PLIF were included. L + PLIF patients with contraindications to standalone A + LLIF were excluded. Propensity score matching, based on age, BMI, PI–LL mismatch and stenosis severity, yielded 90 1:1-matched patients. The primary outcome was revision surgery. Secondary outcomes included spinopelvic alignment, cage subsidence, and perioperative metrics.
Results
Baseline characteristics were comparable between groups (mean age 57 ± 10 years; median fusion levels: 2 [range 2-4]). The 5-year cumulative incidence of revision surgery was significantly lower with A + LLIF (1/45 events; 2.2%) than with L + PLIF (14/45 events; 31.1%; P < .001), with superior perioperative outcomes and comparable radiographic alignment.Operative time, blood loss, and length of stay were significantly lower in the A + LLIF group (P < .001 for all). Spinopelvic parameters were largely equivalent, except for improved distal lordosis and LPA–PI mismatch in the A + LLIF group (P = .003 and P = .019, respectively). Cage subsidence rates were low and similar between groups.
Conclusions
In carefully selected patients, combined standalone anterior and lateral interbody fusion offers a paraspinal muscle-preserving alternative to circumferential fusion, with significantly lower revision rates, favorable perioperative outcomes, and comparable radiographic alignment.
Keywords
Introduction
Degenerative disc disease is a leading cause of disability worldwide, most commonly affecting the lower lumbar spine and lumbosacral junction.1,2 As such, it represents the most common site of spine surgical intervention, yet fusion across the lumbosacral junction remains challenging due to high rates of mechanical complications, including pseudarthrosis and adjacent segment disease (ASD), driven by increased biomechanical stress on instrumented and adjacent levels. 3
Posterior pedicle screw instrumentation remains the gold standard for spinal reconstruction and fusion across the lumbosacral junction (Figure 1), but it is associated with paraspinal muscle injury and related drawbacks.4,5 Increasing evidence highlights the critical role of the paraspinal musculature in postoperative recovery, function, and ASD prevention.6,7 Consequently, there is growing interest in fusion techniques that minimize iatrogenic muscle disruption. Case Illustration of a Circumferential L + PLIF Procedure. (A) Preoperative T2-weighted MRI of a 65-year-old patient demonstrating right-sided foraminal stenosis at L4/5 and L5/S1 without significant central canal compromise. (B) Preoperative lateral radiograph showing multilevel degenerative disease with disc space collapse, most prominently at L4/5. (C) One-year postoperative radiograph after L + PLIF demonstrating restored disc height and segmental lordosis at L4/5 more than L5/S1
Anterior lumbar interbody fusion (ALIF) and lateral lumbar interbody fusion (LLIF) provide large anterior footprint support, restore segmental height and lordosis, and allow for indirect decompression.
8
Although these techniques are often supplemented with posterior instrumentation to improve construct stability,
9
when performed as standalone procedures, ALIF and LLIF offer muscle-preserving alternatives to conventional posterior fusion.10-12 We herein propose a combination of standalone ALIF at L5/S1 and standalone LLIF at more proximal levels (A + LLIF) as a comprehensive, muscle-preserving strategy for multilevel fusion across the lumbosacral junction (Figure 2). While this approach may carry risks related to reduced construct stability, such as cage subsidence and pseudarthrosis, its muscle-preserving nature may help mitigate the risk of adjacent segment revision surgery. Case Illustration of a Standalone A + LLIF Procedure. (A) Preoperative T2-weighted MRI of a 65-year-old patient. Midsagittal view shows multilevel disc degeneration. Axial view at L4/5 demonstrates moderate central canal stenosis. Foraminal views reveal right greater than left foraminal stenosis at L4/5 and L5/S1, as well as moderate bilateral foraminal stenosis at L3/4. (B) Preoperative lateral spine radiograph demonstrating multilevel degenerative changes with disc space collapse. (C) One-year postoperative radiographs following standalone A + LLIF showing restored disc height and segmental lordosis across all treated levels
The purpose of this study was to compare revision risk, as well as perioperative clinical and radiographic outcomes, between standalone A + LLIF and circumferential posterior fusion combining LLIF and posterior lumbar interbody fusion (L + PLIF) with pedicle screw instrumentation for multilevel lumbosacral degenerative disease.
Materials and Methods
Patient Population
This retrospective cohort study was conducted at a single academic institution. Institutional Review Board approval was obtained prior to study initiation (2020-1877). The study follows STROBE guidelines for reporting observational studies. 13 Patients who underwent multilevel lumbosacral fusion between August 2016 and January 2024 using either combined standalone A + LLIF or circumferential L + PLIF with pedicle screw instrumentation were included.
In the A + LLIF group, L5/S1 was treated with standalone ALIF and more proximal levels with standalone LLIF, without posterior instrumentation. In the L + PLIF group, L5/S1 was instrumented using PLIF and more proximal levels with LLIF, with pedicle screw instrumentation at all treated levels.
Exclusion criteria included prior lumbar fusion, fusion of five or more levels, and pathology unsuitable for standalone A + LLIF, defined as moderate to severe central canal stenosis (Schizas grade C or D), 14 isthmic lysis, spondylolisthesis of Meyerding grade 2 or higher. 14
In clinical practice, standalone A + LLIF is selected for patients with multilevel degenerative disease of the lower lumbar spine and lumbosacral junction who demonstrate mild to moderate central canal stenosis (Schizas grades A–B), symptomatic foraminal stenosis without severe sagittal imbalance, no isthmic defect, and spondylolisthesis of Meyerding grade ≤2, and in whom safe anterior and lateral access anatomy was present. Patients with more advanced stenosis, greater instability or deformity, or unfavorable anatomy for anterior or lateral approaches are preferentially treated with posterior instrumented fusion with posterior pedicle screw instrumentation.
Minimum clinical and radiographic follow-up was one year, except in cases of revision surgery within the first year, in which case no minimum follow-up was required. Preoperative imaging requirements included MRI and standing anteroposterior and lateral full-spine radiographs.
Surgical Technique
All procedures were performed by four experienced, board-certified spine surgeons. LLIF was performed using a mini-open transpsoas approach with the patient in the lateral decubitus position.14,15 ALIF procedures were performed with the patient in the supine position. PLIF and pedicle screw instrumentation were performed in the prone position via a midline open posterior approach.
Clinical Metrics
Baseline demographic characteristics, comorbidities, surgical details, and perioperative data were collected from the electronic medical record. The primary outcome was the incidence of revision surgery following the index lumbosacral fusion procedure. Secondary perioperative outcomes included operative time, estimated blood loss, and length of hospital stay.
Radiographic Evaluation
Preoperative MRI scans were reviewed to assess the severity of central canal stenosis at the levels treated using the Schizas classification 16 as follows: Grade A (no or minor stenosis): cerebrospinal fluid (CSF) is clearly visible in the dural sac surrounding the rootlets. Grade B: (moderate stenosis): some CSF is still visible and rootlets can be recognized, but they occupy the whole of the dural sac. Grade C (severe stenosis): No CSF visible and no rootlets are visible, epidural fat remains. Grade D (extreme stenosis): No CSF and nod rootlets visible, epidural fat is obliterated.
Preoperative and one-year postoperative standing lateral spine radiographs were evaluated with commonly used spinopelvic alignment metrics.17,18 Global spinopelvic parameters included lumbar lordosis (LL), measured from the superior endplate of L1 to S1; pelvic incidence (PI); pelvic tilt (PT); PI-LL mismatch 17 ; L1 lumbar pelvic angle (LPA); and the difference between ideal and measured LPA, calculated as: (0.5 x PI) - 21 - LPA. 19 Distal spinopelvic alignment included the distal lordosis (DL) between the upper endplate of L4 and sacral endplate; Lordosis Distribution Index (LDI = DL/LL), 20 and the DL/PI ratio. 21
Cage subsidence was assessed on one-year postoperative standing lateral radiographs and graded according to the Marchi et al. 22 classification which grades the relative amount of cage height subsided into the vertebral endplates as follows: Grade 0: 0-24%; Grade I: 25-49%; Grade II: 50-74% or Grade III: 75-100%. Subsidence was evaluated for LLIF cages only, because the differing geometry and radiographic appearance of ALIF and PLIF cages would make direct comparison across cage types unreliable using a single grading system.
Statistical Analysis
All analyses were performed using Stata/BE 18.0 (StataCorp LLC, College Station, TX, USA). Continuous variables were assessed for normality using histograms and Q–Q plots. Normally distributed data are reported as mean ± standard deviation and compared using Student’s t-tests. Non-normally distributed data are reported as median with interquartile range (IQR) and compared using Wilcoxon rank-sum tests. Categorical variables were compared using chi-square or Fisher’s exact tests, as appropriate. One-to-one propensity score matching was performed based on age, body mass index (BMI), preoperative PI–LL mismatch, and stenosis severity (Schizas grade), using a nearest-neighbor approach.
Kaplan–Meier survival curves and log-rank tests were used to compare survival distributions between groups. Cox proportional hazards regression models were constructed, and annual revision incidence was calculated using person-time analysis and reported as events per 100 person-years. Hazard ratios (HRs) with 95% confidence intervals (CIs) were reported. The proportional hazards assumption was verified using Schoenfeld residuals.
As a sensitivity analysis, the survival analysis was repeated in the unmatched cohort to assess whether differences in revision risk persisted. To account for multiple hypothesis testing, a false discovery rate (FDR) correction was applied to postoperative alignment parameters using the Benjamini–Hochberg method. The association between postoperative radiographic alignment parameters and revision surgery was evaluated using univariate logistic regression. A two-sided P-value <.05 was considered statistically significant.
Results
Patient Characteristics
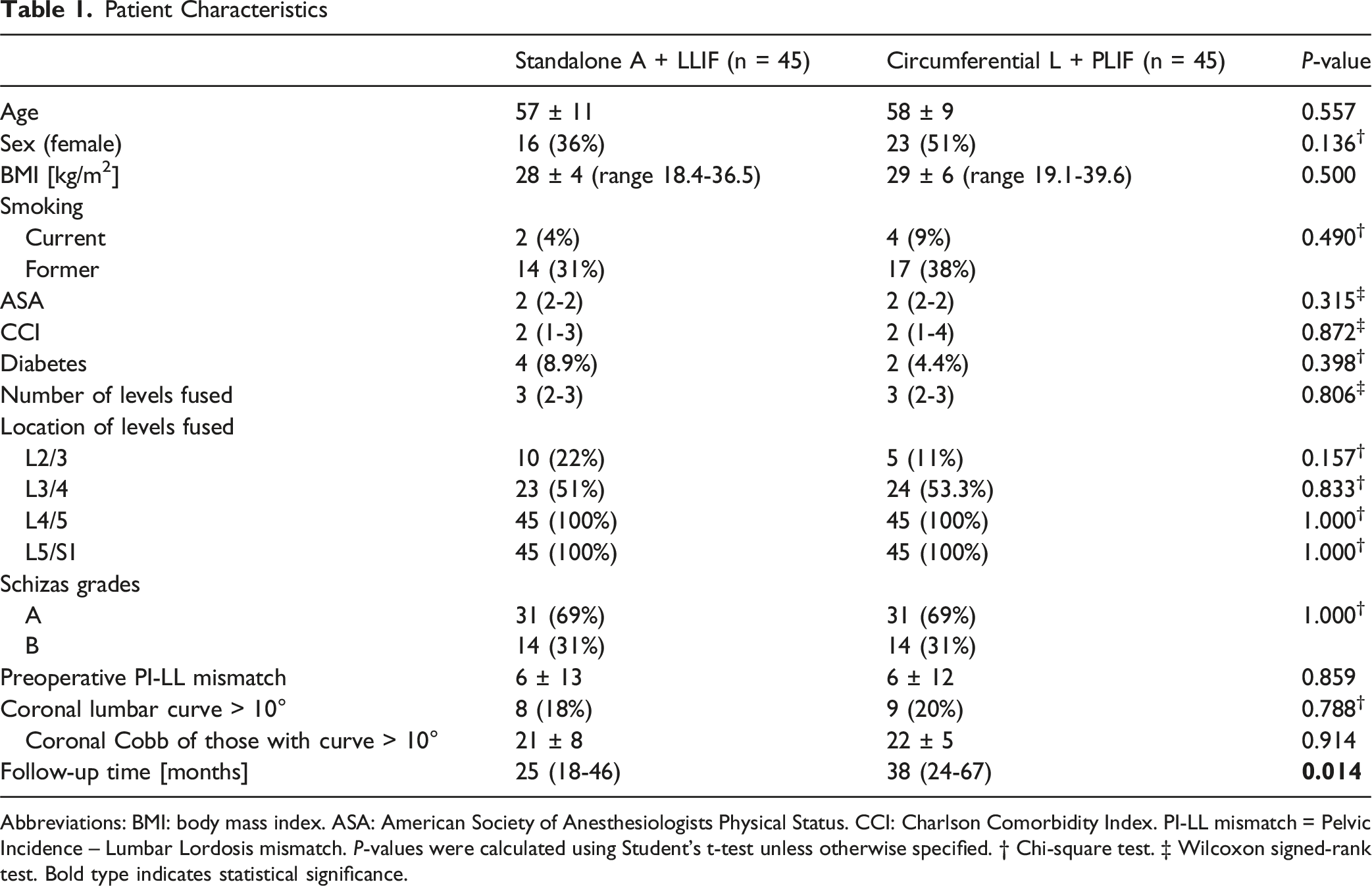
A total of 144 patients met inclusion and exclusion criteria, of whom 132 (91.7%) had complete clinical and radiographic follow-up (n = 47 A + LLIF, n = 85 L + PLIF) (Figure 3). After 1:1 propensity score matching, 90 patients were included in the final analysis (n = 45 A + LLIF, n = 45 L + PLIF). The mean age was 57 ± 10 years, the mean BMI was 28.2 ± 5.2 kg/m2, and 43.3% were female. Baseline demographic characteristics, radiographic parameters, and levels treated were well balanced between groups (Table 1). The median number of fused levels was 2 (range 2-4) in both groups. The median follow-up duration was 28 months (IQR 21-54 months), with significantly longer follow-up in the L + PLIF group compared to the A + LLIF group (38 vs 25 months, P = .014). Study flowchart Patient Characteristics Abbreviations: BMI: body mass index. ASA: American Society of Anesthesiologists Physical Status. CCI: Charlson Comorbidity Index. PI-LL mismatch = Pelvic Incidence – Lumbar Lordosis mismatch. P-values were calculated using Student’s t-test unless otherwise specified. † Chi-square test. ‡ Wilcoxon signed-rank test. Bold type indicates statistical significance.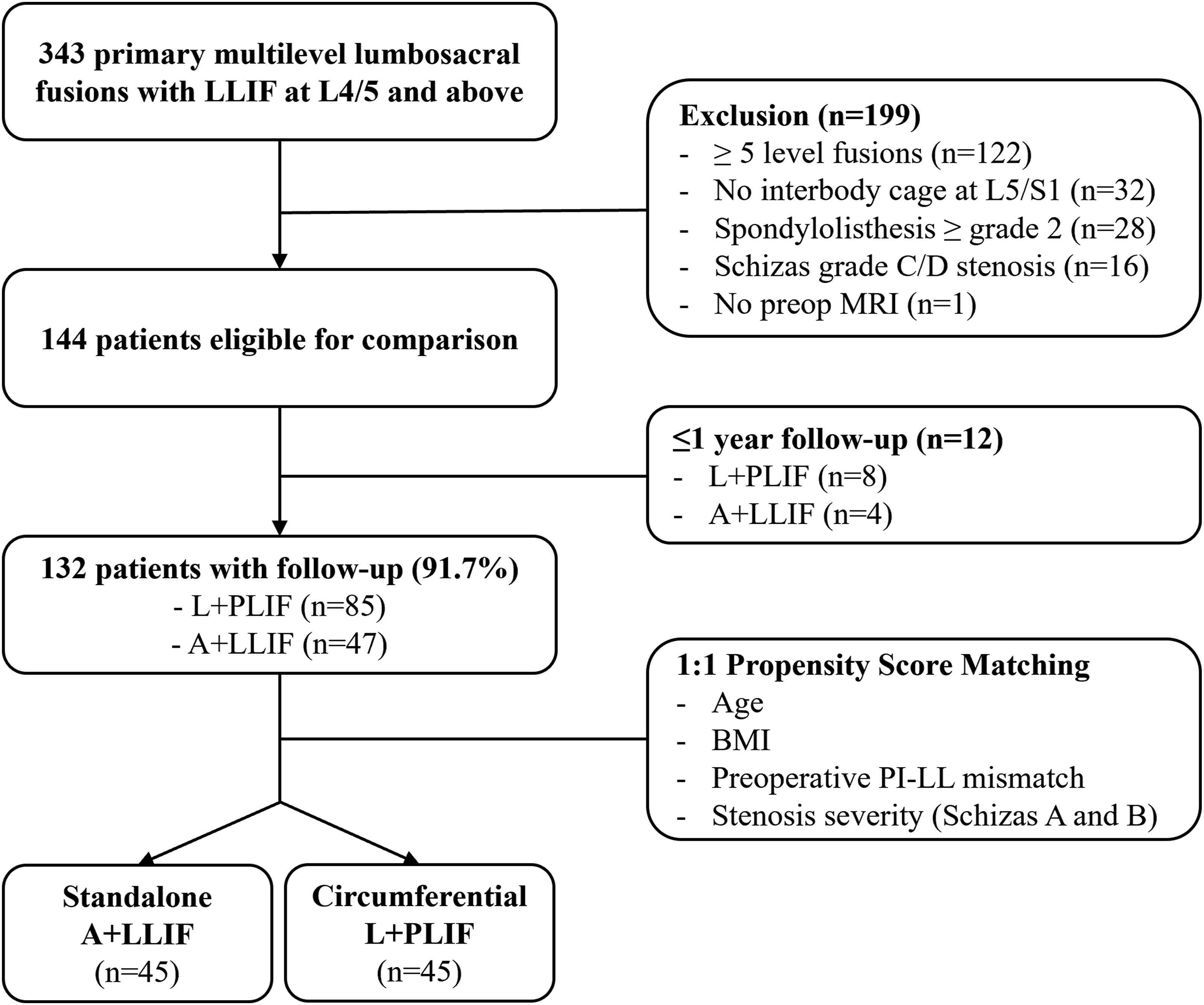
Revision Surgery
Revision Procedures
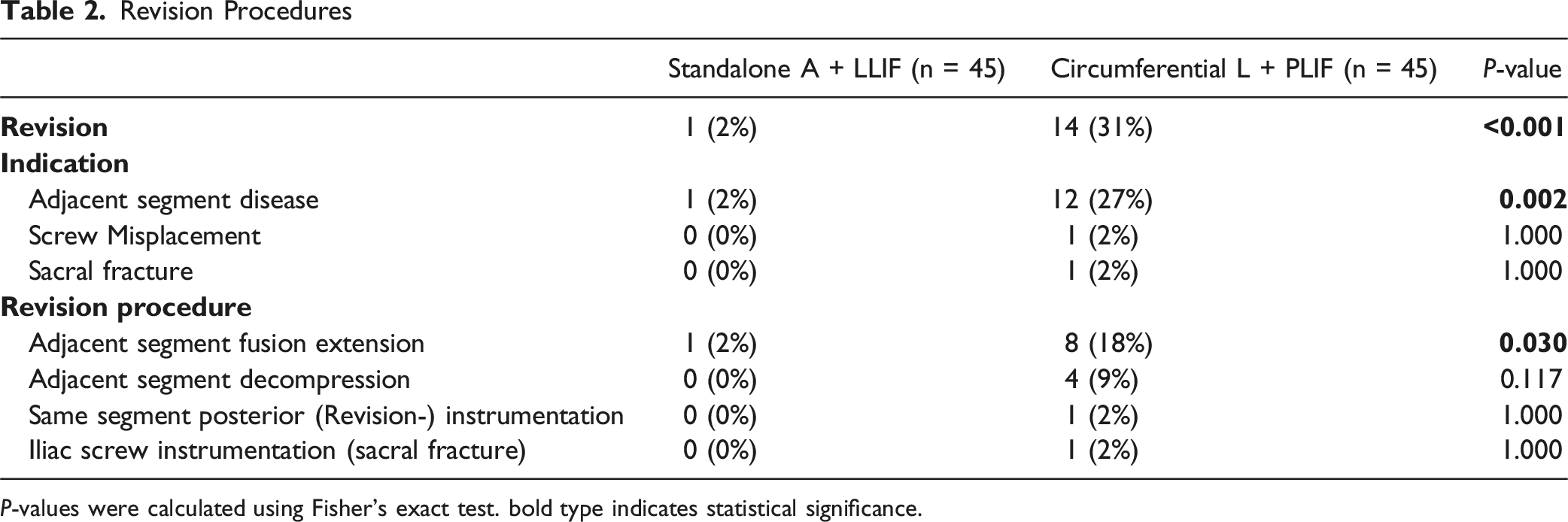
P-values were calculated using Fisher’s exact test. bold type indicates statistical significance.
Kaplan–Meier analysis confirmed a significantly lower cumulative risk of revision in the A + LLIF group (log-rank P = 0.0010; Figure 4). At five years, the predicted risk of revision was 2.7% (95% CI, 0.4%–17.7%) for A + LLIF and 33.9% (95% CI, 21.5%–50.9%) for L + PLIF. Based on person-time analysis, the average annual incidence of revision surgery was 8.7 per 100 person-years in the L + PLIF group and 0.7 per 100 person-years in the A + LLIF group. On Cox proportional hazards regression, A + LLIF was associated with a 92.6% relative reduction in the hazard of revision surgery compared to L + PLIF (HR = 0.074, 95% CI, 0.010-0.564; P = .012). Kaplan-Meier Curve Illustrating Five-Year Revision-free Survival Following Standalone (A + LLIF) and Circumferential (L + PLIF) Lumbosacral Fusion. P-value calculated using log-rank test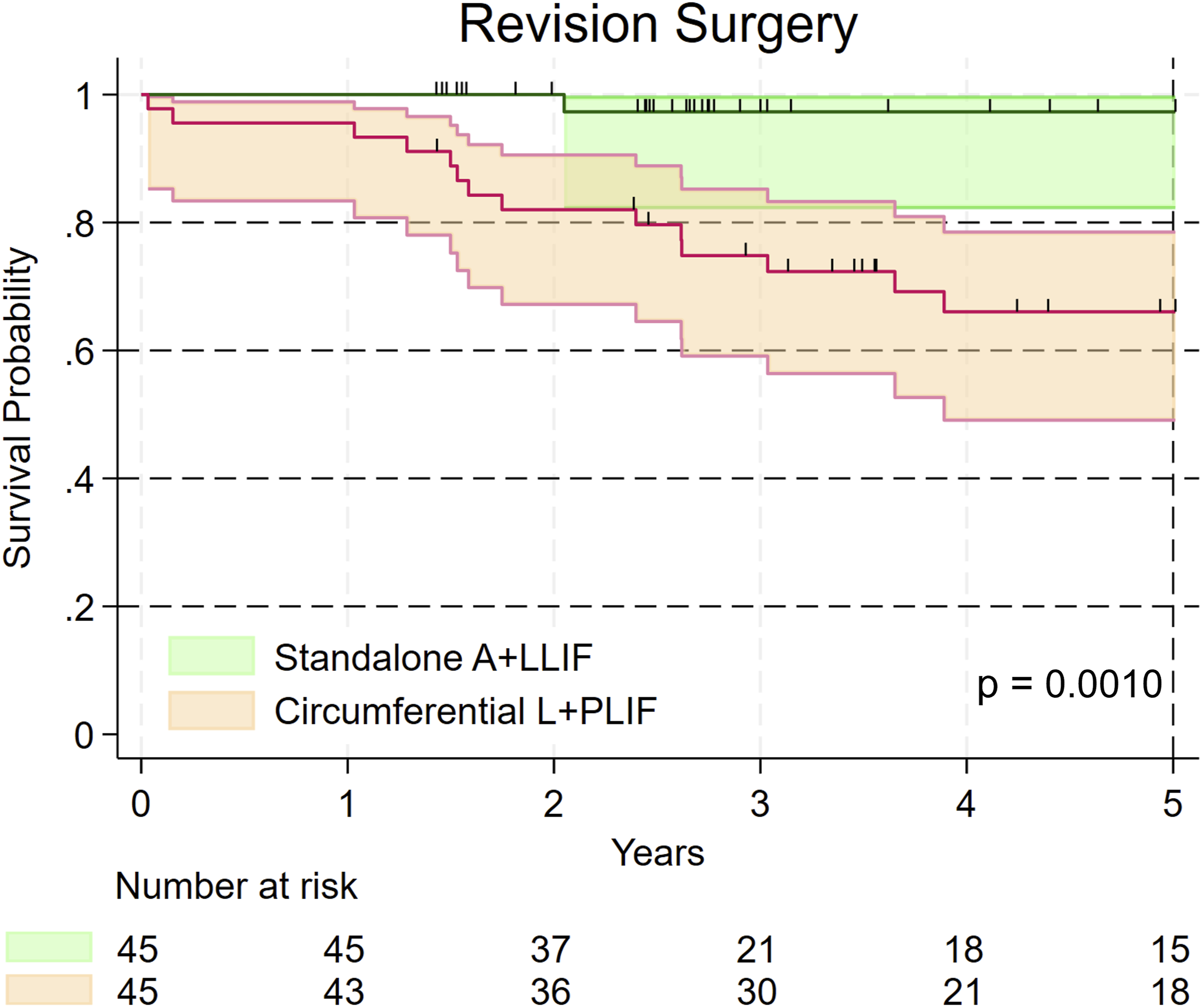
In the full unmatched cohort of 132 patients, revision surgery risk remained significantly lower in the A + LLIF group, with a 5-year revision incidence of 2.6% vs 31.7% in the L + PLIF group (log-rank P = .0010), and a similarly reduced hazard of revision surgery for A + LLIF (HR = 0.074, 95% CI, 0.010-0.546; P = .011).
Perioperative Outcomes
Compared to the matched circumferential L + PLIF cohort, A + LLIF was associated with significantly shorter operative times (median 205 minutes, IQR 183-239 vs 336 minutes, IQR 227-407), lower estimated blood loss (100 mL, IQR 50-100 vs 600 mL, IQR 300-1000), and shorter hospital stays (2 days, IQR 2-3 vs 4 days, IQR 3-6), with all comparisons P < .001. No major intraoperative complications were observed in either group.
Radiographic Outcomes
Preoperative and 1-Year Postoperative Spinopelvic Alignment
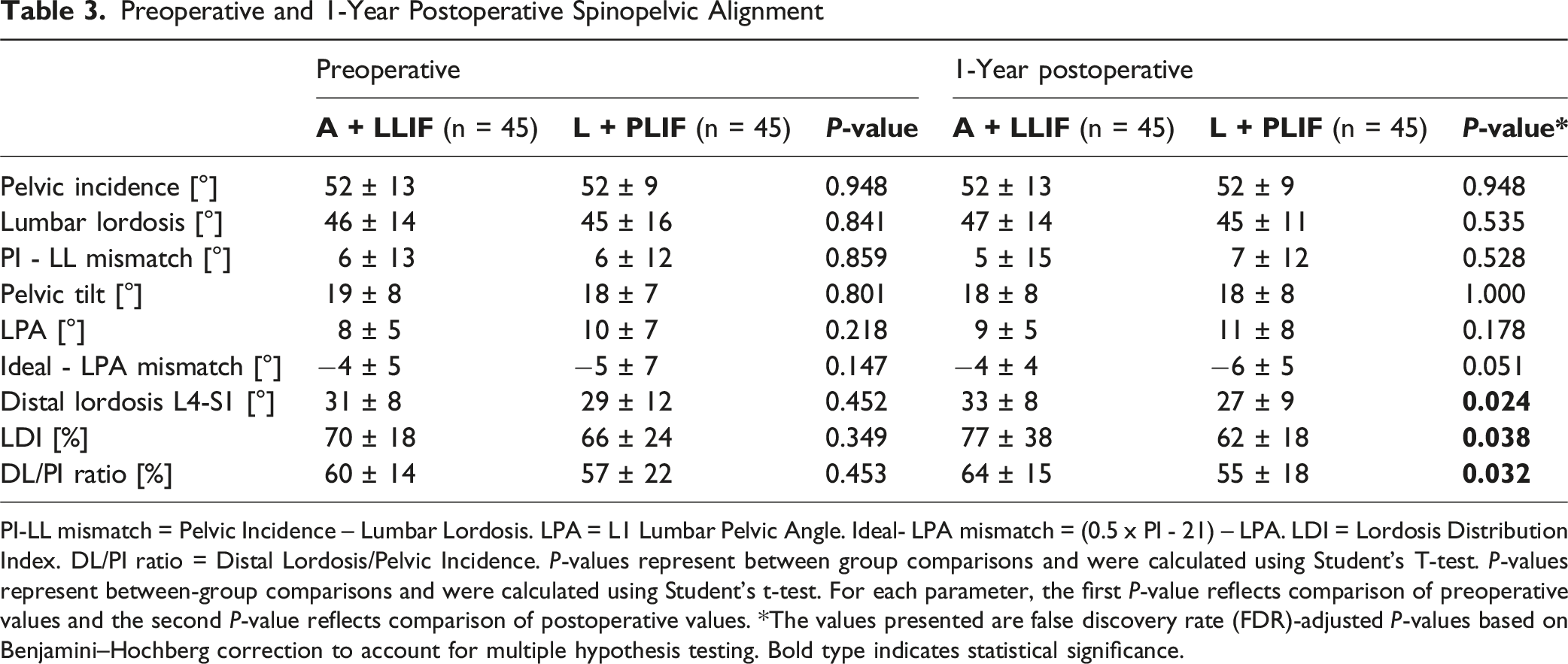
PI-LL mismatch = Pelvic Incidence – Lumbar Lordosis. LPA = L1 Lumbar Pelvic Angle. Ideal- LPA mismatch = (0.5 x PI - 21) – LPA. LDI = Lordosis Distribution Index. DL/PI ratio = Distal Lordosis/Pelvic Incidence. P-values represent between group comparisons and were calculated using Student’s T-test. P-values represent between-group comparisons and were calculated using Student’s t-test. For each parameter, the first P-value reflects comparison of preoperative values and the second P-value reflects comparison of postoperative values. *The values presented are false discovery rate (FDR)-adjusted P-values based on Benjamini–Hochberg correction to account for multiple hypothesis testing. Bold type indicates statistical significance.
A + LLIF was associated with significantly greater restoration of distal lordosis at L4–S1 (P = 0.024, FDR-adjusted), higher LDI (P = 0.038, FDR-adjusted), and a more favorable DL/PI ratio (P = .032, FDR-adjusted), indicating improved distribution of lordosis across the lumbosacral junction. On univariate logistic regression, none of the preoperative or postoperative alignment parameters were associated with revision surgery.
Cage Subsidence

Subsidence grades are reported according to the Marchi classification. P-values were calculated using Fisher’s exact test.
Discussion
This study evaluates the surgical technique of standalone A + LLIF for multilevel lumbosacral fusion surgery. The key findings of this propensity-score matched comparison to circumferential L + PLIF fusion are that (1) standalone A + LLIF was associated with lower risk of revision surgery, particularly for ASD, (2) spinopelvic alignment was comparable between both techniques, with greater restoration of distal lordosis observed with A + LLIF, (3) Cage subsidence rates were similarly low with both techniques; and (4) A + LLIF was associated with reduced operative times, blood loss, and hospital stay.
Revision Risk and Adjacent Segment Disease
One of the key findings of this study wasthat combined standalone ALIF and LLIF was associated with a low revision rate, with a predicted 5-year revision risk of only 2.7%, which was significantly lower than that of circumferential fusion using LLIF, PLIF, and posterior pedicle screw instrumentation. Although no prior study has evaluated the combination of standalone ALIF and LLIF, similarly low revision rates have been reported for standalone ALIF or LLIF individually. Nguyen et al. 23 found a revision rate of 5.7% after standalone ALIF or LLIF and a mean follow-up of over two years, with same-level revisions accounting for 3.8% and adjacent-level revisions 1.9%. In a series by Nayar et al., 24 the incidence of adjacent segment revision surgery was 3.3% at four years after standalone LLIF. A recent study comparing standalone vs circumferential LLIF found a >50% reduction in ASD risk with the standalone technique. 25
In contrast, revision rates for posterior and circumferential constructs vary widely, with some reporting a revision rate of 17.2% after an average of 15.5 days for 1-4 segment fusions, 26 and others reporting a rate of 23.2% after an average of 5.9 years. 27 In our study, the predicted 5-year revision risk with circumferential L + PLIF was 33.9%. Ghiselli et al. 28 reported a 3.9% annual risk of surgically relevant ASD, which is lower than the annual incidence of 8.7 per 100 person-years in our L + PLIF cohort. In a more recent study, Singh et al. 29 a 2-year incidence of ASD of 32.7% was reported after 1-3 level transforaminal lumbar interbody fusion, with 19.6% undergoing revision, underlining the high burden of adjacent segments after posterior instrumented fusion.
Taken together, these findings are consistent with the hypothesis that preservation of the posterior musculature and avoidance of pedicle screw instrumentation may reduce biomechanical stress at adjacent levels and protect against ASD.
Radiographic Outcomes
A + LLIF achieved a postoperative sagittal alignment comparable to L + PLIF, with greater restoration of distal lordosis. This is consistent with prior studies showing that ALIF and LLIF yield greater segmental lordosis than posterior-based technique. 30 From a biomechanical perspective, a more physiologic distribution of lordosis across L4–S1 has been proposed toreduce stress transfer to adjacent segments and has been associated in some reports with improved mechanical durability of short-segment constructs, although results across the literature remain inconsistent. In our cohort, greater distal lordosis did not correlate with revision risk, and standardized patient-reported outcomes were not available to determine whether this radiographic difference translated into symptomatic or functional benefit.
In contrasts, Rothenfluh et al, 31 who reported a tenfold increase in the risk of ASD-related revision surgery among patients with a PI–LL mismatch >10°. However, recent studies have failed to consistently link alignment metrics with ASD in short-segment fusions.21,32,33 While a postoperative physiological alignment should remain a surgical goal, our findings support selective fusion strategies in cases without overt deformity, particularly when rigidly addressing all alignment metrics would require more extensive interventions.
Cage subsidence was infrequent in both groups and mostly mild. No association was found between subsidence grade and revision risk. While subsidence has traditionally been viewed as mechanical failure, mild-to-moderate settling may represent a controlled process that does not impair outcomes.34,35 Nevertheless, careful patient selection and endplate preparation remain essential to minimize clinically relevant subsidence.
Perioperative Outcomes
Standalone A + LLIF was associated with significantly reduced operative time, blood loss, and length of stay, consistent with prior reports on standalone ALIF and LLIF.36,37 These muscle-preserving techniques may be associated with shorter recovery trajectories, which could be relevant for both younger patients and elderly or comorbid individuals who are less tolerant of prolonged surgery. In addition, accelerated recovery may reduce postoperative muscle disuse and could influence longer-term function, although this remains speculative and warrants further study.
Patient Selection
The findings of this study should be interpreted in appropriate clinical context. We do not advocate standalone A + LLIF for all patients requiring multilevel fusion and for many indications, such as severe deformity or clearly unstable scenarios, posterior pedicle screw instrumentation may be more appropriate. However, for carefully selected individuals, standalone interbody fusion may provide a durable, muscle-preserving alternative. In our experience, A + LLIF is best suited for patients without sagittal imbalance, with ≤ grade 2 spondylolisthesis, only mild central stenosis, and favorable neurovascular anatomy permitting safe anterior access to L5/S1 and lateral access to L4/5 and above. Posterior instrumented fusion remains the standard of care for patients outside these criteria.
Limitations
Several limitations should be acknowledged. This was a retrospective, single-center study with a relatively small sample size, which may limit the generalizability of the findings. Despite the use of strict exclusion criteria, propensity score matching, and well-balanced cohorts, residual confounding from unmeasured variables cannot be ruled out. Standardized bone density measures from DEXA or quantitative CT-scan were not routinely available and could not be included in the analysis. Patient selection was also intentionally restrictive (mild stenosis and ≤ grade 2 spondylolisthesis), meaning that the findings may not be generalizable to patients with more advanced deformity, instability, or severe stenosis. The duration of follow-up differed between groups, with longer follow-up in the L + PLIF cohort, which could influence revision risk estimates. Although this was addressed analytically using time-to-event methods including Kaplan–Meier and Cox proportional hazards modeling, differences in clinical surveillance intensity may persist. Patients undergoing circumferential fusion may require more frequent or prolonged follow-up due to more complex postoperative courses, which could increase the likelihood of detecting revision-requiring pathology compared with patients with uneventful recoveries after A + LLIF who were often discharged from routine follow-up after one year. Fusion status was not formally assessed, as postoperative CT imaging was not routinely obtained and fusion determination based solely on plain radiographs is limited in accuracy in multilevel constructs. In addition, the clinical relevance of radiographic outcome parameters such as fusion, cage subsidence, and alignment restoration in this context remains uncertain; therefore, revision surgery was used as a more objective and clinically meaningful outcome measure. Finally, standardized patient-reported outcomes assessing pain, function, and health-related quality of life were not available, which limits interpretation of whether lower revision rates and improved perioperative metrics translate into patient-perceived benefit. Future prospective studies incorporating validated PROMs are needed to strengthen clinical interpretation.
Conclusion
In carefully selected patients, standalone A + LLIF provides a muscle-preserving alternative to circumferential posterior multilevel fusion. This approach was associated with significantly lower revision rates, more favorable perioperative outcomes, and comparable radiographic alignment. Multicenter prospective studies are needed to validate these findings and refine patient selection criteria.
Footnotes
ORCID iDs
Ethical Considerations
The hospital’s institutional review board (IRB) approved the conduct of the study (#2022-0108).
Consent to Participate
Written and informed consent to participate in this study and to publish their data was obtained from all individual participants included in the study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Marco D. Burkhard, Torben Stepan, Anna-Maria Milke, and Ali Guven. The first draft of the manuscript was written by Marco D. Burkhard and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclose the following conflicts of interest, all of which lie outside the submitted work. FPG reports royalties from Lanx and Ortho Development; ownership interest in Centinel Spine and BICMD; consulting fees from Lanx, Ortho Development, and SeaSpine; and stock ownership in Centinel Spine and Healthpoint Capital Partners LP. FPC reports research support from Camber Spine, Centinel Spine, Choice Spine, DePuy Synthes, and Royal Biologic; ownership interest in 4WEB Medical/4WEB, Healthpoint Capital Partners LP, ISPH II, ISPB III Holdings, VBVP VI LLC, VBVP X LLC, Medical Device Partners II and III, Orthobond Corporation, Spine Biopharma, Tissue Differentiation Intelligence, and Tissue Connect Systems. AAS reports royalties from Ortho Development, DePuy Spine Products/Medical Device Business Services, and Clariance; private investments in Vestia Ventures, MiRUS Investment, ISPH II, ISPH 3, and Centinel Spine (Vbros Venture Partners V); consulting fees from DePuy Spine Products/Medical Device Business Services, Clariance, and Kuros Biosciences AG; and research support from Spinal Kinetics/Orthofix. APH reports research support from Kuros Biosciences AG and Expanding Innovations; private investments in Tissue Connect Systems; and fellowship support from NuVasive and ATec. For the remaining authors, no conflicts of interest were declared.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.