
Abstract
Study Design:
Retrospective case-control study.
Objectives:
To investigate whether mechanical bowel preparation (MBP) improve surgical performance and decrease operative complications in anterior lumbar interbody fusion (ALIF).
Methods:
This study involved a retrospective analysis of 48 consecutive patients who underwent ALIF with MBP and a control cohort of 50 consecutive patients who underwent the same surgeries without MBP. The quality of each surgical procedure, operative time, estimated blood loss (EBL), intraoperative complications, changes in vital signs and patient symptoms on the day of surgery, and bowel function postoperatively were also compared between the procedures.
Results:
Baseline demographic characteristics were similar between the 2 groups (all Ps > .05). The quality of each procedure, operative time, EBL, intraoperative complications, and changes in body temperature and heart rate were not different between the groups (all Ps > .05). The MBP group showed more headache, tiredness, thirst, and abdominal discomfort (all Ps < .001) and decrease of the systolic blood pressure (P = .041) on the day of surgery. The return of bowel movement was not different between the groups (P = .278).
Conclusions:
Given the similar surgical result with the substantial patient discomfort, MBP can be omitted in ALIF.
Keywords
Introduction
Mechanical bowel preparation (MBP) before abdominal surgery has been believed to improve surgical visualization and bowel handling, and to decrease peritoneal contamination in case of bowel injury. 1 MBP was considered standard care in colorectal surgery and extrapolated to gynecologic surgery, urologic surgery, as well as anterior lumbar surgery. 2 -4 MBP includes the use of oral laxative solutions, retrograde enema, and oral dietary restriction preoperatively, which causes substantial patient discomfort. In addition, it might induce electrolyte disturbances, dehydration, insomnia, general weakness on the day of surgery, and gastrointestinal discomfort postoperatively. 5,6 Although systemic reviews could not demonstrate any significant benefit of MBP regarding intraoperative and perioperative complications, 7 -10 MBP is still performed in many institutes before various transabdominal surgeries. 11 -13
The anterior approach to the lumbar spine can allow direct and wide exposure of the anterior column, which has many advantages in spinal reconstruction surgery. 4,14 Moreover, the anterior approach can avoid neural injury and back muscle damage during posterior surgery. With progress in surgical techniques and instruments, anterior lumbar interbody fusion (ALIF) and oblique lateral interbody fusion (OLIF) have gained popularity among spine surgeons. 15 -17
MBP before anterior lumbar or lumbosacral surgery has been performed to increase the quality of surgical exposure and each procedure in either retroperitoneal or transperitoneal approach. 4 However, few studies have evaluated the effectiveness of MBP in anterior lumbar surgery. In the current study, we aimed to compare the surgical performance and perioperative complications regarding MBP in ALIF.
Methods
Patients
This study involved a retrospective analysis of 48 consecutive patients who underwent minimally invasive retroperitoneal ALIF between L2-3 and L5-S1 level with MBP and a control cohort of 50 consecutive patients who underwent the same surgeries without MBP. The former was recruited between July 2012 and December 2014, and the latter was recruited between January 2015 and December 2016 through the department of orthopedic surgery in a tertiary hospital. All patients had a diagnosis of lumbar degenerative disease and undergone a minimum of 6 months of futile conservative management. Under general anesthesia, each patient was placed in the 45° to 90° lateral decubitus position (L2-3 to L4-5 level) or supine position (L5-S1 level) on a Jackson spinal surgery table (Mizuho OSI, Union City, CA, USA). An anterior retroperitoneal approach was made between the psoas muscle and major vessels (L2-3 to L4-5 level) or between the major vessel bifurcations (L5-S1 level). The disc and endplates were then prepared for interbody fusion. An anterior lordotic polyetheretherketone (PEEK) cage (Perimeter; Medtronic Inc, Minneapolis, MN, USA) filled with autologous iliac crest bone graft and bone graft expander was then placed into the disc space. Supplemental posterior pedicle screw instrumentation was then performed with either an open or percutaneous technique. Posterior decompression was undertaken as necessary. Informed consent was obtained for this study. The hospital’s ethics committee reviewed and approved the present study.
Patients with MBP took oral laxative solutions (Colyte powder; Taejoon Pharma Co, Ltd, with 4 L of water) with dietary restriction on the day before surgery. Patients without MBP had a normal preoperative diet with fasting from the midnight before surgery. All patients included in the study had a clinical follow-up period of more than 1 year. Each patient’s medical records were reviewed with regard to demographic characteristics, body mass index (BMI), current smoking status, severity of pain (visual analog scale score), Oswestry disability index (ODI), diagnosis, level of surgery, operative time, estimated blood loss (EBL), any perioperative adverse event, vital signs, and perioperative general symptoms and signs.
Comparison of Surgeons’ Performance With or Without MBP
Surgeries were performed by either of the 2 spine surgeons (CJ or NC). Immediately postoperatively, the operating surgeon completed a self-administered questionnaire assessing the easiness of each surgical procedure on a 4-point Likert-type scale (1 = excellent, 2 = good, 3 = fair, 4 = poor). The questionnaires involved peritoneal mobilization during the retroperitoneal approach, surgical field exposure for ALIF, and performance of interbody fusion procedure. The operative time, EBL, and occurrence of any intraoperative complication were also compared between patients with MBP and without MBP.
Evaluation of Patients’ Perioperative Condition With or Without MBP
Perioperative patient parameters included the changes in vital signs, patient symptoms on the day of surgery, and postoperative bowel function. The differences in the vital signs measured at baseline (at admission) and on the day of surgery were calculated. Patient symptoms on the day of surgery, for example, headache, nausea or vomiting, tiredness, anxiety, thirst, and abdominal discomfort, were assessed using a visual analog scale. Postoperative bowel function included the return of bowel movement and occurrence of ileus. The return of bowel movement was identified by auscultating the patient’s bowel sound. Postoperative ileus was diagnosed as no sign of flatus and/or passage of stool until postoperative day 3 with radiological evidence. 18
Statistical Analysis
Data was recorded and analyzed using SPSS for Windows software (version 19.0; IBM Corp, Armonk, NY, USA). Descriptive statistics are presented as frequencies (percentages) for categorical variables and as means ± standard deviation for continuous variables. Demographic characteristics, surgical parameters, and the changes in patients’ parameters between the two groups were compared using the Student’s t test, chi-square test, and Mann-Whitney U test. In all analyses, a P value <.05 was considered to indicate statistical significance.
Results
Subject Characteristics
The demographic characteristics of the 2 groups are shown in Table 1. Mean ages were 66.4 ± 10.1 years (range, 43-83 years) for the patients with MBP and 62.9 ± 9.6 years (range, 36-86 years) for the patients without MBP (P = .081). There were 14 (29.2%) men in the group with MBP and 17 (34.0%) men in the group without MBP (P = .607). There were no differences in BMI, smoking status, severity of pain, ODI, vital signs at admission, diagnosis, or level of surgery between the 2 groups (all Ps > .05).
Demographic Characteristics.a
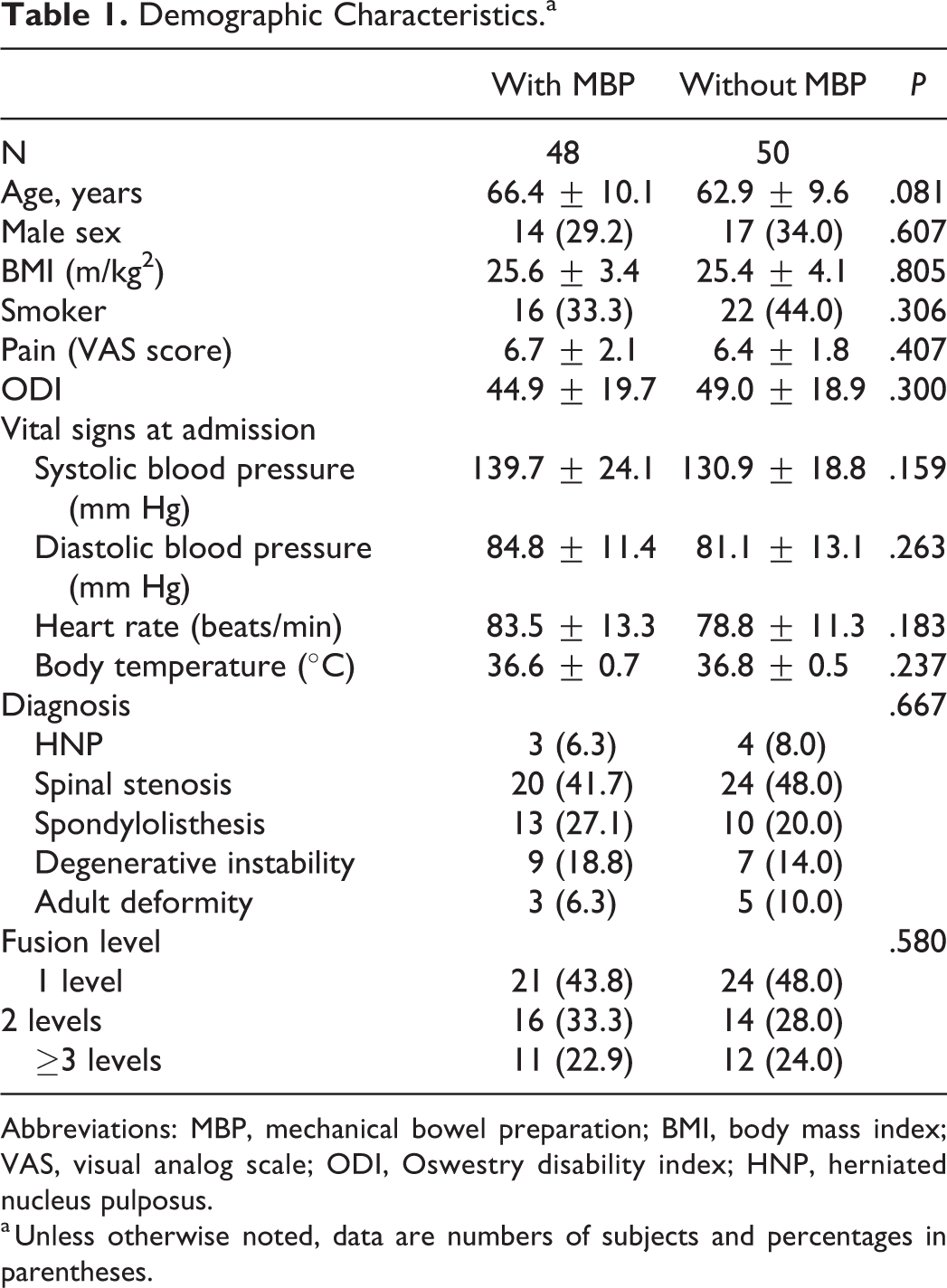
Abbreviations: MBP, mechanical bowel preparation; BMI, body mass index; VAS, visual analog scale; ODI, Oswestry disability index; HNP, herniated nucleus pulposus.
a Unless otherwise noted, data are numbers of subjects and percentages in parentheses.
Surgeon’s Performance With or Without MBP
The quality of peritoneal mobilization was noted to be excellent/good in 43 (89.6%) patients with MBP and in 47 (94.0%) patients without MBP (P = .630; Table 2). The quality of surgical field exposure was excellent/good in 43 (89.6%) patients with MBP and in 43 (86.0%) patients without MBP (P = .584). Performance of the interbody fusion procedure was excellent/good in 41 (85.4%) patients with MBP and in 42 (84.0%) patients without MBP (P = .879). The operative time, EBL, and occurrence of intraoperative complications were not different between the 2 groups (all Ps > .05).
Parameters on Surgeons’ Performance.a
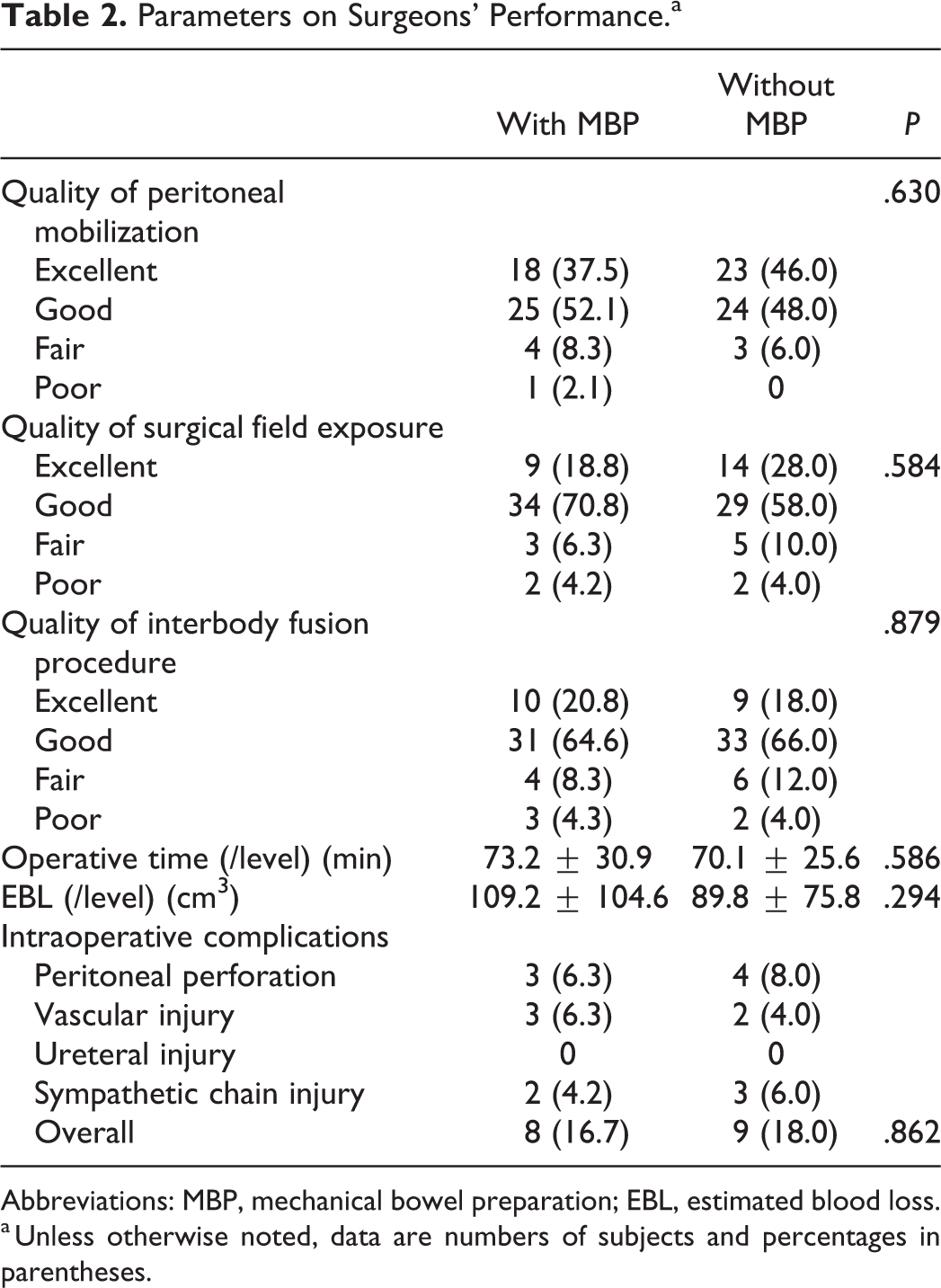
Abbreviations: MBP, mechanical bowel preparation; EBL, estimated blood loss.
a Unless otherwise noted, data are numbers of subjects and percentages in parentheses.
Patient’s Perioperative Condition With or Without MBP
The systolic blood pressure decreased in patients with MBP as 4.2 ± 12.4 mm Hg but increased in patients without MBP as 9.72 ± 16.2 mm Hg, which was significantly significant (P = .041; Table 3). Other vital signs did not change significantly (all Ps > .05). The MBP group showed more headache, tiredness, thirst, and abdominal discomfort on the day of surgery (all Ps < .001) compared with the group without MBP. The return of bowel movement postoperatively and the occurrence of postoperative ileus were not different between patients with MBP and without MBP (P = .278 and P = .478, respectively).
Parameters on Patients’ Perioperative Condition.a
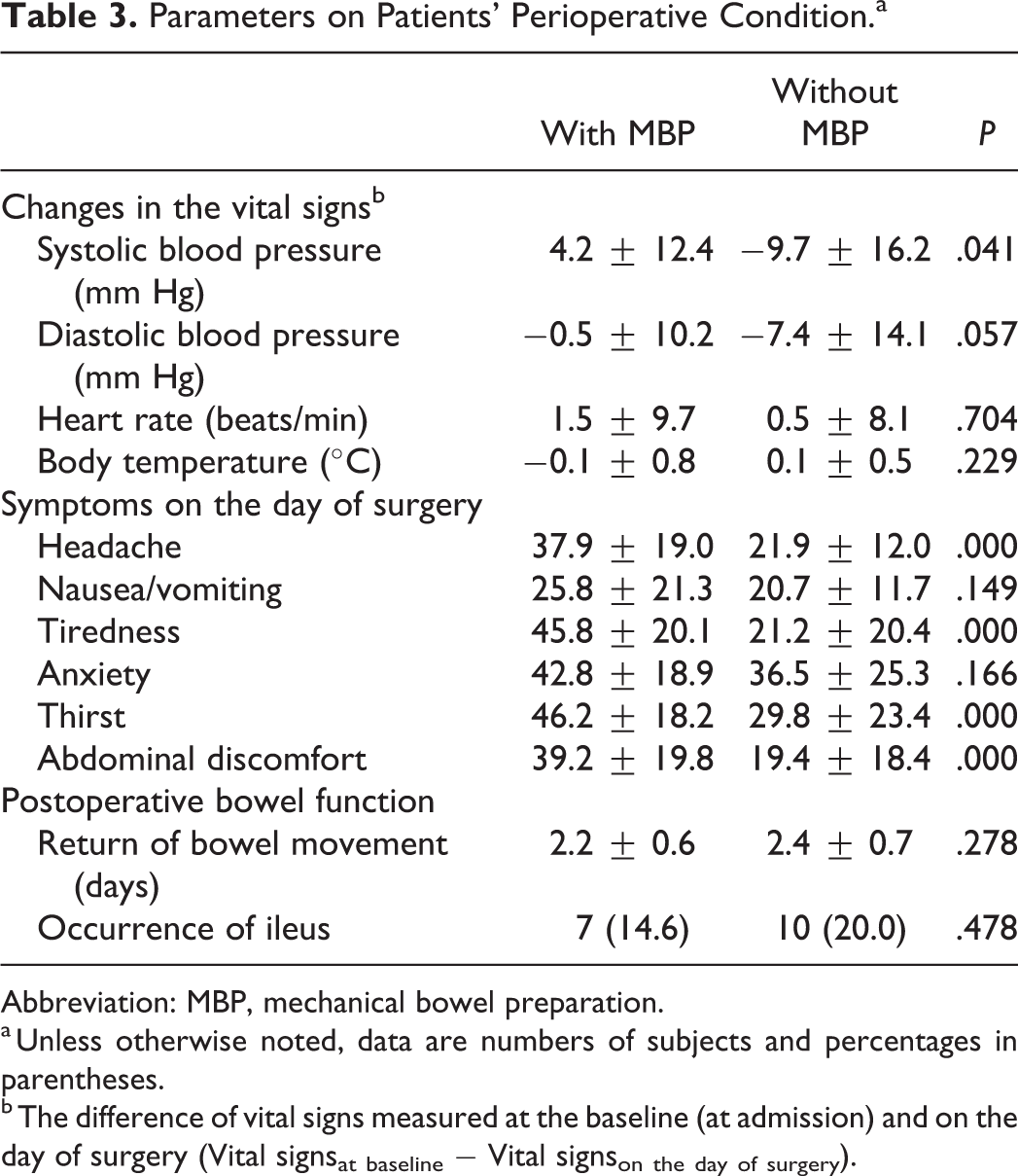
Abbreviation: MBP, mechanical bowel preparation.
a Unless otherwise noted, data are numbers of subjects and percentages in parentheses.
b The difference of vital signs measured at the baseline (at admission) and on the day of surgery (Vital signsat baseline − Vital signson the day of surgery).
Discussion
The anterior approach to the lumbar spine can provide direct and extensive exposure to the anterior disc, which allows for easier and better removal of the disc material and cartilaginous endplate without violating the epidural space. 4 Consequently, it is beneficial in the achievement of solid fusion, distraction of the neural foramen, and reconstruction of lumbar lordosis. 17 With advancement of the minimally invasive surgical technique and instrument, ALIF has become favorable options for the surgical treatment of lumbar degenerative disease. Recently, considerable attention has been paid to ALIF in the surgery of adult spinal deformity as alternative techniques to invasive posterior lumbar osteotomy. 14
Mobilization of the peritoneal content to expose the anterior disc space is the key access procedure during ALIF. 4,16 MBP is the mechanical decompression of the intestines, which may improve peritoneal mobilization and surgical field exposure. Thus, MBP has been considered standard care for both the transperitoneal and retroperitoneal approach in colorectal surgery, gynecologic surgery, urologic surgery, as well as anterior lumbar surgery. 2 -4 However, numerous studies have failed to demonstrate the effectiveness of MBP in transabdominal surgeries. Guenaga et al 7 evaluated the usefulness of MBP in elective colorectal surgery using Cochrane database. They concluded that MBP can be safely omitted in colorectal surgery because the surgical outcome was not improved by MBP. Current clinical guidelines in colorectal surgery recommend that MBP should not be routinely used before open colorectal surgery. 2 In gynecologic surgery, randomized clinical trial studies repeatedly found no benefit of MBP in the surgical performance and perioperative complications. 19 -21 Additionally, MBP did not also show any advantageous effect on the overall complications, operative time, and total costs in urologic surgery. 6,22
Moreover, MBP can reduce total body water, which causes patient discomfort, including thirst, general weakness, anxiety, and abdominal discomfort, preoperatively. 5,6 Dehydration due to MBP may affect circulatory function in elderly patients, especially those with cardiac, renal, or hepatic disease. 23
However, MBP is still routinely used in many institutes for various transabdominal surgeries. 11 -13 To the best of our knowledge, the role of MBP in anterior lumbar surgery has never been reported. We aimed to evaluate whether MBP improves the surgical performance and reduces perioperative complications in ALIF. The quality of surgical performance, operative time, EBL, occurrence of intraoperative complications, and postoperative bowel function were not different between patients with MBP and without MBP. Patients with MBP showed significant reduction of systolic blood pressure and more generalized symptoms on the day of surgery. Therefore, our study provides an evidence that routine use of MBP is not recommend in ALIF.
The first main limitation of this study was the subjective nature regarding several outcome measurements. The parameters of surgeons’ performance and patients’ discomfort were graded using a self-administered questionnaire, which has intrinsic measurement bias. Moreover, the unblinded nature of MBP in this study could have caused selection or detection bias. Second, the negative effectiveness of MBP could be resulted from a type II error due to the small sample size. Third, the retrospective design introduced a degree of uncertainty due to missing and erroneous data in the medical records, as well as a lack of clinical information. Fourth, the changes in hematologic markers, such as sodium, potassium, blood urea nitrogen, or creatinine, after MBP were not examined in this study. That data may have improved the strength of this study. Finally, radiological parameters were not analyzed, which may also reflect the quality of the surgical outcome. Further investigations, including randomized, controlled trials, are warranted to confirm whether MBP could ameliorate the radiological and clinical outcomes in ALIF.
Conclusions
In this study, MBP did not improve the quality of surgical performance, occurrence of intraoperative complications, and postoperative bowel function in ALIF. Given its side effect and patient discomfort, routine MBP is not recommended in ALIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.