
Abstract
Study Design
Retrospective comparative study.
Objectives
To investigate the clinical and radiological outcomes after anterior column realignment (ACR) through pre-posterior release-anterior-posterior surgery (PAP) and minimally invasive surgery -lateral lumbar interbody fusion (MIS-LLIF) using hybrid anterior-posterior surgery (AP).
Methods
A total of 91 patients who underwent ACR with long fusions from T10 vertebra to the sacropelvis with a follow-up period of at least 2 years after corrective surgery for adult spinal deformity were included and divided into two groups by surgical method: AP and PAP. AP was performed in 26 and PAP in 65 patients. Clinical outcomes and radiological parameters were investigated and compared. A further comparison was conducted after propensity score matching between the groups.
Results
The more increase of LL and decrease of PI-LL mismatch were observed in the PAP group than in the AP group postoperatively. After propensity score matching, total operation time and intraoperative bleeding were greater, and intensive care unit care and rod fracture were more frequent in the PAP group than in the AP group with statistical significance. Reoperation rate was higher in PAP (29.2%) than in AP (16.7%) without statistical significance.
Conclusions
PAP provides a more powerful correction for severe sagittal malalignment than AP procedures. AP results in less intraoperative bleeding, operation time, and postoperative complications. Therefore, this study does not suggest that one treatment is superior to the other.
Level of Evidence
III.
Keywords
Introduction
Surgical correction of adult spinal deformity (ASD) with severe dynamic sagittal imbalance (DSI) is challenging for spine surgeons. 1 The primary goal of all surgical strategies is to restore sagittal and coronal balance. In particular, sagittal balance has been demonstrated to be closely associated with health-related quality-of-life outcomes in the treatment of ASD. 2 Recently, advanced sagittal correction of ASD has been introduced, such as pre-posterior release-anterior-posterior instrumentation (PAP) as a combined approach (anterior column realignment, ACR)3-5 and hybrid technique (ACR and posterior, AP) using minimal approach (lateral lumbar interbody fusion, LLIF) and open posterior instrumentation.6,7 ACR through PAP has conventionally invasive approaches, which have limited utility for severe spectrum of sagittal plane deformity. 8 Additionally, PAP is an extensive surgery and is associated with a large amount of intraoperative blood loss and significant complications rates.2,8 Thus, ACR through hybrid minimal invasive surgery (MIS) has been introduced to mitigate surgical morbidity and related complications. However, not all patients may be candidates for hybrid surgery because MIS-LLIF with incomplete anterior release for ACR and without pre-posterior release may lead to relative under-correction of severe forms of sagittal imbalance of the spine. Nonetheless, both AP and PAP approaches might show a higher correction rate than posterior instrumentation alone for severe DSI.3,6,9,10
To the best of our knowledge, there is a paucity of literature on the direct comparison between the two surgical procedures with the same fusion level, similar age and diagnosis. Therefore, this study aimed to evaluate and compare the clinical and radiological outcomes and complications of two different surgical procedures for the correction of ASD with DSI.
Methods
Data Collection
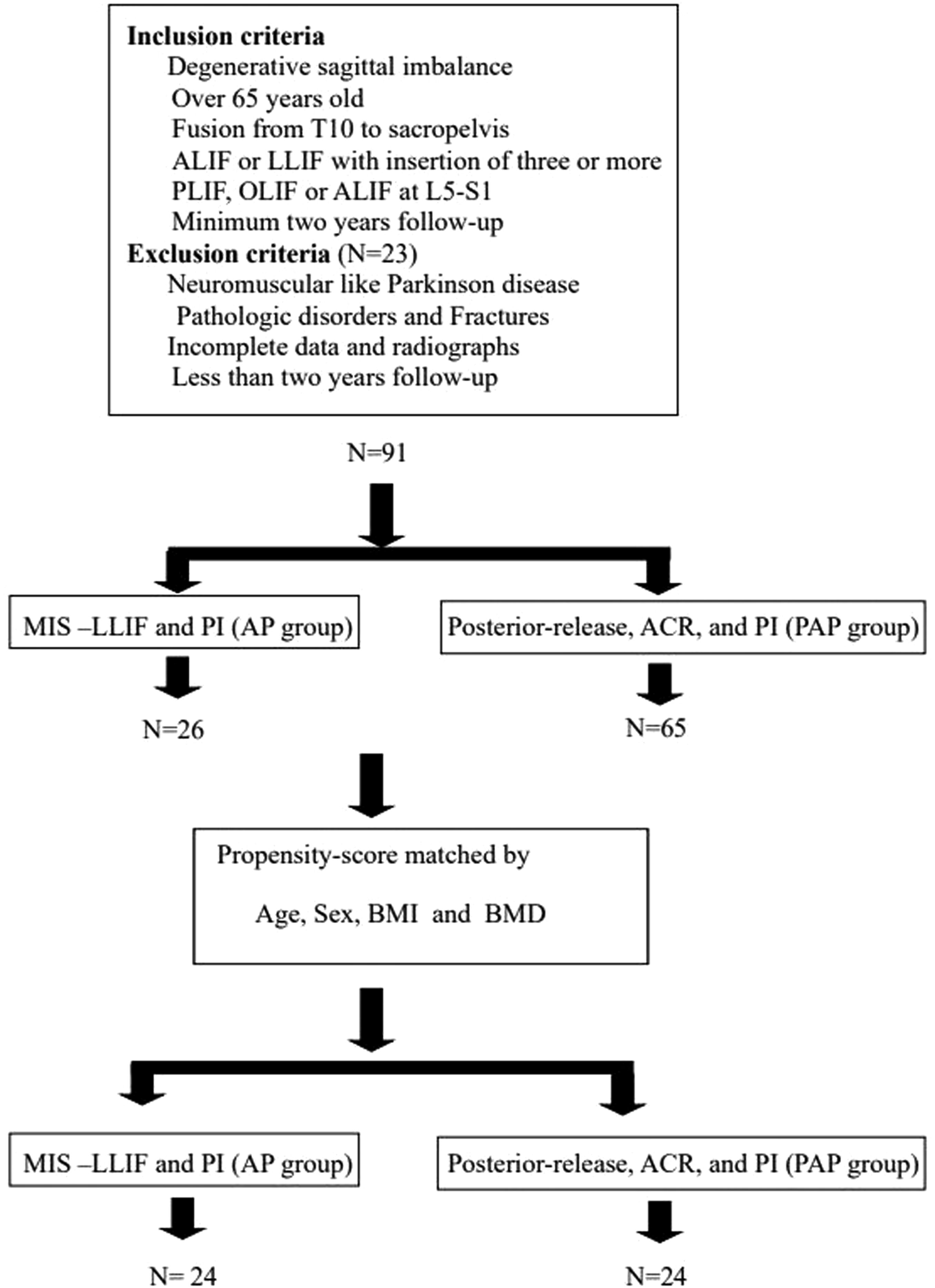
This study was performed after obtaining approval from the Institutional Review Board (IRB) of Kyung Hee University Hospital at Gangdong (approval number: KHNMC- 2020-12-021). Written informed consent was obtained from all the participants. Among the various ASD diseases, patients diagnosed with DSI between May 2012 and July 2019 were included in this retrospective study. The inclusion criteria were as follows: (1) age >65 years at the index surgery; (2) DSI without major coronal imbalance; (3) ACR with proximal fusion level to T10 and distal to the sacropelvis using bilateral iliac screws; (4) posterior two-rod instrumentation; and (5) patients who underwent anterior lumbar interbody fusion (ALIF) or minimally invasive lateral lumbar interbody fusion (LLIF) with insertion of three or more cages from L1-L5, and/or posterior lumbar interbody fusion (PLIF) or ALIF for L5-S1. In the AP group, L5-S1 fusion was performed using oblique lateral interbody fusion if cage insertion was accessible. However, 23 patients (4 patients in the AP group and 19 patients in the PAP group) who were ineligible for assessment due to follow-up loss before postoperative 2 years were excluded. All patients underwent two-staged surgery. The AP group underwent ACR through hybrid MIS-LLIF without pre-posterior release followed by open posterior instrumentation, whereas the PAP group underwent open pre-posterior release first, and then ACR and open posterior instrumentation were performed simultaneously in the second stage surgery. However, grade 2 Schwab posterior osteotomies
11
during posterior release in the PAP group and posterior instrumentation in the AP group were performed at the segments based on the degree of fixed regional and global malalignments. (Figure 1) Finally, 91 patients who met the inclusion criteria were enrolled. Subsequently, all included patients were divided into two groups according to the surgical procedures. Additionally, a further comparison was conducted after propensity score (PS) matching between the groups. (Figure 2) Diagram of the surgical procedures of the AP and PAP approaches. Flow diagram showing the selection of patients ACR: Anterior column realignment, PAP: Pre-posterior release, anterior and posterior instrumentation, MIS-LLIF: Minimally invasive surgery-lateral lumbar interbody fusion, AP: Anterior surgery and posterior instrumentation, ALIF: Anterior lumbar interbody fusion, LLIF Lateral lumbar interbody fusion, OLIF: Oblique lumbar interbody fusion, UIV: Uppermost instrumented vertebra, PI: Posterior instrumentation.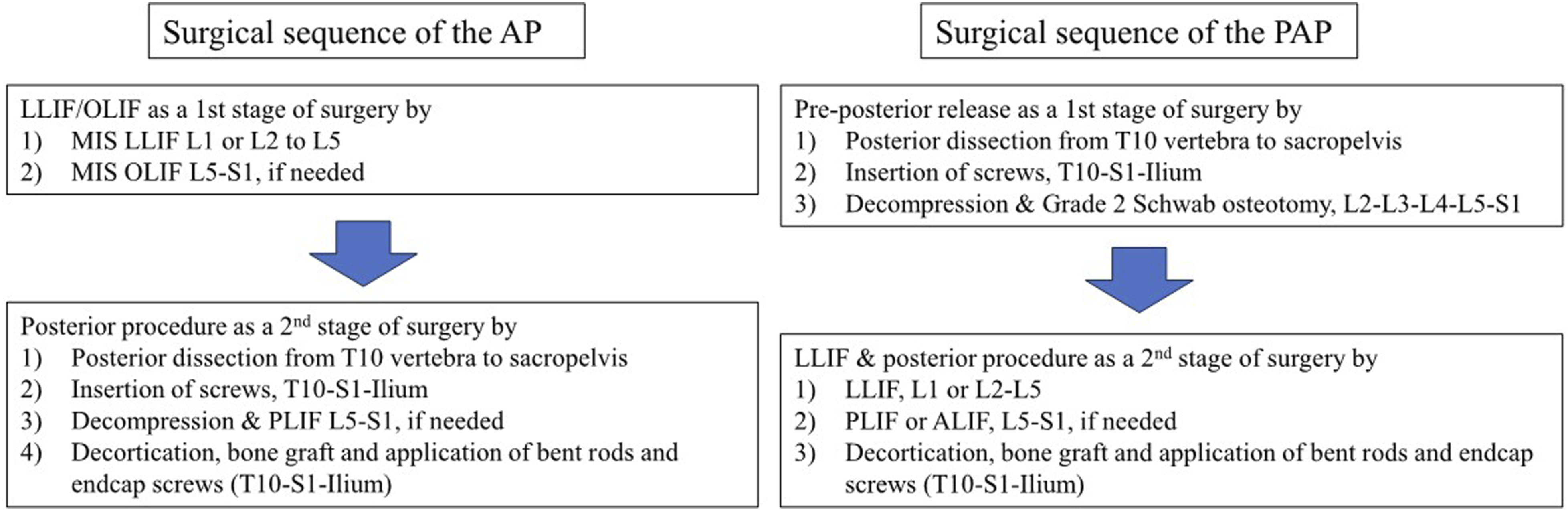
Radiographic Assessment
Radiographic measurements were performed by two independent spine fellows who did not participate in either surgery at the preoperative, the immediate postoperative, and the regular postoperative outpatient visits (3, 6, 9 months, 1-, 2-year and the final follow-up), respectively. Radiographic measurements included the standard sagittal spinopelvic parameters. Pelvic tilt (PT), sacral slope (SS), and pelvic incidence (PI) were measured. Spinopelvic parameters such as lumbar lordosis (LL), thoracic kyphosis (TK), C7 sagittal vertical axis (C7SVA), T1 pelvic angle (T1PA), proximal junctional angle (PJA), and sagittal Cobb angle between the caudal endplate of the uppermost instrumented vertebra (UIV), cephalad endplate of UIV+2, and postoperative lordosis distribution index (LDI, [L4 S1 lordosis/L1 S1 lordosis] x100) were measured at each time point.
Proximal junctional kyphosis (PJK) was defined as a PJA >20° and ≥20° greater than the preoperative measurement without any bone or instrumentation failures, based on previous studies.12,13 Proximal junctional failure (PJF) was considered as patients presenting with symptoms and radiographs showing the followings: fractures at UIV or UIV+1, junctional subluxation, and failure of UIV fixation. Failure of metallic fixation was defined as the pullout or dislodgment of screws from rods and fractures of the screws or rods. Reoperations due to mechanical complications, such as PJK/PJFs or rod fractures (RF), were also recorded.
Clinical Assessment
Clinical data collected from the medical records included age at the time of index surgery, sex, body mass index (BMI), medical comorbidities, smoking history, lowest T-score of bone mineral density (BMD), Charlson comorbidity index (CCI) 14 and previous history of spinal surgery. Surgery-related data included the surgical techniques.
Statistical Analysis
IBM SPSS Version 21.0 software (IBM Corporation, Armonk, NY, USA) was used for all the statistical analyses. Numerical data are presented as mean ± standard deviation (SD). Continuous data were analyzed using student’s t-test, and categorical data were analyzed using Fisher’s exact test. Statistical significance was set at P < .05.
Results
Patients Demographic Data
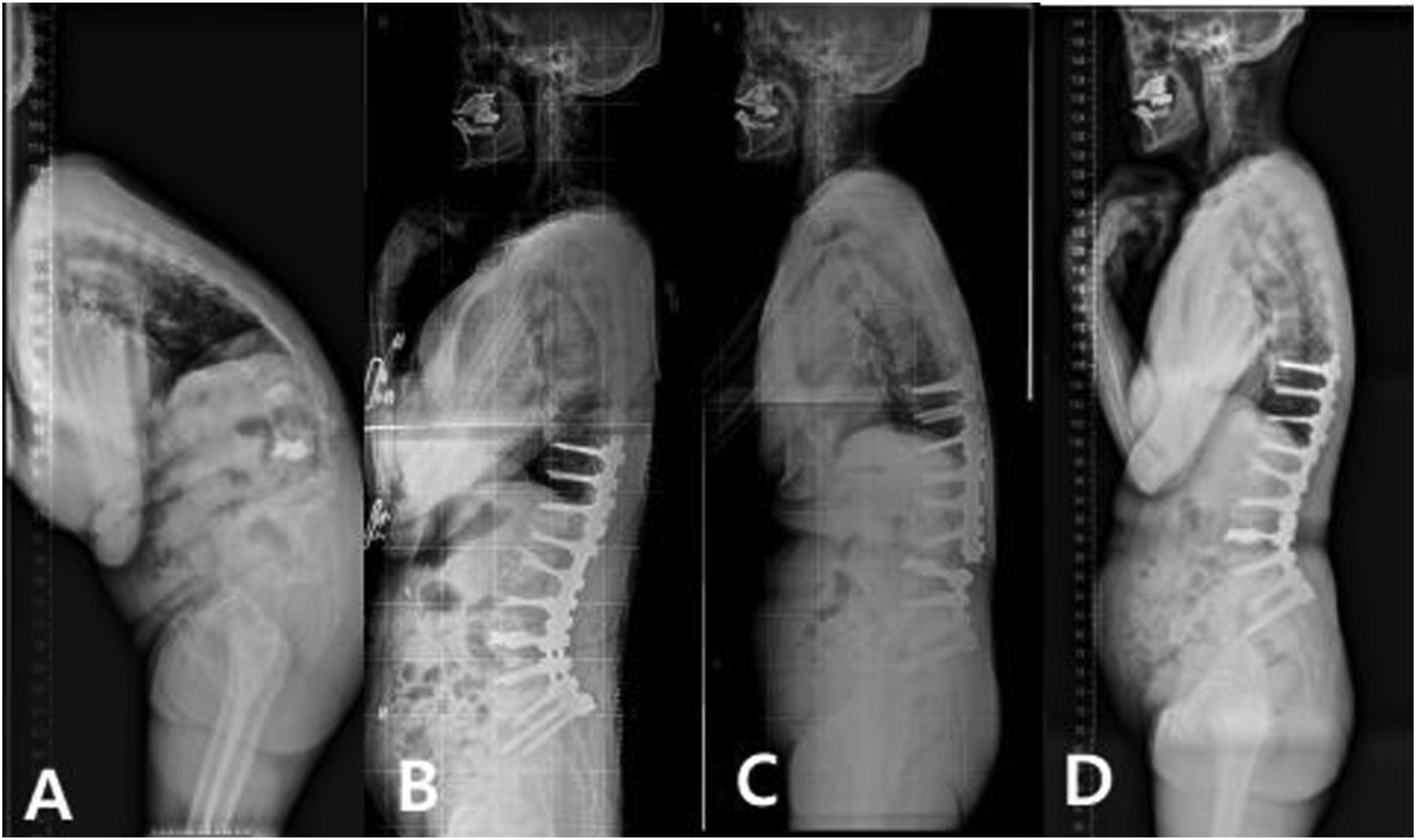
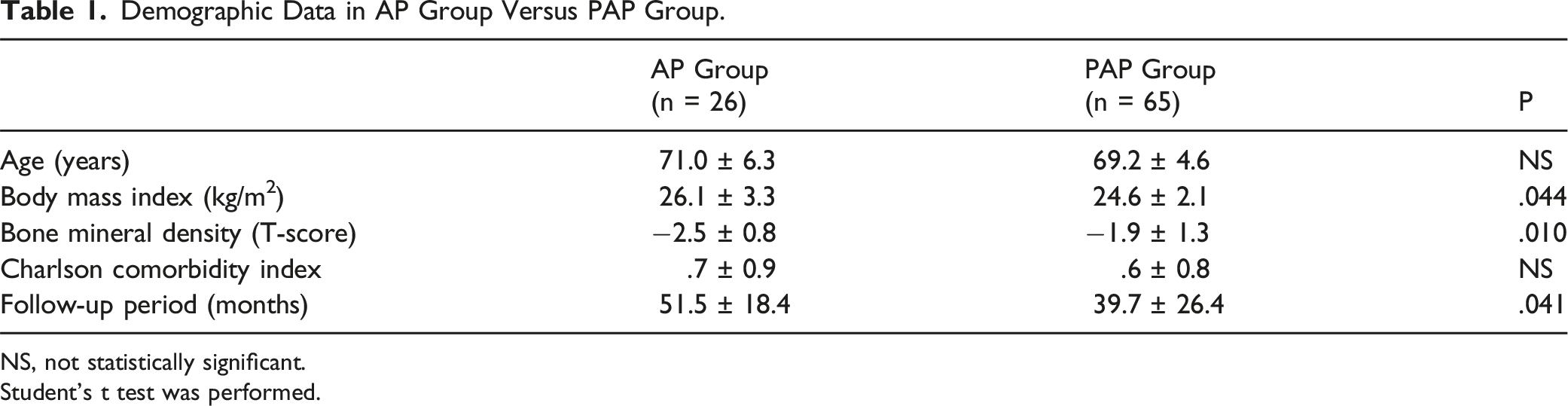
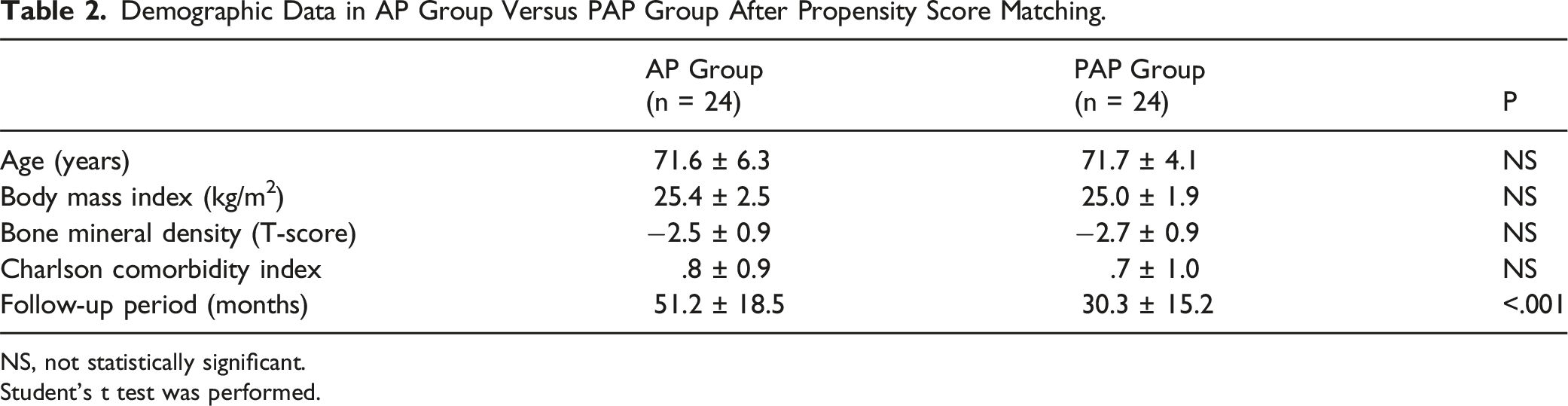
A total of 91 patients who met the inclusion criteria were enrolled, of whom 26 underwent MIS-LLIF ACR followed by posterior surgery (AP group) (Figure 3) and 65 underwent posterior release-ACR-posterior surgery (PAP group) (Figure 4). The mean age was 69.7 ± 5.2 without statistically significant difference between the two groups, and 88 of the 91 patients were female. The mean follow-up period was 51.5 ± 18.4 in the PAP group, and 39.7 ± 26.4 (P = .041) in the AP group. Mean CCI was .7 ± .9 in the AP and .6 ± .8 in the PAP group without significant difference. Although the mean age was not different between the two groups, AP group had greater BMI (26.1 ± 3.3 m/kg2 vs 24.6 ± 2.1 m/kg2, P = .044) and lower T-score of BMD (−2.5 ± .8 vs −1.9 ± 1.3, P = .010) than PAP group (Table 1). After PS matching, only follow-up period between the groups was different (Table 2). Sequential radiographs of a 71-year-old female patient with degenerative sagittal imbalance who underwent MI-LLIF using hybrid anterior-posterior surgery (AP group). (A) Preoperative whole spine standing lateral radiograph (B) Postoperative 1-year whole spine standing lateral radiograph (C) Postoperative 5-year follow-up showing stable maintenance of fused construct with slightly increased C7 sagittal vertical axis. Sequential radiographs of a 69-year-old female patient with degenerative sagittal imbalance who underwent pre-posterior release with ACR and posterior instrumentation (PAP group) (A) Preoperative whole spine standing lateral radiograph showing major sagittal deformity. (B) Postoperative 3 months’ whole standing lateral radiograph showing a restoration of global sagittal alignment. (C) Postoperative 2 years’ whole spine standing lateral radiograph showing aggravated global sagittal alignment due to nonunion with rod fracture at L3-L4 level. (D) After revision surgery (additional bone graft and change of rod), sagittal malalignment was restored. Demographic Data in AP Group Versus PAP Group. NS, not statistically significant. Student’s t test was performed. Demographic Data in AP Group Versus PAP Group After Propensity Score Matching. NS, not statistically significant. Student’s t test was performed.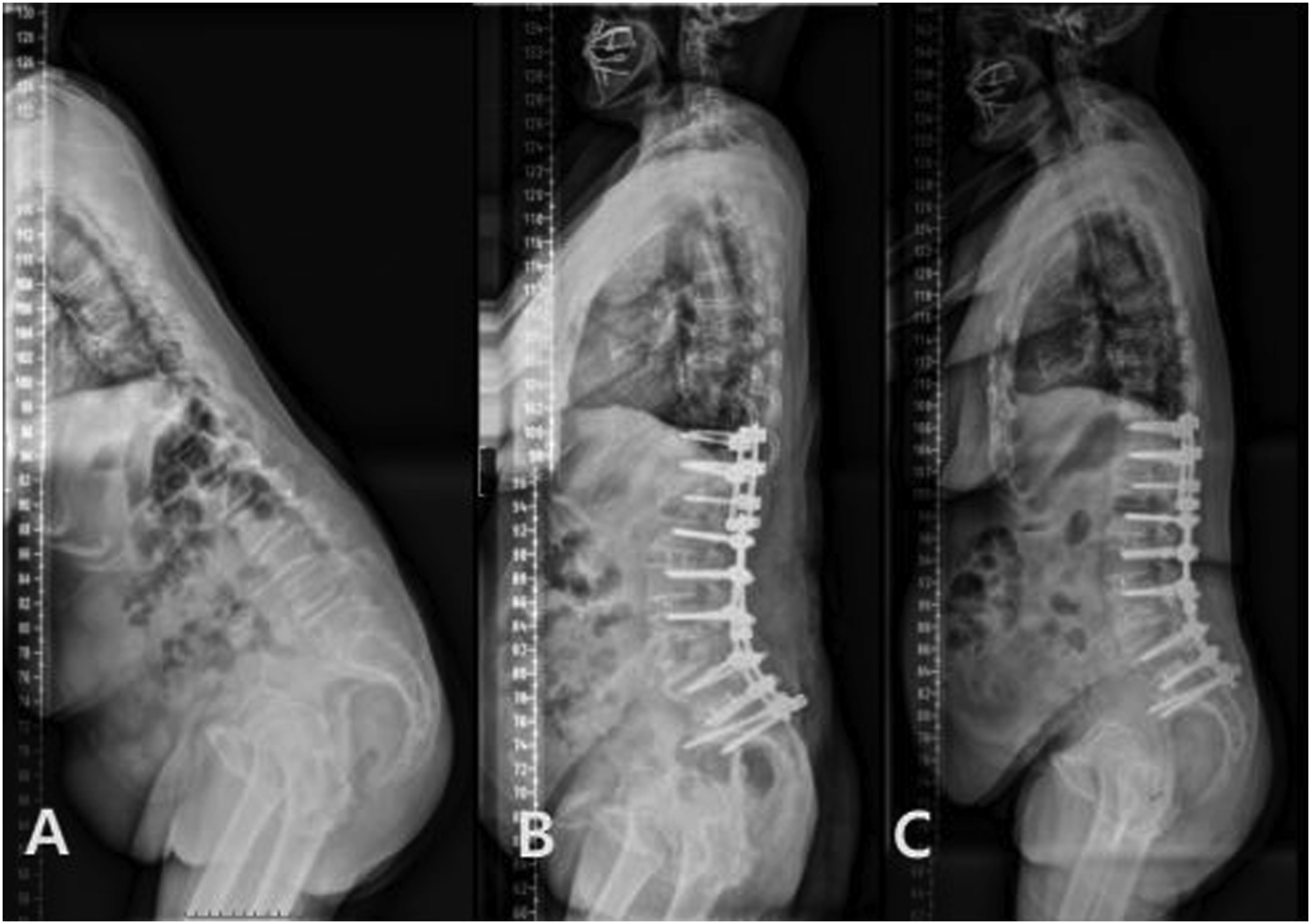
Perioperative Complications
Perioperative Complications in AP Group Versus PAP Group.
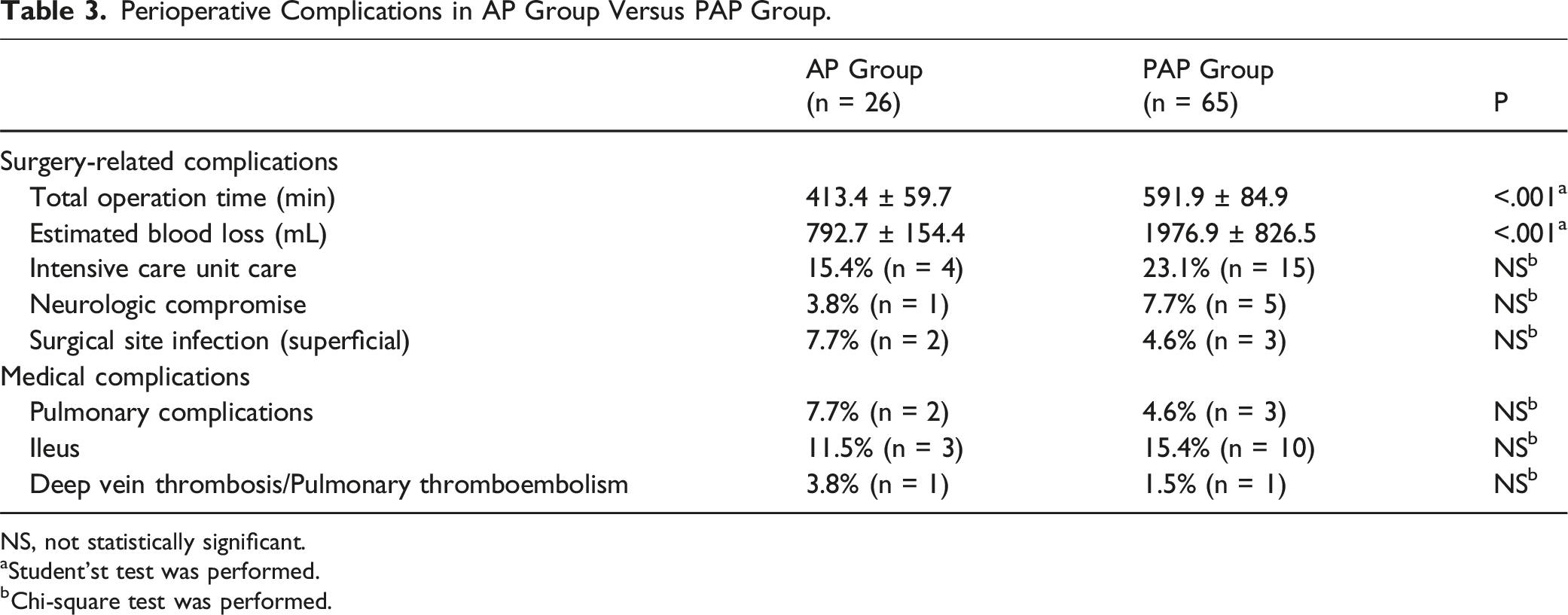
NS, not statistically significant.
aStudent’st test was performed.
bChi-square test was performed.
Perioperative Complications in AP Group Versus PAP Group After Propensity Score Matching.
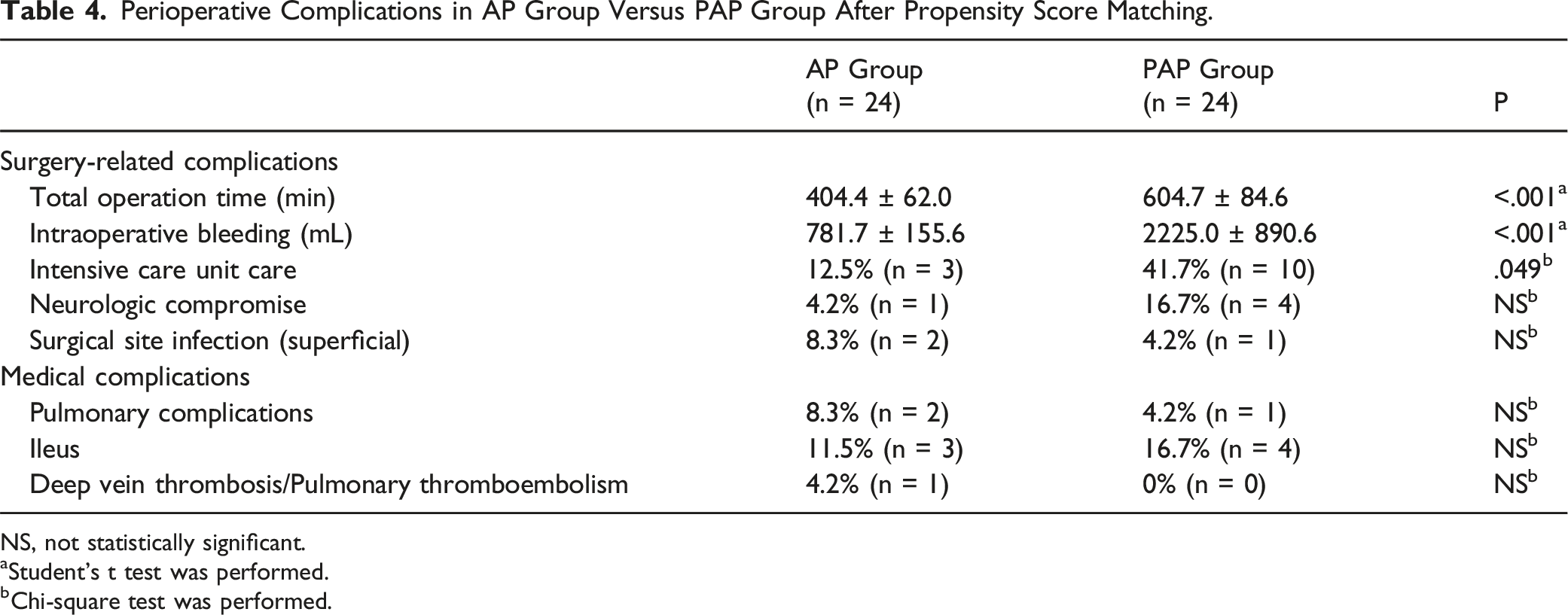
NS, not statistically significant.
aStudent’s t test was performed.
bChi-square test was performed.
Radiological Outcomes
Comparison of Radiological Outcome Between AP and PAP Groups.
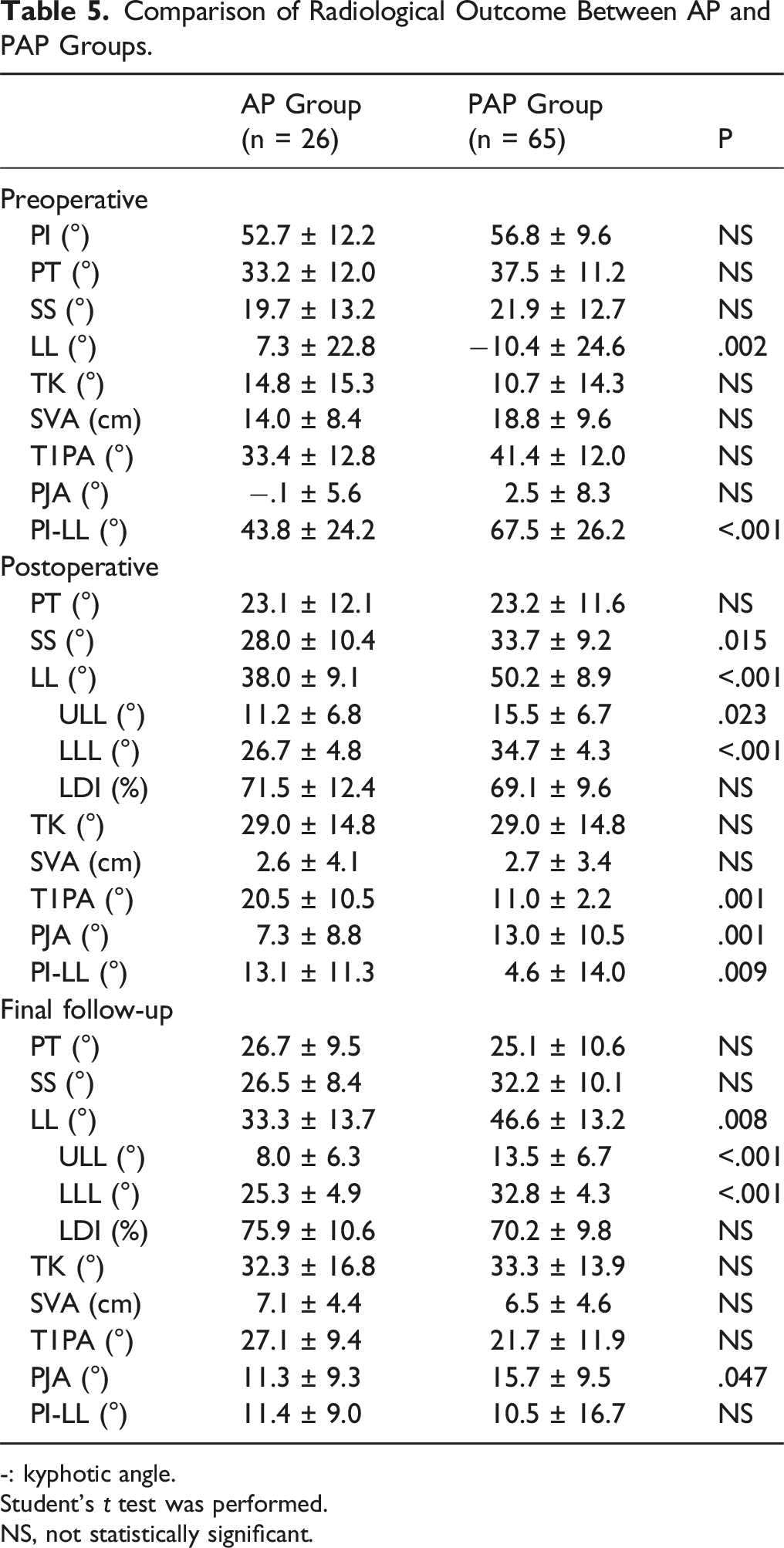
-: kyphotic angle.
Student’s t test was performed.
NS, not statistically significant.
Mechanical Complications and Reoperations
Postoperative Mechanical Complications and Reoperation in AP Group Versus PAP Group.
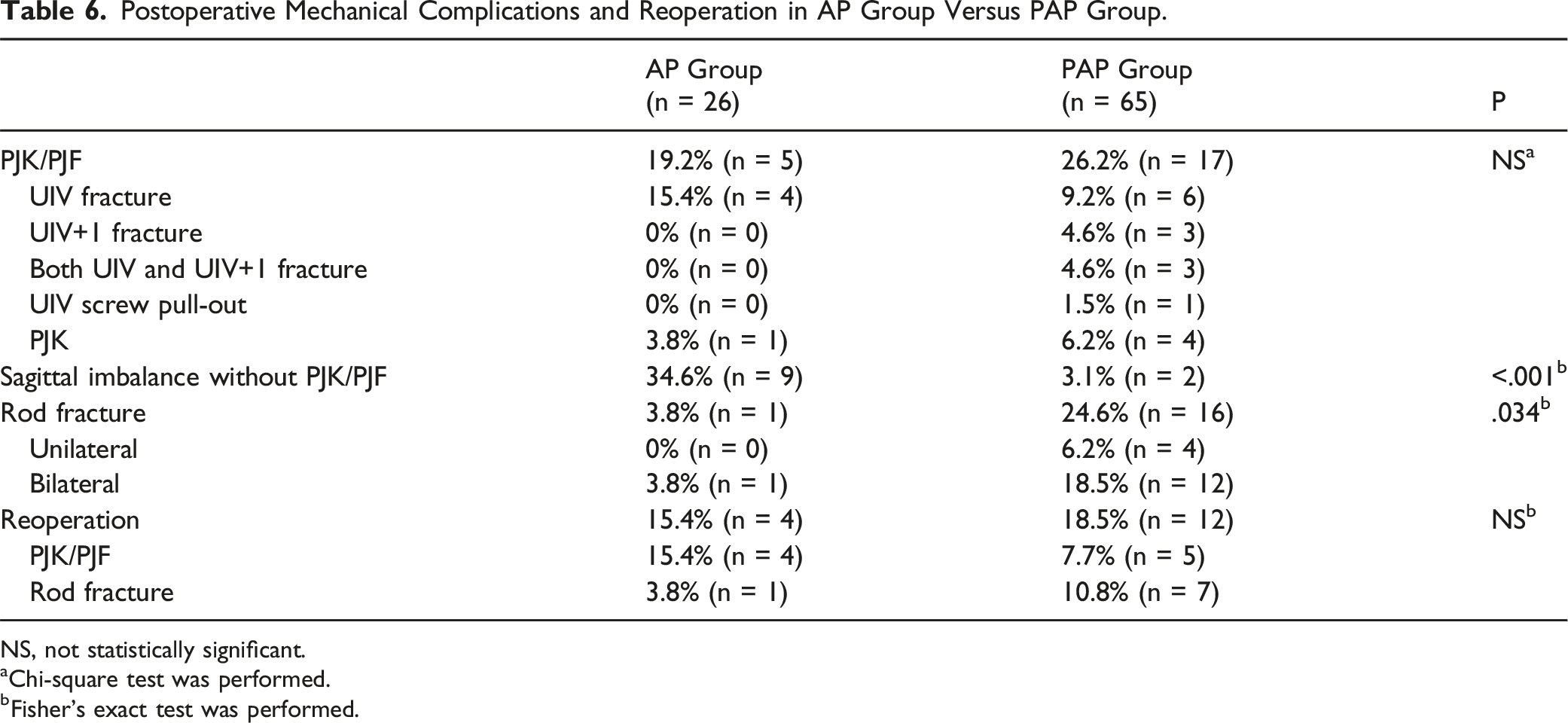
NS, not statistically significant.
aChi-square test was performed.
bFisher’s exact test was performed.
Postoperative Mechanical Complications in AP Group Versus PAP Group After Propensity Score Matching.
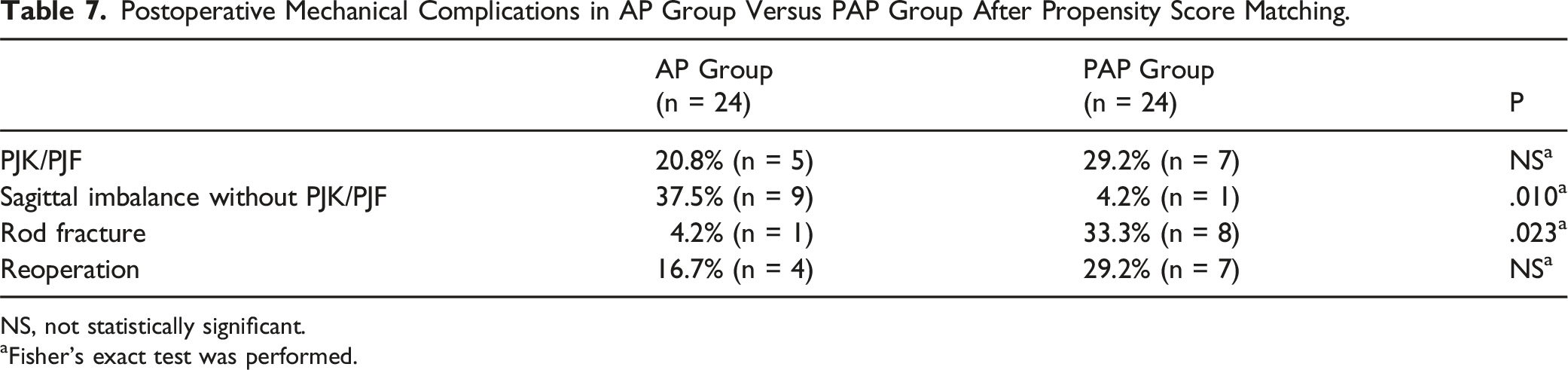
NS, not statistically significant.
aFisher’s exact test was performed.
Clinical Outcomes
Comparison of Clinical Outcomes.
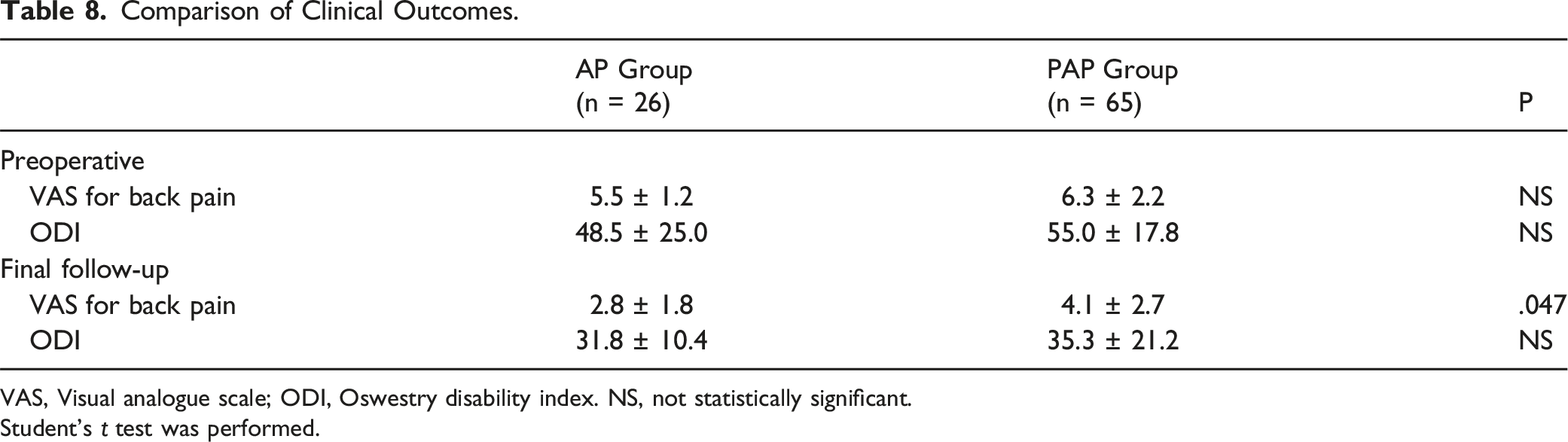
VAS, Visual analogue scale; ODI, Oswestry disability index. NS, not statistically significant.
Student’s t test was performed.
Discussion
Generally, it is accepted that PAP showed superior radiological outcomes compared with AP for surgical correction because AP through MIS LLIF with a small surgical window could be fundamentally limited to adequate exposure of the anterior longitudinal ligament (ALL) due to the risk of vascular injury.3-5 However, each surgical procedure has its own merits and demerits.9,15,16 ACR by MIS-LLIF was not suitable for the treatment of sagittal imbalance greater than 7 cm of SVA, and open approaches, including three-column osteotomies, were recommended. 8 PAP is a valuable complement to other realignment techniques for severe sagittal plane deformities and was the most effective at the lower lumbar spine using hyperlordotic cages.17,18 Akbarnia et al 19 also suggested that fixed deformities required more extensive surgery and were relative contraindications to ACR without posterior osteotomies.
In our study, both groups showed an SVA of >10 cm (average, 14 cm vs 18.8 cm) and PI-LL mismatch greater than 40° with PT greater than 30° preoperatively. A significant improvement in spinopelvic alignment was observed after surgical correction in the both groups. However, the PAP group showed greater improvement in spinopelvic parameters (SS, LL, T1PA, and PI-LL) compared with those of the AP group. In particular, postoperative LL (38.0° ± 9.1° vs 52.2° ± 12.5°, P < .001) and PI-LL (13.1° ± 11.3° vs 4.6° ± 14.0°, P = .009) significantly improved more in the PAP group. In PAP, it was thought that the segments became more mobile during anterior surgery (LLIF) by performing posterior muscle dissection and grade 2 Schwab osteotomy in on-involved segments, so that it could be inserted with lesser damage to the bony endplates or a larger size could be inserted during cage insertion, and which resulted in more gain of disc space height. This suggests that PAP provides a more powerful correction for sagittal imbalances.
However, in our study, the PAP group had higher incidence of RF than the AP group did. RFs, either unilateral or bilateral, were identified in 16 patients (24.6%) in the PAP group and in one patient (3.8%) in the AP group (P = .034). Nevertheless, the overall incidence (18.7%) of RF was similar to 12% to 47% in other reports.20,21 Based on these results, patients in the PAP group had larger sagittal deformity (7.3° ± 22.8° in AP vs −10.4° ± 24.6°in PAP) preoperatively, which eventually required more forceful correction of LL leading to RF. It is considered that excessive removal of the ALL and the posterior bony structures to obtain desirable LL consequently resulted in the instability of the fusion construct and the lack of posterior bony fusion area. In addition, the posterior rods should be customized to bear the newly surgically obtained LL. In biomechanical studies,22-24 it was demonstrated that rod contouring could significantly reduce the yield strength of the rods. Thus, sacrificing ALL and overcorrection with rod contouring may be major contributors to the RF development. Despite more frequent mechanical complications, the corrective power was better in the PAP. Therefore, if there is an additional effort to reduce mechanical complications, this method can be used carefully. Other studies have suggested the use of multi-rod technique 25 or the use of cobalt-chrome rod 26 as alternative solution to reduce RF.
With regard to the relationship between PJK/PJFs and correction rate, moderate PJK was observed with undercorrection and severe PJK with overcorrection of the sagittal balance. 27 The highest incidence of PJK/PJFs was also reported in patients with overcorrection beyond age-adjusted sagittal alignment.28,29 In our study, overall, 22 (24.2%) patients developed PJK or PJF. The incidence of PJK/PJFs in this study at the age of 65 years was similar to that reported previously.12,29,30 However, the PAP group had a higher tendency for PJK/PJF, with an incidence of 17 patients (26.2%) in the PAP group than in five (19.2%) in the AP group, although the difference was not statistically significant. The higher incidence of PJK/PJF in the PAP group may be explained by larger LL correction. Not only the amount of corrected LL, however, the effect of LDI on PJK has been investigated by several researchers and its impact on the occurrence of PJK is still in ongoing debate in recent studies.31-33 We further measured and compared the postoperative LDI, and which was not statistically different between the two groups. (Table 5) It was thought that it was intended to improve the lower lumbar lordosis (L4-S1 lordosis) to create physiological curves during surgery in the both groups, and this has not been clarified in this study. In recent studies,34-37 moreover, methods for evaluating bone strength for each vertebral body have been introduced such as HU (Hounsfield Units) values and VBQ (Vertebral Body Quality) scores, and which are thought to help quantitatively analyze the preoperative bone quality of UIV or UIV+1 level causing PJF by bony failure. In this study, however, since not all patients had preoperative computed tomography (CT) or magnetic resonance imaging (MRI) including the segments above UIV, the assessment of HU or VBQ was not performed. It would have been better study if those methods were added to distinguish the cause of PJF or PJK in each group.
However, sagittal imbalance with an increase of more than 5 cm at the final follow-up compared to postoperative SVA was noted in 9 patients (34.6%) in the AP group and 2 patients (3.1%) in the PAP group, with statistical significance (P < .001). Park et al 38 reported postoperative sagittal imbalance would develop without PJK/PJFs that were associated with less correction of sagittal alignment and degeneration of the paravertebral muscles, resulting in the hip joint serving as the center of rotation. Therefore, these results could explain the relatively higher incidence of sagittal imbalance without PJK/PJFs in patients in the AP group resulting from less correction of sagittal alignment than in the PAP group.
Deformity correction is associated with a high risk of complications in elderly populations. Smith et al 29 noted a 78.9% complication rate in the 65-86-year-old group vs 55.4% in the 18-44-year-old group. It was not surprising that increased age was a factor associated with selecting an MIS approach, given the decreased exposure-related morbidity and perceived decreased complication risk. 39 Conversely, increasingly severe deformities and the need for open decompression were the main factors influencing the selection of traditional open surgery. Soroceanu et al 40 reported the incidence of mechanical complications was approximately 31.7%, with half requiring revision surgery. In our study, 20 patients (22.0%) had medical complications and 50 (54.9%) of 91 patients developed mechanical complications; of these, 16 (17.6%) of 91 patients underwent reoperation, 4 (15.4%) in the AP group, and 12 (18.5%) in the PAP group. Of those who underwent reoperation, 4 underwent reoperation due to recurrence of UIV and UIV+1 fracture in two patients in each group. Of the 17 patients with RF in both groups, seven underwent reoperation due to progression of kyphotic deformity with pseudarthrosis at the RF site in the PAP group. Our study showed that 41.2% of the patients with RF required revision surgery.
Clinically, the PAP group had higher VAS score for back pain at the final follow-up, which may be related to the higher incidence of RF and PJK/PJF. Therefore, spine surgeons should be aware that each surgical procedure has different advantages and disadvantages for the correction of ASD with DSI. Recently, the preference of our spine team was to perform AP in patients with more medical comorbidities as this study showed that the PAP group manifested more intraoperative bleeding and longer operation time (P < .001), even though major medical complications were treated without any sequelae with conservative treatment.
Several inherent limitations of this study must be acknowledged. First, this was a non-randomized, retrospective cohort study. Especially, AP group basically included very small numbers of patients. However, its strength was the reduction of possible sampling bias with the same fusion levels, similar disease entities, and similar ages for the two different surgical procedures by PS matching. Second, this study could not select the best procedure for both the surgical approaches. However, the PAP procedure showed significant improvement with statistical significance in sagittal correction, which might be recommended for pre-posterior release for severe fixed DSI with less flexibility. Preoperative evaluation of spinal flexibility would have enabled to clarify the indication of each method. Moreover, because it is thought that patients who needed larger sagittal correction belonged to the PAP group, the presence of some selection bias is considered a limitation of this study. It would have been a better study if the patient groups with equal or similar preoperative spinopelvic parameters. However, the indications for the two surgical approaches could vary according to the surgeon’s preference, magnitude of radiographic correction, and preoperative medical comorbidity.
In conclusion, PAP provides a more powerful correction for severe sagittal malalignment than AP. However, AP results in less intraoperative bleeding, operation time, and postoperative complications. Therefore, this study does not merely suggest that one treatment is superior to the other. Prior to undergoing correction surgery for ASD with severe DSI, thorough consideration of potential complications and reduction of the risks associated with mechanical complications is of paramount importance.
Footnotes
Authors’ Contributions
JA: manuscript writing, critical revision, statistical analysis; SIK: statistical analysis; YCK, KTK, and YHK: critical revision; SMK and TK: data acquisition; KYH: study concept/design, draft manuscript writing, and critical revision. All authors have read, reviewed, and approved the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare no competing interests regarding any of the materials or devices described in this article. No benefits in any form have been received or will be received from a commercial party directly or indirectly related to the subject of this study. JA, nothing to disclose; SIK, nothing to disclose; YCK, nothing to disclose; KTK, nothing to disclose; YHK, nothing to disclose; SMK, nothing to disclose; TK, nothing to disclose; KYH, nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The patients’ data were collected in Kyung Hee University Hospital at Gangdong. The datasets generated and/or analyzed during the current study are available from the corresponding author (KYH) upon reasonable request.
Statement of Human and Animal Rights
Human subjects in this study are not identifiable, such that patients’ names, initials, hospital numbers, dates of birth, or other protected healthcare information were not disclosed.