
Abstract
Study Design
Retrospective cohort study.
Objective
To provide updated rates for approach-related postoperative motor deficits following lateral lumbar interbody fusion (LLIF) and identify risk factors.
Methods
1000 stand-alone LLIF procedures between 2006 and 2024 were reviewed and divided into the first decade (2006-2015, n = 395) and the second decade (2016-2024, n = 605). Electronic records were screened for iliopsoas and quadriceps deficits preoperatively and postoperatively (at discharge, 6 weeks, 3 months, 6 months, 1 year, and last follow-up) defined as a decline in MRC strength grades relative to baseline.
Results
The incidence of postoperative ≥1 MRC grade iliopsoas deficits declined from 12.7% to 4.1% and quadriceps deficits from 5.3% to 1.7% at 6 weeks (P < 0.001 and P = 0.002, respectively). In the second decade, persistent iliopsoas or quadriceps weakness was observed in 0.8% and 0.5% (n = 3) of patients at 6 months and 1 year, respectively. At 2 years, only 1 of 605 patients had residual ≥1 MRC grade quadriceps weakness, and no patient had persistent iliopsoas weakness. Independent predictors of deficits were surgery at L4/5 (iliopsoas: OR 2.2, 95% CI 1.1-4.5; quadriceps: OR 5.9, 95% CI 1.3-26.5) and operative time [per hour] (iliopsoas: OR 1.4, 95% CI 1.2-1.6; quadriceps: OR 1.4, 95% CI 1.1-1.7).
Conclusions
Rates of postoperative motor deficits after standalone LLIF have improved significantly over the past decade. Increased surgical time and surgery at L4/5 remain key risk factors, but most deficits are transient. LLIF at L4/5 can be considered safe in appropriately selected patients.
Introduction
Since its introduction in 2006, lateral lumbar interbody fusion (LLIF) has become a valuable surgical strategy in managing degenerative and deformity-related lumbar spine pathologies, gaining popularity in recent years.1,2 The LLIF technique utilizes a minimally invasive retroperitoneal transpsoas approach, offering multiple advantages over traditional posterior lumbar interbody fusion (PLIF), or transforaminal lumbar interbody fusion (TLIF). 3 These benefits include indirect neural decompression, larger interbody graft placement, avoidance of direct manipulation of the thecal sac and nerve roots, and preservation of posterior spinal musculature.4-6
Biomechanically, LLIF achieves superior anterior column support compared to posterior techniques, with cages spanning the dense apophyseal rings bilaterally. 7 Clinically, the technique offers reduced blood loss, shorter operative times, and reduced length of hospital stay. 8 Additionally, by preserving posterior muscles, LLIF may lower the risk of long-term complications such as paraspinal muscle atrophy and adjacent segment disease.9,10
Despite these advantages, the transpsoas corridor traverses the lumbar plexus, introducing a risk of postoperative motor deficits, particularly at the L4/5 level, where the femoral nerve migrates more anteriorly within the psoas muscle. 11 Early experiences with LLIF reported transient and persistent motor weakness rates of up to 51% and 49%, respectively, 12 leading some to question the broader role of LLIF in spinal fusion surgery. 13
Interpretation of these early results is complicated by several factors. Many prior studies examined either isolated quadriceps or iliopsoas weakness, or included unrelated muscle groups such as the tibialis anterior, which is not directly affected by the lateral approach. 14 In addition, patient cohorts were often heterogeneous, including posterior decompressions and supplemental instrumentation, which confounded attempts to isolate the specific neurologic risks of the lateral approach.
The perception of high complication rates may have discouraged some surgeons from adopting LLIF or led to its limited application at L3/4 and above. However, these early complication rates do not reflect our institutional experience, where LLIF has been routinely performed, including at L4/5, since its initial introduction in 2006. Over time, technical refinements and greater anatomic understanding have improved the safety profile of LLIF.11,15,16 More recently, preoperative imaging to assess lumbar plexus and vascular anatomy has informed patient selection, helping avoid cases with unfavorable trajectories. 17 As such, previously reported complication rates may not accurately reflect current practice.
The primary aim of this study was to provide a contemporary, practice-based description of the incidence and recovery trajectory of approach-related postoperative motor deficits following LLIF and to contextualize how these outcomes have changed over time. A secondary aim was to re-examine risk factors for motor deficits, with a particular focus on reassessing the risk associated with surgery at L4/5.
Methods
Patient Population
Institutional Review Board (IRB) approval was obtained prior to study initiation (IRB #2020-1877). The reporting of this study follows the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative. 18 Patients who underwent lateral lumbar interbody fusion (LLIF) for degenerative disc disease (DDD) at our academic institution between 2006 and 2024 were retrospectively reviewed. Patient selection for LLIF followed standard institutional criteria throughout the study period. Standalone LLIF was considered in patients with lumbar spondylosis resulting in back pain and radiculopathy, including those with foraminal stenosis, lateral recess stenosis, or mild to moderate central stenosis, but not in patients with severe central stenosis, isthmic lysis, or high-grade spondylolisthesis.19-21 Preoperative MRI and CT were routinely reviewed to assess psoas morphology, plexus position, and vascular anatomy. 17 At L4/5 in particular, lateral access was pursued only when imaging demonstrated a safe working corridor, and cases with unfavorable anatomic features, including a rising psoas configuration or laterally positioned vascular structures, were not considered candidates for a lateral approach at that level. 22 Patients were excluded if they underwent concomitant posterior decompression and/or instrumented fusion or additional anterior lumbar interbody fusion (ALIF). Patients were grouped into the first and second decade of surgery, defined as 2006-2015 and 2016-2024, respectively. Baseline demographic data, comorbidities, surgical details, and perioperative data were collected.
Motor Deficit Assessment
All motor examinations were performed by attending spine surgeons or trained clinical providers using a consistent institutional protocol, which included assessment of the same muscle groups at each postoperative visit. Motor strength examinations were performed for the iliopsoas (hip flexion) and quadriceps (knee extension) muscle groups bilaterally. For all patients, neurologic assessments performed preoperatively, and at 6 weeks, 6 months, and 1 year postoperatively were evaluated. For patients treated in the second decade, additional neurologic assessments at hospital discharge and 3 months were reviewed to characterize within-cohort recovery trajectories; between-decade comparisons were limited to follow-up timepoints available in both decades (6 weeks, 6 months, and 1 year). Patients with persistent motor weakness at 1 year underwent continued follow-up beyond this time until the last follow-up available. Motor strength was graded according to the Medical Research Council (MRC) method 23 on a scale from 0 to 5: 0 = no muscle contraction; 1 = muscle contraction without movement; 2 = movement with gravity eliminated; 3 = movement against gravity; 4 = movement against mild resistance; and 5 = full strength. A decline of ≥1 motor grade in any muscle group compared to preoperative baseline was considered a postoperative motor deficit. Accordingly, all postoperative deficits reported in this study represent new or worsened weakness relative to each patient’s own preoperative strength, and preexisting weakness alone was not classified as a postoperative deficit. For example, a patient with preoperative MRC grade 4 iliopsoas strength who declined to grade 3 postoperatively, or a patient who developed new contralateral weakness despite stable ipsilateral strength, was classified as having a postoperative motor deficit. A reduction of motor strength of ≥2 MRC strength grades relative to baseline was further defined as a ≥2 MRC grade deficit. In patients with preexisting weakness, a new deficit was defined as either further decline in the same muscle, involvement of a different muscle group, or new weakness on the contralateral side. Sensory deficits and reflex changes were not included in this analysis due to inconsistencies in assessment and documentation.
Surgical Technique
LLIF procedures were performed by 4 experienced, board-certified orthopedic spine surgeons using a mini-open technique with the patient in the lateral decubitus position, as described previously.24-26 After fluoroscopy-guided positioning and level detection, a diagonally oriented skin incision (∼5 cm) was made along the external oblique muscle fibers. Following a sharp incision of the external oblique fascia, blunt dissection was carried through the internal oblique and transversus abdominis muscles to access the retroperitoneal space and the psoas muscle. Retroperitoneal fat was swept off the psoas muscle from posterior to anterior, preserving the integrity of the peritoneum. The psoas muscle was palpated, and the disc space accessed via blunt dissection using the finger or Kittner dissectors, sweeping across the disc space in an anteroposterior direction. The lumbar plexus could often be palpated, especially at L4/5, and was carefully retracted posteriorly. The vertebral bodies were not further exposed to avoid injury to segmental arteries. Discectomy and endplate preparation were performed under direct visualization, with care taken to preserve endplate integrity. Interbody cages were inserted to span the apophyseal ring bilaterally. The standard cage width was 22 mm in the anteroposterior dimension, with 18 mm occasionally and 26 mm rarely selected based on individual patient anatomy. Lateral augmentatin with plating or integrated lateral screw fixation was used selectively based on implant fit, without supplemental posterior instrumentation. Retraction time was minimized as much as possible, ideally kept under 20 minutes per level. Intraoperative neuromonitoring included somatosensory evoked potentials (SSEP) and free-run electromyography (EMG) in all cases throughout the study period. 27 Transcranial motor evoked potentials (tc-MEP) and triggered EMG were applied selectively at the discretion of the surgical team.
Statistical Analysis
All statistical analyses were conducted using STATA (version 18.0; StataCorp LLC, College Station, TX, USA). Data distributions were evaluated by histogram inspection and Q–Q plots. Baseline characteristics were compared using Student’s t-tests, Wilcoxon rank-sum tests, or chi-square tests, as appropriate. Rates of motor deficits at each time point and for each muscle group were compared using chi-square or Fisher’s exact tests. Because neurologic recovery was assessed at discrete, clinically scheduled follow-up visits rather than at continuous or precisely timed intervals, time-to-event analyses were not performed. Recovery was therefore analyzed using point-prevalence at standardized postoperative time points. Multivariable logistic regression was used to identify predictors of iliopsoas and quadriceps weakness at 6 weeks postoperatively. The number of covariates included in each model was determined by the number of observed events to maintain an appropriate events-per-variable ratio and minimize overfitting. For the iliopsoas model, 75 events were observed, permitting inclusion of 6 covariates, corresponding to approximately 12 events per variable. For the quadriceps model, 31 events were observed, and the model was therefore restricted to 3 core covariates, corresponding to approximately 10 events per variable. Model discrimination was assessed using the area under the receiver operating characteristic curve. Multicollinearity was assessed using variance inflation factors (VIF), and all predictors demonstrated acceptable levels. Statistical significance was defined as P < 0.05.
Results
Patient Characteristics
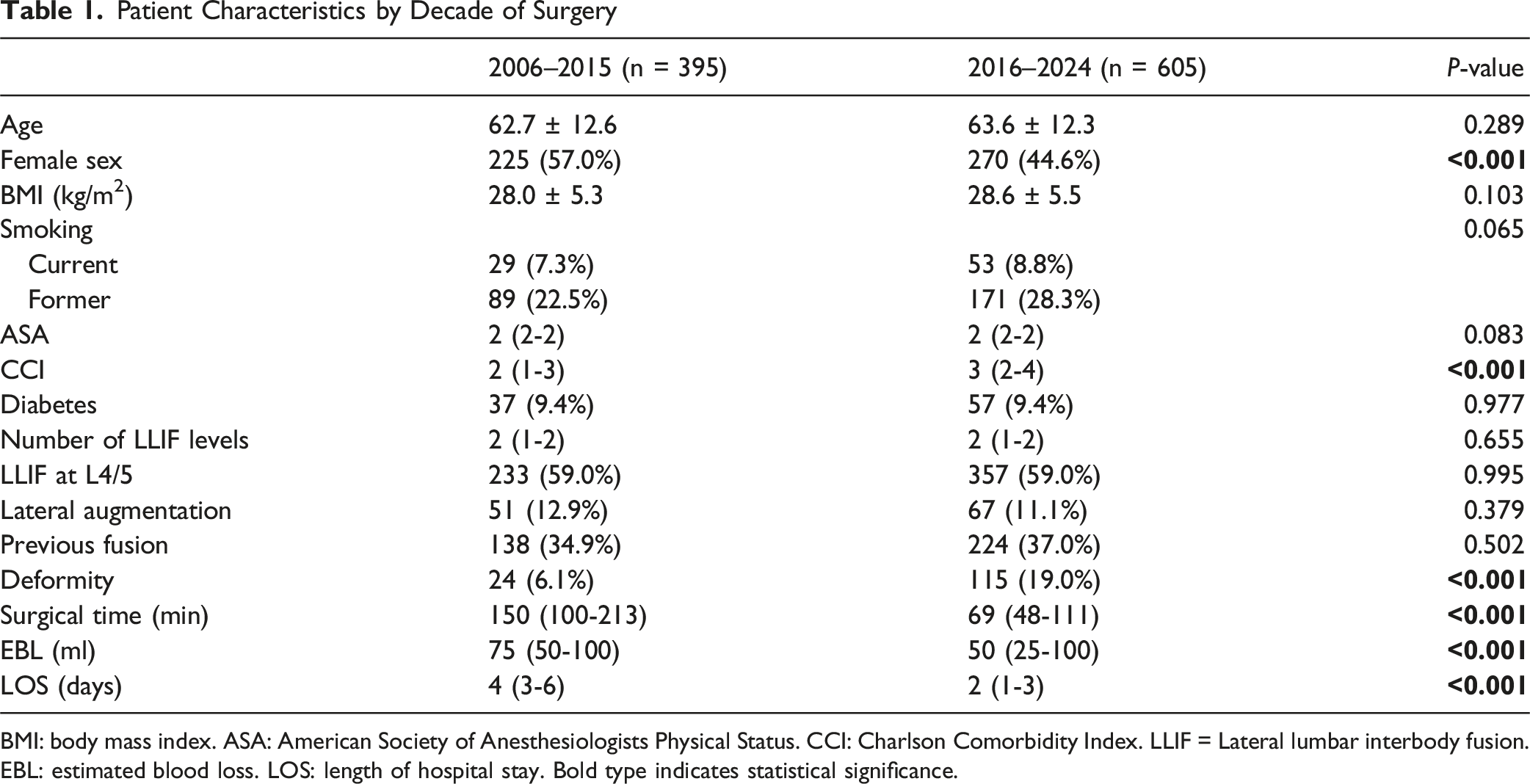
A total of 2394 LLIF procedures were performed between 2006 and 2024. After excluding patients with posterior decompression and instrumentation (n = 1190) and those with concomitant ALIF (n = 83), 1121 patients remained (Figure 1). Of these, 1000 patients (89.2%) had complete preoperative and postoperative strength examinations at all time points in the first postoperative year and were included in the analysis. Among the 1000 patients included, 395 (39.5%) were treated in the first decade and 605 (60.5%) in the second. Patient characteristics differed between decades in sex distribution, comorbidity burden, and percentage of deformity cases (Table 1). The median number of levels fused was 2 (range 1-4), and the proportion of LLIF performed at L4/5 (59.0%) was consistent across both decades. Surgical time from skin incision to closure (150 minutes vs 69 minutes), estimated blood loss (75 mL vs 50 mL), and length of hospital stay (4 days vs 2 days) were all significantly lower in the second decade compared to the first (all P < 0.001). Lateral augmentation was used in 11.8% of cases and did not differ between decades and was not associated with postoperative motor deficits. Although baseline characteristics differed between decades, subsequent analyses focused on standardized neurologic endpoints and common follow-up timepoints to allow consistent comparison of approach-related motor outcomes. Study flow chart Patient Characteristics by Decade of Surgery BMI: body mass index. ASA: American Society of Anesthesiologists Physical Status. CCI: Charlson Comorbidity Index. LLIF = Lateral lumbar interbody fusion. EBL: estimated blood loss. LOS: length of hospital stay. Bold type indicates statistical significance.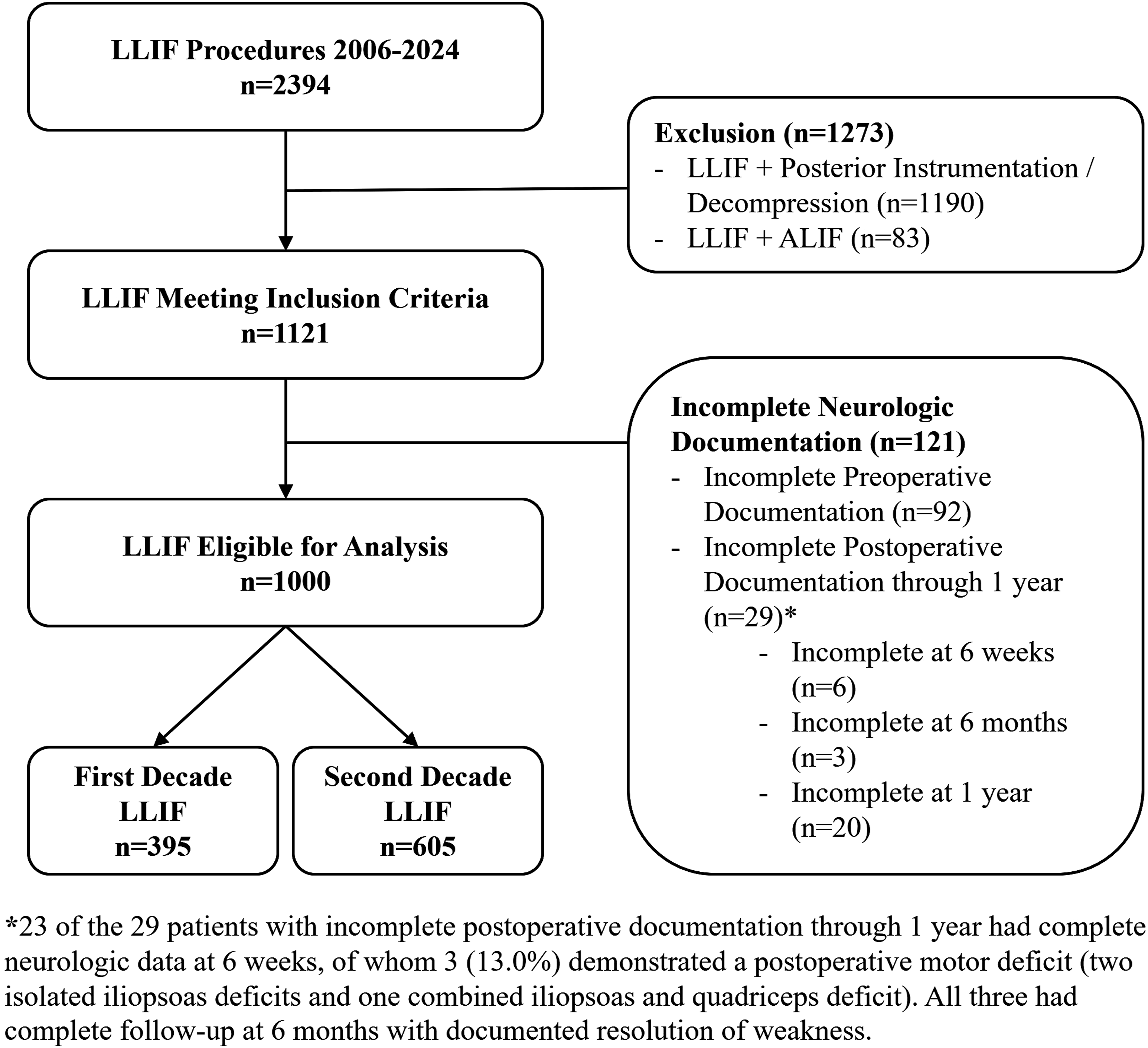
Motor Deficits in First vs Second Decade
Postoperative motor deficits were less frequent in the second decade (Figure 2). At 6 weeks, iliopsoas weakness occurred in 12.7% of patients in the first decade vs 4.1% in the second (P < 0.001). At 1 year, persistent iliopsoas weakness was observed in 0.8% (n = (3) of patients in the first decade and 0.3% (n = (2) in the second (P = 0.308). A ≥2 MRC grade deficit at 6 weeks postoperatively occurred in 2.5% (n = 10) of first-decade patients vs 0.7% (n = (4) in the second (P = 0.015). No patients had a ≥2 MRC grade iliopsoas deficit at or beyond 6 months. Motor deficits and recovery by d of Surgery. (A) Iliopsoas. (B) Quadriceps. Weakness defined as loss of ≥1 strength grade are shown at 6 weeks, 6 months and 1 year postoperatively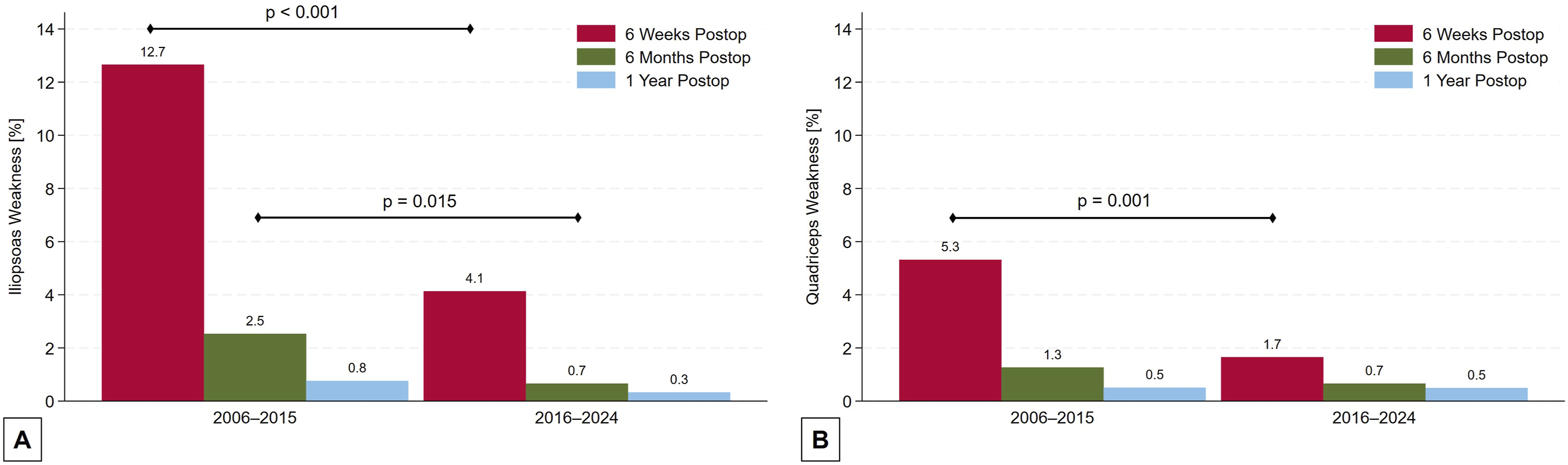
Quadriceps weakness followed a similar trend. At 6 weeks, 5.3% of first-decade patients and 1.7% in the second decade had quadriceps weakness (P < 0.001). Rates at 6 months (1.3% vs 0.7%, P = 0.322) and 1 year (0.5% vs 0.5%, P = 0.982) did not differ significantly between decades. The incidence of ≥2 MRC grade quadriceps deficits at 6 weeks was 1.0% (n = 4) in the first decade and 0.7% (n = 4) in the second (P = 0.542).
Incidence of Motor Deficits and Recovery Rates in Recent Surgical Decade
In the second decade, the incidence of iliopsoas and/or quadriceps weakness with ≥1 grade loss was 17.2% (104 of 605 patients) at discharge, including 16.4% (n = 99) with iliopsoas and 6.0% (n = 36) with quadriceps involvement. Motor deficits steadily improved over the patients follow-up. 74.0% (77/104) fully recovered by 6 weeks postoperatively, leaving 25 patients with a persistent iliopsoas deficit and 10 with a persistent quadriceps deficit. 3-month, 6-month, and 1-year recovery rates were 89.4% (n = 11), 95.2% (n = 5), and 97.1% (n = 3), respectively. Two of the 3 with persistent motor deficits at 1 year had both iliopsoas and quadriceps weakness and 1 had an isolated quadriceps weakness. All patients ultimately recovered full strength between the first and second year postoperatively, except for 1 individual with a persistent ≥2 MRC grade quadriceps deficit at 1 year who improved to MRC grade 4 at 2 years postoperative and remained highly satisfied with the outcome and maintained an active lifestyle.
The incidence of ≥2 MRC grade deficit was low and declined steadily over time. At discharge, 3.0% (n = 18) had such deficits (18 iliopsoas deficits, 4 quadriceps deficits). By 6 weeks, the rate decreased to 1.0% (n = 6) (4 iliopsoas, 4 quadriceps), and by 3 months, it further declined to 0.7% (n = 4; 2 iliopsoas, 3 quadriceps). At 6 months and beyond, only 1 patient had a persistent ≥2 MRC grade deficit, which was a quadriceps deficit, which persisted to the 1-year follow-up but improved to MRC grade 4 at 2 years postoperative.
Motor Deficits and L4/5
Motor deficits were more frequent when the L4/5 level was involved but showed high recovery rates by 6 weeks and continued improvement thereafter (Figure 3). In the second decade, iliopsoas weakness at discharge occurred in 19.1% of patients with L4/5 surgery vs 12.5% with no L4/5 involvement (P = 0.032). At 6 weeks, this rate was 5.9% vs 1.6% (P = 0.006); at 3 months, 2.8% vs 0.4% (P = 0.025). No iliopsoas weakness was observed beyond 6 months in the non–L4/5 group. In the L4/5 group, 1.1% and 0.6% had deficits at 6 months and 1 year, respectively; all recovered over time. ≥ 2 MRC grade iliopsoas deficits at discharge were documented in 4.8% in the L4/5 group vs 0.4% in non–L4/5 (P = 0.001). No non–L4/5 patient had a ≥2 MRC grade iliopsoas deficit beyond 6 weeks. Motor deficits and recovery by L4/5 involvement 2016-2024. (A) Iliopsoas. (B) Quadriceps. Weakness with loss of ≥ 1 strength grade and ≥ 2 strength grades are shown at time of hospital discharge, 6 weeks, 3 months, 6 months and 1 year postoperatively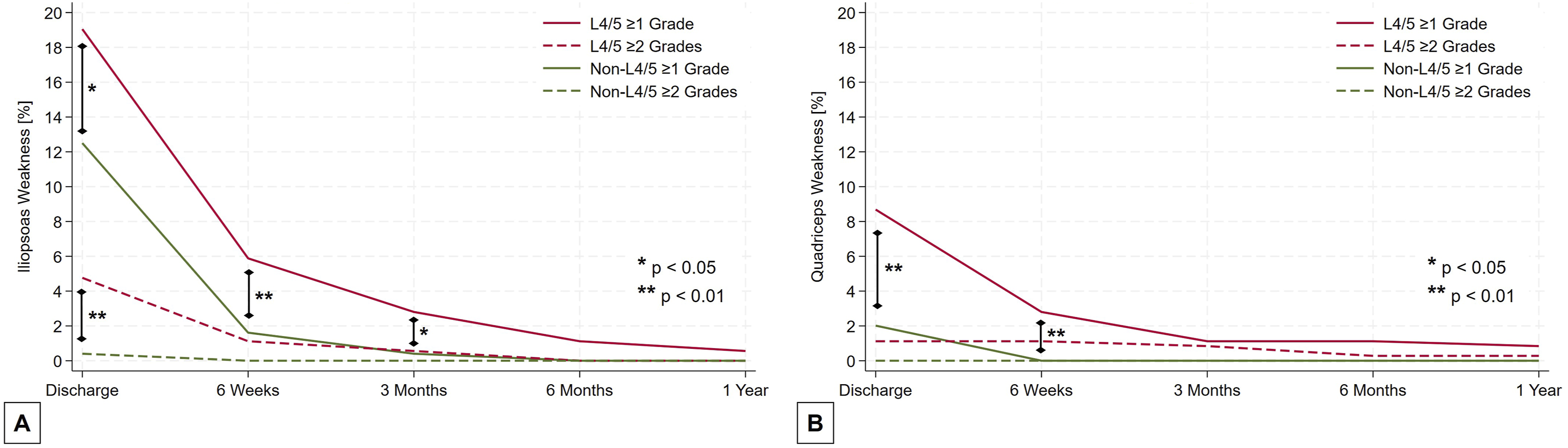
Quadriceps weakness followed a similar pattern. At discharge, 8.7% of L4/5 patients had weakness vs 2.0% in non–L4/5 (P = 0.001). All non–L4/5 patients had recovered by 6 weeks. In the L4/5 group, persistent deficits were seen in 2.8% at 6 weeks, 1.1% at 3 and 6 months, and 0.8% at 1 year. Of these, 2 recovered fully and 1 improved to MRC grade 4 out of 5. No non–L4/5 patient experienced a ≥2 MRC grade quadriceps deficit, whereas in the L4/5 group, 1.1% (n = 4) had a ≥2 MRC grade quadriceps deficit at discharge; 3 fully recovered by 6 months, and 1 improved to MRC grade 4 after 1 year.
Predictors of Motor Deficits
Multivariable Logistic Regression for Outcome Iliopsoas Deficit at 6 Weeks
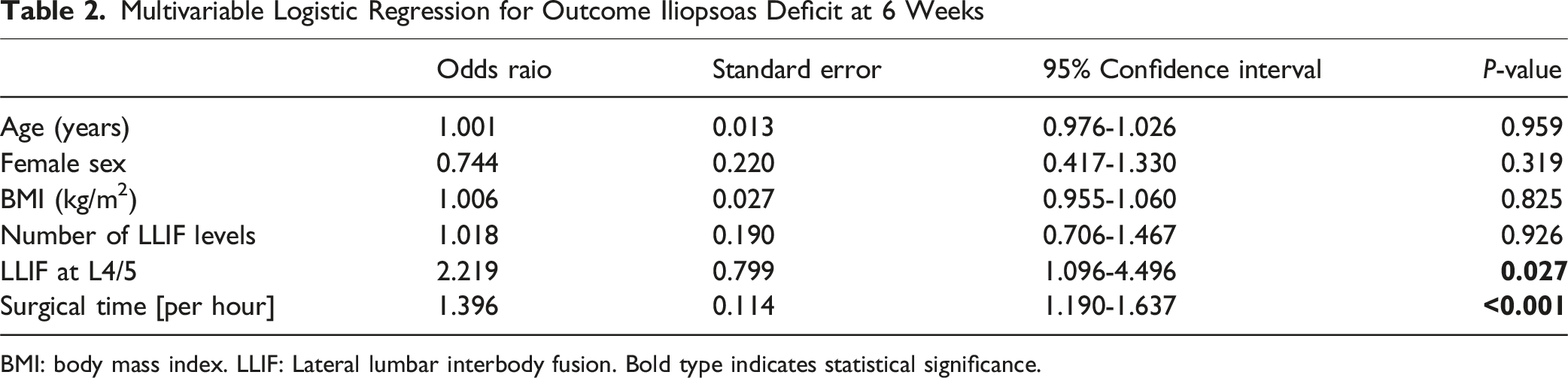
BMI: body mass index. LLIF: Lateral lumbar interbody fusion. Bold type indicates statistical significance.
Multivariable Logistic Regression for Outcome Quadriceps Deficit at 6 Weeks

BMI: body mass index. LLIF: Lateral lumbar interbody fusion. Bold type indicates statistical significance.
Discussion
This is the largest study to date evaluating neurological morbidity of LLIF and how it evolved over time, with a specific focus on approach-related motor deficits. The key findings of this study are as follows: The rate of postoperative motor deficits has substantially declined in recent years, likely reflecting improvements in surgical efficiency, patient selection, and enhanced understanding of plexus anatomy. In experienced hands, strength deficits in hip flexion and/or knee extension occur in approximately 20% of patients at discharge, 5% at 6 weeks, and <1% at 6 months. At 6 weeks, ∼1% of patients present with a ≥1 MRC grade deficit quadriceps deficit, and another ∼1% with a ≥2 MRC grade deficit. 99% of all deficits eventually resolve, with 95% recovering fully by 6 months. LLIF at L4/5 is associated with a two-fold increased risk of iliopsoas weakness and nearly a six-fold increased risk of quadriceps weakness, although both are transient. Increased surgical time is a risk factor for transient weakness in both muscle groups.
The reduction in motor deficits occurred despite an increase in overall comorbidity burden in the contemporary cohort, suggesting that patient comorbidities were not major determinants of approach-related neurologic risk. These findings should be interpreted as reflecting the evolution of clinical practice, surgical efficiency, and anatomic understanding over time, rather than as evidence of a causal effect of surgical era itself. Accordingly, the reported recovery trajectories represent interval-based clinical snapshots rather than precise time-to-event estimates, consistent with real-world postoperative follow-up patterns.
While earlier studies reported iliopsoas weakness rates up to 51%, with persistent deficits in as many as 49% of patients,12,28 our contemporary rates of 4.1% for iliopsoas and 1.7% for quadriceps weakness at 6 weeks highlight the improvements achieved with experience and standardization. Compared with other large LLIF series, including the cohorts reported by Mundis et al, Patel et al, Aichmair et al, and Salzmann et al, our rates in the contemporary decade are among the lowest published and demonstrate a clearer decade-to-decade decline than previously reported. This decline appears to reflect a combination of greater familiarity with the lateral anatomy, more consistent identification of high-risk features on preoperative imaging, and refined intraoperative workflow that reduces retraction time and psoas manipulation. A previous trend toward improved neurological outcomes during the early era of LLIF (2006-2012) did not reach statistical significance at the time. 29 In our study, ≥2 MRC grade quadriceps paresis occurred in only 0.7% of patients, comparable to the 1.8% rate recently published in a multicenter study. 30 Our recent decade incidences of iliopsoas weakness (16.4% at discharge, 4.1% at 6 weeks, and 1.8% at 3 months) are consistent with those reported by Mundis et al.,23,31 who found 21.9% immediately postoperatively and 2.4% at 3 months.
The inclusion of only standalone LLIF cases performed by highly experienced surgeons at a single institution is a major strength of this study and likely explains the somewhat lower rates of motor deficits observed compared to prior reports. By excluding posterior decompression and instrumentation, as well as anterior lumbar interbody fusion, we eliminated confounding factors such as postoperative radiculitis, compressive hematoseromas, and pedicle screw-related nerve injury, which are unrelated to the lateral approach. 29
L4/5 Involvement
L4/5 involvement remained a significant predictor of postoperative motor weakness. In our multivariable analysis, surgery at L4/5 was associated with a more than two-fold increased risk of iliopsoas weakness and nearly six-fold increased risk of quadriceps weakness. These findings align with prior studies, including Salzmann et al [14], who reported higher deficit rates at L4/5. Anatomically, the working corridor at L4/5 narrows due to anterior migration of the lumbar plexus. 11 Importantly, despite this elevated early risk, over 95% of patients recovered by 6 months and over 99% recovered by 2 years postoperative. In contrast to our findings, Patel et al. 30 have not found any association with level involvement in their study.
Surgical Time
Prolonged surgical time was also independently associated with early motor deficits, supporting concerns that extended retraction may increase the risk of plexus injury. 16 However, the odds ratios were relatively low (OR 1.396 and OR 1.353 for iliopsoas and quadriceps, respectively). A categorical analysis further demonstrated substantially higher rates of transient motor deficits in procedures exceeding 120 minutes compared with those completed within 60 minutes, reinforcing operative duration as a clinically meaningful risk marker rather than a strict threshold effect. This aligns with recent evidence questioning the utility of the strict “20-minute rule”. Patel et al. 30 found retraction time alone was not a reliable predictor of postoperative palsy. Although retraction time was not captured in our dataset, our findings suggest that minimizing it is beneficial, but meticulous surgical technique and anatomic awareness are more critical.
Neuromonitoring-Guided Approach vs Mini-Open Approach
Our institutional technique uses a mini-open approach that permits palpation and direct visualization of the psoas and lumbar plexus. This contrasts with a fluoroscopy- and neuromonitoring-guided transpsoas approach used by others. Triggered EMG is no longer routinely performed at our institution, as prior studies have reported variable specificity and mixed predictive value.16,32 While triggered EMG may provide information regarding relative proximity to the lumbar plexus, it does not fully account for stretch or compression injury, therefore may offer limited incremental protective value in the setting of direct anatomic visualization.31,33 Neuromonitoring nevertheless remains an integral component of our intraoperative safety strategy.Free-run EMG and SSEPs, including saphenous nerve monitoring, are used routinely in our practice, and intraoperative alerts lead to standard corrective maneuvers such as reducing table break, decreasing retractor tension, and adjusting anesthesia per protocol. 34 We acknowledge that centers employing a purely transpsoas, dilation-based approach without direct visualization may reasonably rely more heavily on triggered EMG and may reach different conclusions regarding its utility. Future studies incorporating granular neuromonitoring data across different surgical techniques are needed to more definitively define the role and predictive value of these modalities in LLIF.
Motor Deficits in LLIF vs Other Spine Procedures
The 17.4% rate of new motor deficits at discharge observed with the lateral approach in our study is notably higher compared to other common spine procedures. In a recent study of open posterior instrumented fusion with posterior lumbar interbody fusion for degenerative conditions, a lower rate of 5.5% was reported, though the affected muscles differed, with the extensor hallucis longus and tibialis anterior being most commonly involved. 35 Notably, neuromonitoring in that study also failed to predict postoperative motor deficits. Others have reported overall rates of new motor deficits in spine surgery of 10.4%, 36 and a 3.0% incidence of ≥2 MRC grade deficits, matching the rate observed in our standalone LLIF cohort. Importantly, in the present study, the rate of any motor deficit (≥1 grade) declined to 4.1% by 6 weeks, <1% at 6 months, with only 1 of 605 (0.2%) patients experiencing a persistent deficit at final follow-up at 2 years postoperative.
What Have We Learned in Two Decades
Several factors may have contributed to the improved neurologic outcomes: 1. Patient selection and anatomical understanding: Recognition of risk signs such as the “rising psoas” or “Mickey Mouse sign” and unfavorable vascular anatomy is essential. Lateral surgery should be avoided in these cases, particularly at L4/5.17,22 Although a high iliac crest may limit access, we find L4/5 accessible in most cases with angled instruments. The observed shift in gender distribution likely reflects caution with standalone LLIF in women due to lower bone quality and increased risk of cage subsidence.
19
2. Surgical efficiency: Median surgical time decreased from 150 minutes in the first decade to 69 minutes in the second, with similar average levels treated. Retractor time, although not recorded, likely followed the same trend. This reduction may explain the lower neurologic morbidity and is 1 reason we have moved away from direct neuromonitoring in routine cases. Limiting table break, especially at levels above L4/5, has also proven effective and aligns with findings from other centers.
31
Limitations
This study has certain limitations, which must be acknowledged. As a retrospective analysis, it is subject to potential selection and reporting biases despite standardized data collection. Motor strength was assessed by clinicians, introducing possible interobserver variability, and formal inter-rater reliability metrics were not available. Sensory deficits and reflexes were not systematically documented and were thus not included in our analysis. Because sensory findings are inconsistently assessed in routine postoperative examinations and are generally less clinically meaningful than motor deficits, their inclusion would have introduced substantial variability and reduced the reliability of the dataset. Long-term outcomes such as fusion status and functional scores were not evaluated, and patient-reported outcomes were not systematically collected during the study period, limiting our ability to correlate neurologic findings with long-term functional recovery or quality-of-life measures. Other perioperative and long-term complications, including vascular, visceral, sympathetic chain, infectious, and hardware-related events, were not analyzed, and therefore broader safety profiling of standalone LLIF surgery was beyond the scope of this study. Additionally, all procedures were performed by highly experienced surgeons, potentially limiting generalizability to surgeons earlier in their learning curve. Because the study was conducted at a single high-volume academic center with consistent technique and considerable surgeon experience, the results may not fully reflect outcomes in centers with different workflows, case mixes, or levels of technical familiarity with the lateral approach. This concentration of experience likely contributed to the low rates of persistent deficits reported here, and institutional practice patterns may also affect applicability elsewhere. For these reasons, validation through prospective multicenter studies that include surgeons with varied experience and diverse practice environments is needed to confirm the generalizability of our findings, and causal inference regarding the effect of surgical era or evolving practice patterns was not the objective of this study. Prospective multicenter studies with longer follow-up and patient-reported outcomes are warranted.
Conclusions
The incidence of approach-related motor deficits after standalone LLIF has become low, with nearly all deficits resolving within 1 year. Although L4/5 surgery and prolonged operative time remain risk factors for transient weakness, LLIF, including at L4/5, remains a safe and effective option in appropriately selected patients.
Supplemental Material
Supplemental Material - Lateral Lumbar Interbody Fusion: An Update on Motor Deficits in 1000 Patients Across Two Decades
Supplemental Material for Lateral Lumbar Interbody Fusion: An Update on Motor Deficits in 1000 Patients Across Two Decades by Marco D. Burkhard, Charlotte Jones, Simon Ortiz, Torben Stepan, Bryce Demopoulos, Bruno Verna, Ali E. Guven, Anna-Maria Mielke, Jennifer Shue, Federico P. Girardi, Frank P. Cammisa, Andrew A. Sama, Alexander P. Hughes in Global Spine Journal
Footnotes
ORCID iDs
Ethical Considerations
The hospital’s institutional review board (IRB) approved the conduct of the study (#2022-0108).
Consent to Participate
Written and informed consent to participate in this study and to publish their data was obtained from all individual participants included in the study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Marco D. Burkhard, Charlotte Jones, Simon Ortiz, Torben Stepan and Bryce Demopoulos. The first draft of the manuscript was written by Marco D. Burkhard and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FPG reports royalties from Lanx and Ortho Development; ownership interest in Centinel Spine and BICMD; consulting fees from Lanx, Ortho Development, and SeaSpine; and stock ownership in Centinel Spine and Healthpoint Capital Partners LP. FPC reports research support from Camber Spine, Centinel Spine, Choice Spine, DePuy Synthes, and Royal Biologic; ownership interest in 4WEB Medical/4WEB, Healthpoint Capital Partners LP, ISPH II, ISPB III Holdings, VBVP VI LLC, VBVP X LLC, Medical Device Partners II and III, Orthobond Corporation, Spine Biopharma, Tissue Differentiation Intelligence, and Tissue Connect Systems. AAS reports royalties from Ortho Development, DePuy Spine Products/Medical Device Business Services, and Clariance; private investments in Vestia Ventures, MiRUS Investment, ISPH II, ISPH 3, and Centinel Spine (Vbros Venture Partners V); consulting fees from DePuy Spine Products/Medical Device Business Services, Clariance, and Kuros Biosciences AG; and research support from Spinal Kinetics/Orthofix. APH reports research support from Kuros Biosciences AG and Expanding Innovations; private investments in Tissue Connect Systems; and fellowship support from NuVasive and ATec. For the remaining authors, no conflicts of interest were declared.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.