
Abstract
Study Design:
Prospective cohort study.
Objectives:
To assess rate and degree of interbody bone fusion and evolution in Oswestry Disability index (ODI) and visual analog scale (VAS) of pain after minimally invasive far lateral lumbar interbody fusion.
Methods:
Twenty-three patients with single-level lumbar instability or degenerative disc were treated by this method and prospectively included. VAS of pain and ODI were evaluated preoperatively and at last follow-up. Computed tomography scan was performed 6 months after surgery to assess interbody fusion.
Results:
Between preoperative and 2 years postoperative follow-up, mean VAS decreased by 2.4 points (P < .001); mean ODI improved by 21.8% (P < .001). Computed tomography scan showed fusion in all patients but one. No severe complications were observed.
Conclusions:
Minimally invasive far lateral lumbar interbody fusion resulted in satisfactory clinical and radiological results.
Keywords
Introduction
Interbody fusion is frequently aimed in the treatment of lumbar spinal degenerative disorders. It is typically accomplished by either an anterior, lateral, or posterior approach to the intervertebral disc. Advantages of the interbody technique for fusion include availability of the large bony surface for fusion and ability to improve lumbar lordosis and neural foraminal height by disc space distraction. 1 Many complications of interbody fusion surgery are associated with the surgical approach to the disc space. 2 –7
The intertransverse approach, initially described by Wiltse and colleagues 8,9 for spondylolisthesis and usually performed for the treatment of far lateral lumbar disc herniation, 10 permits exposure of intervertebral disc laterally to the neural foramen, 11,12 and ventrally to the transverse processes without violation of either the abdominal cavity or the spinal canal. The current interest to this approach is related to wide diffusion of minimally invasive (MI) surgical techniques. In fact, open posterior approach needs muscle stripping and retraction, potentially affecting patient outcomes. 13,14 In contrast, MI lumbar fusion is performed via a muscle-dilating approach, diminishing the amount of iatrogenic soft-tissue injury. 15 –18 As a result, MI far lateral lumbar interbody fusion (FLLIF) also known as extraforaminal lumbar interbody fusion (ELIF), has shown the potential to reduce rate of complications, blood loss, postoperative pain, and duration of hospital stays. 18,19 This kind of approach is indicated in selected lumbar diseases requiring interbody fusion without spinal canal decompression. In literature, few reports are dedicated to this technique and no prospective studies. The aim of this study was to evaluate, in a prospective series, both clinical and radiologic efficacy of lumbar interbody fusion by minimally invasive intertransverse process approach.
Methods
This research followed the principles of the Declaration of Helsinki. All procedures and follow-up were approved by the institutional review board according to the standardized Reference Method 003, and the approval number is 2017728 v 0. All patients provided their verbal consent to the use of their clinical and radiological data and acknowledged that they cannot be identified as all data was fully anonymized.
We prospectively included all patients with symptomatic lumbar degenerative disc disease, spondylolysis, or low-grade spondylolisthesis (Figure 1a and b) treated with one-level interbody fusion via MI paraspinal approach to the lumbar spine in one institution (Figure 2a and b).
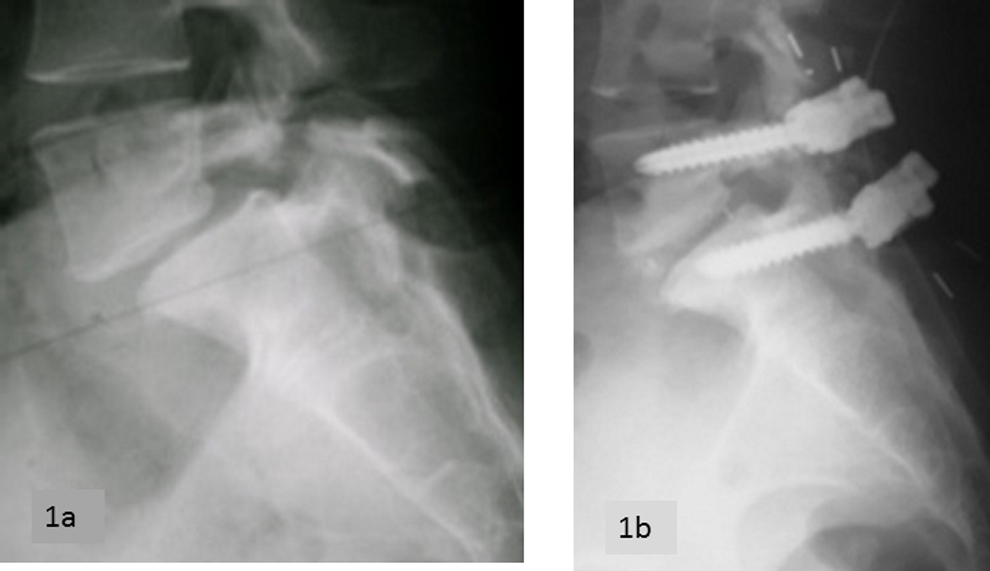
(a) Preoperative lateral view of low-grade L5-S1 spondylolisthesis. (b) Postoperative lateral view showing pedicular screws, PEEK (polyethetetherketone) rods, interbody cage, and reduction of L5 olisthesis.

Fluoroscopy scans on anteroposterior (a) and lateral (b) views. PEEK (poluetheretherketone) rods and cage are radiologically transparent and identified by lines. (c) Computed tomography scan shows many bony bridges between vertebral endplates indicating achieved fusion.
Degenerative disc disease was diagnosed with magnetic resonance imaging (MRI) according to common literature. 20 Spondylolysis and spondylolisthesis were diagnosed on X-ray or computed tomography (CT) scan. 21 Preoperative MRI was performed in all cases.
All patients presented with mechanical back pain and/or radicular pain (Table 1), refractory to at least 12 months of conservative management (analgesic, physiotherapy, and brace).
Patients Data.
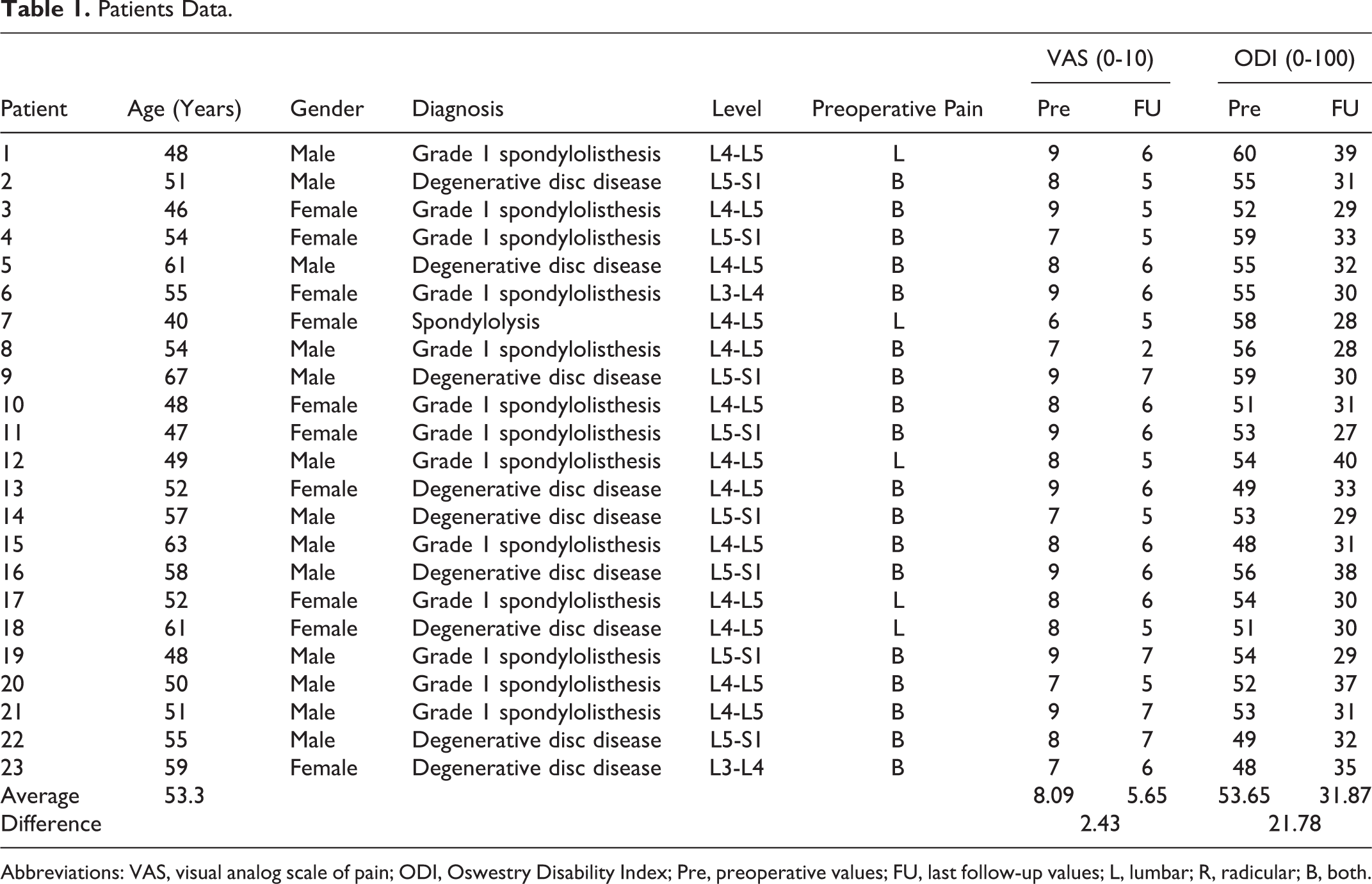
Abbreviations: VAS, visual analog scale of pain; ODI, Oswestry Disability Index; Pre, preoperative values; FU, last follow-up values; L, lumbar; R, radicular; B, both.
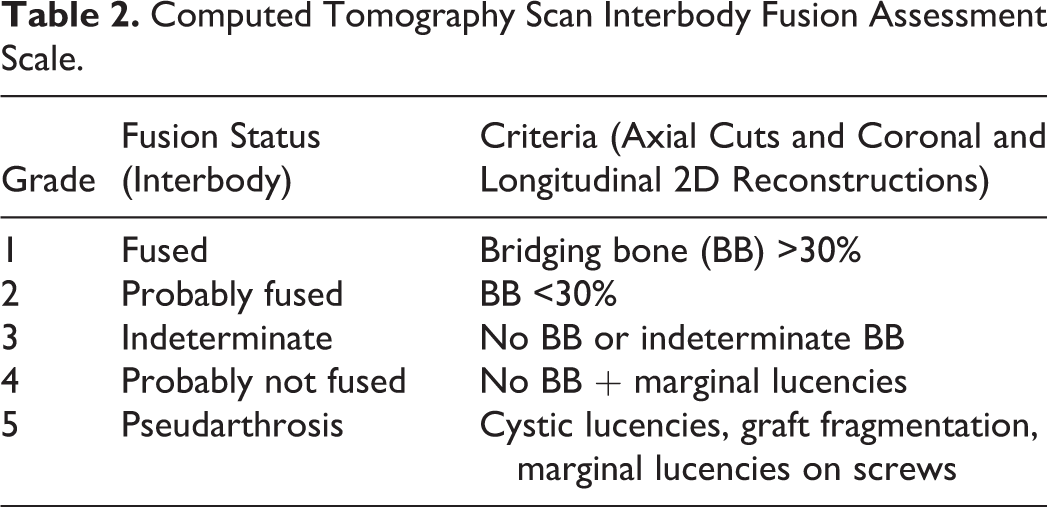
The following data was recorded: demographics, level, diagnosis (Table 1) operative time, blood loss, length of hospital stay, and complications. We also reported preoperative and last follow-up evaluations by the Oswestry Disability Index (ODI) and the visual analog scale (VAS; 0-10 points) for pain. All patients were clinically scheduled for follow-up postoperatively at 12 weeks, 24 weeks, 1 year, and 2 years. Six months after surgery, all patients underwent CT scan with 2-dimensional coronal and sagittal reconstructions, for evaluation of fusion by an independent radiologist. Qualitative criteria were used for fusion assessment by CT scan as detailed in Table 2. 22 Endplate to endplate bridging bone surface ≥30% was required to consider the interbody fusion to be achieved (Figure 2c).
Computed Tomography Scan Interbody Fusion Assessment Scale.
The surgical procedure consisted of placing patients in the prone decubitus position, performing fluoroscopic localization of the affected level, and performing a posterior 5- to 7-cm skin incision approximately 10 cm lateral to the midline. Paraspinous thoracodorsal fascia was incised to expose the sacrospinalis muscle groups. The multifidus and longissimus muscles were separated with blunt dissection. Once an arm was mounted, MAST quadrant expandable retractor (Medtronic Sofamor Danek, Memphis, TN, USA) was placed and the appropriate transverse processes were cleared of soft tissue. The intertransverse membrane was opened with blunt dissection. The pedicle and neural foramen were palpated from outside the spinal canal to aid location of the extraforaminal nerve root. The latter, identified at the issue from the neural foramen, was mobilized laterally and proximally in the intertransverse space by gentle blunt dissection (Figure 1). After bipolar hemostasis, subtotal discectomy was performed from the lateral aspect of the disc across the midline to the contralateral annulus, while preserving the anterior and posterior longitudinal ligaments. Cartilage was removed from endplates. The interbody cage made from polyetheretherketone (PEEK) and filled with tricalcium phosphate and hydroxyapatite was placed from the same lateral approach. The interbody cage (OPAL, Synthes, Oberdorf, Switzerland) measured 10 mm wide, 7 to 17 mm in height, and 28 to 32 mm in length (Figures 1b and 2b). Through the expandable retractor, the fusion was augmented with ipsilateral intertransverse graft positioning after removal of cortical bone from transversal processes. Ipsilateral pedicle screws and PEEK rod were implanted by the same approach while contralateral were implanted percutaneously (Figures 1b and 2a and b). Sextant reduction system (Medtronic Sofamor Danek, Memphis, TN, USA) was used in all patients to increase lordosis. All procedures were monitored with perioperative electromyogram.
Statistical Analysis
A P value <.05 was considered significant. Analysis of categorical variables was performed through Fisher’s exact test. Comparisons between quantitative parameters were performed by t test after assessment of normal distribution and homoscedasticity.
Results
No patient was lost to follow-up. The mean operative time from induction to extubation was 108 minutes (range 80-140 minutes). The mean total blood loss was 180 mL (range 80-300 mL). The average duration of stay in the hospital was 6.2 days (range 5-10 days). Mean follow-up was 26 months (range 24-36 months). No patient required blood transfusion. There were no cerebrospinal fluid leaks, wound infections, general complications, or postoperative weaknesses identified. Three patients (13%) experienced transient postoperative sciatic pain ipsilateral to approach side, spontaneously recovering within 3 months.
Preoperative diagnosis or site of pain did not influence clinical outcome or fusion (P > 0.1).
Both VAS and ODI were improved in all patients at 24 months. Mean improvement of 2.4 points in VAS scores (P < .001) and 21.8% in the ODI was observed (P < .001). Fusion was classified through CT scan as grade 1 in 17 patients and as grade 2 in 5 patients (Figure 2). One patient did not present evidence of fusion (grade 3) but was clinically improved, not requiring further surgery.
Discussion
Our results show high rate of fusion and clinical improvement in all patients, better than published data for other techniques of lumbar fusion. 5,6
The strengths of this study are prospective inclusion, complete follow-up, and radiologic evaluation by an independent radiologist through CT scan, which is the “gold standard” for fusion assessment. The main limitations are lack of comparative series and the small sample size.
In our opinion, the best indications for MI FLLIF are symptomatic low-grade spondylolisthesis or degenerative disc disease. High-grade spondylolistheses are technically challenging and are optimally treated via an open approach. In case of unilateral severe foraminal compression, direct decompression is possible through the same approach. On the other hand, in case of bilateral mild compression, FLLIF is efficient since contralateral decompression can be indirectly achieved by foraminal height restoring. In patients with severe contralateral lateral recess stenosis, a contralateral minimally invasive decompression can be performed through a separate incision using a tubular retractor.
Concerning technical aspects, in case of close anatomic relationship between the ala of the sacrum and the L5 transverse process, adequate exposure of the extraforaminal portion of L5-S1 intervertebral disc is hard, needing removal of the transverse process of L5 or an alternative approach to the disc.
The use of electromyogram neuromonitoring seemed useful to avoid severe complications related to injury of nerve roots in the extraforaminal area, although we reported some cases of transient radicular pain.
In our series, the average duration of stay in the hospital was long for a minimally invasive procedure because we used the same protocols as for “traditional” lumbar fusion surgery, for example, posterior lumbar interbody fusion and we are currently shortening the durations.
Our fusion rate was very high, whereas published fusion rate with PEEK implants is varied ranging from 60% (Mavrogenis et al 23 ) to 100% (Qi et al 24 ) for constructs with screws, rods, and cages. We do not have a formal explanation, but we think that careful discectomy, endplate preparation, and intertransverse grafting are very influential. Comparison with published data for other techniques of one-level lumbar fusion shows similar outcomes. 25
Finally, as with all novel techniques, there is a learning curve that must be overcome with experience and repetition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.S. received grants from Medicrea Int (outside this work). M.B. received grants from Nuvasive and K2M (outside this work).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.