
Abstract
Oblique lateral interbody fusion (OLIF) is a minimally invasive spinal surgery that is popular for lumbar degeneration and spinal deformity treatment because it causes minimal damage to the stability of the intervertebral structures. However, when encountering abnormal anatomical structures caused by situs inversus, surgical routes must be adjusted to avoid serious complications. A 42-year-old woman with lumbar spinal stenosis presented to our hospital. Preoperative X-ray and computed tomography indicated situs inversus totalis, with the abdominal aorta and inferior vena cava reversed. We established an appropriate surgical approach for OLIF via the right abdomen according to the characteristics of the anatomical structures. Postoperative X-rays showed adequate positioning of the interbody fusion cage and internal fixation screws. At the 3-month follow-up, the patient reported resolution of her symptoms. Vascular variations caused by situs inversus totalis can affect the course of OLIF. Understanding the unique anatomical structure in such patients is crucial for successful surgery and to avoid intraoperative complications.
Keywords
Background
Oblique lateral interbody fusion (OLIF) has attracted increasing attention in the field of minimally invasive spinal surgery and has become a popular procedure. In OLIF, the natural gap between the posterior peritoneal psoas major muscle and the abdominal aorta is used as a reference to establish a surgical approach, which reduces the risk of damage to the psoas major muscle and nerve roots of the lumbar plexus. Unlike posterior surgery on the paravertebral muscles and lumbar spine, OLIF cannot damage the facet joints.1–3 Anatomically, the inferior vena cava is usually located on the right side of the abdominal aorta. Therefore, patients undergoing OLIF usually lie on their right side, and a surgical incision is made in the left abdomen. A right-sided approach can be considered in some cases, considering the concave side of scoliosis or the surgeon’s preference. Situs inversus totalis (SIT) refers to the translocation of all organs in the chest and abdomen, from their normal position. A SIT patient is referred to as a “mirror person”. We report a case of lumbar spinal stenosis in a patient with total visceral reversal who underwent OLIF in the left lateral position. Our case report complied with the CARE guidelines. 4
Case presentation
A 42-year-old woman had a history of low back pain for at least 5 years. As there was no significant impact on her life and work, she relied on bed rest or massage therapy and physiotherapy to relieve her symptoms. However, in the past year, the lower back pain had gradually worsened, and she developed pain with numbness and intermittent claudication of the lower limbs, mainly in the lateral thighs, posterolateral lower legs, and the tops of her feet. Chest X-ray indicated dextrocardia (Figure 1), and lumbar X-ray showed a straightened lumbar spine curvature and lumbar spine instability (Figure 2). Lumbar computed tomography (CT) indicated L4–L5 disc degeneration with spinal stenosis (Figure 3), and abdominal CT indicated no other abnormalities except SIT. Physical examination revealed obvious tenderness on both sides of the lumbosacral spinous processes and paraspinal muscles, weakness of bilateral extensor digitorum longus muscles (muscle strength: level 3 for the left side and 4 for the right side), and positive straight leg raising test in both lower limbs (60°). The patient tried oral analgesics and epidural steroid injections at another hospital with no benefit; the details of this treatment were unknown. She then decided to undergo surgical treatment. According to the patient’s conditions, a surgical plan for OLIF combined with percutaneous posterior pedicle screw internal fixation was scheduled. Considering the presence of SIT and that the inferior vena cava was located on the left side of the abdominal aorta, a surgical approach via the right abdomen was chosen. The sizes of the different operative windows were: 1.25 cm for the vascular window, 1.00 cm for the bare window, 1.48 cm for the psoas major window, and 2.48 cm for the actual operative window (Figure 4), ensuring a large operating space. The operation was successful, and there were no intraoperative complications.

Chest X-ray demonstrating dextrocardia.

Lateral X-ray of the lumbar spine showing that the lumbar lordosis angle (a) is 31°, and the sagittal rotation angle between b and c is changed by more than 10° in the hyperextension and hyperflexion positions, indicating L4–L5 instability.

Preoperative axial computed tomography (CT) image of L4–L5 showing spinal stenosis, and that the inferior vena cava is located on the left side of the abdominal aorta.

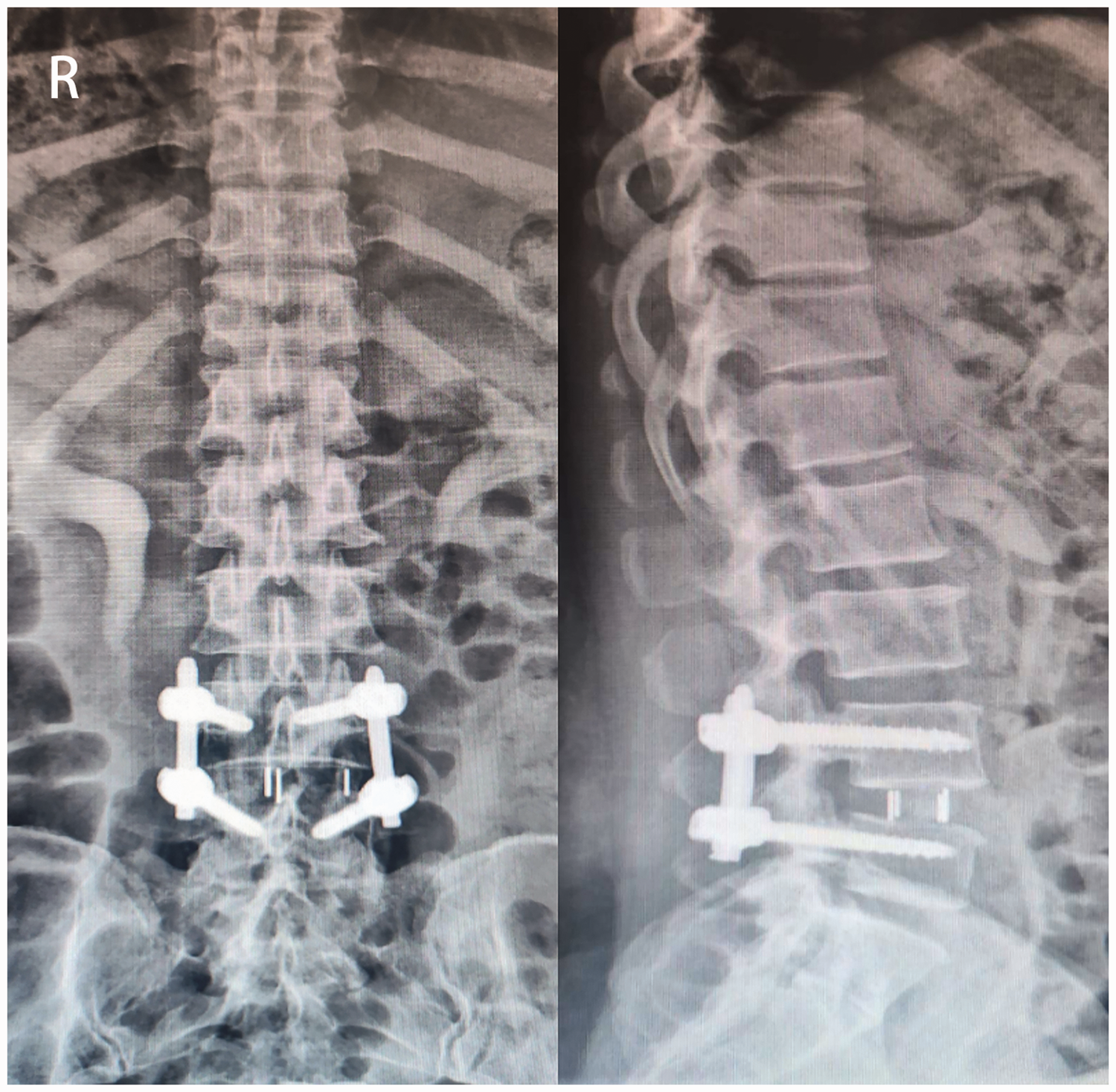
Anteroposterior and lateral X-rays of the lumbar spine 3 days after the operation.
On the second day after surgery, lower back pain and lower limb pain with numbness were significantly relieved, without complications. Postoperative X-rays showed that the interbody fusion cage and internal fixation screws were well-positioned (Figure 5). Three months after the operation, the patient had recovered well, and the preoperative symptoms were completely relieved.
Axial computed tomography (CT) image of L4–L5 AA: abdominal aorta; IVC: inferior vena cava; PM: psoas major muscle; O: approximate elliptical center of the intervertebral space; AB: vascular window; BC: bare window; CD: psoas major window. The ideal operative window =vascular window (AB) + bare window (BC) + psoas major window (CD), while the actual operative window = bare window (BC) + psoas major window (CD).
Discussion
Situs inversus is a rare congenital malformation that comprises SIT and situs inversus partialis, and there is no understanding of its specific mechanism. Studies have shown that situs inversus may be related to chromosomal function defects or ciliary motility disorders during embryonic development.5,6 Patients with situs inversus generally show no distinguishing characteristic related to organ function except that their visceral organs are arranged in a mirror image of the normal positions. Most people with SIT have no medical symptoms and generally display no significant pathophysiological issues. The patient reported in this study presented with SIT. Lumbar spinal stenosis combined with SIT is rare. Although SIT is not a contraindication to surgical treatment, it can be associated with splenic abnormalities or other mutations, among which vascular malformations are most likely.7,8 When surgical treatment is scheduled for patients with SIT, relevant radiological examinations are required. It is best to determine whether there are related anatomical variations before performing invasive procedures.
OLIF can shrink the posterior ligamentous complex by increasing the height of the intervertebral space and facilitating indirect decompression of the spinal canal. At the same time, OLIF can reconfigure the vertebral body sequence to enhance stability. This procedure possesses advantages that are characteristic of minimally invasive surgery, while achieving the same curative effect as traditional posterior surgery. We endeavored to maintain the integrity of the posterior spinal structures as much as possible, in the current patient, with the goal of effectively relieving her pain. Our patient met the indications for surgery, and OLIF was considered a good treatment plan. OLIF neither invades the spinal canal nor does it need to pass through the psoas major muscle. Compared with posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, and extreme lateral interbody fusion, OLIF has the advantages of less overall damage, bleeding, and nerve damage rates, and faster postoperative recovery. 3 OLIF’s surgical route is through the natural gap between the psoas major muscle and the retroperitoneal blood vessels, which can be exposed by bluntly separating the external and internal oblique muscles, transversus abdominis, and transverse fascia, and by exposing and retracting the psoas major muscle. A guide needle is inserted into the target vertebral gap, which is then expanded step-wise to allow access to the target region. According to CT imaging data, Liu et al. 9 divided the OLIF operative windows into vascular, bare, psoas major, ideal operative, and actual operative windows. The vascular window should be avoided when establishing the surgical procedure, and attention should be paid to the position of the abdominal aorta and inferior vena cava, as well as to the presence of lumbar segmental arteries on the posterior lateral vertebral body. 10 Preoperative preparations comprise fully understanding the width of the gap between the psoas major muscle and the large blood vessels in the abdominal cavity, and estimating the actual size of the operative window. The psoas major muscle should not be excessively stretched, otherwise there may be damage to the lumbar plexus nerve root. OLIF should be performed with care in patients with large vascular malformations or particularly narrow gaps between the psoas major muscle and abdominal large vessels. If the evaluation shows that the operative window is not suitable for OLIF, other treatment options, such as extreme lateral interbody fusion or traditional posterior decompression and fixation can be considered.
The abdominal aorta is most often located in front of the vertebral body, slightly to the left, and the inferior vena cava is located close to the right side of the abdominal aorta. In the current patient, CT images showed that the abdominal aorta was positioned slightly to the right and in front of the vertebral body, and the inferior vena cava was on the left, representing a mirror image of the normal positions. The sizes of the different operative windows were appropriate (Figure 4) and ensured a large operating space.
Operating via the right abdomen was successful in this case; however, the long-term postoperative curative effect must be evaluated by analyzing follow-up data. Congenital anatomical variants have the potential to significantly change the anatomy of the blood vessels. Both Berry 11 and Liu et al. 12 reported cases in which the inferior vena cava was located on the left side of the abdominal aorta owing to congenital vascular anatomical variations, and OLIF was successfully performed via the right abdomen. MRI and CT can reveal the trajectory of the great abdominal blood vessels and their anatomical relationships. To avoid intraoperative complications for SIT patients, surgeons should overcome the disorientation caused by the reversal from normal anatomical positions and carefully plan the surgical route before surgery.
Our study emphasizes the importance of accurate diagnosis and preoperative evaluation of anatomical structures. Under normal conditions, selecting an appropriate surgical window for OLIF can avoid most postoperative complications. When encountering abnormalities in blood vessels or organ anatomy, surgeons must accurately assess the anatomical structure according to imaging data and adjust the surgical strategy accordingly.
Footnotes
Authors' contributions
All authors contributed to the study conception and design. FengKai Yang, ChenTao Dou and XiaoKang Cheng prepared the materials and collected the data. The first draft of the manuscript was written by FengKai Yang. FengKai Yang and Bin Chen revised the manuscript. All authors read the manuscript critically to improve the intellectual content. All authors read and approved the final manuscript.
Availability of data and materials
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval
This research was approved by the ethics committee of Chengde Medical University Affiliated Hospital.
Written informed consent was obtained from the patient to undergo treatment and to publish this report.
Funding
This research was supported by the Department of Health of Hebei Province (20150019).