
Abstract
Design
Post-hoc analysis of data from prospective multicenter observational study.
Objectives
Adult spinal deformity (ASD) can have significant impact on various aspects of a patient’s social life. This study aims to examine the impact of ASD surgery on the social functioning among elderly patients.
Methods
Patients ≥60 years undergoing ≥5 levels of spinal fusion from 12 international centers were enrolled and followed up 2 years post-operatively. The outcome measures of interest in the current report were questions 14 and 18 of the Scoliosis Research Society-22r questionnaire (SRS-22r), and question 9 from the Oswestry Disability Index (ODI).
Results
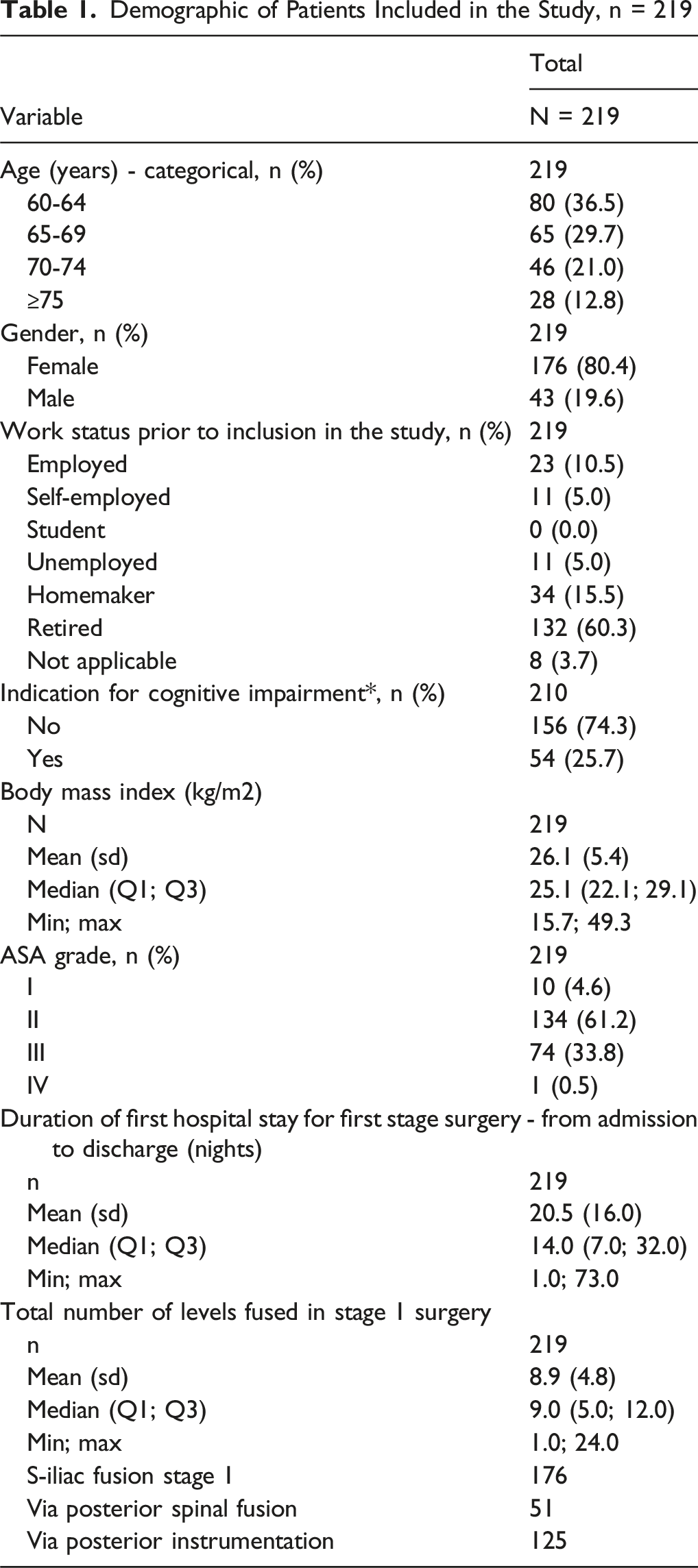
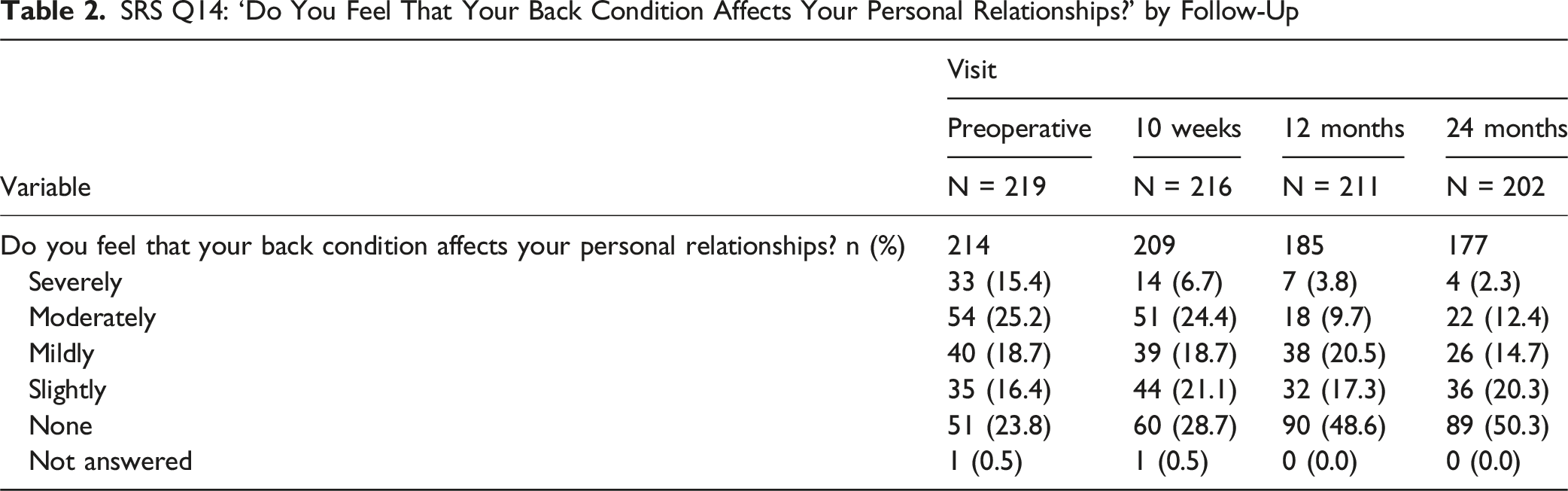
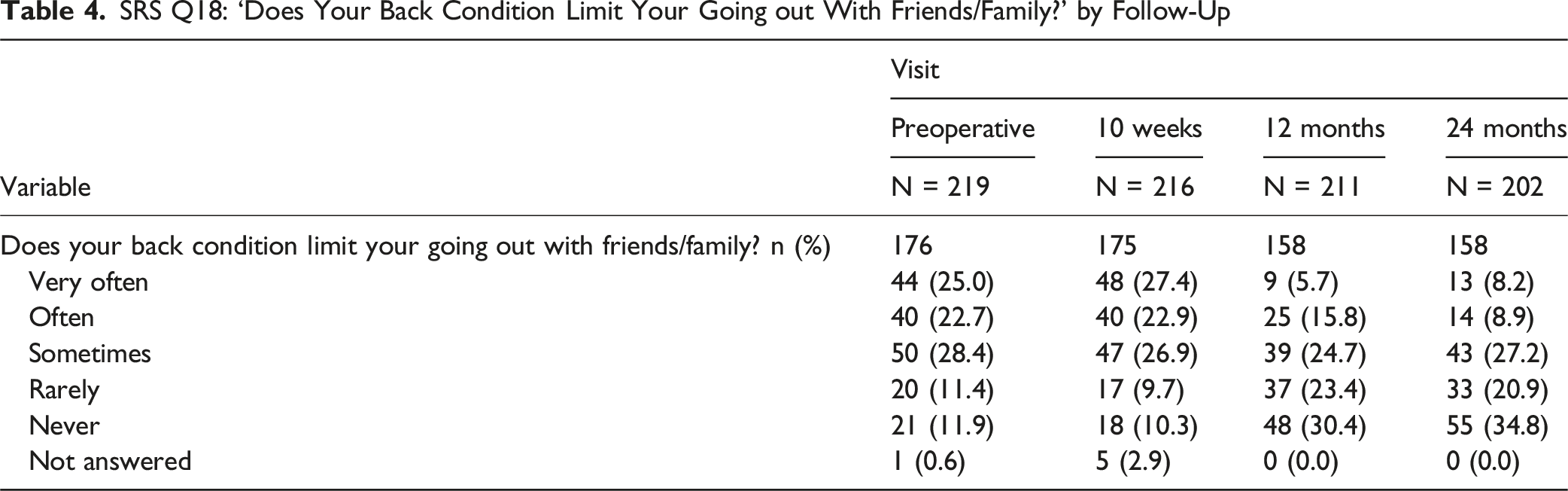
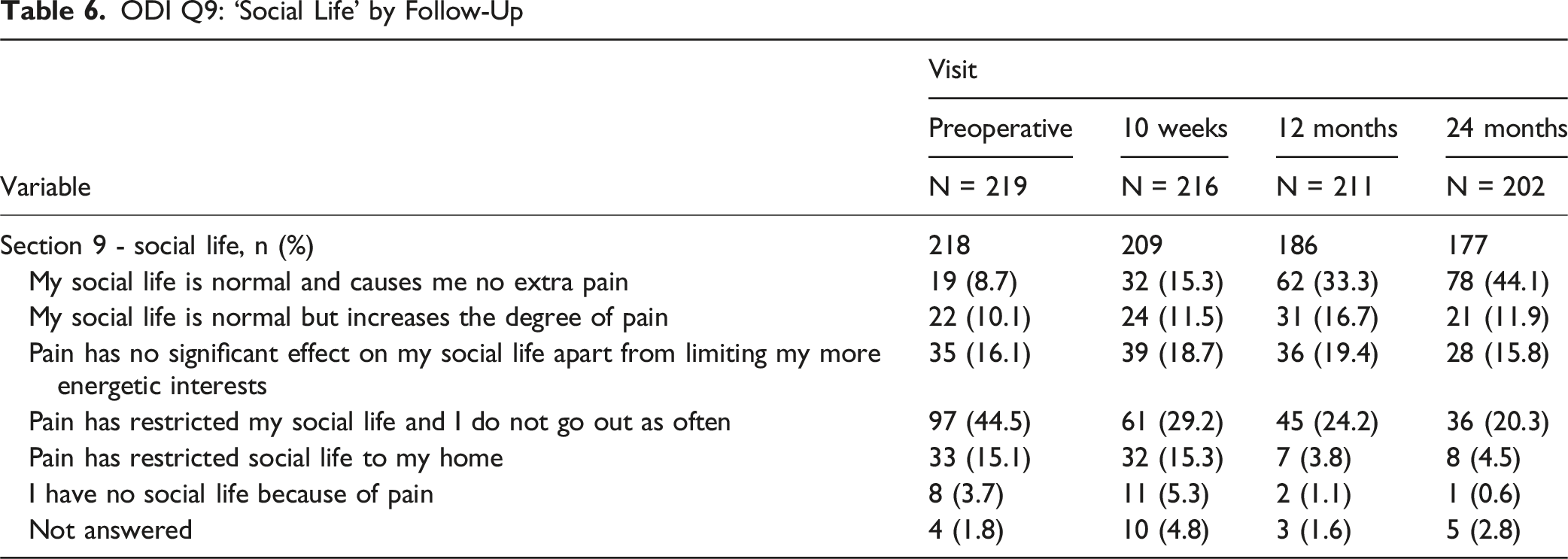
219 patients met the inclusion criteria, with a median age of 67.5 and 80.4% being female. More than a third were employed or homemakers, 60.3% were retired and 25.7% showed cognitive impairment. For the SRS-22r Q14, at baseline, 40.6% of patients felt their back condition moderately or severely affected their personal relationships compared to 14.7% at 2-years. For SRS-22r Q18, at baseline, 47.7% of patients felt their back often or very often limited them going out with friends/family compared to 17.1% at 2-years. For the ODI, Q9, 8.7% of patients felt that their social was normal and does not cause them extra pain pre-op compared to 44.1% of patients at 2-years.
Conclusion
While many factors can affect a patient’s social function, in this cohort ASD surgery had a positive impact on social function.
The ClinicalTrails.gov identifier: NCT02035280.
Keywords
Introduction
Adult spinal deformity (ASD) is a common problem affecting up to 68% of the elderly population.1-3 As our population ages, these numbers will continuously increase. Symptoms arising from ASD include low back pain and/or radicular leg pain with or without neural deficit, which limits the patient’s ability to walk, stand upright and perform daily activities. These functional limitations cause a severe decrease in health-related quality of life, comparable to other chronic disease states such as arthritis, chronic pulmonary disease, congestive heart failure, diabetes and cancer.4,5 Surgical treatment has shown to improve quality of life in ASD patients who have failed to improve with non-operative treatment.3,6,7
Social functioning has been recognized as a domain of health-related quality of life, focusing on difficulties with participation in social activities and relationships. 8 Social well-being involves factors such as education, employment, lack of financial burden, good interpersonal relationships and supportive care. ASD may impair social interactions not only through functional limitations, but also through poor body self-image and social stigma.9,10 This may lead to social isolation, which is correlated with increased morbidity and mortality.11,12 This effect is more pronounced in the elderly, due to the increased prevalence of chronic illnesses and already limited social connectedness.
While there is significant research on outcomes of ASD surgeries regarding the domains of pain, function and mental health, there is limited granular data on the effects of ASD and its treatment in social functioning in the elderly. This study aims to examine social functioning before and after ASD surgery among a cohort of surgical patients 60 years of age or older. We hypothesized to observe an improvement in social functioning as compared with baseline status in patients undergoing ASD surgery, based on changes in scores for social-function related questions from Scoliosis Research Society questionnaire (SRS-22r) and Oswestry Disability Index (ODI).
Methods
This is a post hoc analysis of data from a prospective, multicenter, multi-continental, observational longitudinal cohort study performed on patients 60 years or older undergoing primary spinal fusion surgery of 5 or more levels for spinal deformity (PEEDS). The PEEDS study was conducted in accordance with the ethical principles set forth in the Declaration of Helsinki including amendments as well as the International Council for Harmonisation Good Clinical Practice guidelines, the European Standard EN ISO14155/2003-2011, and the laws and regulations of the individual countries in which the research was conducted. The clinicaltrails.gov identifier Is: NCT02035280.
Patients were included if they were 60 years or older at the time of the surgery, underwent 5-level or more spinal fusion procedure for a coronal, sagittal or combined deformity. Patients had to provide consent and sign for participation in the cohort. Exclusion criteria included prior spinal surgeries (except prior decompression of up to 2 levels), neurodegenerative diseases or paralysis, doubtful compliance during follow up, were institutionalized or prisoners, medically unfit, recent substance abuse, psychosocially disturbed, had an active tumor or infection, had a recent tumor or fracture of the spine or participation in other studies that could influence the results of the current study.
Demographic variables collected in this study were gender, age, height, weight, body mass index, race, work status, type of work, and American Society of Anesthesiologists grade, as well as Animal Fluency Test (AFT), as a metric for cognitive function.13,14 In this test, patients had to name as many animals as possible in 60 seconds. Fifteen or less animals are an indication of cognitive impairment. Patients were reviewed and outcome forms were completed at baseline, 10 weeks, 12 months, and 24 months. The Adverse Events (AEs) were collected prospectively throughout the study at discharge, 10 weeks, 12 months, and 24 months follow up.
SRS-22r, ODI, back and leg numerical rating scale (NRS) were answered by the patient at each time point. The SRS-22r is commonly used to assess quality of life in both adolescent and adult cohorts of patients with spinal deformity.15-17 It includes 5 domains: function, pain, self-image, mental health and satisfaction with treatment. Self-image and function domains were found to correlate with SF-36 social functioning component in adults. 18 The Oswestry Disability Score (ODI) is another specific patient-reported outcome commonly used in ASD.19,20 It comprises 10 sections, including one that focuses specifically on limitations in social life imposed by low back pain. From the social functioning standpoint, outcome measures of interest were SRS-22r questions 14 (do you feel your back condition affects your personal relationships?) and 18 (does your back condition limit your going out with friends/family?). Additionally, we focused on ODI question 9 (impact of back pain on social life).
Simple descriptive statistics were used to present mean and standard deviation or median and range for continuous data and frequency and proportions for categorical data. Shift tables were produced for SRS-22r questions 14 and 18 and ODI question 9 to display transitions between the preoperative social function and social function at 24 months. Five logistic regression models adjusted for age, gender, BMI, Charlson comorbidity score, and baseline social function were performed to evaluate high (ODI question 9 score 3-5) vs low social function (ODI question 9 score 0-2) at 24 months for 5 selected predictors (complications, AFT, SRS22-r – Function, SRS-22r – Mental Health, and SRS22r – Pain). Significance was defined as P < .05. All statistical analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC, USA).
Results
Demographic of Patients Included in the Study, n = 219
SRS Question 14: Do You Feel Your Back Condition Affects Your Personal Relationships
SRS Q14: ‘Do You Feel That Your Back Condition Affects Your Personal Relationships?’ by Follow-Up
SRS Q14: ‘Do You Feel That Your Back Condition Affects Your Personal Relationships?’ Baseline vs 24 Months
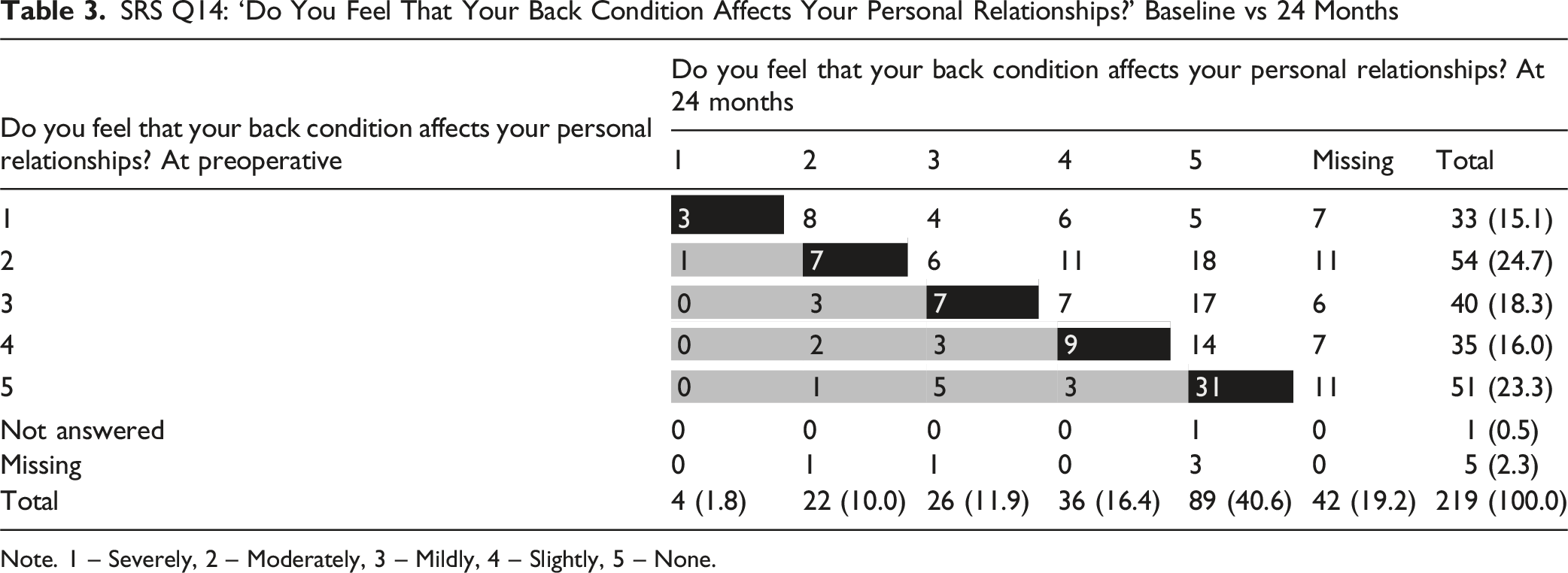
Note. 1 – Severely, 2 – Moderately, 3 – Mildly, 4 – Slightly, 5 – None.
SRS Question 18: ‘Does Your Back Condition Limit Your Going Out With Friends/Family
SRS Q18: ‘Does Your Back Condition Limit Your Going out With Friends/Family?’ by Follow-Up
SRS Q18: ‘Does Your Back Condition Limit Your Going Out With Friends/Family?’ Baseline vs 24 Months
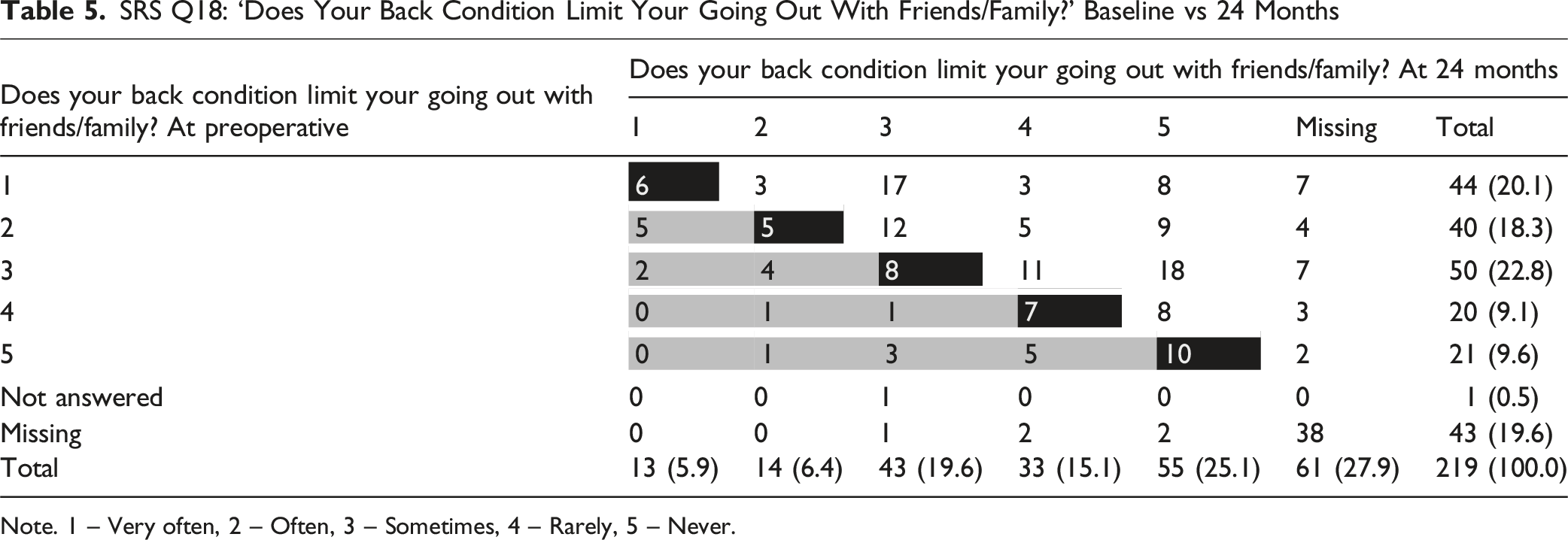
Note. 1 – Very often, 2 – Often, 3 – Sometimes, 4 – Rarely, 5 – Never.
ODI Q9, Social Life Impacted by Back Pain
ODI Q9: ‘Social Life’ by Follow-Up
ODI Q9 - Social Life Baseline vs 24 Months
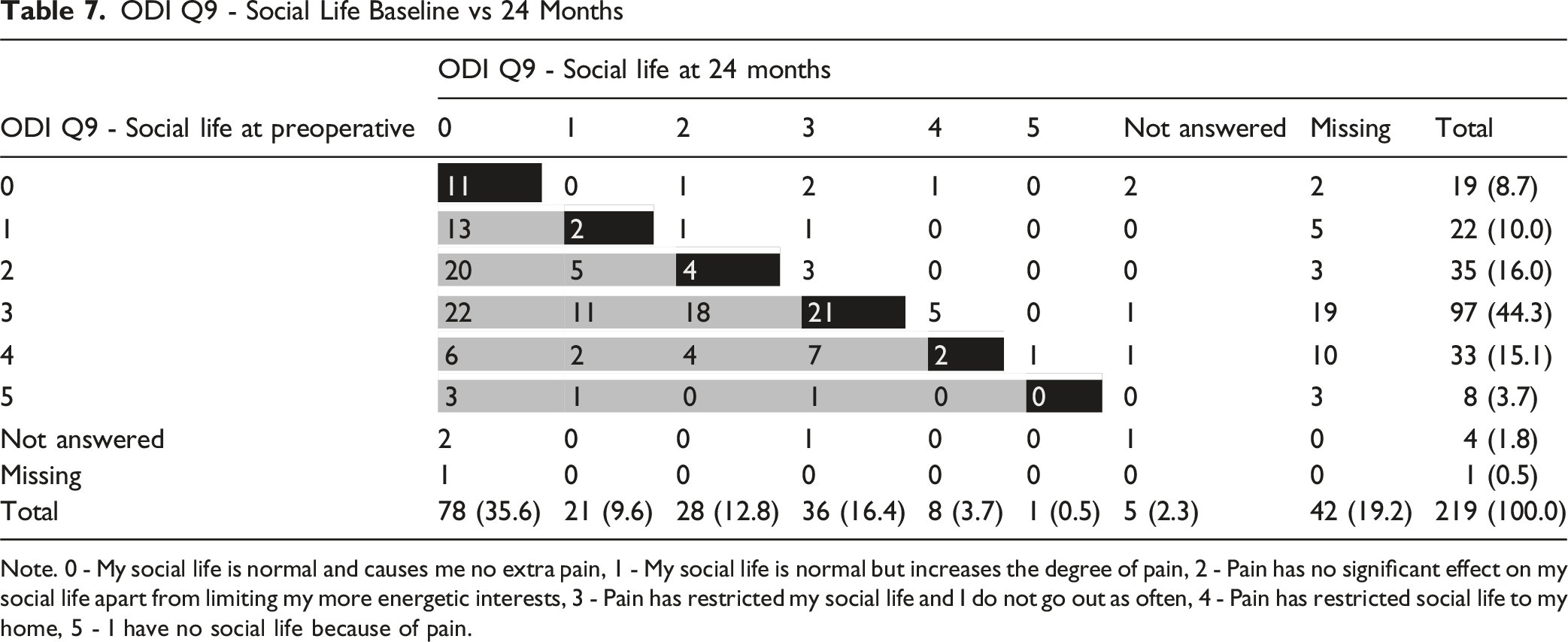
Note. 0 - My social life is normal and causes me no extra pain, 1 - My social life is normal but increases the degree of pain, 2 - Pain has no significant effect on my social life apart from limiting my more energetic interests, 3 - Pain has restricted my social life and I do not go out as often, 4 - Pain has restricted social life to my home, 5 - I have no social life because of pain.
Odds Ratios for High vs Low Social Function by Predictor at 24 Months
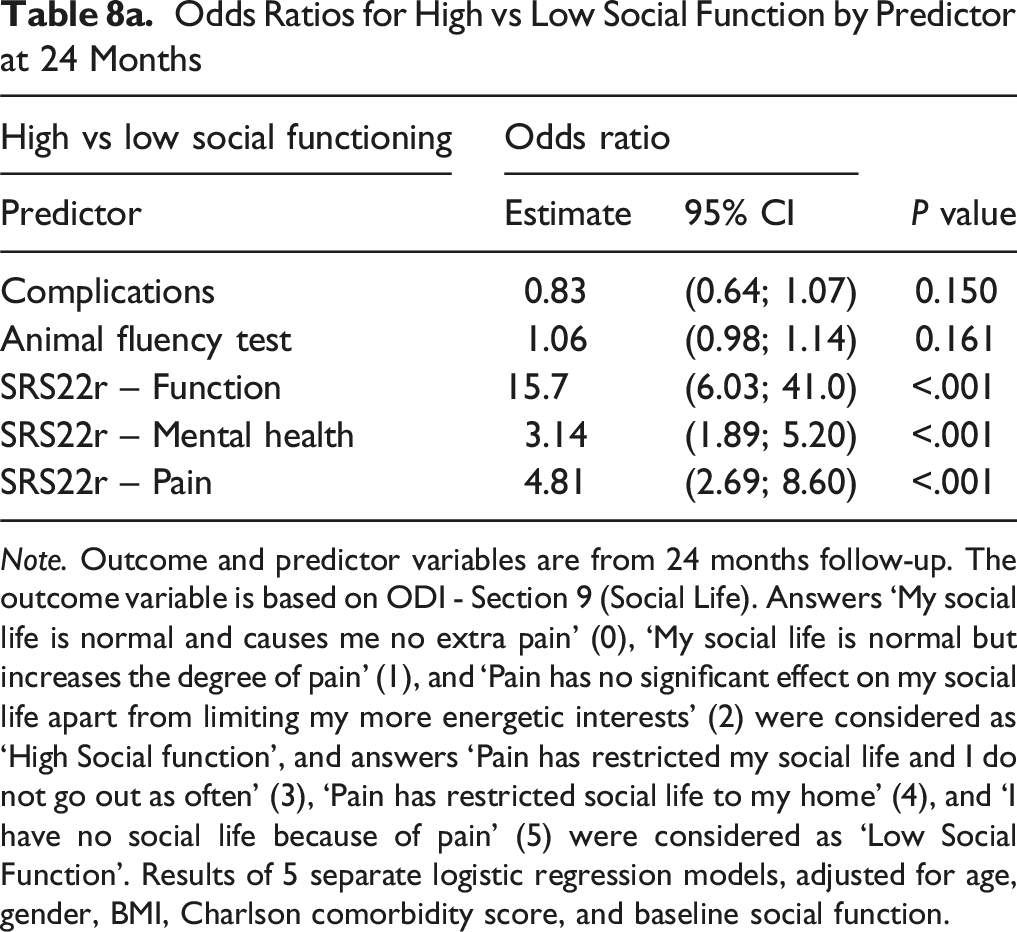
Note. Outcome and predictor variables are from 24 months follow-up. The outcome variable is based on ODI - Section 9 (Social Life). Answers ‘My social life is normal and causes me no extra pain’ (0), ‘My social life is normal but increases the degree of pain’ (1), and ‘Pain has no significant effect on my social life apart from limiting my more energetic interests’ (2) were considered as ‘High Social function’, and answers ‘Pain has restricted my social life and I do not go out as often’ (3), ‘Pain has restricted social life to my home’ (4), and ‘I have no social life because of pain’ (5) were considered as ‘Low Social Function’. Results of 5 separate logistic regression models, adjusted for age, gender, BMI, Charlson comorbidity score, and baseline social function.
Odds Ratios for High vs Low Social Function at 24 Months by Baseline Predictors
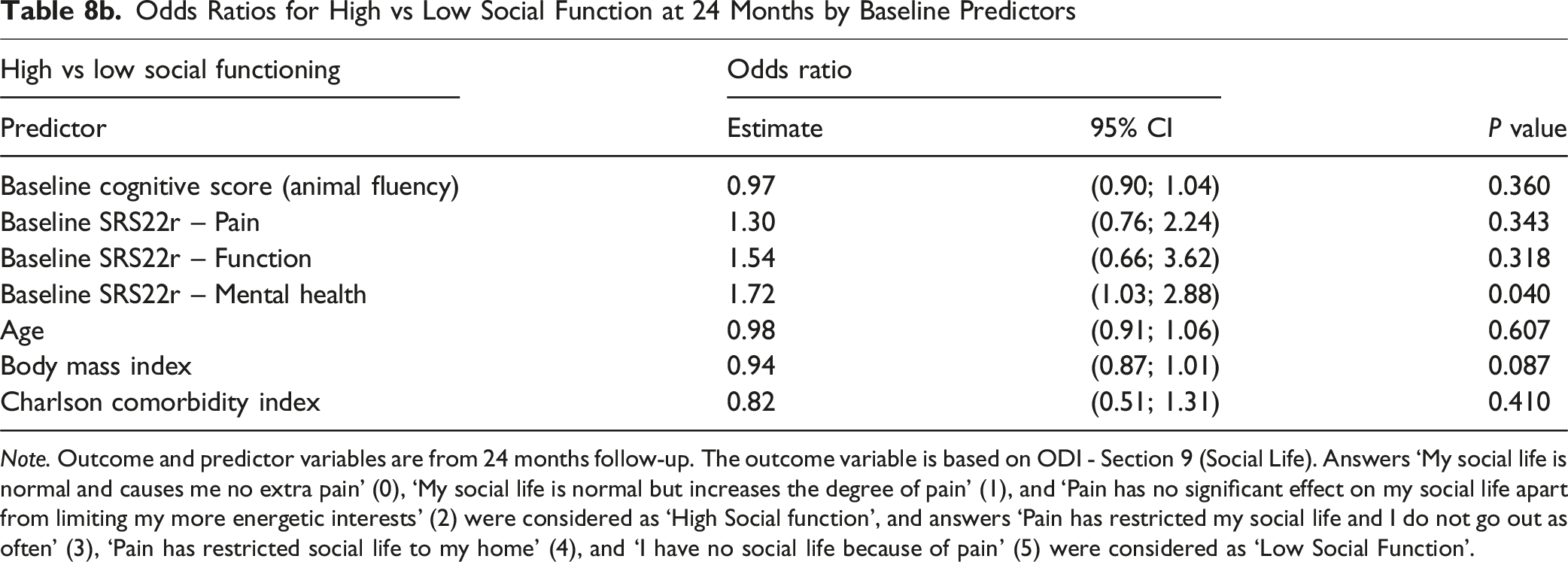
Note. Outcome and predictor variables are from 24 months follow-up. The outcome variable is based on ODI - Section 9 (Social Life). Answers ‘My social life is normal and causes me no extra pain’ (0), ‘My social life is normal but increases the degree of pain’ (1), and ‘Pain has no significant effect on my social life apart from limiting my more energetic interests’ (2) were considered as ‘High Social function’, and answers ‘Pain has restricted my social life and I do not go out as often’ (3), ‘Pain has restricted social life to my home’ (4), and ‘I have no social life because of pain’ (5) were considered as ‘Low Social Function’.
Discussion
The current study demonstrates lower degrees of social limitations secondary to ASD after surgery compared to before, in an international cohort of patients 60 years and older. These results are particularly valuable as they represent a socially vulnerable population, with over two-thirds of patients retired and a quarter showing evidence of cognitive impairment. Despite this, more than half of the patients who were severely or moderately affected in terms of personal relationships and social outings improved at 2 years postoperatively. In this cohort, only 8.7% of patients had normal pain-free social interaction preoperatively, a proportion that increased more than fivefold at 2 years after ASD surgery. Furthermore, as the cohort consists of patients from diverse regions worldwide, it has enhanced external validity, applying to a broader sociocultural context.
Although our adjusted regression models did not identify a significant association between complications and social function, this might be due to limitations in our study, which was not primarily designed to address this specific question, and/or that social function is less sensitive to the occurrence of complications. Our primary analysis of complications and patient-reported outcomes will be presented in a separate publication. Nevertheless, prior literature demonstrates a heterogeneous effect of complications on outcomes with some studies showing that patients can still achieve significant clinical improvement and satisfaction despite major complications1,2
The results of this study are important, because social functioning is a fundamental aspect of health-related quality of life that is frequently overlooked by studies, which often emphasize more biomedical outcomes. However, understanding this more personal aspect can help patients and surgeons better assess the day-to-day effects of ASD surgery and thus assist in decision-making. Additionally, it may aid the interdisciplinary team in planning and providing social support and accommodations for more challenged patients.
Social functioning is not routinely reported in ASD literature and efforts are being made to include a more granular view of it, alongside other aspects such as employment, time to recovery and challenges in daily activities. 21 Notably, a panel of international experts has reached a consensus on the importance of social functioning as a metric to individualize patient care. 22 There is also recognition that social participation is a function of environmental and cultural factors. However, these more comprehensive profiles of ASD patients await further validation and broader usage. Our study, comprising a large cohort of multi-continental ASD patients is a step forward in highlighting the social domain effects on patients treated for ASD across different cultural contexts.
It is well recognized that spinal deformity impacts psychosocial aspects of patients’ lives in both adolescents and adults.23-25 Initial studies reported on non-treated idiopathic scoliosis patients and the psychosocial impact of their condition. In a psychiatric evaluation of twenty-six women with severe curvatures, participants expressed that their lives were significantly marked by the deformity, even though they appeared superficially well-adjusted. 26 In an untreated natural history cohort of 177 late onset idiopathic scoliosis patients, the majority of patients dealt with such issues as difficulty in purchasing clothes, decreased physical capacity, and self-consciousness. 27 Danielsson et al reported on the quality of life more than 20 years after surgical or brace treatment for adolescent idiopathic scoliosis in patients in their fourth decade.28-30 Significantly more patients (34.5-48.6% vs 15%) than controls, felt their backs had limited their social activities and ability to have satisfying relationships, mostly due to difficulties with physical participation in activities, fear of injury or self-consciousness about their appearance. Pain was a minor limiting factor in this age group. Similarly, 49 ASD patients with a mean age of 63 years, had lower social functioning component scores on the SF-36, compared with young general population, general population age 55-64 years and population with co-morbid conditions. 31 Loss of lumbar lordosis was associated with lower social functioning, role emotional and general health components of SF-36. However, in a cohort of 75 asymptomatic volunteers older than 60 years, although a high prevalence of ASD was found, this was not associated with lower SF-36 scores compared with age norms, excepting for the vitality component in a subgroup with curves between 10-20° of Cobb angle. 32 Most of these reports included younger cohorts, untreated patients and patients treated surgically with non-modern instrumentation and mostly of idiopathic etiology, that may limit comparison with modern studies.
In newer publications, there is limited data addressing specifically social functioning in ASD. Ackermans et al. studied a small cohort of ASD patients (n = 43) regarding their baseline limitations in participating in social activities, as measured through the impact on participation and autonomy questionnaire (IPA). 33 Patients had an overall IPA of 28.5% (maximum score 0%), which was worse than the scores for spinal cord injury patients and age-matched healthy individuals (23.9% and 6.3%, respectively). Interestingly, the most affected IPA domains were “family role” and “autonomy outdoors”, indicating limitations in household activities and visiting relatives. Additionally, they correlated this metric with other variables like age, mini-mental status examination, comorbidities, radiographic parameters, BESTest (clinical balance test) and SRS-22r. The strongest correlation in a multivariate linear regression was with the SRS-22 total score. However, this study only described a small cohort of patients, in their baseline status with no surgical or nonsurgical treatment. 33
Yoshida et al reported on 170 patients undergoing surgery for ASD from a multicentric European database. They reported a 11.3% mean improvement in social function at 2 years according to the SF-36 domain and 34.3% of improvement at the social life component for ODI. 34 They did not report specifically on questions 14 and 18 of the SRS-22r, but they observed 14.1% and 41.7% improvement on function and self-image domains at 2 years, respectively. Their ODI improvement compares favorably with our study, although their sample was younger (mean age 52.1 years).
Neuman et al reported on return to work after ASD surgery, another component of social functioning. In a cohort of 188 patients with a mean age of 51 years, 69% were working full time, according to their definition using question 9 from the SRS-22r score. 35 At 2 years of follow-up, the proportion of patients working full time increased to 84%. However, the percentages of patients working full time only applied to those employed at baseline, and employment/unemployment proportions were not given for the entire cohort. Our cohort includes older patients, with more than 60% of them retired at baseline; thus, return to work may not be a valuable metric for this population. Nevertheless, both studies use a similar methodology focusing on social functioning aspects relevant for patient and surgeon decision-making and expectations. In a similar study, Durand et al described improvements in work/school productivity and decreased absenteeism in surgically treated ASD patients at 2 years, as opposed to non-operatively treated patients who did not improve. 36
Regarding the practical implications of this study, elderly patients with adult spinal deformity can be counseled that surgery is likely to produce meaningful improvements in their social life — beyond relief of pain and restoration of mobility. These improvements include greater ease in going out with relatives and friends and reduced interference of back-related limitations on personal relationships. Importantly, these gains appear to occur regardless of the presence of complications or cognitive impairment. The benefit is most pronounced among those who are socially limited before surgery: approximately three-quarters of the most affected patients improve at 2 years, and more than 90% of those who were previously home-restricted report enhanced social participation.
The social dimension should be systematically assessed in ASD patients, as it represents a critical determinant of recovery, reintegration, and overall quality of life. Its relevance has been recognized by the World Health Organization (WHO), the Organization for Economic Co-operation and Development (OECD), 3 and international expert groups such as the Core Outcome Study in Scoliosis (COSSCO) 4 initiative by the Scoliosis Research Society and the AO Spine Adult Spinal Deformity Patient Profile project. 5 Although a universally adopted instrument for measuring social functioning in ASD is lacking, several validated tools can be incorporated into future studies to provide a more comprehensive assessment. These include the PROMIS® Social Function domains (Participation and Satisfaction), 6 the SF-36 Social Functioning subscale, 7 the WHOQOL-BREF Social Relationships domain, 8 and the Impact on Participation and Autonomy (IPA) 9 questionnaire—recently applied in ASD cohorts, among others.
This study has some limitations. The retrospective nature of our analysis, though based on a prospectively collected database, as well as lack of comparison group may introduce some bias. We used measurement instruments that may not fully capture the entire social functioning phenomenon as affected by ASD but rather focus on pain-related limitations (as measured by the ODI) and isolated questions from the SRS-22r, perhaps oversimplifying the social functioning alterations in our patients. These outcome forms were not designed or validated to be used in isolation as has been done in this study. Using single or partial items from multidimensional questionnaires may reduce measurement reliability and content validity, limit comparability with prior studies or reference values, and increase measurement error, as these tools were developed and validated as whole constructs rather than as stand-alone items. Hence, the findings should be interpreted as exploratory, reflecting proxies of social participation rather than definitive measures of social function. What is more, some of the other social determinants of health were not measured or discussed, such as financial stability, caregiver support, and living situation. Nevertheless, the 2 questions chosen from the SRS-22r most closely represent the pertinent aspects of social function in the cohort we were studying. Despite these limitations, the data still provides useful information for both patients and surgeons on the potential effects on this aspect of their condition. Also, a follow-up period of 2 years, while providing useful data, may be short for understanding the long-term transitions in social function after surgery, as complications or other comorbidities, especially in cognitive decline, may arise over longer periods that could have significant impact on the patients’ social function. Finally, although external validity is strengthened by the participation of centers from multiple continents, the findings may still not be fully representative of all clinical settings.
Conclusions
In this study, we report on improved social function after ASD surgery in a diverse international group of patients over 60 years of age as measured by the ODI social function question and through 2 questions of the SRS 22r. The improvement was observed in all continents in this multicenter study and was not affected by complications as measured at the predetermined time points. Improved social function was highly correlated with improvement in the SRS 22r function domain. The data is presented as both means as well as based on pre-operative social function to provide more granular information on the expected outcome for patients based on their presenting social function. The data provided in this series adds practical information on the expected outcomes following ASD surgery in older patients and could be included in preoperative patient counselling. Future studies should explore the sustainability of these results over the long-term using validated tools, and their association with other domains, such as function, satisfaction, and cognition.
Supplemental Material
Supplemental Material - Can Social Function Improve in Older Patients Undergoing Multi-Level Spinal Deformity Surgery?
Supplemental Material for Can Social Function Improve in Older Patients Undergoing Multi-Level Spinal Deformity Surgery? by Mauricio Andres Campos Daziano, Lauren Daunt, Vanessa Vashishth, Eliana Seider, Aazad Abbas, Anna Rienmueller, Yukihiro Matsuyama, Yong Qiu, Michael Kelly, Justin S. Smith, Benny T. Dahl, Maarten Spruit, Marinus de Kleuver, David Polly, Jonathan Sembrano, Ferran Pellisé-Urquiza, Kenneth M. C. Cheung, Ahmet Alanay, Lawrence G. Lenke, Christopher I. Shaffrey, Sigurd H. Berven, Stephen J. Lewis, PEEDS Study Group and AO Spine Knowledge Forum Deformity in Global Spine Journal
Footnotes
Acknowledgement
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Spine Deformity experts. AO Spine is a clinical specialty of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research and the AO Innovation Translation Center, Clinical Evidence.
PEEDS Study Group:
Stephen J. Lewis, MD, MSc Department of Surgery and Spine Program, University of Toronto, Toronto, Ontario, Canada
Lawrence G. Lenke, MD Department of Orthopedic Surgery, The Spine Hospital, Columbia University Medical Center, New York, NY, USA
Christopher I. Shaffrey, MD Department of Orthopaedic Surgery, Duke University, Durham, NC, USA
Justin S. Smith Department of Neurosurgery, University of Virginia, Charlottesville, VA, USA
Kenneth MC Cheung, MD Department of Orthopaedics and Traumatology, The University of Hong Kong, Hong Kong SAR, China
Sigurd H. Berven, MD Department of Neurosurgery and Orthopaedic Surgery, University of California, San Francisco, San Francisco, CA, USA
Yong Qiu, MD Spine Surgery, Drum Tower Hospital of Nanjing University Medical School, Nanjing, Jiangsu, China
Yukihiro Matsuyama, MD, PhD Department of Orthopedic Surgery, Hamamatsu University School of Medicine, Hamamatsu, Shizuoka, Japan
Ferran Pellisé-Urquiza, MD, PhD Hospital Universitari de la Vall d’Hebron, Barcelona, Spain
Jonathan Sembrano, MD Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, MN, USA
Benny T. Dahl, MD Division of Orthopedic Surgery, Texas Children’s Hospital, Baylor College of Medicine, Houston & Rigshospitalet, National University of Denmark, Copenhagen, Denmark
Michael Kelly, MD, MSc Orthopaedic Surgery, Washington University School of Medicine, St Louis, MO, USA
Maarten Spruit, MD, PhD Sint Maartenskliniek Nijmegen, Ubbergen (near Nijmegen) Gelderland, the Netherlands
Ahmet Alanay, MD Department of Orthopedics and Traumatology, Acibadem Mehmet Ali Aydinlar University, Istanbul, Turkey
ORCID iDs
Ethical Considerations
Ethics/Institutional Review Board approval was given at each site. The main IRB approval was obtained from University Health Network Research Ethics Board, 700 University Ave, Toronto, Ontario M5G 1Z5, University of Toronto on 18.03.2014. Authorization number (Approval number): 13-6942-AE.
Consent to Participate
Informed consent was obtained from all patients.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine, a clinical specialty of the AO Foundation, which is an independent medically-guided not-for-profit organization.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.