
Abstract
Study Design:
Retrospective case series.
Objective:
Despite numerous advances in the technology and techniques available to spinal surgeons, lumbar decompression remains the mainstay of degenerative lumbar spine surgery. It has proven efficacy in trials, but only limited evidence of advantage over conservative management in large scale systematic reviews. We collated data from a large surgically managed cohort to evaluate the patient-reported outcomes.
Methods:
We performed a retrospective analysis of a prospectively populated database. Patient demographics, surgical details, and patient outcomes (Spine Tango core outcome measures index [COMI]–Low Back) were collected for 2699 lumbar decompression surgeries.
Results:
Lumbar decompression was shown to be successful at improving leg pain (mean improvement in visual analogue scale [VAS] at 3 months = 4) and to a lesser extent, back pain (mean improvement in VAS at 3 months = 2.61). Mean improvement in COMI score was 3.15 for all-comers. Minimal clinically important improvement (MCID) in COMI score (−2 points) was achieved in 73% of patients by 2-year follow-up. Primary surgery was more effective than redo surgery: odds ratio 0.547 (95% CI 0.408-0.733, P < .001). The benefits across all outcomes were maintained for the 2-year follow-up period. Patients can be classified according to their outcome as “early responders”; achieving MCID by 3 months (61% primary vs 41% redo), “late responders”; achieving MCID by 2 years (15% vs 20%) or nonresponders (24% vs 39%).
Conclusions:
Lumbar decompression is effective in improving quality of life in appropriately selected patients. Patient-reported outcome measures collected routinely and collated within a registry are a powerful tool for assessing the efficacy of lumbar spine interventions and allow accurate counseling of patients perioperatively.
Keywords
Introduction
Lumbar stenosis is a degenerative condition resulting in diminished spinal canal caliber and compression of the contained neural structures before they exit the neural foramen. This may manifest as back pain, radicular pain, paresthesia, weakness, or clinical syndromes such as neurogenic claudication and cauda equina syndrome. 1 Lumbar decompression has demonstrated efficacy over conservative management for the treatment of radicular symptoms in trials; however, results of large-scale systematic reviews are neutral. 2 -10
There are a multitude of surgical decompression strategies to decompress neural structures with no convincing evidence to support one technique over another. 11 -16 These may be augmented by instrumentation to achieve vertebral fusion, correction of deformity, or structural imbalance. Indirect decompression via implantation of a motion-preserving stabilizing device or interspinous device has latterly fallen out of favor due to lack of efficacy with higher complication and reoperation rates. 17 There has been much attention paid to the question of decompression alone versus decompression plus fusion for the management of lumbar stenosis, particularly in the presence of degenerative spondylolisthesis. 10,18 -24
There is often a disconnect between the radiological severity of stenosis, and the severity of clinical symptoms. Consequently, a patient with severe narrowing and significant neural effacement may be asymptomatic or may present only with minor symptoms and vice versa. 25 The decision to operate is largely clinically driven and thus a secure and thorough understanding of the features which most affect patients is crucial to guide decision making. 26 -29
Historically, the assessment of surgical success was based on largely subjective clinical and/or radiological assessment by the surgeon. This is inadequate given the poor correlation between magnetic resonance imaging findings and symptoms described above and has since been superseded by the development of patient-reported outcome measures (PROMs). PROMs while subjective are based on patients’ experiences and symptom reporting and so have much better reliability and “real-world” applicability. 30 Numerous instruments have been developed to extract outcome data focused on dimensions of quality of life (QoL), including generic and disease-specific questionnaires focused on lower back pain and its impact. 31 -34 The relative merits of these are reviewed elsewhere. 35 -37 All instruments quantify the impact of a pathological process on aspects of QoL and vary by how dimension specific they are. 38 One example of these is the COMI-Back questionnaire, which comprises 7 questions in disease-specific domains (pain, function, symptom-specific well-being, quality of life, and disability), which are aggregated into a single, validated, and widely used “COMI-score.” 39 -41
Spine Tango is an international registry built to assess the effectiveness and safety of spinal surgery. 42 Launched in 2002 under the auspices of EuroSpine, it records baseline patient demographic and disease specific data as well as surgical data. Patient-reported outcome data is collected in the form of the core outcome measures index (COMI) score as well as the Oswestry Disability Index (ODI) at baseline, 3 months, 12 months, and 24 months. 26,31
PROMs are thus of great utility to the surgeon as they provide a reliable inventory of outcomes that patients themselves have nominated as being the most important. 43 This affords the surgeon a common language with which to communicate the purpose and indications supporting surgery, as well as the likelihood of improvement. 3,44
The aim of this study was to review a large dataset from our extensive and growing spinal surgery database to evaluate outcomes of simple decompression surgery from the patient’s perspective.
Methods
Anonymized data from all patients who underwent lumbar decompression surgery of any description at a single UK tertiary neurosurgery unit (Walton Centre NHS Foundation Trust [WCFT]) from January 2012 to October 2016 were extracted from our prospectively maintained Spine Tango database, and retrospectively analyzed. 42 The database was first established in 2012. Approval from the local research, development, and innovation department for collection and analysis of outcome data within this registry was preexisting.
Patient-specific data included age, sex, American Society of Anesthesiologists physical classification score (ASA), body mass index (BMI), and smoking status. Disease-specific data included one primary pathology, and optional multiple secondary pathologies such as disc herniation, lateral stenosis, central stenosis, foraminal stenosis, and synovial cyst. Surgeries performed for tumor, infection, trauma, and any surgery entailing instrumentation were excluded.
Surgery-specific data included the specified therapeutic aim (axial pain relief, peripheral pain relief, functional improvement, bladder/bowel function, prophylactic decompression). In addition, details on surgical approach, mode of decompression, and any other surgical measures, as well as any intraoperative and postoperative complications were recorded.
Statistical analysis was performed with R studio. 45 Statistical significance was defined as P < .05. Univariate analysis was performed using paired and unpaired Student’s T test for paired and unpaired continuous normally distributed data, respectively, and chi-square test for categorical data. Binomial logistic regression was used to assess factors predictive of successful outcome.
In accordance with the published standard, minimal clinically important difference (MCID) was defined as a COMI decrease of 2 points between the pre- and postoperative scores at various time points. This was calculated at 3, 12, and 24 months.
Anecdotal clinical experience has found that some patients respond early, some late, and some never, to lumbar decompression. To assess predictors of this, patients were classified based on their individual interval change in COMI score as: early responders (MCID achieved at 3 months), late responders (MCID achieved at 12- or 24-month follow-up, or nonresponders (MCID not achieved).
Results
Patients
Between January 2012 and October 2016, a total of 2699 lumbar decompression surgeries were performed in 2611 patients at WCFT and data inputted to the Spine Tango database. Demographics are presented in Table 1, and surgical details are presented in Table 2.
Patient Demographics.
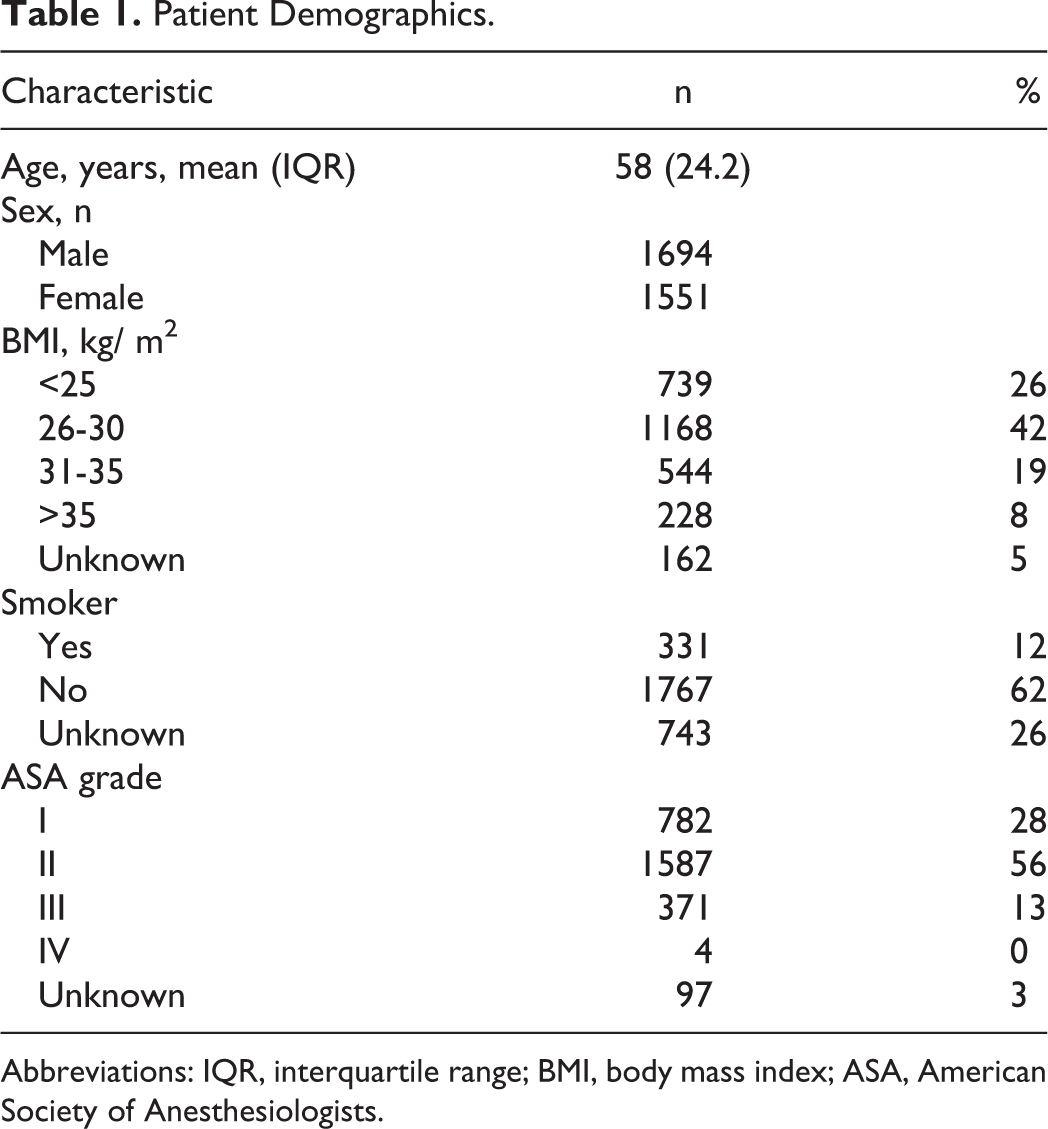
Abbreviations: IQR, interquartile range; BMI, body mass index; ASA, American Society of Anesthesiologists.
Disease-Specific and Surgical Details.
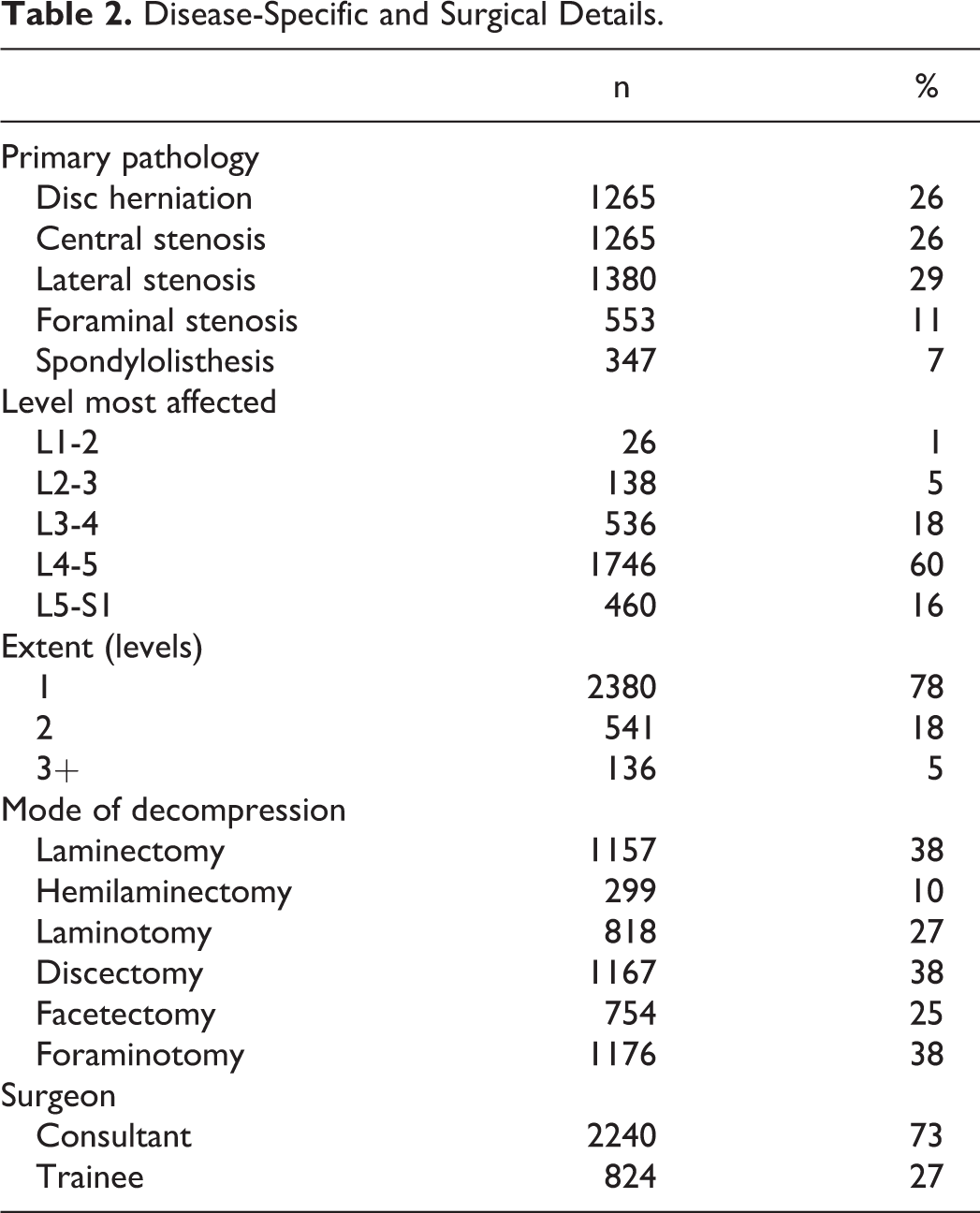
Mean age of patients was 58 years. There was a slight male preponderance (59.6%) and the majority of patients had BMI in either the overweight (47%) or obese (25%) categories. The majority of patients were nonsmokers (62%) and the modal ASA class was II (56%). The most commonly operated level was L4/5 (60%) and most were single-level surgeries (78%).
Return rates for COMI questionnaires were 85% at 3 months, 80% at 1 year, and 58% at 2 years. Paired COMI response rates (ie, baseline and interval response available) were available for 64% at 3 months, 61% at 1 year, and 55% at 2 years. Complete follow-up data (baseline, 3 months, 1 year, and 2 years) was obtained for only 49% of patients.
Symptomatic and QoL Outcomes (Table 3, Figure 1)
Preoperative COMI
Mean COMI was 8.03 (SD 1.53) with the major symptoms ranked by patients as leg/buttock pain (51%) followed by sensory disturbance (28%) and back pain (20%). Mean visual analogue scale (VAS) score at baseline was 7.8 (SD 2.12) for leg pain and 6.6 (SD 2.66) for back pain. QoL was rated as very bad or bad in 70% of respondents, and moderate to very good in 30%.
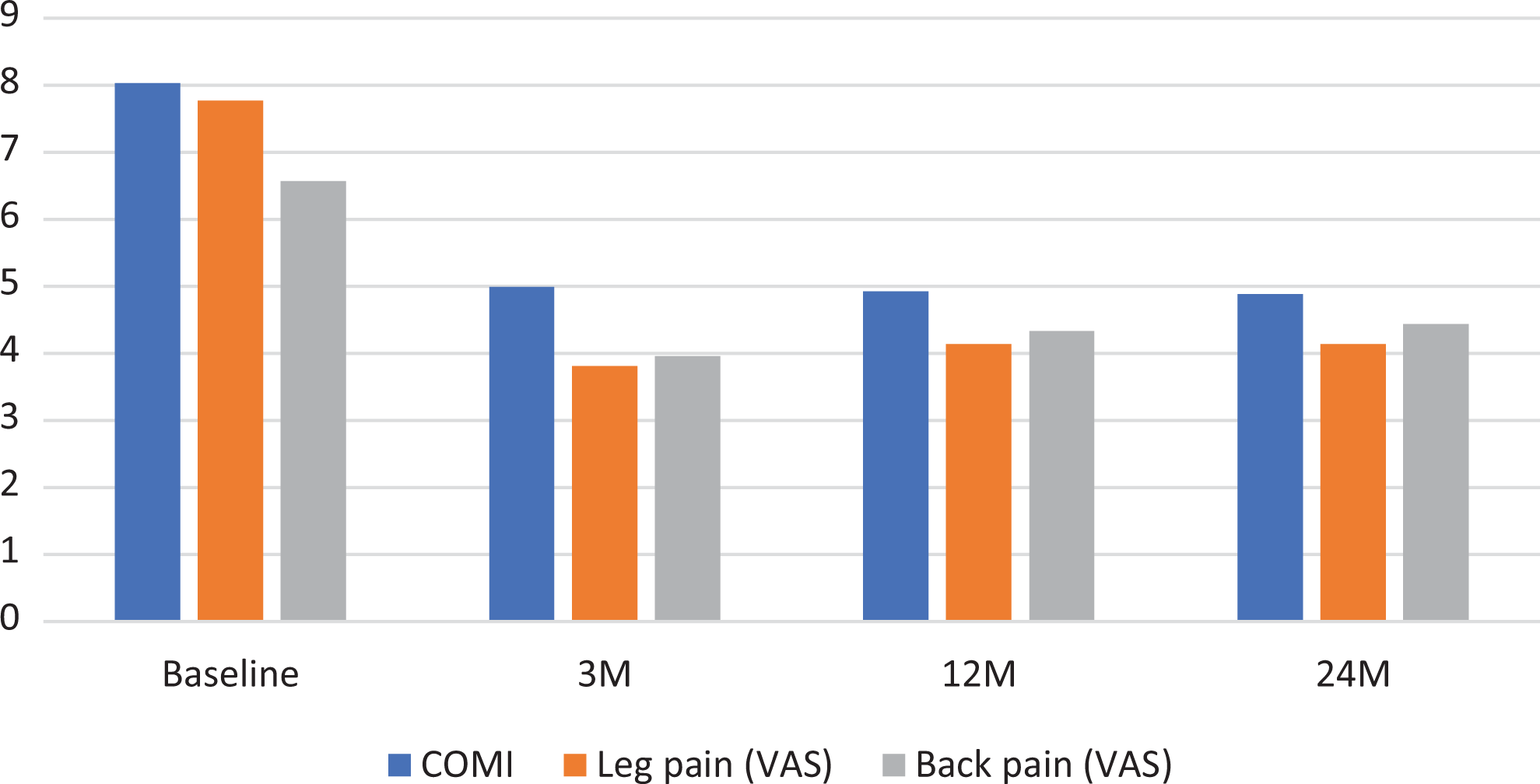
Symptomatic and quality of life (QoL) outcomes following lumbar decompression surgery.
Quality of Life and Symptoms Outcomes Following Lumbar Decompression.
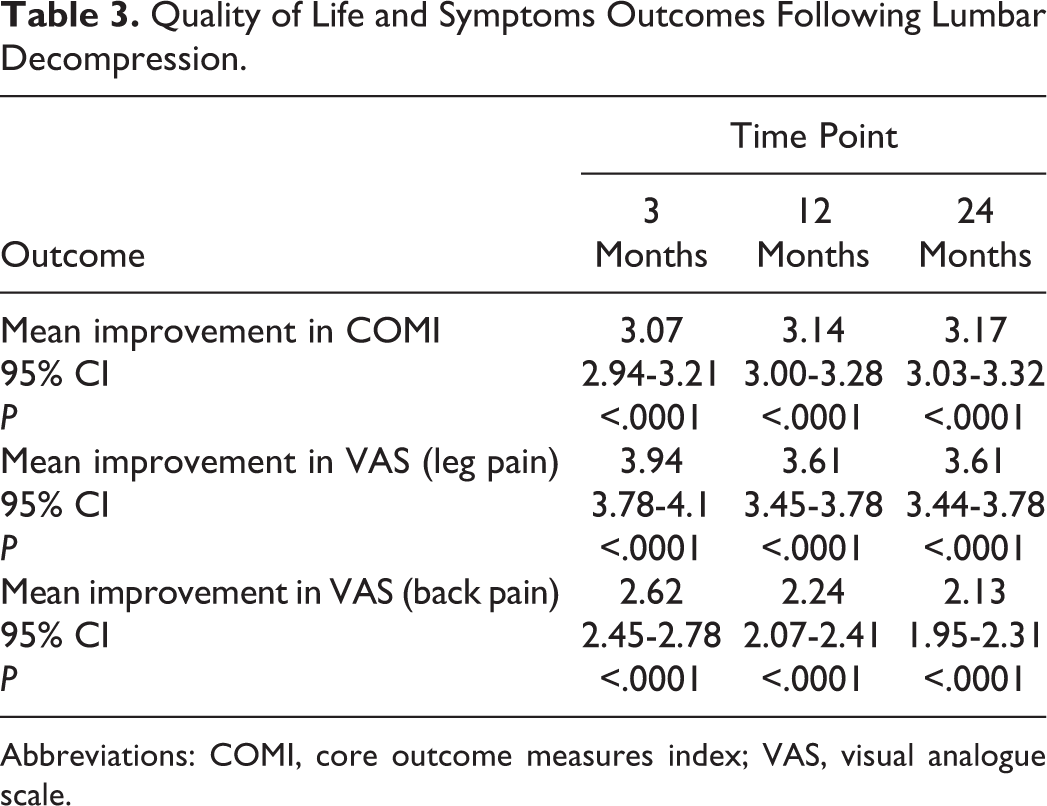
Abbreviations: COMI, core outcome measures index; VAS, visual analogue scale.
3-Month COMI
Mean COMI improved by 3.07 points (95% CI 2.94-3.21, P < .0001) Significant improvements were seen in both leg and back pain mean VAS scores; decreasing by 3.94 (95% CI 3.78-4.10, P < .0001) and 2.62 (95% CI 2.45-2.78, P < .0001), respectively. Accordingly, QoL assessments improved with 25.6% of respondents now rating their QoL as very bad or bad and 74.4% rating it moderate to very good.
1-Year COMI
Improvements seen at immediate (3 months) follow up were maintained at 1-year follow-up with a mean COMI improvement of 3.14 (95% CI 3.00-3.28, P < .0001). Improvements in leg pain and back pain VAS scores were similarly maintained at 3.61 (95% CI 3.45-3.78, P < .0001) and 2.24 (95% CI 2.07-2.41, P < .0001), respectively. There was a small but nonsignificant increase in the proportion of patients rating QoL as very bad or bad (28.5%) versus moderate to very good (71.5%) compared with 3-month follow-up.
2-Year COMI
Two-year COMI responses revealed sustained improvements in overall COMI scores of 3.17 (95% CI 3.03-3.32, P < .0001). Mean improvement in VAS scores remained unchanged; leg pain 3.61 (95% CI 3.44-3.78, P < .001), back pain 2.13 (95% CI 1.95-2.31, P < .0001). A total of 27.1% of respondents rated their QoL as very bad or bad compared with 72.9% moderate to very good.
Redo Versus Primary (Table 4)
A total of 718 of the included cases were revision surgeries. In all, 490 were for previous surgery at least partly involving the same vertebral level. Baseline COMI was significantly worse in those patients undergoing redo surgery compared with primary decompression (mean difference 0.15, 95% CI −0.28 to −0.01, P = .003). Paired COMI scores at 3 months for primary decompression were significantly better than for redo (mean difference −0.78, 95% CI −1.17 to −0.4, P < .001). This difference extended out to 1-year follow-up (mean difference −0.98, 95% CI −1.36 to −0.6, P < .001) and 2-year follow-up (mean difference −1.03, 95% CI −1.45 to –0.6, P < .001).
Comparison of Core Outcomes Measure Index (COMI) Outcomes in Primary and Redo Lumbar Decompression Surgery.

Minimal Clinically Important Difference (Figure 2)
The MCID is defined as a decrease in interval COMI score of at least 2 points 26 . Analysis of unselected respondents shows an MCID response at 3 months in 56% of patients (early responders) with a further 17% achieving MCID by the end of the follow-up period (late responders). A total of 27% failed to achieve MCID. Selecting for those patients who underwent primary surgery reveals a higher rate of early responders compared with redo surgery (61% vs 41%). A further 15% of primary surgery patients had a late response compared with 20% of redo patients. Overall MCID response rates during the follow-up period were 76% for primary surgery and 61% for redo surgery.
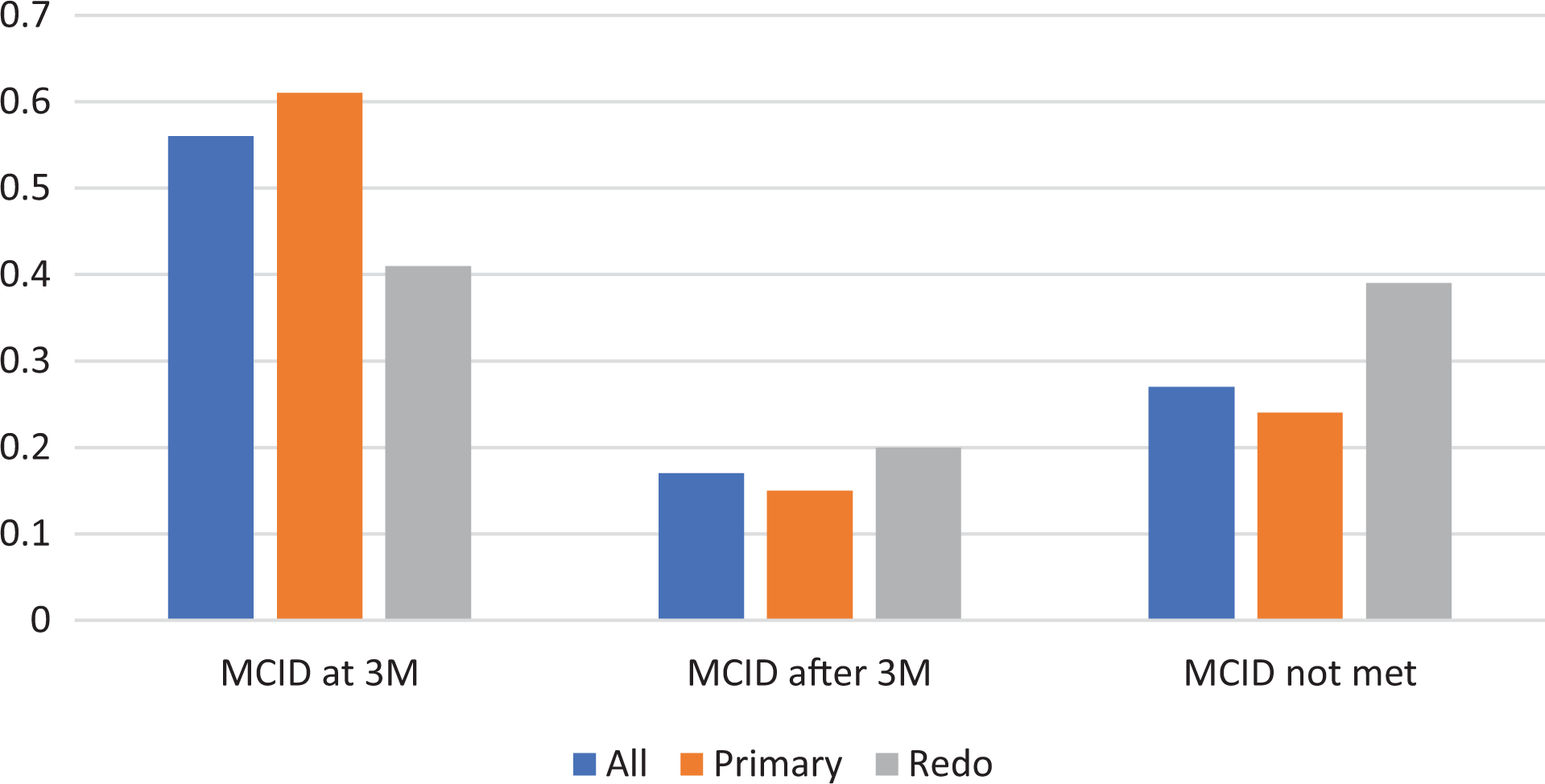
Minimal clinically important difference (MCID) response categories following lumbar decompression surgery.
Multivariate Analysis (Table 5)
Using achievement of MCID as the outcome of interest we performed binominal logistic regression analysis on patient related factors and surgery/pathology related factors as detailed in Table 5. This analysis revealed that in terms of patient-related factors advancing age was an independent positive predictive factor for achieving MCID (odds ratio [OR] 1.017, P = .005) while poor general fitness (ASA III) was an independent negative predictive factor (OR 0.552, P = .011).
Logistic Regression Analysis of Patient, Pathological, and Surgical Factors Influencing MCID Outcome in Lumbar Decompression Surgery.
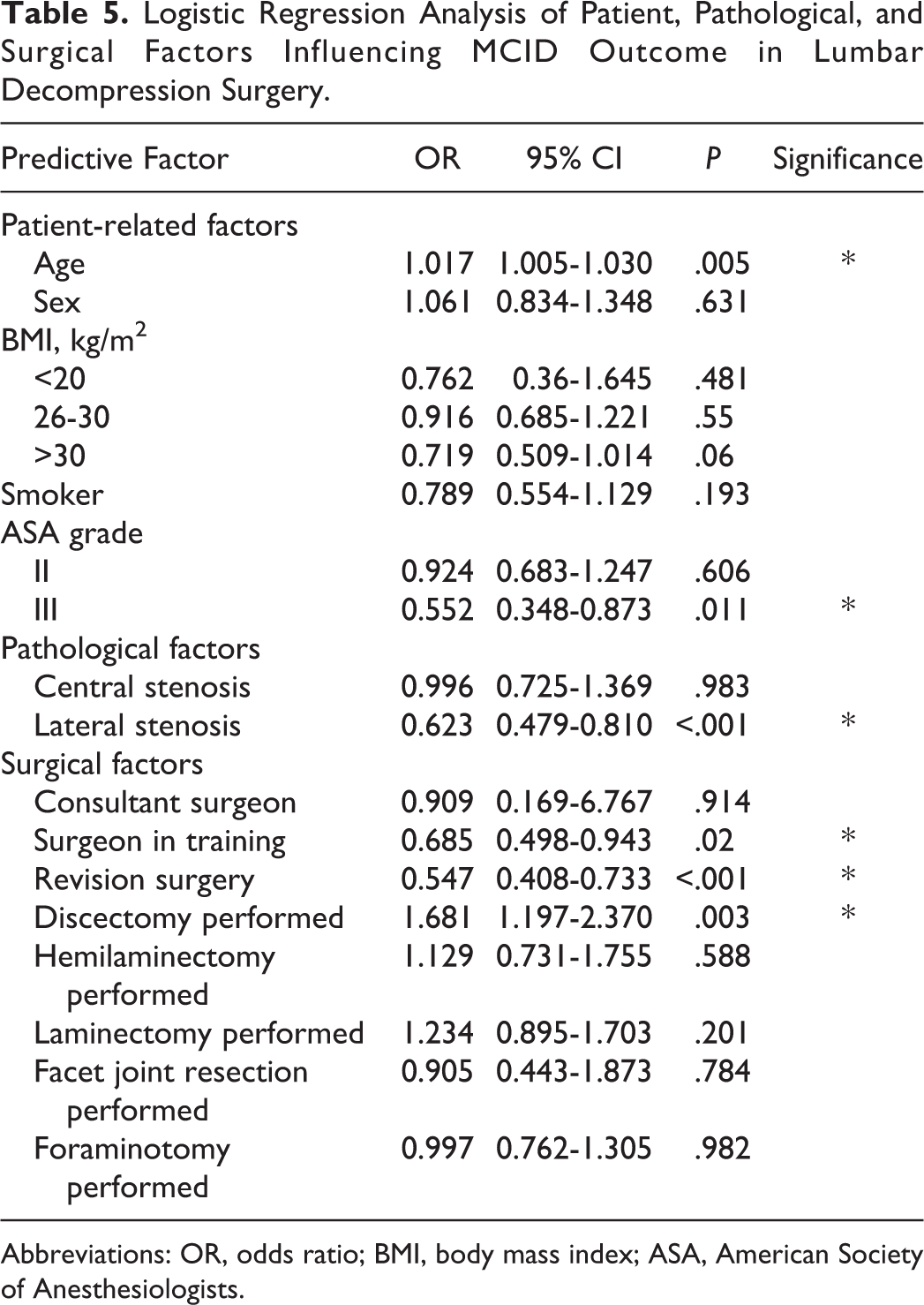
Abbreviations: OR, odds ratio; BMI, body mass index; ASA, American Society of Anesthesiologists.
Analysis of pathological factors revealed that presence of lateral stenosis predicted poorer outcome (OR 0.623, P < .001). Independent negative surgical factors were factors were surgery performed by a surgeon in training (OR 0.702, P = .032), revision surgery (OR 0.547, P < .001), and the only positive predictive factor identified was performance of a discectomy as part of the surgery (OR 1.681, P = .003).
Discussion
Our study sought to assess the response to lumbar decompression surgery in a large unselected cohort using prospective data recorded via a registry platform. Our data confirms the efficacy of lumbar decompression for symptomatic lumbar canal stenosis. Use of the COMI score demonstrates clinically relevant improvements in symptoms and good levels of patient satisfaction with the procedure.
Prospectively collected registry data including patient-reported outcome data is a powerful tool for assessment of the efficacy and acceptability of interventions. They can also permit identification of potential factors predictive of outcome.
Patients undergoing primary decompression surgery have good response rates to surgery with 76% achieving a clinically relevant improvement overall. A total of 61% of these patients will demonstrate improvement by 3 months postoperatively. Patients undergoing redo surgery also demonstrate reasonable response to lumbar decompression for symptomatic stenosis but to a lesser degree. Patients can be categorized retrospectively into 1 of 3 distinct groups depending on the presence and timing of response; early, late, and nonresponders.
The use of PROMs within health care has grown in the past 2 decades as their utility in assessing both acceptability and efficacy of interventions has been recognized. 35,36,46,47 In the United Kingdom, the National Institute for Health and Care Excellence (NICE) routinely collects PROM data for common procedures. 48 In recognition of the unsustainable growth in health care costs and the important role PROMs have to play in this, the US government has established the Patient-Centered Outcomes Research Institute (PCORI). 49 PROMs not only reflect the efficacy of surgery within individual patients but also provide a standard of assessment that allows collation of data from thousands of patients. 50 Collection of this data within a prospective registry then permits direct comparison of practice within and between units and even the establishment of benchmarks of practice and is thus integral to evidence-based health care reform. 51 PROM data is now routinely collated in registries within the United Kingdom and across Europe and the United States. 2,42,52,53 They are widely employed within other areas of healthcare but within spinal surgery, where the focus is primarily on improving QoL, there is a natural fit. 54
Limitations of the Study
The inherently subjective nature of PROMs leaves them vulnerable to bias from interpatient variations in interpretation, recall bias and inaccuracy or inconsistency of self-reporting due to both positive and negative motivations. 55 There is also disparity reported in responses when different tools are used in the same patient cohorts. 56
We have seen significant dropout in return rates for questionnaires with complete datasets achieved for only 49% of patients. This is to some degree inevitable even with a robust setup with employment of dedicated registry staff, as in our department. Establishing and maintaining such infrastructure requires significant investment. The dropout rate may be due in part to discharge of patients from clinical follow-up. It would be unusual for example, to continue reviewing patients for 2 years who demonstrate a successful outcome at 3 months. Incomplete data is a potential for bias though it is not possible to say whether patients with poor outcomes are more, or less likely to respond compared with those with a good outcome, or vice versa.
Posterior spinal decompression comes with a theoretical risk of introducing instability and progressive spondylolisthesis due to disruption of the posterior tension band. Our 2-year follow-up does not permit us to comment on this. Likewise, as our follow-up is based solely on patient-reported outcomes, there is no radiological follow-up data available. Correlation of radiological and PROMs findings in this regard would be an interesting avenue for future enquiry, however.
The value of registry data is also very much dependent on the quality of input and consistency of entries by different clinicians. There will inevitably be inconsistencies between contributors. We do not feel it is appropriate to comment therefore on the efficacy of specific techniques or pathological features which predict response.
Given that our figures are taken from a surgical registry there is no data on outcomes for patients managed nonoperatively. A number of interventional trials have addressed this question; however, prospectively collected longitudinal data on clinical course for conservatively managed patients within a registry would be a valuable resource. 4,5,7 This would enhance the validity of conclusions drawn from analysis of registry data.
Ours is a heterogeneous dataset containing a wide distribution of patient demographics and comorbidities. In our patient population, there is representation of the multiple sites and sources of spinal canal stenosis. The range of surgical approaches employed is therefore broad, reflecting, we believe, the application of a tailored surgical strategy dependent on the site of stenosis. While our data is rich in detail, it was not collected to answer a specific question so should not be used as a surrogate for interventional research. There is significant potential for confounding bias given the multiplicity of factors that influence response following surgery.
Multivariate analysis has been applied with caution in our study and we note the presence of certain negative predictive factors, namely; significant medical comorbidity, junior operator, and redo surgery. Conversely, performance of discectomy was identified as associated with improved outcomes. This could conceivably result from an acute/subacute prolapse precipitating presentation in a patient with more chronic stenotic disease.
Other predictive factors identified appear to the authors as counterintuitive, particularly the association of advancing age and better outcomes and also surgery performed in the presence of lateral stenosis resulting in worse outcomes. We feel these potentially anomalous results may due to confounding bias. Extensive subgroup/regression analysis should therefore be applied with discretion and caution is advised when interpreting these results. As an example: Worse outcome is anticipated in patients presenting as an emergency with cauda equina syndrome versus their elective counterparts. The emergency cohort is more likely to receive surgery out of hours by a trainee neurosurgeon and thus there may be a false association between poor outcome and grade of operator.
We have not in this study attempted to assess the extent or adequacy of decompression. For the most part (particularly in successful clinical response) this is because there would not have been any indication to perform follow-up imaging.
There is an attractive simplicity in the description of 3 cohorts; early, late, and nonresponders. This is a language that patients can understand, and this heuristic scheme should facilitate discussion with patients and permit realistic expectation setting when offering surgical intervention. Establishing realistic expectations early in the conversation should optimize rates of patient satisfaction, even in nonresponding cohorts.
Follow-up to 2 years allows capture of those patients who have a very delayed response. Previous studies have indicated that while 3-month follow-up does not accurately predict later outcomes, 1-year follow-up is sufficient following spinal surgery. 57 We feel our data supports continued follow-up to 2 years to capture the improvements in late responders.
Conclusion
We report a very large and heterogeneous case series that confirms lumbar decompression as an effective strategy when performed primarily for the relief of neurogenic claudication symptoms and to a lesser degree back pain. Redo surgery is significantly less likely to be effective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.