
Abstract
Study Design:
Broad narrative review.
Objective:
To review the evolution, operative technique, outcomes, and complications associated with posterior vertebral column resection.
Methods:
A literature review of posterior vertebral column resection was performed. The authors’ surgical technique is outlined in detail. The authors’ experience and the literature regarding vertebral column resection are discussed at length.
Results:
Treatment of severe, rigid coronal and/or sagittal malalignment with posterior vertebral column resection results in approximately 50–70% correction depending on the type of deformity. Surgical site infection rates range from 2.9% to 9.7%. Transient and permanent neurologic injury rates range from 0% to 13.8% and 0% to 6.3%, respectively. Although there are significant variations in EBL throughout the literature, it can be minimized by utilizing tranexamic acid intraoperatively.
Conclusion:
The ability to correct a rigid deformity in the spine relies on osteotomies. Each osteotomy is associated with a particular magnitude of correction at a single level. Posterior vertebral column resection is the most powerful posterior osteotomy method providing a successful correction of fixed complex deformities. Despite meticulous surgical technique and precision, this robust osteotomy technique can be associated with significant morbidity even in the most experienced hands.
Keywords
Introduction
The treatment of severe spinal deformity presents a difficult challenge to the spine surgeon, often requiring osteotomy to correct sagittal and coronal imbalance. Vertebral column resection (VCR) offers the greatest potential correction of these rigid deformities, but comes at the cost of a more technically demanding procedure with increased operative time, estimated blood loss (EBL), neurologic risks, and significant morbidity. 1 Nevertheless, vertebral column resection has evolved over the past century to become a viable last resort for correction of the most challenging spinal deformities through a single, posterior procedure.
History
In 1922, MacLennan 1 described the first vertebrectomy, which consisted of apical body resection for the treatment of severe scoliosis, using a posterior-only approach followed by postoperative casting. For the next 50 years, vertebrectomy was limited to hemivertebra excision in congenital scoliosis.
In 1965, Hodgson 2 expanded vertebrectomy to the treatment of posttuberculosis kyphosis, which he corrected in two patients with an anterior opening-wedge osteotomy combined with anterior fusion with rib-strut grafts. Bradford 3 was the first to describe circumferential apical VCR in a series of 13 patients with severe, rigid deformity in the late 1980s. In a follow-up of the original case series, Bradford and Boachie-Adjei 4 reported on 16 patients who underwent staged circumferential VCR with a mean coronal correction of 54°, sagittal correction of 41°, and relatively few major complications. They later described a 1-stage circumferential VCR for hemivertebral resection under 1 anesthetic session in 7 pediatric patients with congenital scoliosis. 5 In an effort to decrease operating time, EBL, and risk of complications associated with circumferential VCR, Suk et al 6,7 described the first posterior-based vertebral column resection (PVCR) in the early 2000s. To date, PVCR represents the gold standard last-resort osteotomy for the correction of severe, structural deformity of the spine.
The present review endeavors to summarize the surgical techniques and decision making involved in PVCR, all major outcomes studies, and the prevalence of postoperative complications and how to minimize them.
Surgical Decision Making
In addressing imbalance through a posterior-only approach, the surgeon has a variety of osteotomy techniques in their armamentarium. Posterior column osteotomies (PCOs), pedicle subtraction osteotomies (PSOs), and VCR provide increasing correction per operative level, respectively. VCR is typically reserved for a deformity that is not amenable to correction with lesser osteotomies. As the only surgical technique that allows for translation of the spinal column, VCR is often necessary for rigid, multiplanar deformities. 6 Sharp angular sagittal deformities in the thoracic spine necessitate VCR, as do coronal imbalances, in which the shoulder to pelvis association cannot be corrected by shortening one side of the spine. 8,9 Other conditions suitable for VCR include spondyloptosis at L5, 10 hemivertebra resection, 5 resectable spinal tumors, and failure of formation in congenital kyphosis. 8 Broadly, VCR indications include (a) deformity with Cobb angle >100° that is both angular and rigid (flexibility<10%) and (b) decompensation in the coronal or sagittal plane (asymmetry between the length of the concave and convex curves of the deformity). 6,8,9,11
Authors’ Preferred Operative Technique
The surgical technique for PVCR is technically demanding. The patient first should be positioned appropriately on the Jackson frame with well-padded bony prominences to avoid excessive pressure points, peripheral nerve injury, and to assist in reduction of the spinal deformity (Figure 1). The frame should allow full extension of the hips and a free abdomen. Attention should be given to ensure the facial structures and orbits are free of pressure, so placement into Gardner-Wells tong or temporary intraoperative Halo traction is often performed. Given spinal cord shortening and possible neurologic risk inherent to the procedure, multimodality neuromonitoring is essential.

Proper positioning of the patient on the Jackson frame. All bony prominences are well padded, the abdomen is free from compression, and the patient is positioned in reverse Trendelenberg positioning.
Exposure of the posterior column with meticulous subperiosteal dissection and minimization of blood loss is required. Tranexamic acid, an antifibrinolytic, is also utilized to minimize blood loss at a loading dose of 50 mg/kg and maintenance dose of 5 mg/kg/hr is typically provided. Once exposure is complete, inferior facetectomies are performed. Then PCOs are done at the periapical levels of the deformity corresponding to the levels around the planned VCR. This allows for safer and efficient harmonious correction about the apex. The bone autograft from the osteotomies is saved for the fusion bed. The periapical PCOs also allow direct palpation of the medial border of the pedicle through the spinal canal, which facilitates pedicle screw placement. This is particularly important in the periapical portion of the concavity where the spinal cord often drapes over the medial wall of the pedicle. Of note in patients with severe angular kyphosis we place concave pedicle screws with a temporary rod prior to performing our periapical PCOs since there is a higher risk of subtle stretching of the spinal cord over the kyphotic apex without instrumentation, which can lead to neuromonitoring data loss and potential neurologic complications.
Insertion of pedicle screws is done according to the free-hand technique as originally described by Kim and Lenke, 12 with at least 3 levels cephalad and 3 levels caudal to the planned VCR to allow for a temporary stabilizing rod. We place all concave apical screws in patients with a prior fusion mass under direct palpation of the medial aspect of the pedicle through a wide laminectomy. A fused deformity may also require hook placement directly into the fusion mass above and below the planned VCR in a claw-type construct for additional stability. The wide apical laminectomy is extended from the inferior aspect of the pedicle above to the superior aspect of the pedicle below the area being resected. This allows for sufficient visualization during resection and monitoring dural buckling during correction. Multiaxial reduction screws (MARS) are utilized in the periapical region, particularly caudal to the VCR level. These caudal reduction screws may assist in preventing any ventral drift of the spinal segment inferior to the VCR. MARS also allow for expeditious temporary rod placement during anterior column resection and deformity reduction. Screws from T6 to S1 are tested with an electromyography (EMG) probe to confirm intraosseous placement.
For a VCR done within the thoracic region, the medial portion of bilateral ribs are excised 5 cm at the planned level. The transverse processes are resected bilaterally as well exposing the lateral portion of the pedicles and vertebral body. Bone acquired from the resection of the rib and the transverse process, as well as from PCOs at cephalad and caudal levels should be preserved for the fusion bed. The lateral aspect of the pedicle and vertebral body are dissected with Penfield elevators. The thoracic nerve root on the convexity of the planned VCR level is usually ligated while the concave root is saved. Our protocol is to clamp the nerve root for 10 minutes while checking motor-evoked potentials prior to ligation to minimize the risk of compromising blood supply to the spinal cord.
Prior to anterior column resection, the spine is preemptively stabilized with a temporary rod connected to at least 2 or 3 levels cephalad and caudal to the planned VCR level. For patients with a severe angular kyphosis, we use dual temporary stabilizing rod. For all other patients, we use one unilateral temporary rod. First the concave pedicle is resected both since it lies in a relatively ventral position where blood can pool and resection can decrease tension on the spinal cord by allowing the spinal cord to move medially from its original position draped over the medial aspect of the concave pedicle. Since the concave pedicle is often completely cortical, we use a high-speed burr for resection while protecting the dura. Since the vertebral body is rotated dorsal and lateral on the convex side of the deformity, the convex pedicle allows for a much more direct path for resection of the vertebral body. As a result, the convex pedicle allows access to the majority of the vertebral body. Next the lateral vertebral body is dissected and a malleable retractor or “spoon” retractor is used to protect the pleura, vessels, and sympathetic chain. With the retractor in place, the vertebral body is then excised with the posterior cortex portion resected last to minimize epidural bleeding. A thin portion of the anterior wall is left attached to the anterior longitudinal ligament to promote fusion.
Discectomies above and below may be utilized to minimize the potential bleeding surfaces; however, in cases with previous anterior column fusion, intravertebral resection is necessary. Violation of the endplates at this stage may lead to late subsidence of the intracorporeal strut. Bipolar cautery and topical hemostatic agents are useful for bleeding control. Reverse-angled curettes, Kerrison rongeurs, or posterior wall impactors may be used for removal of the posterior wall. This completes the resection and with resection of any adjacent level osteophytes ensures that there is no ventral cord compression during correction. Following verification that the dura is free, the correction can be performed and the anterior column rigidly reconstructed.
Correction involves shortening and translation of the spine; distraction is performed only after sufficient shortening has produced adequate slack of the concave dura/spinal cord. Convex compression is done either through individual pedicle screws in patients with good bone stock or in a construct-to-construct closure mechanism using dominoes at the apex of the resected area (Figure 2). Correction proceeds slowly through the use of the temporary stabilizing rod to prevent subluxation and dural impingement. An intervertebral cage is then placed at the VCR level to provide anterior column support, prevent anterior shortening, provide correction of kyphosis, and provide shear force stabilization. This is particularly important for patients with severe angular kyphosis since the anterior cage functions as a hinge for kyphosis correction and protects from both overshortening and ventral buckling of the cord. After the majority of the correction is achieved, the contralateral permanent rod is placed and the ipsilateral temporary stabilizing rod is exchanged for a permanent rod. Further closure of the anterior column is performed with final correction maneuvers. Anteroposterior and lateral 36-inch radiographs are obtained to assure spinal balance. Decortication and bone grafting ensue while the laminectomy defect is covered with the previously garnered ribs and morselized bone graft. The rib graft is immobilized by a cross-link or sutures (Figure 3).
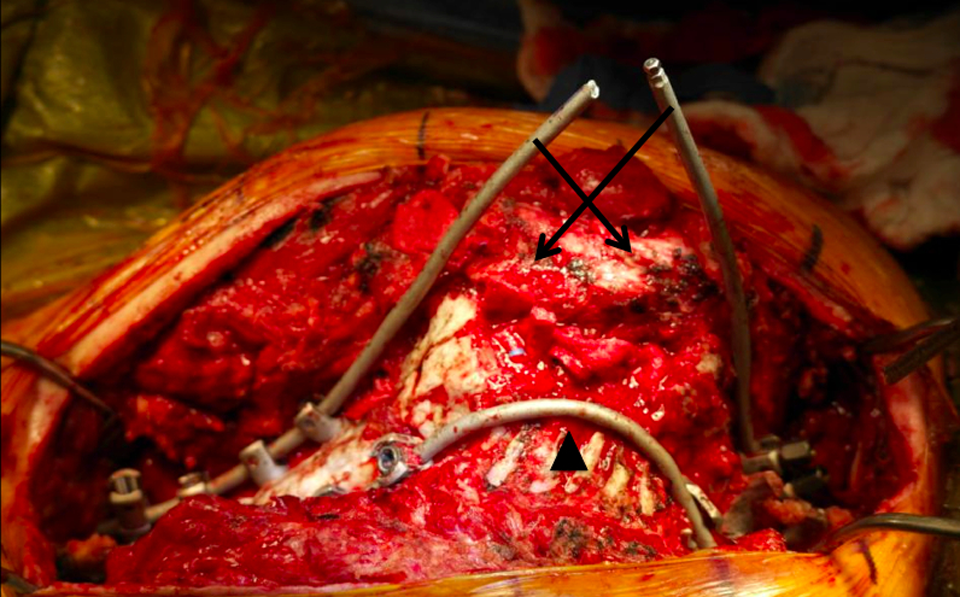
The “joystick correction” is a construct-to-construct closure technique for reduction after column resection. A contralateral tracking rod is placed on the concavity (black arrowhead) to prevent subluxation and dural impingement during reduction. Convex compression is applied across the resection site (black arrows) with proximal and distal joystick rods.

An intraoperative final construct with 3 rods across the vertebral resection site. The laminectomy defect is covered with the previously garnered ribs and morselized bone graft. The rib graft is immobilized by sutures in a cross-linking fashion.
An exemplary case is provided in Figures 4, 5, and 6. The patient is a 21-year-old man with a history of Scheuermann’s kyphosis and multiple prior spine procedures, including a posterior spinal fusion from T2 to L2. He required extension to C3 for proximal junctional disease and extension to L3 for L2 screw pull-out. The patient eventually required removal of all implantation for deep wound infection. He presented to our clinic with progressive pain and kyphosis but no neurologic complaints. The patient underwent a revision posterior spinal fusion from C3 to pelvis with vertebral column resection at L3. Preoperative and postoperative radiographs, as well as clinical photographs reveal the powerful hyperkyphotic correction and sagittal realignment obtained with this procedure.
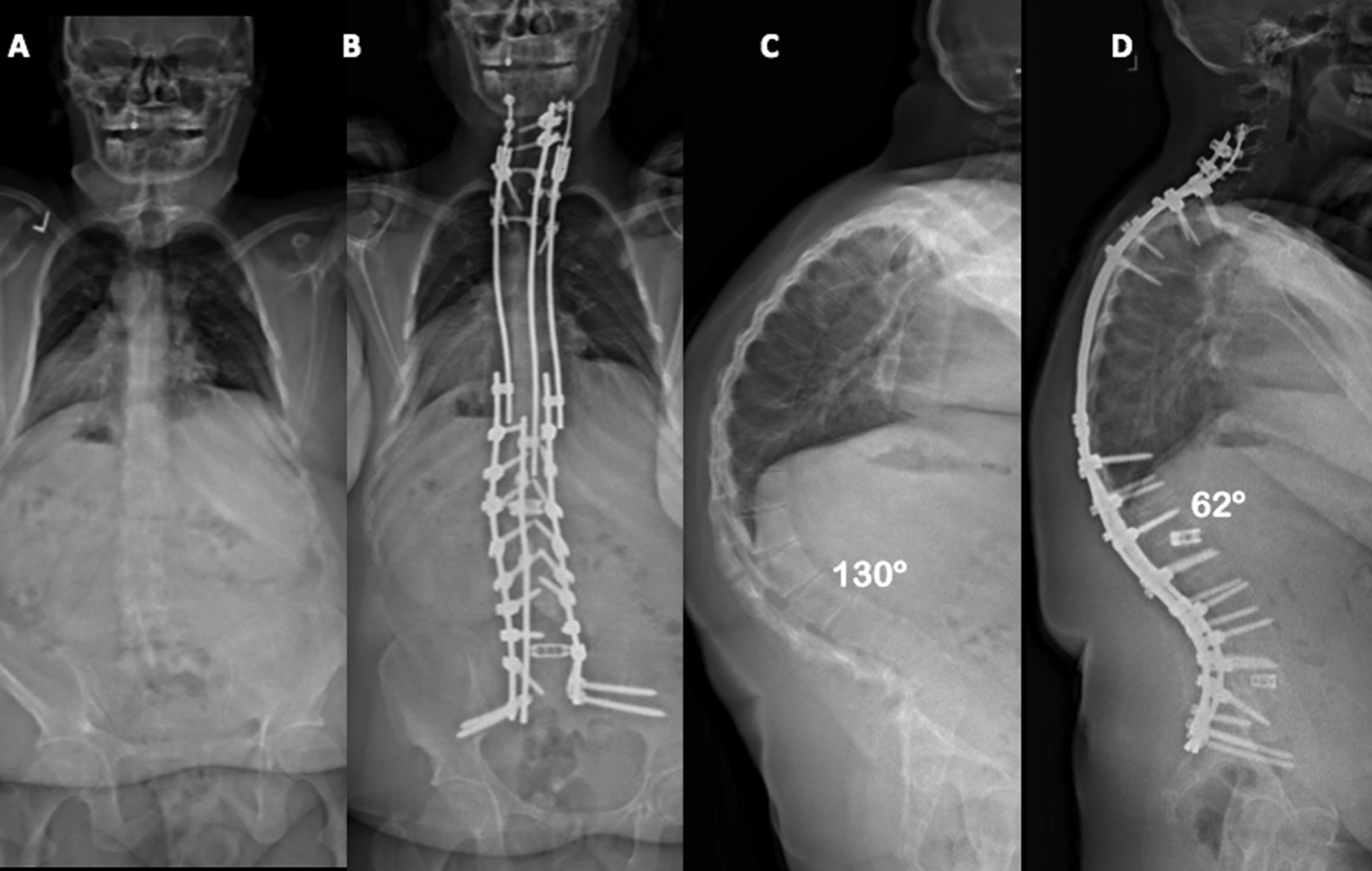
Revision posterior spinal fusion C3 to pelvis with posterior-based vertebral column resection (PVCR) at L1 for correction of Scheuermann’s kyphosis. Preoperative (A) and postoperative (B) Anteroposterior (AP) radiographs. Preoperative (C) and postoperative (D) lateral radiographs show a >50% reduction in the thoracic kyphosis from 130° to 62° with PVCR.
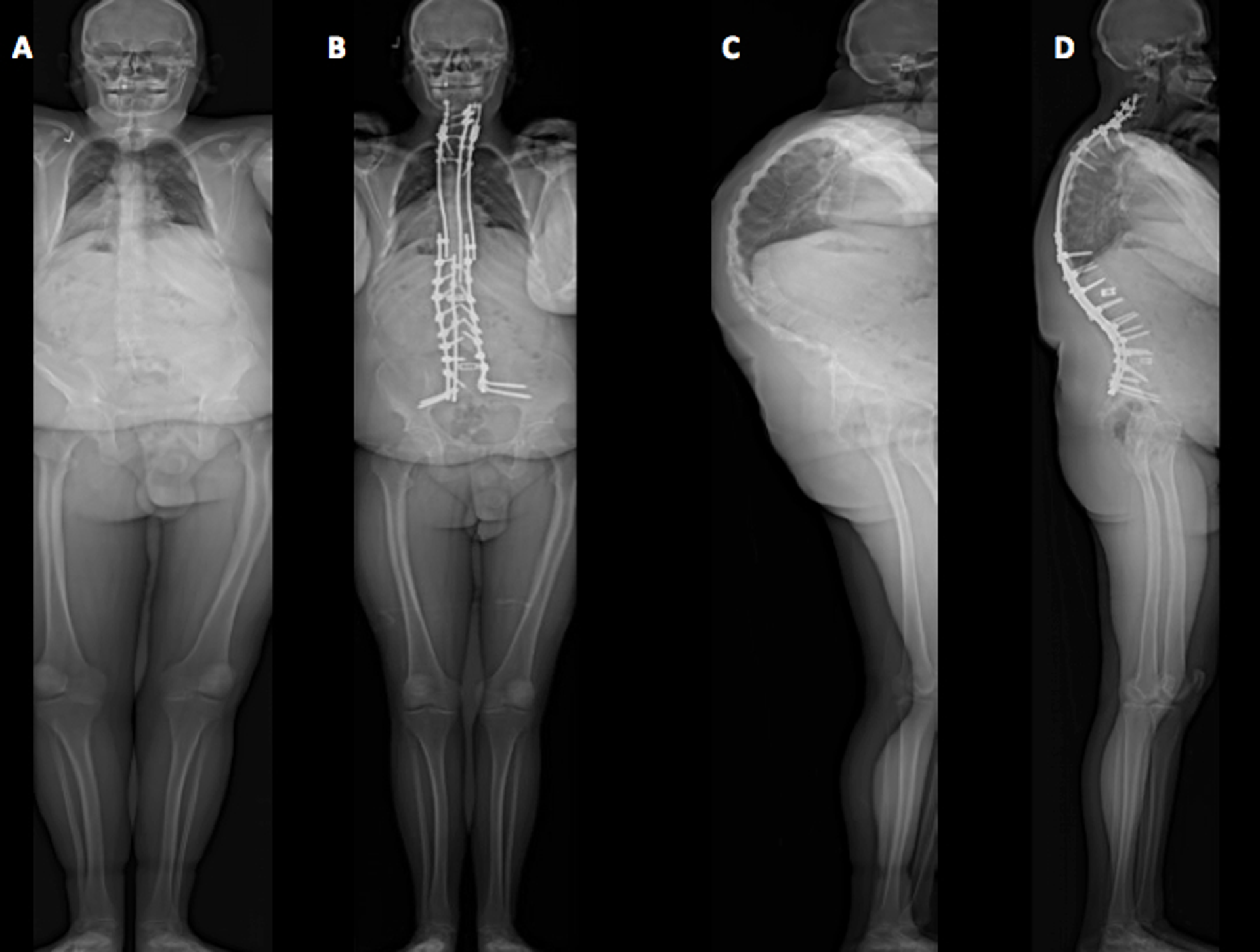
Full-length standing preoperative (A) and postoperative (B) anteroposterior (AP) radiographs. Powerful correction of the sagittal imbalance and chin-brow vertical angle with posterior-based vertebral column resection (PVCR) is demonstrated in the full-length standing preoperative (C) and postoperative (D) lateral radiographs.
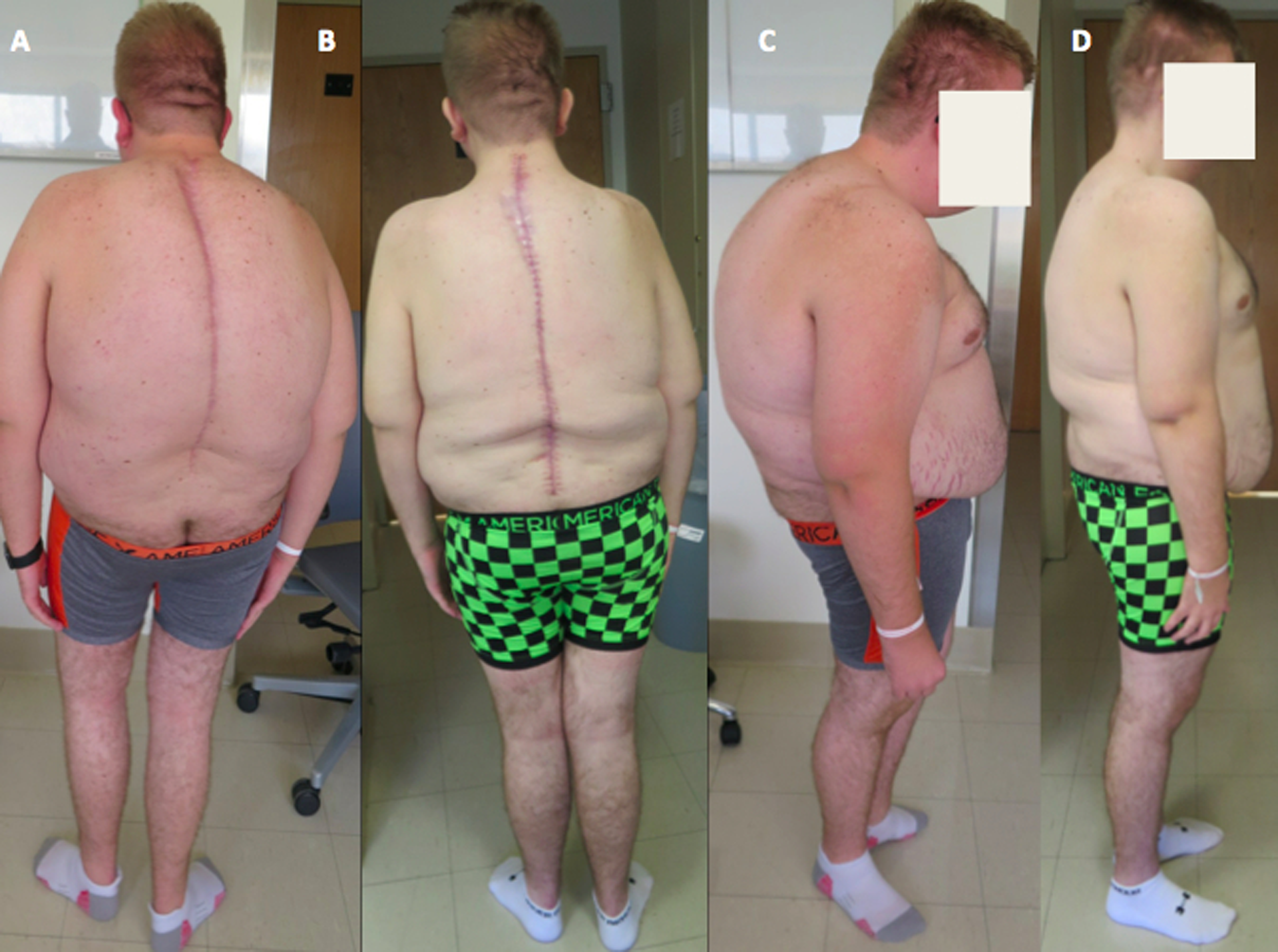
Preoperative (A) and postoperative (B) standing photographs. Preoperative (C) and postoperative (D) lateral photographs revealing restoration of sagittal alignment and horizontal gaze.
Clinical Outcomes
Since the advent of PVCR by Suk in 2002, clinical and radiographic outcomes have been comparable to circumferential VCR and superior to many other osteotomies used for severe spinal deformity. Suk et al 6 first reported on 70 patients (average age 27.4 years with minimum 2-year follow-up) who underwent PVCR for adult scoliosis (curve >80°, <25% flexibility), congenital kyphoscoliosis (trunk imbalance, <25% flexibility, and hemivertebra), or post-infectious kyphosis (rigid, fused vertebral body with <10% flexibility). Overall correction was 61.9% in the coronal plane and 47.5° in the sagittal plane with 2.53 cm restoration of coronal balance and 2.77 cm restoration of sagittal balance. However, complications were significant and occurred in 24 out of the 70 patients (34.3%) in the study, including 2 patients with complete cord injuries.
A subsequent study by Suk et al 7 of 25 patients with fixed lumbosacral deformity who underwent PVCR showed 60% correction and 1.1 cm improvement in the coronal plane and 40% correction and 4.7 cm correction in the sagittal plane. All patients experienced improvement in their preoperative neurologic compromise while 68% of patients experienced reduction in pain. Complication rate was 20% without any permanent paralysis.
Lenke et al 14 reported the first North American study of 43 adult and pediatric PVCR patients at the 42nd Annual Scoliosis Research Society (SRS) Meeting in 2007. Patients were divided into 4 main groups: severe scoliosis, global kyphosis, angular kyphosis, and kyphoscoliosis. The severe scoliosis correction rate of 69%, global kyphosis correction of 54%, angular kyphosis correction of 63% and combined kyphoscoliosis correction of 54% was better than most other prior circumferential or posterior-only VCR reports in the literature. 13 The same group also described the first series of pediatric patients with severe spinal deformities treated by PVCR in 2009 and included 35 consecutive patients with minimum 2-year follow-up and similar amount of correction.
In 2013, Lenke et al 15 published the largest series of pediatric VCR in the literature. It comprised of a multicenter, multisurgeon review of 147 pediatric patients with 127 PVCRs (17 staged) and 20 circumferential VCRs (10 staged) combining an average of 1.6 (range 1-5) resected vertebrae with a mean follow-up of 17 months. The cumulative results showed an improvement of 54% in the coronal plane and 47% in the sagittal plane. Of the patients with minimum 1-year postoperative SRS-30 scores, 90% experienced statistically significant improvement in self-image, function, mental health, and satisfaction subscores. A trend toward improvement in the pain subscore was noted but not statistically significant. Cobb angle improvements tended to underestimate the clinical improvement observed in many patients. Overall complication rate was 58.5%, including 68 intraoperative and 43 postoperative complications, and no deaths. Of note, there was no difference in complication rate between PVCR and circumferential VCR and no difference in complication rate between staged and nonstaged procedures. Increased EBL was associated with a higher risk of intraoperative complication, while patient age, operative time, and preoperative Cobb measurements were not. None of these variables were associated with increased risk of postoperative complication.
Papadopolous et al 16 performed PVCR on 45 patients with severe rigid kyphosis (9 congenital, 36 posttuberculous) and obtained a mean 44.5% correction. SRS-22 scores showed improvement in the self-image domain (P = .01) and non–statistically significant improvement in the pain and function domains. Complication rate requiring revision surgery was 22.2%, including 2 permanent paraplegias.
In 28 patients with rigid spinal deformity curves >100° (kyphosis or kyphoscoliosis), Xie et al 17 noted scoliosis correction of 59% and kyphosis correction of 68%. However, complication rates were particularly high with 64% of patients experiencing at least 1 complication. In a more recent 2014 study by the same group evaluating risk factors for neurologic complications in 76 PVCR patients, Xie et al 18 noted a 65.4% correction of scoliosis and a 69.7% correction of kyphosis.
Ozturk et al 19 described 44 patients with severe spinal deformity treated by PVCR. In the scoliosis patients, coronal curve improved 61.3% with an 81% improvement in coronal imbalance. In the kyphosis patients, sagittal curve improved 60% with a 76% improvement in sagittal imbalance. In the kyphoscoliosis patients, coronal curve improved 60% with a 76% improvement in coronal imbalance and sagittal curve improved 58% with a 71% improvement in sagittal imbalance. Only 11% of patients experienced postoperative complication, including 2 postoperative infections, 2 dural lacerations, and 1 hemopneumothorax.
In one of the larger studies of PVCR, Hamzaoglu et al 20 described 102 patients who underwent PVCR from 1996 to 2007 with minimum 2-year follow-up, including 78 one-level, 15 two-level, and 9 three-level resections. Correction in the coronal plane was 62% with a 72% improvement in coronal balance. Correction in the sagittal plane was 57% with a 71% improvement in sagittal balance. Overall complication rate was not reported.
Kim et al 21 reported on 152 patients who underwent PVCR from 1997 to 2006 and compared patient outcome to 81 patients undergoing vertebral column decancellation (VCD). PVCR offered superior coronal correction (67% vs 51%) and sagittal correction (51.5° vs 40.0°) compared with VCD. The authors noted a complication rate for PVCR of 39.5%, including 14% transient neurologic deficits, 3% permanent neurologic deficits, 8% instrument failures or progressing curves, 7% wound infections (6.6%), and 11% dural tears. These were statistically insignificant from the VCD complication rate of 42.0%.
Auerbach et al 22 compared outcomes of 87 PSO and and 18 VCR patients. VCR offered superior kyphosis correction (64° vs 35.2°), but equivalent improvements in satisfaction, overall SRS score, and self-image SRS subscore. The greater risk of major complication for PSO in comparison to VCR (38% vs 22%) was not statistically significant (P = .28). Overall, 25% experienced major surgical complications and 15% experienced major medical complications; only 4% of major surgical complications and 3% of major medical complications were permanent. Risk factors for major complication included preoperative sagittal balance of 40 mm or greater, age >60 years, and the presence of 3 or more medical comorbidities (P < .05).
Another study comparing PSO and VCR outcomes in a cohort of patients greater than 60 years of age was published by Hassanzadeh et al 23 in 2013. This retrospectively reviewed prospective series included 51 consecutive patients 60 years or older who underwent PSO, VCR or both by a single surgeon from 2005 to 2009. The entire patient cohort experienced statistically significant improvements in the pain, self-image, activity, mental health, and satisfaction domains of the SRS-22 score and in the Oswetry Disability Index. Overall complication rate was 49%, including 18% major (5 in PSO patients and 4 in VCR patients) and 39% minor complications (14 in PSO patients and 6 in VCR patients).
All the presented studies are retrospective in nature with inherent bias. The heterogeneity of patient diagnoses and rarity of severe spinal deformity requiring VCR often precludes use of a control group or rigorous statistical analysis. Nevertheless, the data presented in these qualitative studies clearly demonstrates the large potential of coronal and sagittal correction with PVCR. In fact, most studies averaged between 50% and 70% correction for both scoliotic and kyphotic deformities and frequently demonstrated even greater corrections of coronal and sagittal imbalances. Most importantly, these results were accompanied by significant improvements in various measures of clinical outcomes.
Operative Duration, Estimated Blood Loss, and Infection
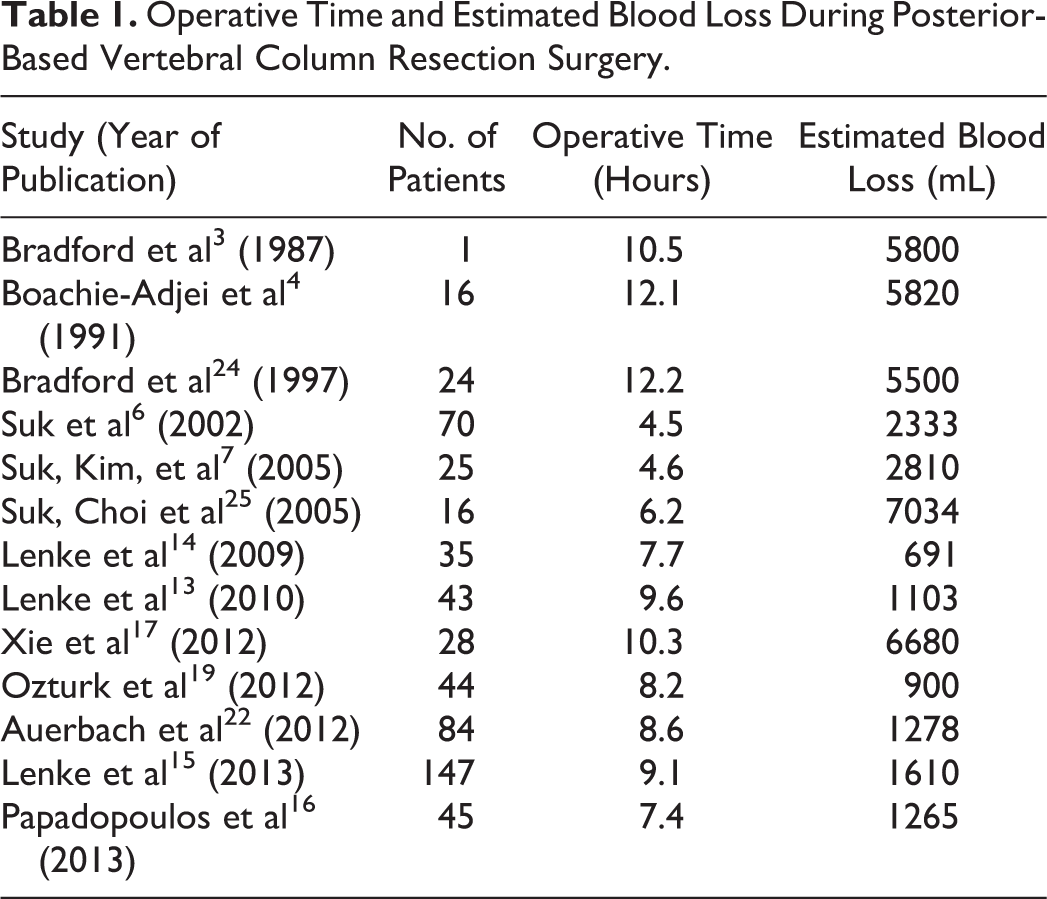
While VCR’s potential for great improvement in radiographic and clinical outcomes has been documented, VCR is a technically demanding procedure with the potential for significant blood loss, operative time, and risk of postoperative infection. Bradford’s first report of staged circumferential VCR had a combined operative time of 10.5 hours and EBL of 5800 mL. 3 Bradford and Boachie-Adjei 4 reported a surgical time of 12.1 hours and EBL of 5850 mL that is similar to the Bradford and Tribus 24 reported surgical time of 12.2 hours and EBL of 5500 mL in staged circumferential VCRs. While PVCR has demonstrated improvement in operative time and EBL, they are not inconsequential. The initial study by Suk et al 6 of 70 patients who underwent PVCR for fixed spinal deformity reduced mean operative time to 4.5 hours and average EBL to 2333 mL. A subsequent study by the same group confirmed the reduced operative time of 4.67 hours and EBL of 2810 mL. 7 However, a third study by Suk et al 25 of patients with severe rigid scoliosis (>80°, <25% flexibility) who underwent PVCR showed higher mean operative time of 6.17 hours and significantly higher EBL of 7034 mL.
While Suk et al 6 pioneered the PVCR procedure, other surgeons have confirmed its improvements in operative time and blood loss. In an early report, Lenke et al 13 described 43 adult and pediatric patients with severe spinal deformity who underwent PVCR and showed an average operative time of 9.62 hours and an average EBL of 1103 mL. Their follow-up study of only pediatric PVCR patients showed average OR time of 7.67 hours and average EBL of 691 mL. 14 In a multicenter study of pediatric VCR patients by Lenke et al, 15 average operative time was 9.07 hours with EBL of 1610 mL. Operative time was significantly less for PVCR (486 minutes) versus circumferential VCR (639 minutes), but no statistically significant difference in EBL was demonstrated between the 2 procedures. As expected, staged procedures had much greater EBL and operative time than single-stage procedures.
Papadapoulos et al 16 described PVCR in patients with severe rigid kyphosis and noted a mean operative time of 7.42 hours and mean EBL of 1265 mL. Xie et al 17 described PVCR in 28 patients with rigid spinal deformity curves greater than 100° and noted mean operative time of 10.33 hours and mean EBL of 6680 mL. Ozturk et al 19 reported on 44 patients with rigid spinal deformity (<30% flexibility) who underwent PVCR with an average OR time of 8.2 hours and average EBL of 900 mL. A study by Auerbach et al 22 showed greater average EBL for PSO than VCR (1867 vs 1278 mL, P < .02) without significant difference in mean operative time (476 vs 518 minutes). A summary of the reported operative durations and EBL can be seen in Table 1.
Operative Time and Estimated Blood Loss During Posterior-Based Vertebral Column Resection Surgery.
The risks of high blood loss are readily apparent and have been directly associated with intraoperative complication. 15 Minimization of EBL is essential with cauterization and antifibrinolytic agents. Previous studies have demonstrated the effectiveness of antifibrinolytics aprotinin, tranexamic acid (TXA), and aminocaproic acid in reducing EBL in spine surgery, 26 but Newton et al 27 performed the first study targeting VCR. In the multicenter review of 136 pediatric patients who underwent PVCR, patients received TXA, aprotinin, or no antifibrinolytic treatment. Total EBL was significantly greater for the non-antifibrinolytic group than the aprotinin group (P = .002) and nonsignificantly greater for the non-antifibrinolytic group than the TXA group (P = .08). Normalized EBL was significantly greater for the non-antifibrinolytic group than the TXA group (P < .01) and the aprotinin group (P < .05), though no difference between the 2 antifibrinolytics was found. Nevertheless, the reduction in metrics of EBL associated with aprotinin and TXA made both potentially desirable adjuncts in PVCR for pediatric patients at the time. With aprotinin’s recent withdrawal from the market, TXA should be considered instead.
In addition to the use of adjunctive antifibrinolytics, the surgeon should take other measures to decrease blood loss. These include meticulous stripping and protection of the segmental vessels, aggressive control of bleeding into the epidural space with cauterization and compression, and segmental artery embolization (3 pairs supplying the artery of Adamkiewicz may be bilaterally blocked without damage to the spinal cord). Unfortunately, epidural bleeding is often difficult to control because direct compression may be precluded by the risk of neurologic compromise. In this setting, judicious use of topical hemostatic agents containing a combination of thrombin, gelatin, and/or a thrombotic matrix may be helpful. The use of hypotensive anesthesia, intrathecal opiods, and performance of discectomy before en bloc excision of the vertebral body are additional strategies for the blood loss reduction in selected patients. It is important to recognize the associated risks of hypotensive anesthesia and intrathecal opiods, especially in the elderly population.
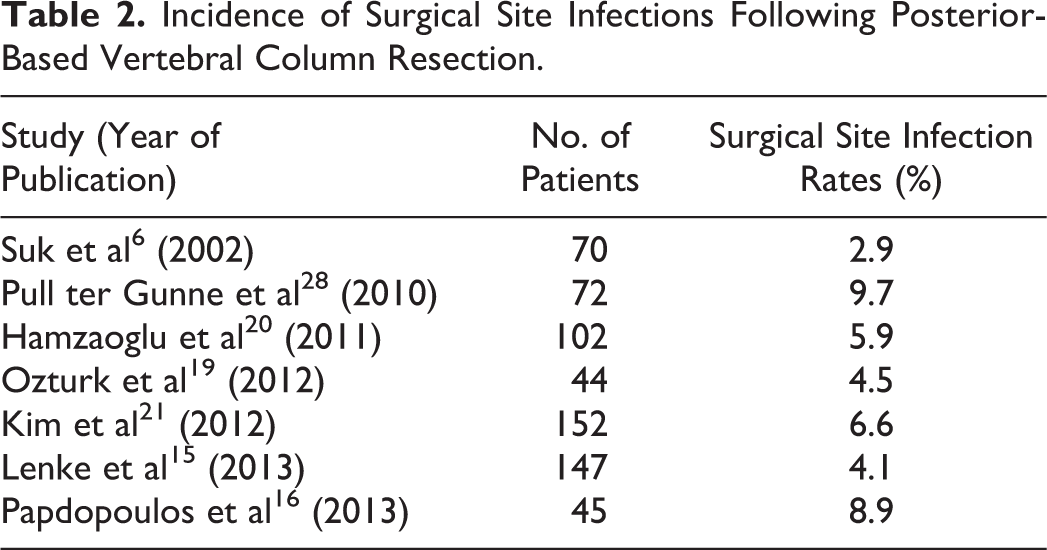
Given extensive surgical exposure and operative time, surgical site infection (SSI) is a concern. Pull ter Gunne et al 28 reported a significantly higher risk of deep SSI with PVCR (9.7%) than PSO (3.4%) and PCO (1.5%), which the authors attributed to the wider exposure required to perform PVCR. There was no statistically significant difference in overall SSI rate or superficial SSI rate for the various osteotomies, though VCR did have the highest SSI rate of 11.1% (vs 4.8% for PSO and 2.9% for PCO). Based on several qualitative studies in the literature, SSI requiring incision and drainage has a reported incidence of 3% to 9% for PVCR 6,15,16,19 –21 as shown in Table 2. In order to minimize SSI, the authors apply 1-2 grams of vancomycin powder directly to the paraspinal musculature following dissection and again immediately prior to closure.
Incidence of Surgical Site Infections Following Posterior-Based Vertebral Column Resection.
Neurologic Complication
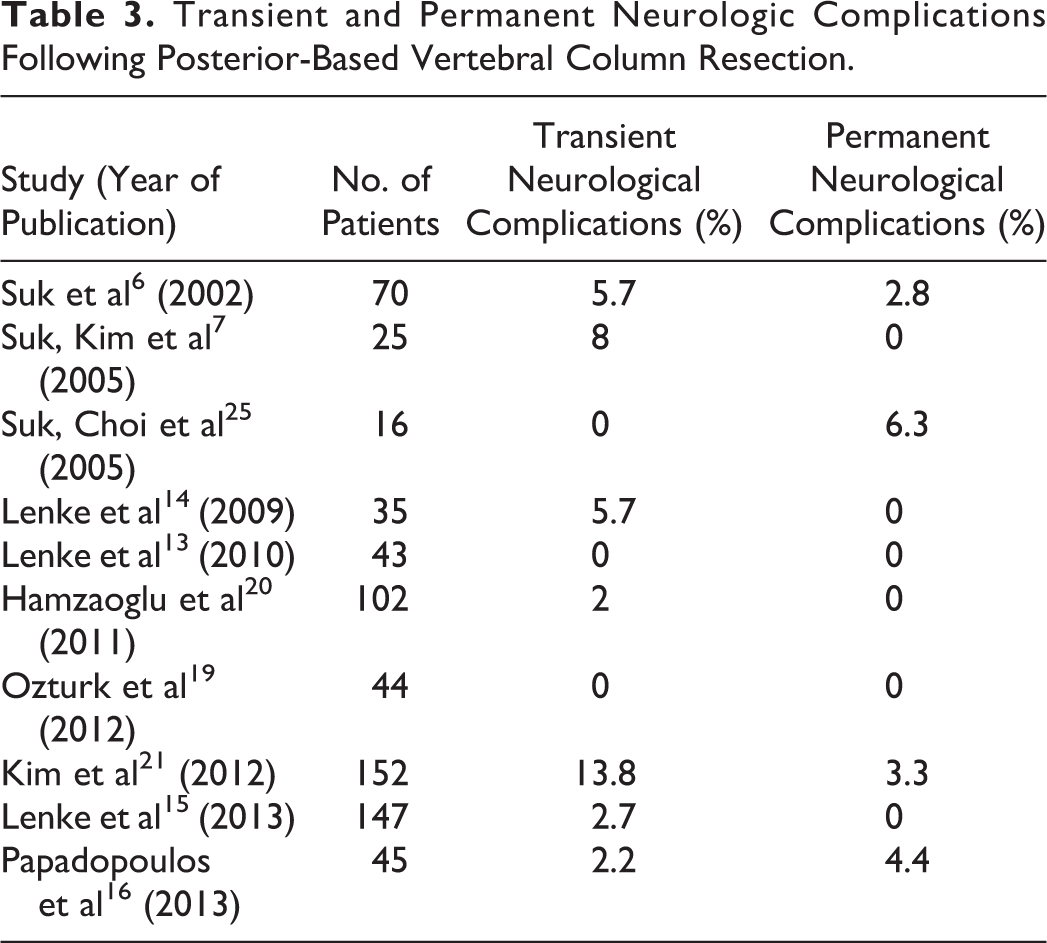
With the potential for significant correction in rigid spinal deformity comes a high risk of neurologic complication. In his first study, Suk et al 6 reported 6% transient nerve root injuries and 3% postoperative permanent complete spinal cord injury. Of note, the spinal cord injury patients had significant preoperative cord compromise and thus a diminished capacity to tolerate the additional stress of extensive surgery. In a follow-up study, Suk et al 7,25 reported 8% transient nerve root injury in PVCR for fixed lumbosacral deformity and 6% (1 patient) complete paralysis in PVCR for severe rigid scoliosis.
Lenke et al 13 reported on 43 adult and pediatric PVCR patients with various severe spinal deformities of which 40 underwent the procedure at L1 or cephalad in spinal cord territory. Following surgery, all patients were at their baseline or showed improved cord function. Seven patients (18%) lost intraoperative neuromonitoring signals but recovered after prompt surgical intervention. Of these 7 patients, all had kyphotic malalignment and 5 had spinal subluxation during vertebrectomy closure causing signal changes. In their study of 35 pediatric only PVCR patients of which 29 underwent the procedure at L1 or cephalad in spinal cord territory, Lenke et al 14 reported only 2 transient neurologic deficits postoperatively. Two other patients had loss of neuromonitoring data during closure that resolved with reopening and closure over a cage and no postoperative deficit. Finally, in the multicenter study of 147 pediatric VCR patients published by Lenke et al, 15 the rate of intraoperative neurologic events was 27%. Postoperative transient neurologic deficit was seen in 3% of cases, and no patients suffered permanent paraplegia.
Papadapoulos et al 16 described intraoperative neuromonitoring changes in 22% patients undergoing PVCR for rigid kyphosis, all due to hypotension, extreme cord manipulation, or osteotomy closure. Two patients (4%) suffered isolated nerve root injuries (1 transient, 1 permanent) and 1 patient (2%) suffered permanent complete spinal cord injury. Ozturk et al 19 described intraoperative changes in 7% though no patients suffered neurologic complication postoperatively. Hamzaoglu et al 20 reported 5% intraoperative neuromonitoring changes, all of which improved with surgical intervention. Only 2 patients (2%) experienced transient nerve root palsies; both resolved by 6 months postoperatively. Kim et al 21 noted 13.8% incidence of transient neurologic deficit with PVCR and 3.3% incidence of permanent neurologic deficit. In summation, nearly one-fourth of all PVCR patients may experience intraoperative neuromonitoring changes. Most of these changes are reversed with surgical intervention. The risk of permanent neurologic complication is likely 2% to 6% as shown in Table 3.
Transient and Permanent Neurologic Complications Following Posterior-Based Vertebral Column Resection.
It is important to identify patients at particularly high neurologic risk prior to performing such a demanding procedure. Xie et al 18 identified risk factors for postoperative neurologic deficits in 76 patients with severe rigid spinal deformities treated with PVCR. While none of the 76 patients suffered permanent paraplegia or nerve root injury, 6 had a postoperative change in neurologic status on physical examination that resolved within 6 months. Preexisting neurologic dysfunction was noted to be the greatest risk factor for postoperative neurologic deficit (odds ratio [OR] = 49.32). Other risk factors were potential intraspinal and brainstem anomalies (OR = 18.42), scoliosis associated with hyperkyphosis (OR = 11.88), and level of vertebral column resection (OR = 8.77). The authors suspected that previous neurological dysfunction may be indicative of preexisting chronic ischemia or “sick spinal cord,” which may decrease the patient’s capacity to withstand distraction of the neural elements or tension on the local vasculature. Similarly, intraspinal and brainstem anomalies, like Chiari malformations and tethered cords, cause fixation of the cord and lead to increased susceptibility to ischemic injury from mechanical traction on segmental vessels.
Kim et al 21 also identified risk factors for postoperative neurologic deficits after 3-column osteotomies. The authors corroborated with multiple logistic regression analysis that preoperative neurologic deficit (OR = 3.04) and resection of 2 or more vertebrae (OR = 4.73) both increased the risk of postoperative neurologic deficit (P < .05). Patients satisfying both of these risk factors experienced a 29-fold increase in neurologic complication rate. Independent variable analysis further noted that preoperative kyphosis (OR = 4.46), a diagnosis of posttuberculous kyphosis (OR = 4.23), fusion extent of >5 segments (OR = 3.20), insertion of titanium mesh (OR = 3.64), operative time >200 minutes (OR = 4.47), and EBL>3000 mL (OR = 3.98) all increased the risk of postoperative transient or permanent neurological deficit; however, these results did not remain significant with multiple logistic regression analysis. When all complications were included (both neurologic and others), multiple logistic regression analysis demonstrated that preoperative neurologic deficit (OR = 3.64), preoperative kyphosis (OR = 3.01), and fusion extent of >5 segments (OR = 1.99) increased the overall complication rate.
Nonunion, Revision, and Other Complications
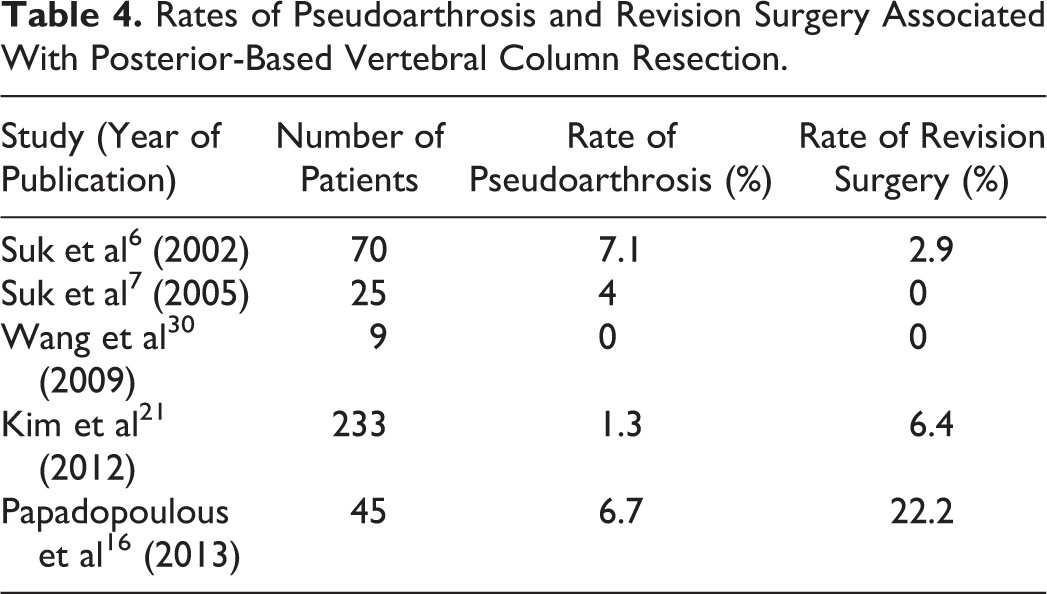
The risk of instrumentation failure, pseudarthrosis, and revision surgery accompany the great magnitude of correction permitted by PVCR. The vertebral void through which this correction is obtained becomes a potential area for nonunion. In their seminal study, Suk et al 6 described a fixation failure incidence of 7.1% (5 patients) in PVCR with minimum 2 years’ follow-up. Of these 5 patients, 3 (4.2%) were successfully treated with 6 months of prolonged localized casting and 2 (2.9%) required revision surgery. In their series of PVCR in fixed lumbosacral deformity, Suk et al 7 experienced 2 (8%) compression fractures and 1 (4%) pseudarthrosis.
The incidence of instrument failure and/or progressive curve in patients with PVCR or PSO was 10.7% in a study by Kim et al. 21 Of these patients, 6.3% required revision surgery. In PVCR for rigid kyphosis, Papadapoulos et al 16 reported 3 patients (6.7%) with pseudarthroses requiring revision surgery. Several other studies mentioned no pseudarthroses complications; the prevalence of such complications may range from 0% to 25% as shown in Table 4. 29,30
Rates of Pseudoarthrosis and Revision Surgery Associated With Posterior-Based Vertebral Column Resection.
Severe thoracic spine deformities may impede proper lung excursion and limit lung capacity, it is possible that PVCR may improve pulmonary function. Bumpass et al 31 recently described the impacts of PVCR on pulmonary function testing in 27 pediatric and 22 adult patients. The authors noted small but statistically significant improvements in mean forced vital capacity (FVC; increase from 2.10 to 2.43 L) and forced expiratory volume in 1 second (FEV1; increase from 1.71 to 1.98 L) in the pediatric patients. These improvements were not observed in the adult patients. The authors hypothesized that the improvement in pediatric patients was due to their greater potential for lung and thoracic cage growth after spinal correction in comparison with mature adults. 32 In comparison to a matched control group of 21 pediatric and 8 adult patients who had undergone circumferential column resections at the same institution, there was no significant difference in pulmonary function postoperatively between the PVCR and circumferential fusion in either adult or pediatric patients. The evidence suggests that although PVCR may slightly improve pulmonary function in pediatric patients, this may not translate into an adult population. Moreover, the potential improvement in pulmonary function with PVCR is no greater than with traditional circumferential column resection.
Conclusion
Severe spinal deformities in the coronal and sagittal plane can be functionally and psychologically debilitating. To obtain a balanced spine, there are various osteotomies in the spine surgeon’s armamentarium. When severity or imbalance is severe enough that other osteotomies cannot correct the deformity, VCR offers the greatest potential correction. However, this powerful method, even in the most experienced hands, can be associated with significant morbidity, particularly in the correction of kyphotic deformity. Because of a variety of reasons, including the relative infrequency of the PVCR procedure, much of the literature reports on combined pediatric and adult outcomes and complications. In order to more clearly define the respective rate of adult and pediatric PVCR complications, future well-stratified studies are needed. Nevertheless, with appropriate application and meticulous surgical technique, PVCR can result in high patient satisfaction and functional outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.