
Abstract
Study Design
Prospective, multicenter, international, observational study
Objective
Identify independent prognostic factors associated with achieving the minimal clinically important difference (MCID) in patient reported outcome measures (PROMs) among adult spinal deformity (ASD) patients ≥60 years of age undergoing primary reconstructive surgery.
Methods
Patients ≥60 years undergoing primary spinal deformity surgery having ≥5 levels fused were recruited for this study. Three approaches were used to assess MCID: (1) absolute change:0.5 point increase in the SRS-22r sub-total score/0.18 point increase in the EQ-5D index; (2) relative change: 15% increase in the SRS-22r sub-total/EQ-5D index; (3) relative change with a cut-off in the outcome at baseline: similar to the relative change with an imposed baseline score of ≤3.2/0.7 for the SRS-22r/EQ-5D, respectively.
Results
171 patients completed the SRS-22r and 170 patients completed the EQ-5D at baseline and at 2 years postoperative. Patients who reached MCID in the SRS-22r self-reported more pain and worse health at baseline in both approaches (1) and (2). Lower baseline PROMs ((1) – OR: .01 [.00-.12]; (2)- OR: .00 [.00-.07]) and number of severe adverse events (AEs) ((1) – OR: .48 [.28-.82]; (2)- OR: .39 [.23-.69]) were the only identified risk factors. Patients who reached MCID in the EQ-5D demonstrated similar characteristics regarding pain and health at baseline as the SRS-22r using approaches (1) and (2). Higher baseline ODI ((1) – OR: 1.05 [1.02-1.07]) and number of severe AEs (OR: .58 [.38-.89]) were identified as predictive variables. Patients who reached MCID in the SRS22r experienced worse health at baseline using approach (3). The number of AEs (OR: .44 [.25-.77]) and baseline PROMs (OR: .01 [.00-.22] were the only identified predictive factors. Patients who reached MCID in the EQ-5D experienced less AEs and a lower number of actions taken due to the occurrence of AEs using approach (3). The number of actions taken due to AEs (OR: .50 [.35-.73]) was found to be the only predictive variable factor. No surgical, clinical, or radiographic variables were identified as risk factors using either of the aforementioned approaches.
Conclusion
In this large multicenter prospective cohort of elderly patients undergoing primary reconstructive surgery for ASD, baseline health status, AEs, and severity of AEs were predictive of reaching MCID. No clinical, radiological, or surgical parameters were identified as factors that can be prognostic for reaching MCID.
Keywords
Introduction
Patient reported outcome measures (PROMs) and health-related quality of life (HRQOL) measures are essential tools in evaluating the quality of care given and overall patient satisfaction. 1 These measures provide a patient-based insight into the patient perception of health status and the impact of spinal disorders on health-related quality of life. Adult spinal deformities encompass a variety of etiologies often requiring multi-level arthrodesis from the thoracic spine to the pelvis.2,3 Although these complex surgeries have shown to improve HRQOL postoperatively, high complication rates coupled with a long recovery period call into question whether prognostic factors that are associated with improved PROMs can be determined.4-6
Treatment efficacy for ASD patients is typically assessed based on subjectively reported outcomes. To understand this further, healthcare professionals and statisticians alike work to coin what the minimal clinically important difference (MCID) is in where both professionals and patients can perceive improvement through a quantitative perspective. Minimal clinically important difference can be defined as the threshold that represents an improvement from baseline that is meaningful enough that the patient would consider repeating the intervention if they were hypothetically in a similar condition.6-8 The Scoliosis Research Society-22r (SRS-22r) is a PROM used in all etiologies of ASD. Its validity, reliability, and representativeness of all treatment effects has been well documented.9-12 The EuroQol5 (EQ-5D) is a generic measurement aimed to evaluate all measures of HRQOL such as mobility, self-care, usual activity, pain, and anxiety. 13
Despite the wide-use and demonstrated effectiveness of the stated PROMs in capturing HRQOL measures, patient and surgical characteristics that affect achieving MCID require further research. It is estimated that the prevalence of ASD in the elderly population is up to 68%, which with time may lead to further deterioration of the patient’s quality of life.14,15 The purpose of this study is to identify independent prognostic factors that are associated with improved PROMs and achieving MCID among ASD patients ≥60 years of age undergoing ASD primary reconstructive surgery.
Methods
A prospective, multicenter, multi-continental, observational longitudinal cohort study was conducted of patients aged ≥60 years undergoing primary spinal deformity surgery consisting of having ≥5 levels fused. The clincialtrials.gov identifier is: NCT02035280.
Patients were included in the study if they were ≥60 years by the date of surgery, diagnosed with a spinal deformity in either the coronal or sagittal plane undergoing ≥ 5-level spinal fusion, willing to comply with the protocol’s follow-up schedule, and understood and signed the informed consent (IRB - AAAQ2318). Patients were excluded from the study if they had any previous spinal procedures except for a prior decompression of ≤2 levels, diagnosed with a neurogenerative disease or paralysis, unlikely to comply with follow-up, were institutionalized or prisoners, medically unfit, recent history of substance abuse, psychosocially disturbed, presence of an active tumor or infection, had a recent history of tumor or fracture of the spine, or participated in other studies that could potentially influence the results of the current study.
Demographic variables such as, age, gender, height, weight, body mass index (BMI), race, employment, and American Society of Anesthesiologists (ASA) grade, were collected.
Local investigators were tasked with screening incoming patients and included them for eligibility. Local surgeons operated on said patients based on their standard of care utilizing surgical techniques based on their experiences and discretion. Patients were then reviewed and completed outcome instruments at baseline, 10 weeks, 12 months, and 24 months postoperatively. Radiographic images (3 foot, antero-posterior, and lateral) were acquired pre-operatively, at discharge, and after 24 months to assess the following radiographic parameters: lumbar lordosis, thoracic kyphosis, sagittal vertical axis (SVA), and the major Cobb angle.
The primary outcome of interest in this study is the change in the Scoliosis Research Society-22r (SRS-22r) subtotal score between baseline and the 24-month follow-up visit to achieve the MCID. The SRS-22r subtotal score only includes the function, pain, self-image, and mental health domains. In addition to the SRS-22r subtotal score, the satisfaction domain was analyzed separately to assess for factors that are associated with improved satisfaction with surgery at the 2-year follow-up visit. The secondary outcome of interest is the change in the EuroQol5 (EQ-5D) between baseline and the 24-month follow-up visit to achieve the MCID.
Statistical Methodology
Minimal clinically important difference was used to dichotomize the patient population into 2 separate groups: those who reached MCID and those who did not. Three approaches were used to assess the most optimal methodology to assess MCID: (1) an absolute change defined as a .5 point increase in the SRS-22r sub-total and a .18 point increase in the EQ-5D index 16 ; (2) a relative change defined as a 15% increase in the SRS-22r sub-total and a 15% increase in the EQ-5D index. 15% was chosen for this approach as it generated the closest value to the observed mean change to baseline of both the SRS-22r and EQ-5D and for the sake of comparison with the absolute change approach to have similar MCID groups repartition; (3) using the predictive model designed by Scheer et al, a relative change with a cut-off in the outcome at baseline defined as a 15% increase in the SRS-22r sub-total score and a baseline score ≤3.2 and a 15% increase in the EQ-5D index and baseline index ≤.7. 17 These cutoff points were implemented to exclude patients who already possess a good baseline condition and represented the third quartile of each outcome in the patient cohort.
First, descriptive statistics were used to observe the repartition of all the demographical, clinical, and adverse event (AE) parameters among patients who reached MCID and those who did not for each of the 3 approaches. Adverse events were stratified between medically and surgically related. The severity of the AE was determined by the investigator at each independent site
Results
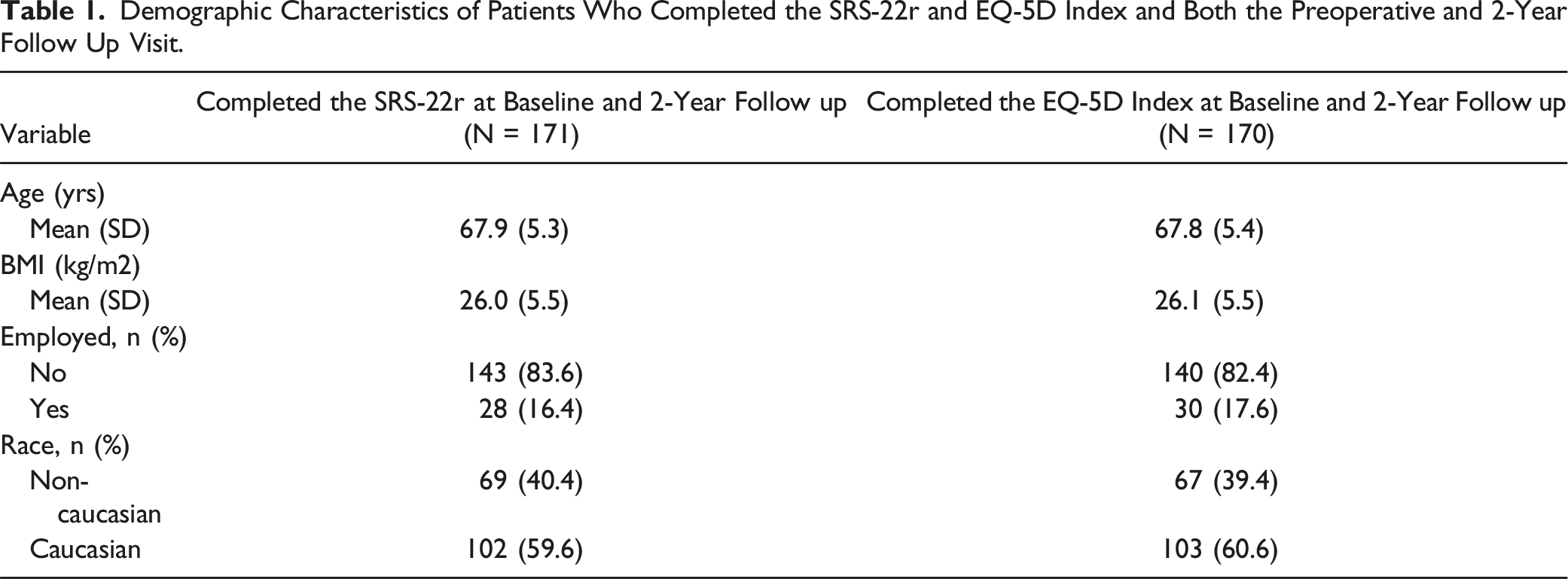
255 patients were enrolled in the PEEDS study; 26 patients were excluded for screening failure, surgery cancelation, or for other reasons pertaining to the criteria set by the study. Of the 229 patients that remained, 219 patients met the inclusion and none of the exclusion criteria for this study. Of the 219 patients, 171 patients completed the SRS-22r at baseline and at the 2-year follow-up visit, and 170 patients completed the EQ-5D during the same time period. Only patients who completed the questionnaires at baseline and the 2-year follow-up visit were included in this analysis (Figure 1). Demographical characteristics for both cohorts are summarized in Table 1. Patient attrition diagram demonstrating the patients included in the analysis. Demographic Characteristics of Patients Who Completed the SRS-22r and EQ-5D Index and Both the Preoperative and 2-Year Follow Up Visit.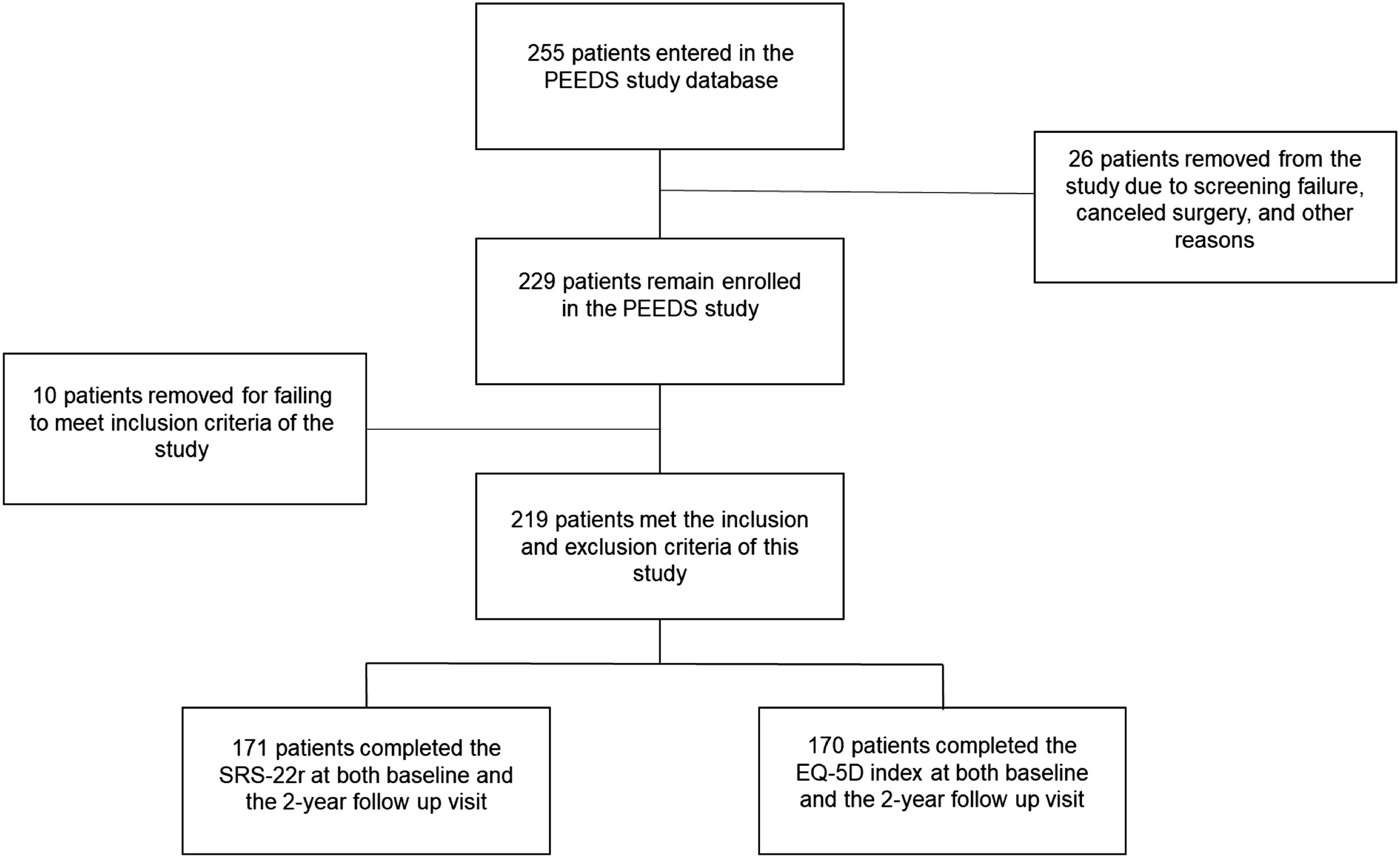
SRS-22r Sub-Total Score and Satisfaction Domain
Absolute MCID
Comparison of Demographics Parameters for the Identification of Predictive Factors Associated Achieving MCID Across All 3 Approaches.
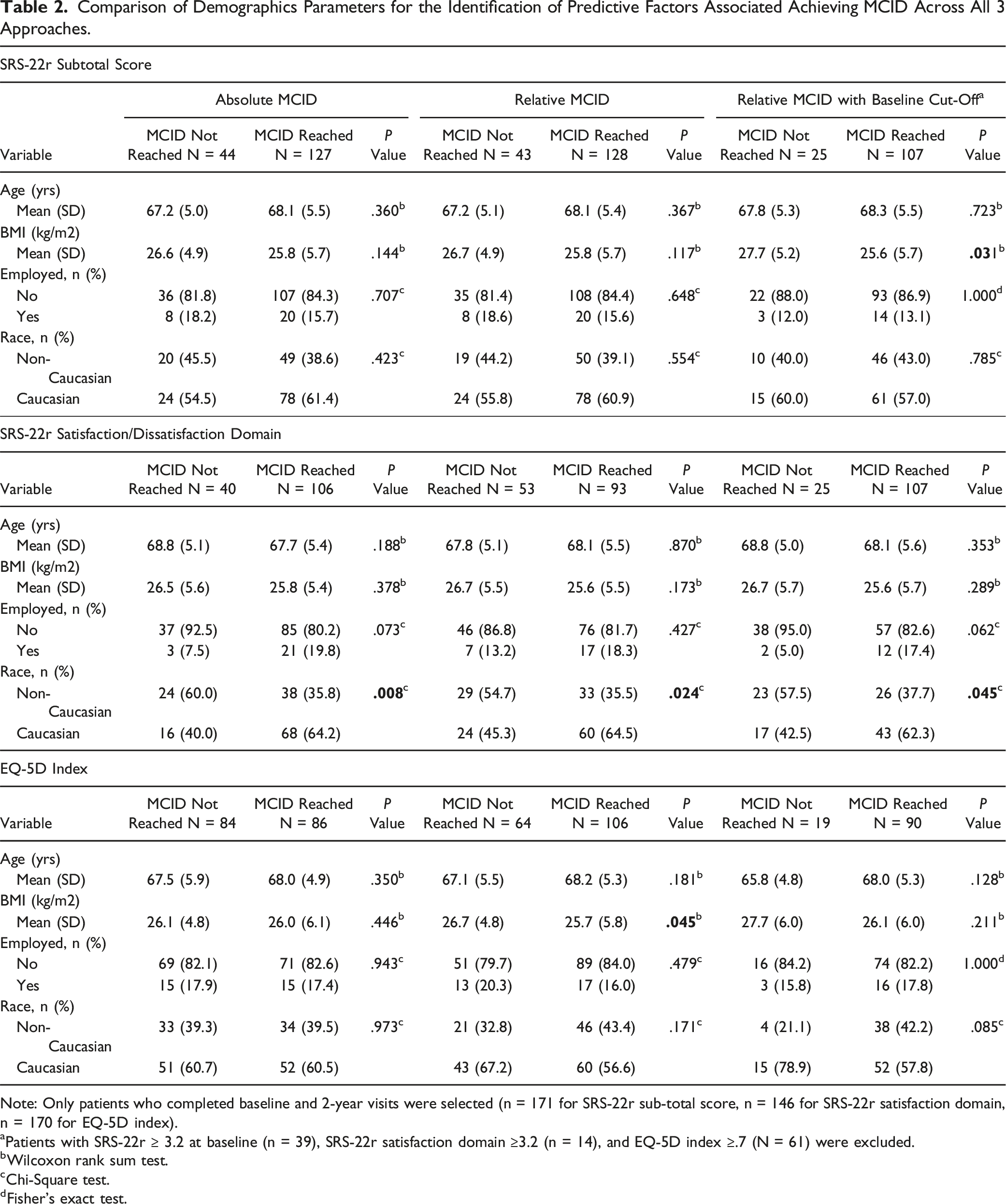
Note: Only patients who completed baseline and 2-year visits were selected (n = 171 for SRS-22r sub-total score, n = 146 for SRS-22r satisfaction domain, n = 170 for EQ-5D index).
aPatients with SRS-22r ≥ 3.2 at baseline (n = 39), SRS-22r satisfaction domain ≥3.2 (n = 14), and EQ-5D index ≥.7 (N = 61) were excluded.
bWilcoxon rank sum test.
cChi-Square test.
dFisher’s exact test.
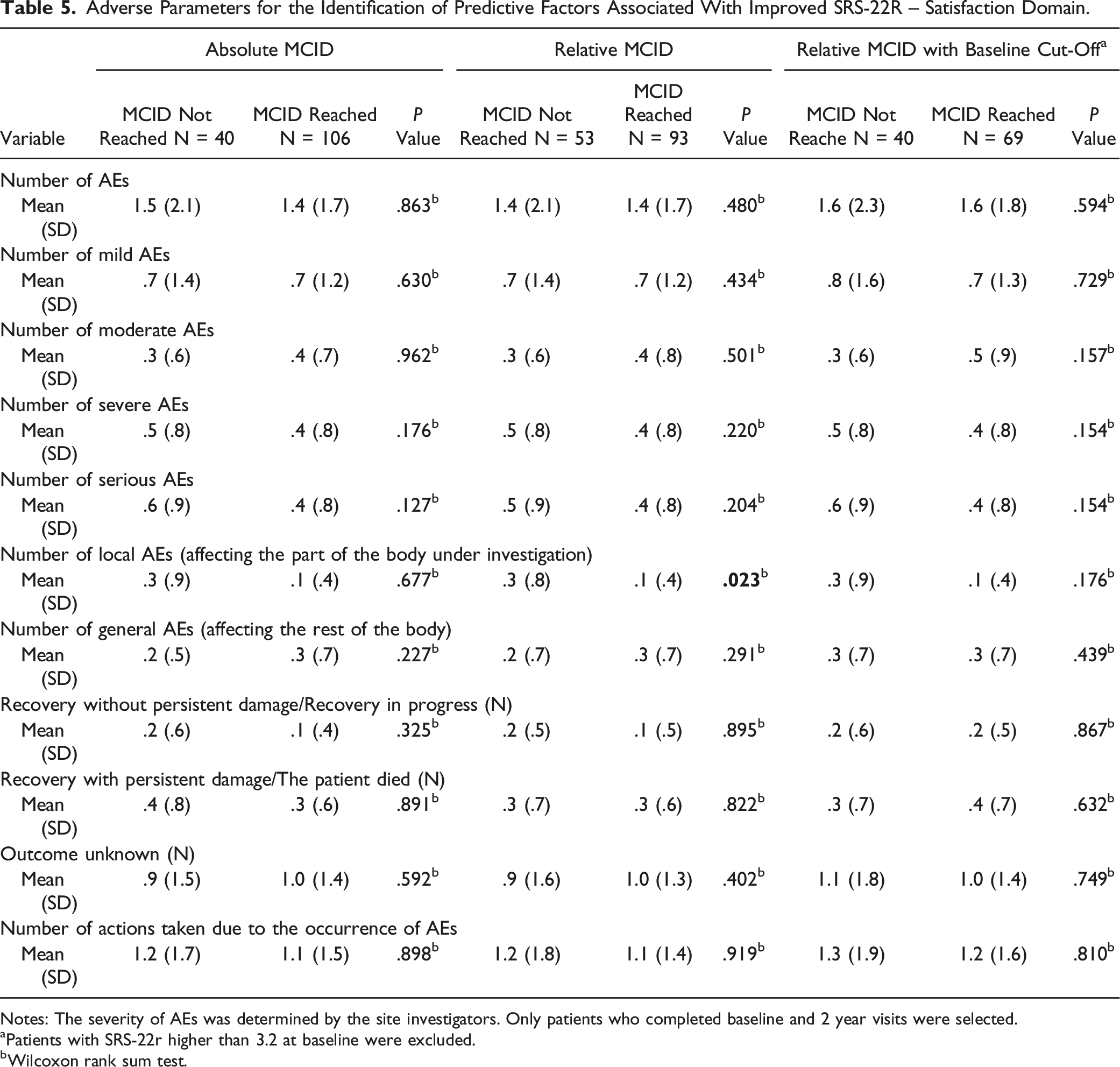
Adverse Parameters for the Identification of Predictive Factors Associated With Improved SRS-22R.
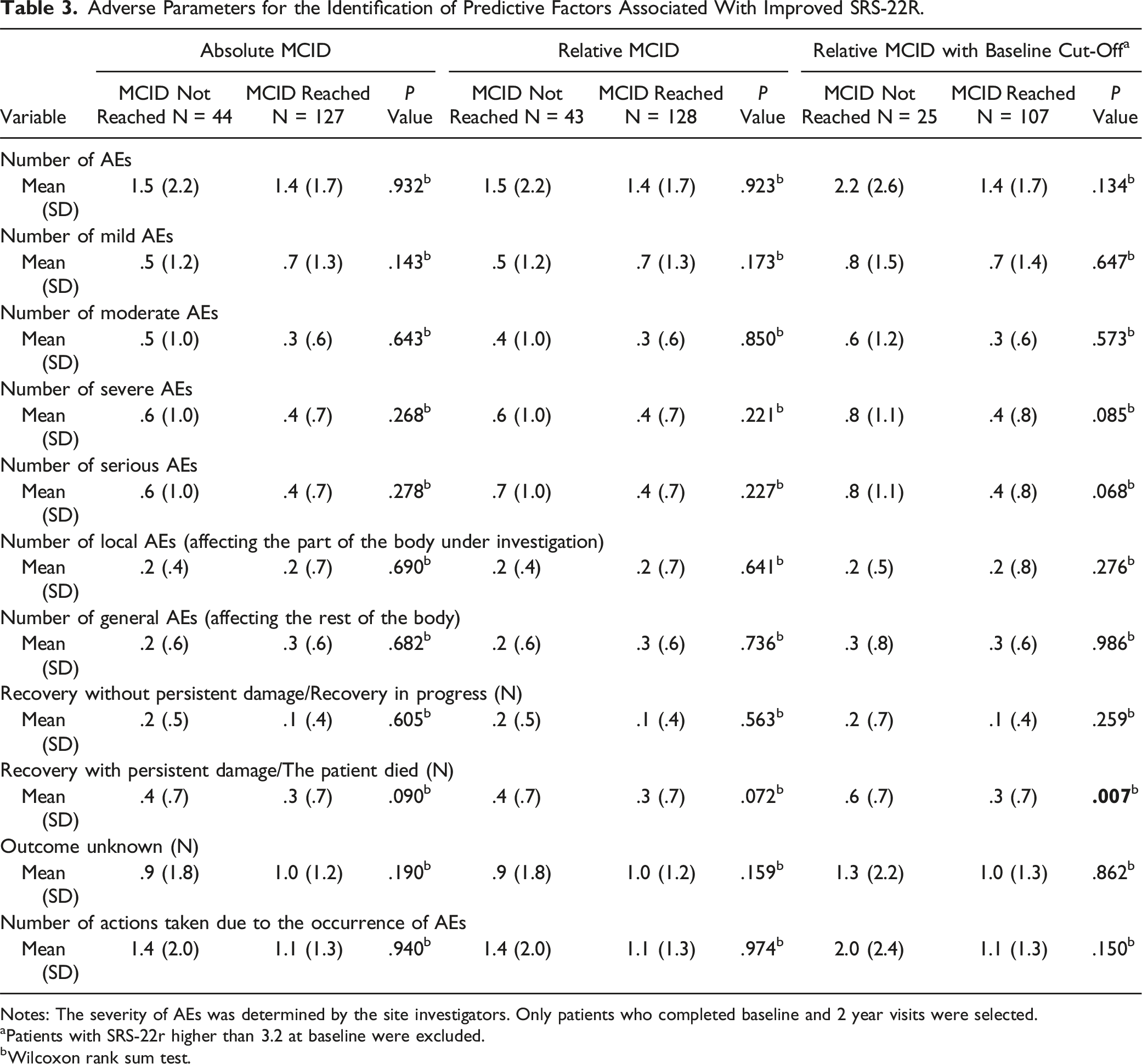
Notes: The severity of AEs was determined by the site investigators. Only patients who completed baseline and 2 year visits were selected.
aPatients with SRS-22r higher than 3.2 at baseline were excluded.
bWilcoxon rank sum test.
Stepwise Selection in the Multivariate Logistic Regression to Identify the Most Relevant Continuous Risk Factors Associated With Achieving MCID a in the SRS-22r Outcome and EQ-5D Index at 2 Years.
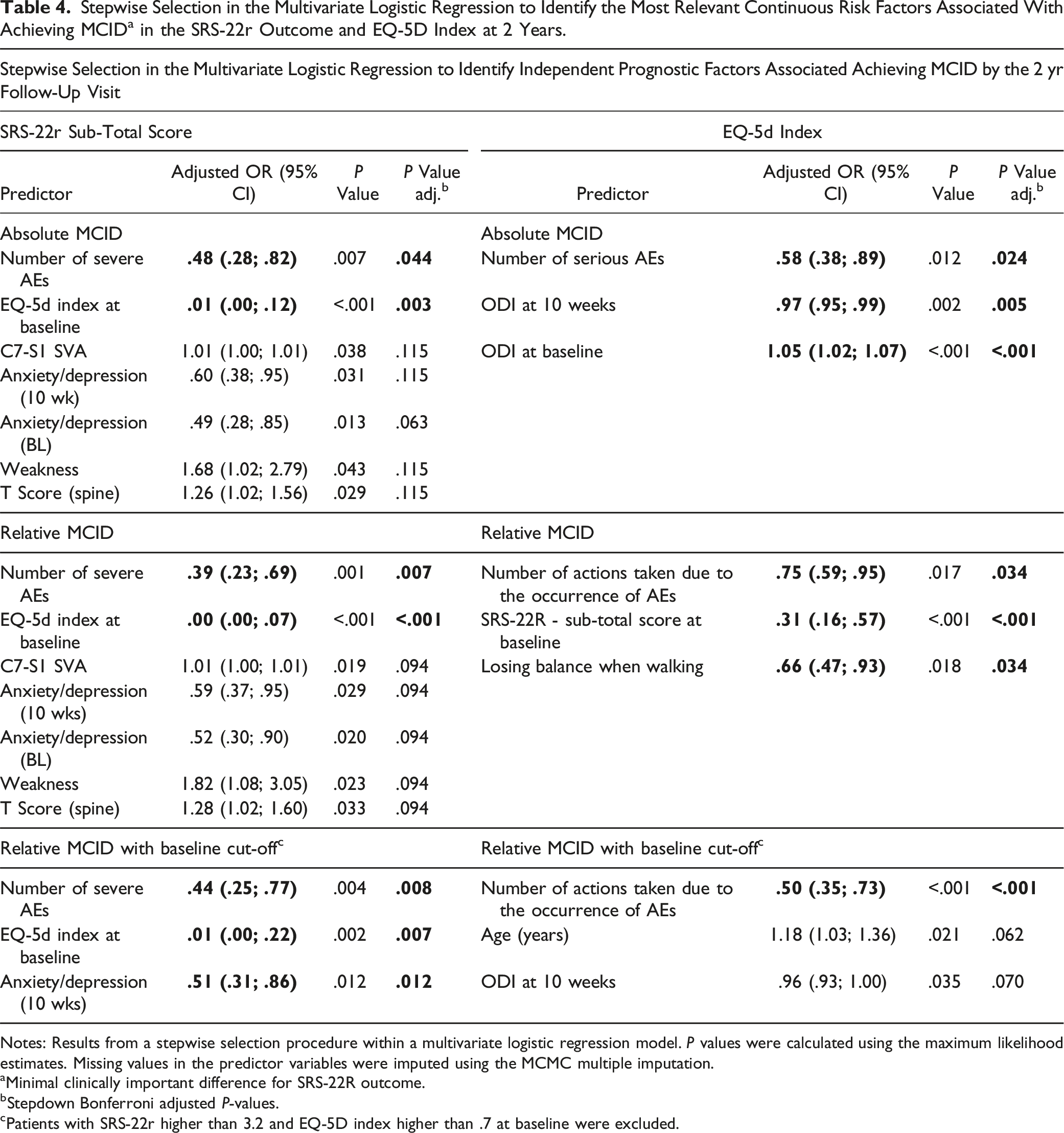
Notes: Results from a stepwise selection procedure within a multivariate logistic regression model. P values were calculated using the maximum likelihood estimates. Missing values in the predictor variables were imputed using the MCMC multiple imputation.
aMinimal clinically important difference for SRS-22R outcome.
bStepdown Bonferroni adjusted P-values.
cPatients with SRS-22r higher than 3.2 and EQ-5D index higher than .7 at baseline were excluded.
Adverse Parameters for the Identification of Predictive Factors Associated With Improved SRS-22R – Satisfaction Domain.
Notes: The severity of AEs was determined by the site investigators. Only patients who completed baseline and 2 year visits were selected.
aPatients with SRS-22r higher than 3.2 at baseline were excluded.
bWilcoxon rank sum test.
Stepwise Selection in the Multivariate Logistic Regression to Identify the Most Relevant Continuous Risk Factors Associated Achieving Mcid a in the SRS-22r – Satisfaction Domain the Management Outcome at 2 Years.
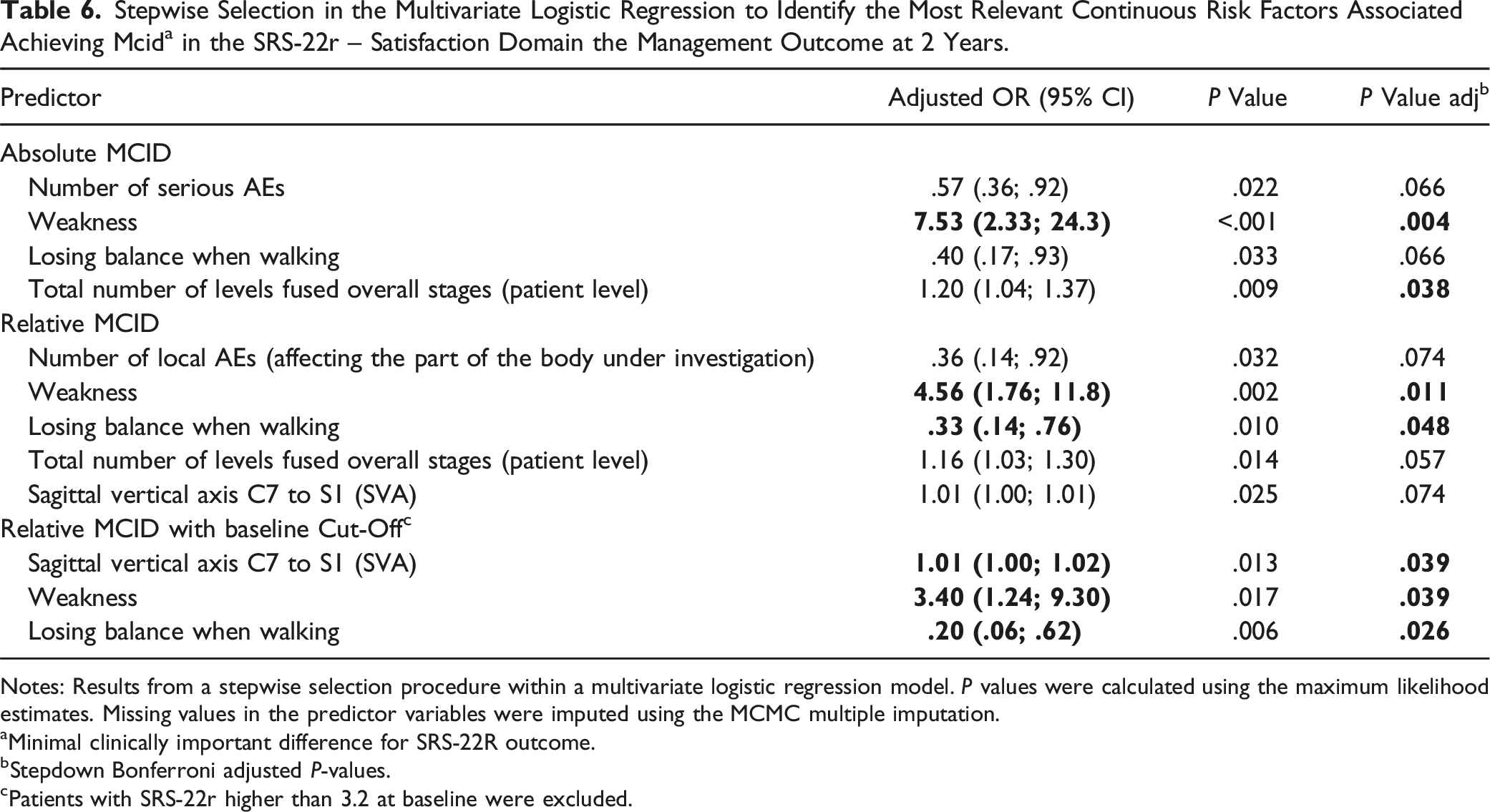
Notes: Results from a stepwise selection procedure within a multivariate logistic regression model. P values were calculated using the maximum likelihood estimates. Missing values in the predictor variables were imputed using the MCMC multiple imputation.
aMinimal clinically important difference for SRS-22R outcome.
bStepdown Bonferroni adjusted P-values.
cPatients with SRS-22r higher than 3.2 at baseline were excluded.
Relative MCID
Using the relative approach to assess MCID, 75% (N = 128) of the patients who completed the SRS-22r at both the preoperative and 2-year follow up visits reached MCID at 2-year postoperative visit. Similarly to the absolute approach, no statistically significant differences were observed among the demographic parameters between the 2 groups
Stepwise selection in the multivariate logistic regression demonstrated that the number of severe AE’s (OR = .39, 95% CI: .23 – .69, P = .007) and the EQ-5D index at baseline (OR: .00, 95% CI: .00 – .07, P < .001) were the only factors associated with reaching MCID at 2 years postoperative (Table 4).
Regarding the satisfaction domain, 64% of patients reached MCID. Caucasian patients remained over-represented amongst patients who reached MCID compared to patients who didn’t (64.5% vs 45.3%, P = .024)
Stepwise selection in the multivariate logistic regression model demonstrated that preoperative weakness (OR = 4.56, 95% CI: 1.76 – 11.8, P = .011) and losing balance while walking (OR = .33, 95% CI: .14 – .76, P = .048) were the only factors associated with reaching MCID in the satisfaction domain at 2 years postoperative (Table 6).
Relative MCID with a Cut-Off at Baseline Score
After excluding the patients with a good baseline condition (SRS-22r sub-total score >3.2), 132 patients remained in the analysis. Of those patients, 81% (N = 107) reached MCID at the 2-year visit. Patients who reached MCID possessed a lower BMI (25.6 ± 5.7 vs 27.7 ± 5.2, P = .031)
Stepwise selection in the multivariate logistic regression demonstrated that the number of severe AE’s (OR = .44, 95% CI: .25 – .77, P = .008), the EQ-5D index at baseline (OR: .01, 95% CI: .00 – .22, P = .007), and being anxious at 10 weeks (OR = .51, 95% CI: .31 – .86, P = .012) were the only factors associated with reaching MCID at 2 years postoperative (Table 4).
Regarding the satisfaction domain, 63% of patients reached MCID. Caucasian patients remained over-represented amongst patients who reached MCID compared to patients who didn’t (62.3% vs 42.5%, P = .045)
Stepwise selection in the multivariate logistic regression model demonstrated that the SVA (OR = 1.01, 1.00 – 1.02, P = .039), preoperative weakness (OR = 3.40, 95% CI: 1.24 – 9.39, P = .039), and losing balance while walking (OR = .20, 95% CI: .06 – .62, P = .026) were the only factors associated with reaching MCID at 2 years postoperative
EQ-5D Index
Absolute MCID
Adverse Parameters for the Identification of Predictive Factors Associated With Improved EQ-5D Index.
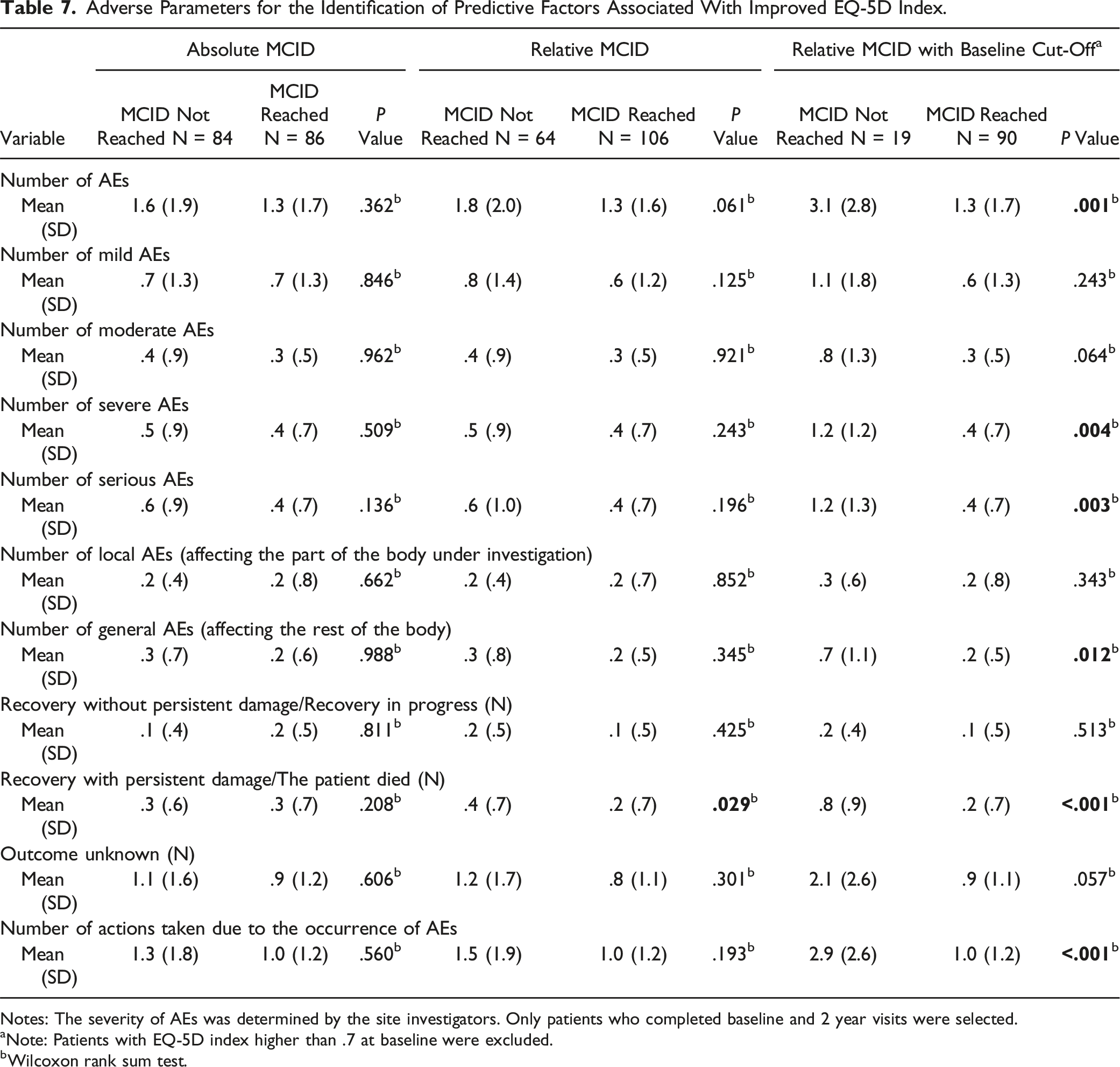
Notes: The severity of AEs was determined by the site investigators. Only patients who completed baseline and 2 year visits were selected.
aNote: Patients with EQ-5D index higher than .7 at baseline were excluded.
bWilcoxon rank sum test.
Stepwise selection in the multivariate logistic regression, after adjusting variables with P < .2 resulting from univariate analyses, demonstrated that the number of severe AE’s (OR = .58, 95% CI: .38 – .89, P = .024), ODI score at 10 weeks (OR = .97, 95% CI = .95 – .99, P = .005), and ODI score at baseline (OR = 1.05, 95% CI: 1.02 – 1.07, P < .001) to be the only factors associated with reaching MCID at 2 years postoperative (Table 4).
Relative MCID
Using the relative approach to assess MCID, only 62% (N = 106) of patients who completed the EQ-5D index reached MCID at the 2-year visit. Patients who reached MCID possessed a lower BMI (25.7 ± 5.8 vs 26.7 ± 4.8, P = .045). However, no other statistically significant differences were observed among the demographic parameters between the 2 groups
Stepwise selection in the multivariate logistic regression demonstrated that the number of actions taken due to the occurrence of AE’s (OR = .75, 95% CI: .59 – .95, P = .034), the SRS-22r sub-total score at baseline (OR = .31, 95% CI: .16 – .57, P < .001) and losing balance while walking (OR = .66, 95% CI: .47 – .93, P = .034) to be the only factors associated with reaching MCID at 2 years postoperative
Relative MCID With a Cut-Off at Baseline Score
After excluding the patients with a good baseline condition (EQ-5D index >.7), 109 patients remained in the analysis. Of those patients, 83% (N = 90) reached MCID at the 2-year visit. No statistically significant differences were observed among the demographic parameters between the 2 groups
Stepwise selection in the multivariate logistic regression demonstrated that the number of actions taken due to the occurrence of AE’s (OR = .50, 95% CI: .35 – .73, P < .001) to be the only factor associated with reaching MCID at 2 years postoperative
Discussion
This study examined the predictive factors associated with achieving MCID in the SRS-22r subtotal score, SRS-22r satisfaction domain, and the EQ-5D index using 3 distinct approaches: absolute MCID, relative MCID, and relative MCID with an imposed baseline cut-off score. Regardless of the approach used in this analysis, we found no radiological or surgical parameters to be identified as prognostic factors for the SRS-22r subtotal score and the EQ-5D index. Instead, the severity of AEs and the EQ-5D index at baseline appeared to be the most influential factors of an improved SRS-22r sub-total score. This was further emphasized by the stepwise multivariate logistic regression model which demonstrated that patients are less likely to reach MCID in the SRS-22r sub-total score given a high number of severe AEs or a high EQ-5D index at baseline.
Comparatively, Arima et al found that the preoperative SRS-22r sub-total score along with a variety or radiographic parameters to be predictive of achieving MCID at the 2-year follow-up period. 6 Despite the variation in the predictive factors, the authors similarly concluded that a poor preoperative HRQOL score at baseline was a significant predictor in achieving MCID. This finding suggests that patients with low baseline scores experience greater improvement resulting from the surgery.
Nonetheless, the analysis conducted by Arima et al was limited to patient demographics, radiographic parameters, and PROMs and did not account for the occurrence of AEs during the postoperative period. On the contrary, the analysis conducted in this study incorporated demographics variables, AEs, clinical parameters such as baseline and 10 weeks PROMs, comorbidities as well as the radiographic and surgical parameters, in our multivariate model all at once. As a result, we observed the effect size surrounding the severity of AEs to remain consistent across all 3 approaches. The perception of AEs plays a significant role in subjective outcomes. In a comparison study of the perception of AEs, Hart et al found that, in general, patients’ perception on the impact and severity of AEs on postoperative outcomes was greater than that of the surgeons. 18 As PROMs rely on the subjective assessment of the patient’s recovery, it is no surprise that the occurrence of severe AEs may serve as a preventative in achieving MCID.
After excluding patients with a good baseline condition, SVA and weakness/losing balance while walking were found to be the only predictive factors of achieving MCID in the SRS-22r satisfaction domain. It is worth noting that the SVA was identified to be the only radiographic parameter to be associated with achieving MCID and was not associated with achieving MCID in the overall SRS-22r sub-total score. Previous studies have demonstrated the association between HRQOL and sagittal alignment suggesting that patients with positive sagittal imbalance reported worse self-assessments in pain, function, and self-image domains as they experience greater imbalance and risk while walking.19-21 We demonstrated that patients who achieved MCID in this domain tended to have a more invasive surgery as highlighted by the higher number of vertebral levels fused. Requiring extensive instrumentation and pelvic fixation has shown to reduce mobility around the waist.22-24 Despite the imposed physiological restrictions, it is understandable as to why correction in the sagittal plane can serve as a predictor for reaching MCID in the satisfaction domain. By implying the cut-off approach, patients are more likely to be maligned in the sagittal plane and possess far more room for improvement. Improvement of sagittal alignment tends to improve the patient’s ability to walk with balance and perform other activities of daily life. 25 Patients are more likely to be satisfied with the outcome of their surgery after witnessing improvements in standing, reduced pain, and enhanced walking ability. 26
In almost every approach taken for assessing MCID, greater pain at baseline, number of actions taken due to the occurrence of AE’s, or both has been significantly associated in achieving MCID in the EQ-5D index. Ibrahim et al assessed the outcomes and life improvements among elderly patients undergoing multilevel spinal fusion to determine the factors associated with MCID of multiple HRQOL measures including the EQ-5D index. Resembling the absolute MCID approach used in this analysis, Ibrahim et al utilized the MCID criteria coined by Parker et al of a .15 increase in the EQ-5D index.27,28 The authors found that increased activity preoperatively and a longer length of stay to be correlated with improvement in EQ-5D index. An explanation to this can be that patients with low a baseline EQ-5D index are more likely to undergo a more complex procedure resulting in a longer length of stay and evidently have greater room for improvement.6,27 In contrast, longer and more complex surgeries are associated with higher rates of AEs which were not accounted for in the aforementioned study. 29 Although the EQ-5D index score itself at baseline was not seen to be a predictive factor for the outcome of interest in any of the approaches, our analysis demonstrated that in the absolute and relative approaches, a higher ODI score and lower SRS-22r sub-total score at baseline, respectively, are associated with achieving MCID in the EQ-5D index. This finding indicates the possibility of improvement given poor baseline scores. Decreased number of AEs in the absolute approach and actions taken in the occurrence of AEs in both the relative and relative/cut-off approach were associated with achieving MCID, addressing the effect of AEs which was not previously mentioned by Ibrahim et al.
With the complication rate of ASD surgery ranging from 40% to 71%, it is no surprise that the occurrence of AEs and their severity may hinder a patient’s postoperative recovery and achieving MCID.30-32 Nonetheless, the effects of AEs on PROMs have been investigated in prior studies. Carreon et al reported serious AEs in addition to the maximum preoperative cobb angle as predictive factors of a lower 2-year SRS-22r score. 33 Although this analysis did not find any radiographic parameters to be predictive of MCID, this may be attributed to the homogeneity of the PEEDs cohort as demonstrated by lack of significant differences in radiographic characteristics, comorbidities, and surgical variables such as ASA grade across all 3 approaches. In addition, Nunez-Pereira et al demonstrated that patients who were operated on due to severe complications within the first year did not reach MCID in both the SRS-22 and ODI by 2 years postoperatively. 34 Reoperation was not assessed in the analysis, however, severe surgically related AEs that may indicate the need for reoperation were incorporated in our models and demonstrated significance. Hence, the notion that AEs and their associated impacts are predictive of achieving MCID is supported thus requiring surgeons to be attentive to modifiable factors that may limit them.
This study is not without limitations. First, despite the extensive collaboration between centers, the study lacked standardization in surgical indications, techniques, and peri-operative management to the patients included in this cohort. Surgical approach and overall care may have differed across centers possibly affecting patients’ postoperative recovery and, as a result, their subjective outcomes. In addition, assessing the severity of AEs was at the discretion of each site investigator for their respective patients. This introduces a subjective element in how patient outcomes are categorized. Secondly, as part of the exclusion criteria, patients who were deemed medically or psychologically unfit were not enrolled. This may have inadvertently introduced a selection bias as this cohort of patients may be healthier than what is deemed representative of the study population. Thirdly, physical activity was not analyzed in this analysis despite physical function being a subdomain of the SRS-22r. Jakobsson et al suggested that patients who started with a low level of preoperative physical activity are more likely to increase their activity postoperatively. This is due to the fact that those who experienced a sedentary life prior to surgery are more likely to experience the health-enhancing benefits of physical activity after surgery possibly increasing their odds of achieving MCID. 35 Further research into physical activity and its association with reaching MCID would be beneficial. Lastly, there is greater risk and cost associated with ASD surgery. Thus, MCID may not be an applicable measure of overall patient improvement. Other methodologies to assess patient improvement such as substantial clinical benefit (SCB) and patient acceptable symptomatic state (PASS) should be explored.
Conclusion
In this large multicenter prospective cohort of elderly patients undergoing primary reconstructive surgery for ASD, our analysis across all 3 approaches, demonstrated that the baseline condition of the patient and AE severity seemed to be the most predictive factors for reaching MCID. Patients who experience more pain and discomfort at baseline are more likely to reach MCID as they have more room for improvement. Meanwhile, patients that experience severe AEs are less likely to reach MCID as their occurrence may impede the patient’s postoperative progress. No clinical, radiological, or surgical parameters were identified as factors that can be prognostic for reaching MCID suggesting that patient perception may be more indicative to whom will benefit from surgery. The finding that AEs and their associated impacts are predictive of achieving MCID offers guidance regarding possible modifiable factors to limit such events.
Supplemental Material
Supplemental Material - Independent Prognostic Factors Associated With Improved Patient-Reported Outcomes in the Prospective Evaluation of Elderly Deformity Surgery (PEEDS) Study
Supplemental Material for Independent Prognostic Factors Associated With Improved Patient-Reported Outcomes in the Prospective Evaluation of Elderly Deformity Surgery (PEEDS) Study by Fthimnir M. Hassan, Lawrence G. Lenke, Sigurd H. Berven, Michael P. Kelly, Justin S. Smith, Christopher I. Shaffrey, Benny T. Dahl, Marinus de Kleuver, Maarten Spruit, Ferran Pellise, Kenneth M. C. Cheung, Ahmet alanay, David W. Polly Jr., Jonathan Sembrano, Yukihiro Matsuyama, Yong Qiu, Stephen J. Lewis, and AO Spine Knowledge Forum Deformity in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards (IRB - AAAQ2318).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.