
Abstract
Introduction
Social determinants of health have been shown to influence various outcome measures after elective orthopaedic procedures, including spine surgery. However, there has been limited research investigating the influence between social determinants of health and healthcare resource utilization after elective spine surgery. The purpose of this study was to investigate the influence of social vulnerability on opioid use, healthcare utilization, and patient-report outcome measures (PROMs) after elective lumbar decompression procedures.
Methods
Patients undergoing elective 1- or 2- level lumbar decompression procedures between 2013 and 2018 at a single tertiary medical center were retrospectively identified. Various demographic variables, including the ZIP code of residence for each patient were reported. The Centers for Disease Control and Prevention (CDC) Social Vulnerability Index (SVI) scores were calculated for each patient. Social vulnerability was defined as combined socioeconomic and housing vulnerability scores in the upper quartile. Several outcome measures were compared between patients with or without social vulnerability. The outcomes of interest included healthcare utilization and patient-reported outcome measures – pain interference (PI) and physical function (PF) within 1 year postoperatively. Healthcare utilization metrics included opioid use, emergency department visits, urgent care visits, MRI studies, pain management referrals, and revision surgeries. The minimal clinically important difference (MCID) was defined as 8 for both PI and PF scores.
Results
A total of 216 patients were included in the cohort −58 patients met criteria for social vulnerability. Patients with social vulnerability were more likely to be female and ASA class 2. Otherwise, patient demographics and medical comorbidities were similar between the 2 groups. Patients with social vulnerability were more likely to utilize the emergency department within 1-year postoperatively and to have persistent opioid use at both 6 months and 1 year postoperatively. On multivariate regression, SVI was independently associated with pre-operative opioid use, post-operative emergency department utilization, and persistent opioid use after surgery. Relative improvement in PI and PF scores and rates of MCID attainment were similar between groups.
Conclusions
Patients with social disparities were more likely to utilize the emergency department and have persistent opioid use at 6 months and 1 year postoperatively from elective lumbar decompression procedures.
Keywords
Introduction
Social disparities have implications for timely access to healthcare and outcomes. Various factors, including socioeconomic status, housing stability, access to transportation, racial disparities, and language barriers, can significantly affect the quality of medical care and patient outcomes.4-7 There has been increasing interest in the relationship between these social factors and outcomes after surgery, including elective spine surgery. Identifying social barriers that may negatively influence surgical outcomes is an important first step in providing quality healthcare to this vulnerable patient population.
Prior studies have investigated the influence of various social disparities on perioperative outcomes, patient-reported outcomes, and pain management after elective spine surgery.7,12,15,19 Socioeconomic disparities have been associated with worse patient reported outcome measures after spine surgery. 15 Social disparities have been associated with hospital length-of-stay, discharge disposition, and 30-day readmission. 7 Furthermore, lower household income has been associated with higher rates of 3-month opioid script renewal after spine surgery. 2 However, there is a lack of research investigating the influence of social disparities on healthcare resource utilization after elective spine surgery.
Patients experiencing particular social disparities may engage with and perceive the healthcare system in varied and unpredictable ways, especially following major surgical procedures. The purpose of this study is to investigate the relationship between social vulnerability and both healthcare resource utilization and patient-reported outcome measures (PROMs) after elective lumbar decompression procedures at an urban academic center.
Methods & Materials
Data Source
This study was approved by the Institutional Review Board (IRB) at our respective institution. Patients who underwent elective lumbar spine surgery between November 1, 2013, and September 30, 2018, at a single academic institution were retrospectively identified using a deidentified patient-reported outcome measures (PROMs) database. All patients underwent surgery by 1 of 3 fellowship-trained orthopaedic spine surgeons.
Inclusion/Exclusion Criteria
One- and two-level, posterior-based lumbar decompression procedures (eg, laminectomy, laminotomy with discectomy) were included. Only primary elective procedures were included in the analysis. Any procedures performed for tumor, infection, or traumatic indications were excluded. Patients with less than 1 year of follow-up were also excluded. Patients with incomplete follow-up data, including PROMs, were excluded from the analysis. Any revision procedures were excluded from the analysis.
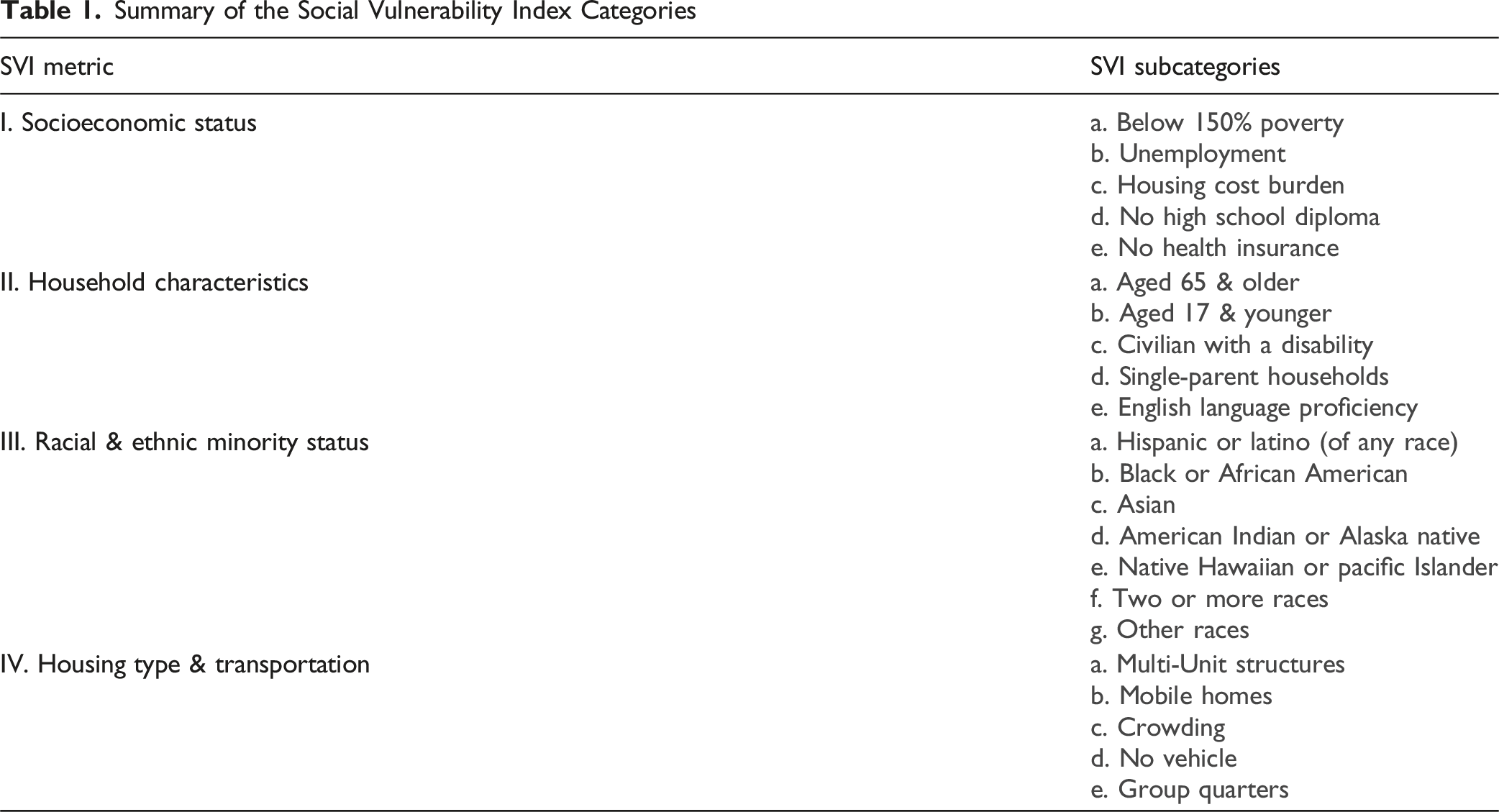
Social Vulnerability Index
Summary of the Social Vulnerability Index Categories
Groups and Variables of Interest
Social vulnerability was defined as a home address in a ZIP code with “socioeconomic status” or “household characteristics” SVI scores in the upper quartile nationally. 1 The other patients were included in the control group. Race/ethnicity, insurance status, and insurance payor type were also reported and included as variables of interest.
Several patient demographics, medical and surgical variables were reported for each patient. Sex, age, body mass index (BMI), Charlson comorbidity index (CCI), and several medical comorbidities were reported for each patient. Age was categorized into the following groups: 18-39 years, 40-49 years, 50-59 years, 60-69 years, 70-79 years, and 80+ years. BMI was categorized into the following groups: underweight (<18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), obese class I (30.0-34.9 kg/m2), obese class II (35.0-39.9 kg/m2), and obese class III (40.0+ kg/m2). Charlson comorbidity index (CCI) was defined as previously described. 24 Medical comorbidities of interest included HIV/AIDS, cerebrovascular disease, chronic pulmonary disease, congestive heart failure, diabetes with or without chronic complications, hemiplegia/paraplegia, malignancy, metastatic solid tumor, mild and moderate or severe liver disease, myocardial infarction, peptic ulcer disease, peripheral vascular disease, renal disease, and rheumatic disease.
Various healthcare utilization metrics within the first year postoperatively were reported and compared between groups. These metrics included emergency department visits, urgent care visits, persistent opioid use, number of opioid prescriptions, post-operative lumbar spine magnetic resonance imaging (MRI) studies, pain management referrals, physical therapy referrals, nerve blocking medication use (eg, gabapentin), epidural injection use, and any revision surgery. Persistent opioid use was defined as any new opioid prescriptions prescribed at the follow-up time point of interest. Pre-operative opioid use within 60 days of surgery was also recorded.
Patient-reported outcome measures (PROMs) – pain interference (PI) and physical function (PF) were also recorded at preoperative baseline and 6 weeks, 3 months, and 12 months postoperatively. The relative change in these metrics from baseline were recorded at each follow-up time point. The absolute scores and the mean change in scores were compared between the groups. The minimal clinically important difference (MCID) was defined as 8 for both PI and PF scores, as previously described in the literature. 29 The percentage of patients achieving MCID at each time point was also reported and compared between groups.
Statistical Analysis
Continuous variables were compared using unpaired t-tests. Categorical variables were compared using Chi-squared analysis or Fisher exact tests when appropriate. Multivariate logistic regression was used to identify any potential variables associated with various outcomes of interest, including pre-operative opioid use, non-home discharge, emergency department visits, urgent care visits, persistent opioid use, post-operative MRI lumbar spine studies, pain management referrals, physical therapy referrals, nerve blocking medication use, and epidural injection use. Additionally, multivariate logistic regression was used to identify any potential variables associated with achieving MCID in the PF or PI scores at 1 year postoperatively. Statistical significance was defined as P < 0.05. All statistical analyses were undertaken using IBM SPSS Version 29.0 (Armonk, NY: IBM Corp).
Results
Patient Demographics and Medical Comorbidities
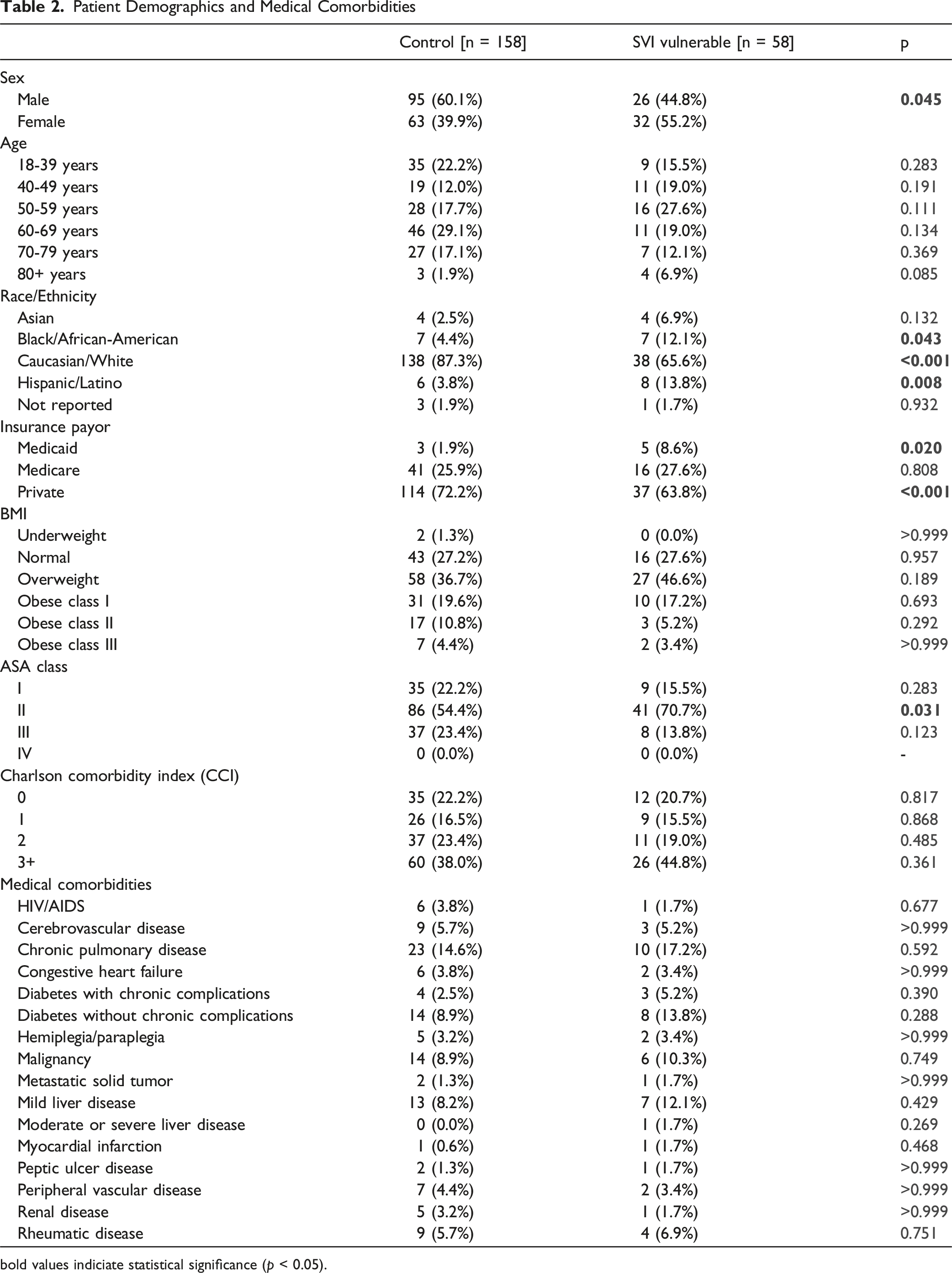
bold values indiciate statistical significance (p < 0.05).
Summary of SVI Scores for the Entire Cohort

aSTD – standard deviation.
Healthcare Utilization Metrics Within 1-Year Post-operatively
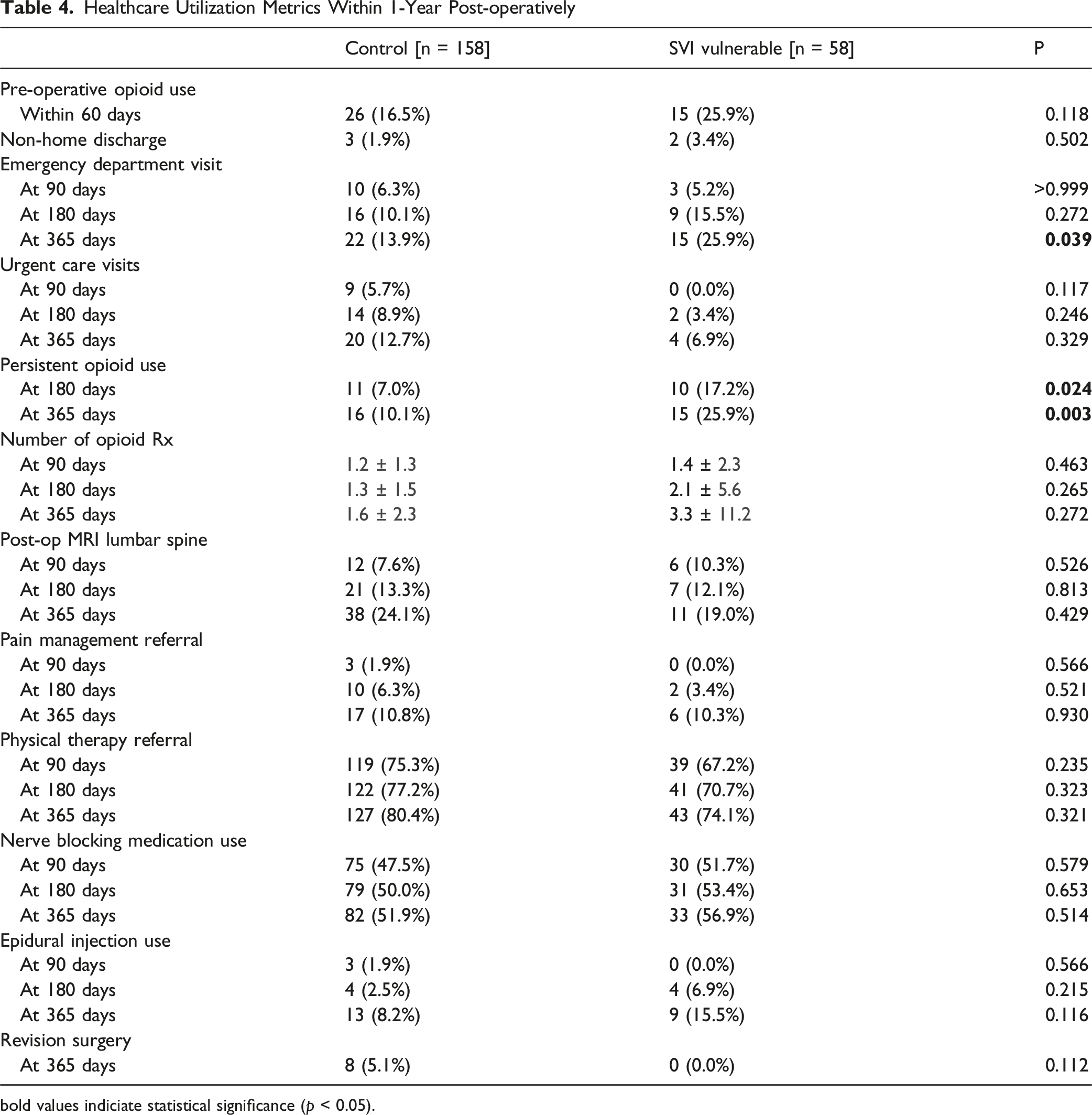
bold values indiciate statistical significance (p < 0.05).
Multivariate Logistic Regression Identifying Independent Risk Factors for Various 1-Year Post-operative Healthcare Utilization Metrics
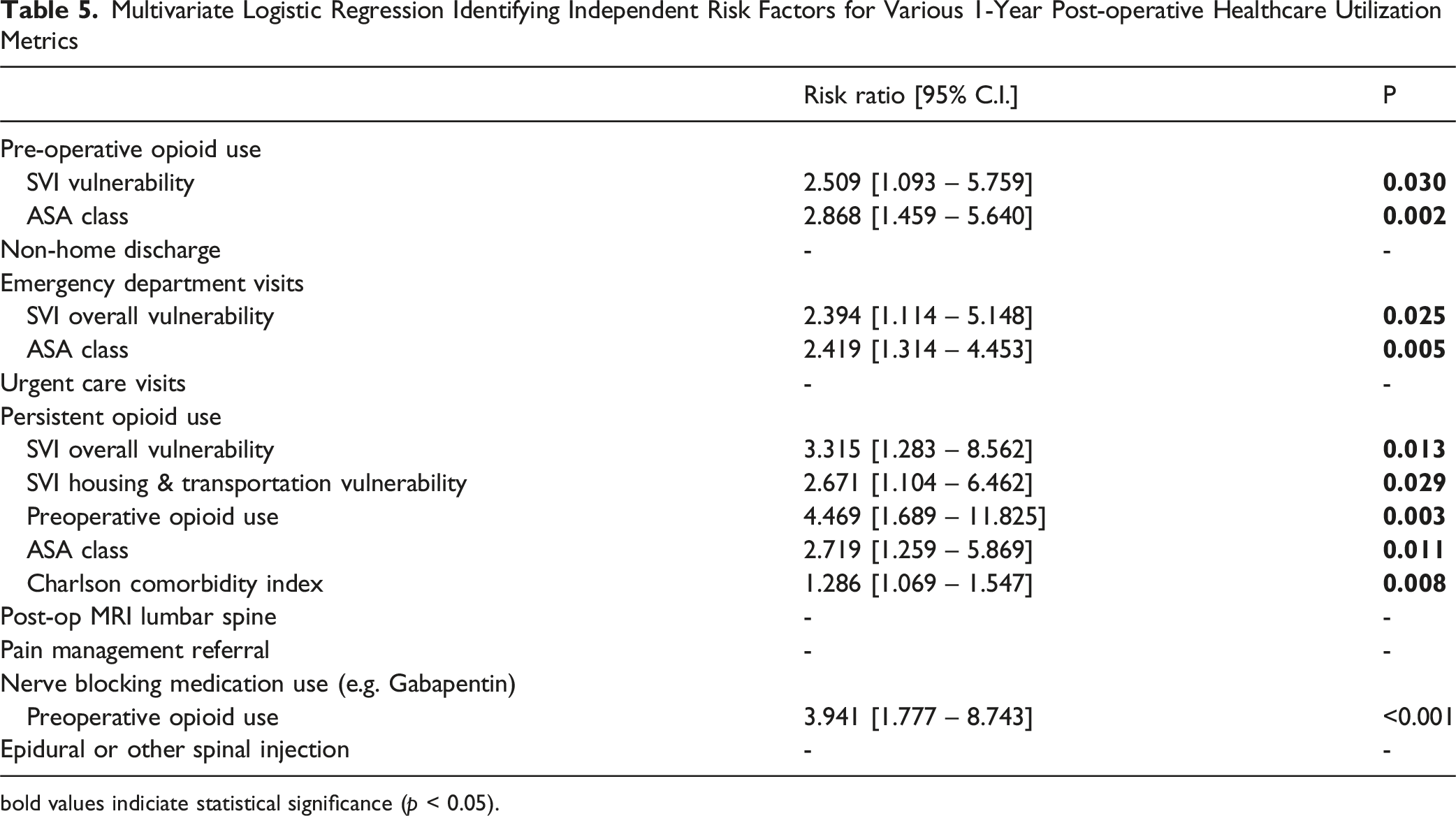
bold values indiciate statistical significance (p < 0.05).
Healthcare Utilization Metrics Within 1-Year Post-operatively for Patients With and Without Preoperative Opioid Use
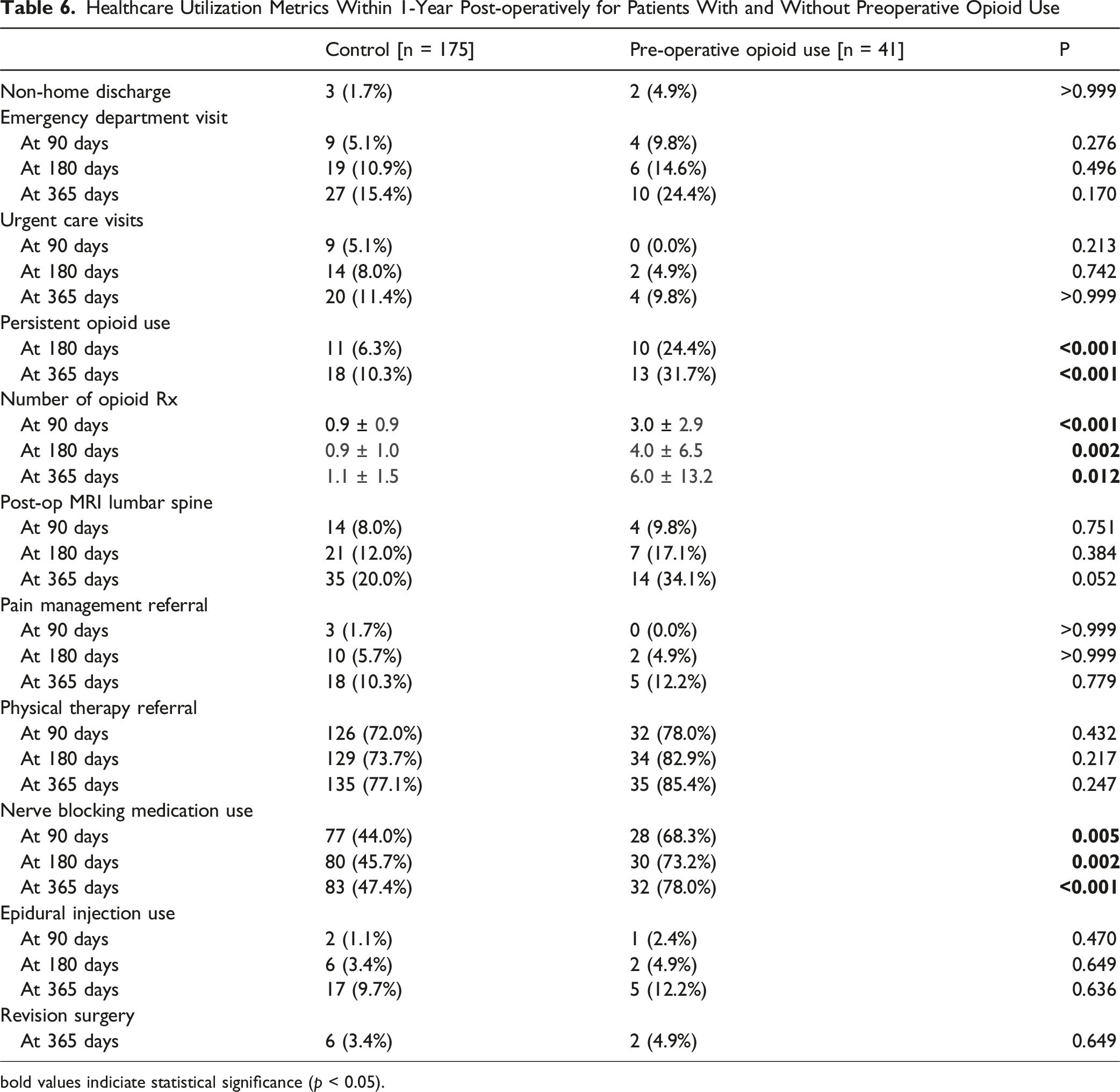
bold values indiciate statistical significance (p < 0.05).
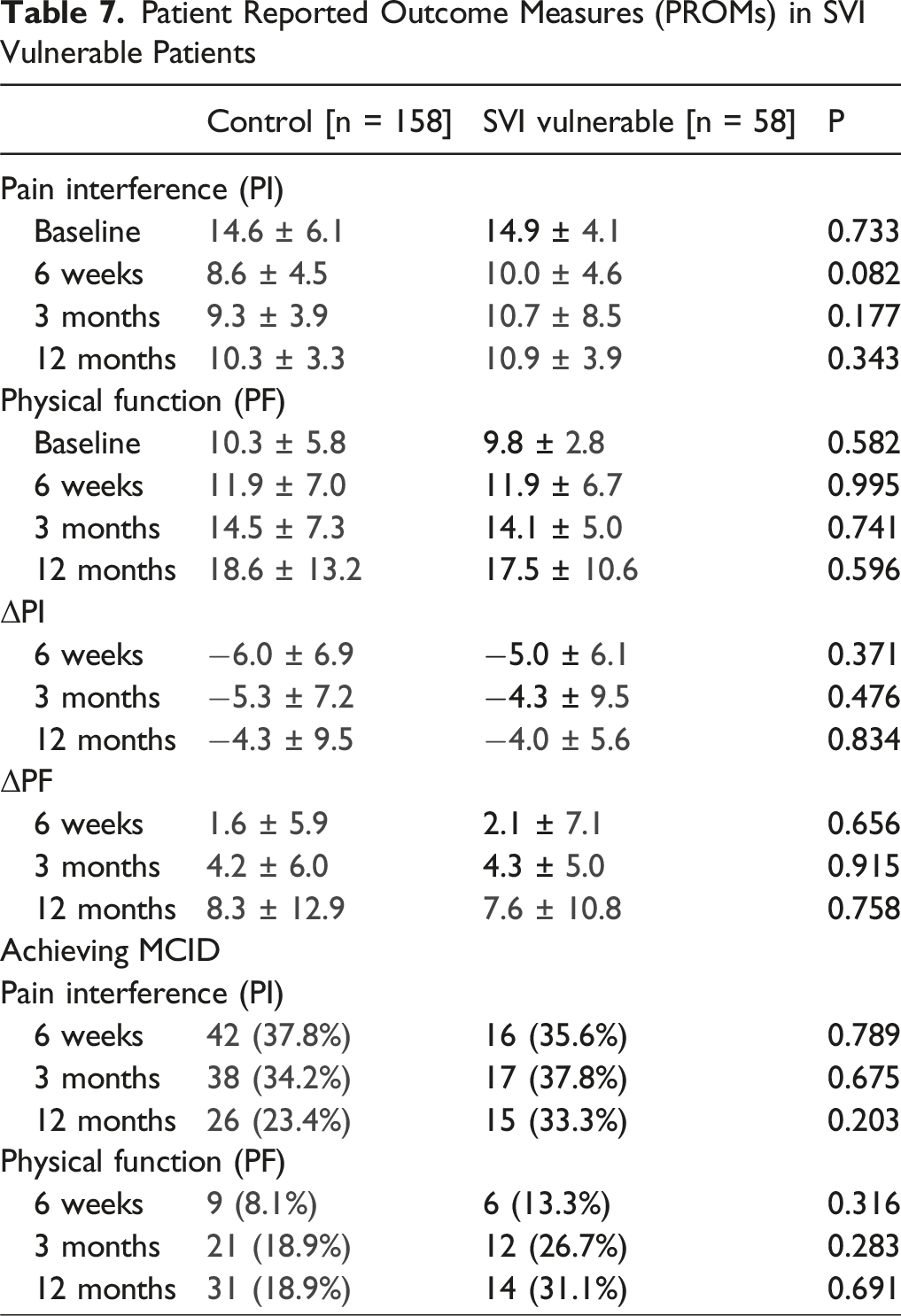
Patient Reported Outcome Measures (PROMs) in SVI Vulnerable Patients
Logistic Regression Identifying Factors Associated With Achieving MCID at 1 year
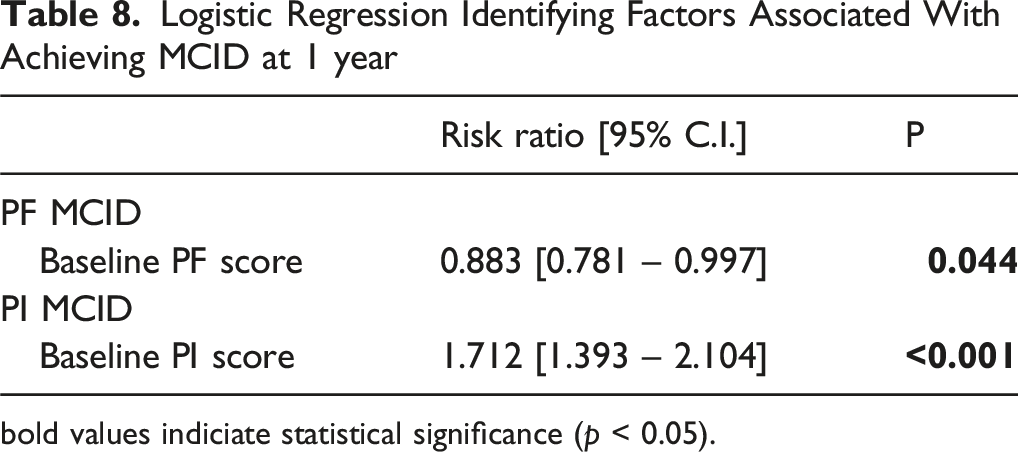
bold values indiciate statistical significance (p < 0.05).
Discussion
In this cohort, patients with social vulnerability were more likely to utilize the emergency department within 1-year postoperatively. Additionally, patients with social vulnerability were nearly 3 times more likely to have persistent opioid use at 1-year postoperatively compared to the control group. Although preoperative opioid use was associated with persistent postoperative opioid use, social vulnerability was independently associated with persistent opioid use on multivariate regression. Additionally, on multivariate logistic regression analysis, SVI was independently associated with preoperative opioid use and postoperative emergency department utilization. The relative improvement in PROMs (ie, PI and PF scores) and rates of MCID achievement were similar between groups. On multivariate analysis, only baseline PROMs were associated with MCID achievement in this cohort – patients with better baseline PROMs were more likely to achieve MCID.
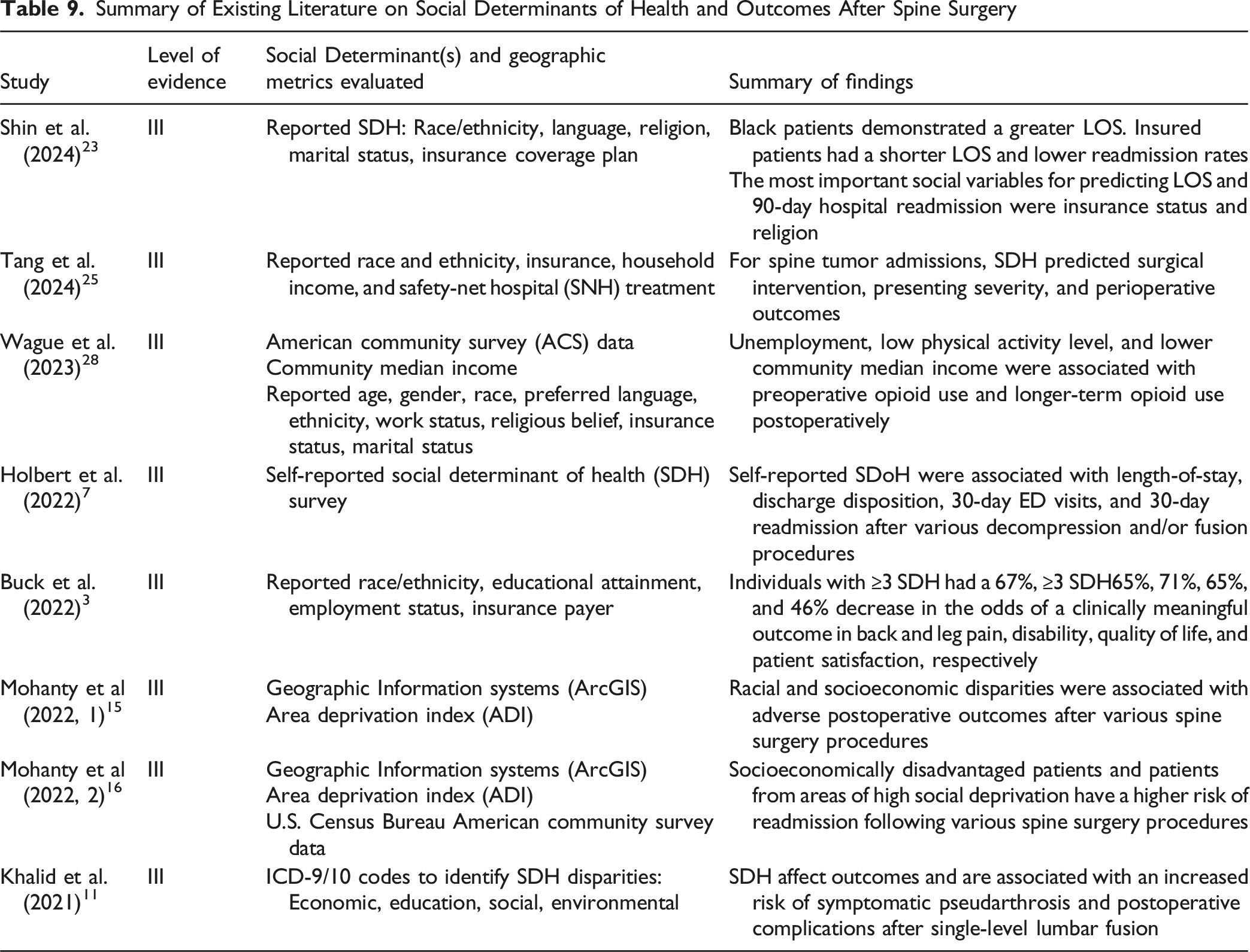
Summary of Existing Literature on Social Determinants of Health and Outcomes After Spine Surgery
The Area Deprivation Index (ADI) and SVI are 2 frequently referenced socioeconomic deprivation indices. 21 The SVI was originally developed by the CDC to identify vulnerable communities that may need additional support during natural disasters, hazardous events, and disease outbreaks. 21 However, its use has been extended more broadly in health policy and healthcare outcome studies. 26 The SVI is based on 15 indicators within 4 categories: socioeconomic status, house composition and disability, minority status and language, and housing type and transportation. The ADI was developed to quantify social deprivation in different neighborhoods using 17 U.S. census indicators of income, education, employment, and housing quality. 21 In contrast to the SVI, the ADI does not take race/ethnicity into consideration. 26 Both the SVI and ADI have been correlated with various healthcare outcome measures,6,17 although research has suggested that the 2 indices do not always correlate with each other and that they can not necessarily be used interchangeably. For instance, 1 study found that the ADI’s inclusion of unstandardized housing price items can lead to misclassification of certain urban environments as “not deprived” in comparison to SVI, which excluded these items. 21 Additionally, 2 recent studies have suggested that SVI may provide better discriminative performance and granularity relative to ADI in identifying disadvantaged patients at risk for poor outcomes.20,31
The current study demonstrated direct association of SVI and postoperative healthcare utilization. In our cohort, patients with social vulnerability were nearly twice as likely to utilize the emergency department within 1 year postoperatively. Prior research has suggested that patients in the immediate postoperative period often visit the emergency department, but there is significant variability in these utilization patterns. 13 Durand et al. reported a 9% rate of 90-day emergency department visits after outpatient spine surgery, with roughly 10% occurring on the same day of surgery. 5 The most common reasons for ED presentation reported were pain, chest pain, headache, abdominal pain, and limb pain. 5 Jain et al. previously reported that risk factors for ED utilization after primary lumbar spine fusion included having Medicare insurance, anterior lumbar fusion, drug abuse/dependence, age less than 50 years old, African American ethnicity, and various medical comorbidities. 9 Additionally, Holbert et al. found that certain social factors were associated with decreased risk of 30-day emergency department visits and hospital readmission. 7 Emergency department utilization is associated with a significant cost burden. Wiley et al. reported that the mean direct hospital cost of an ED visit after elective lumbar spine surgery was $1,971, and the total cost to the institution over 5 years was $5.1 million. 30 Furthermore, emergency department utilization after lumbar spine surgery has been associated with lower patient Satisfaction and Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores. 20 However, the study did not investigate the influence of socioeconomic factors on emergency department utilization. Our findings demonstrated that social disadvantage, as defined by SVI, is associated with increased emergency department utilization after elective lumbar spine surgery. Developing a specific plan to address postoperative concerns, particularly for patients with social barriers, may be an opportunity to improve the quality of care and reduce costs for patients.
Persistent opioid use before and after spine surgery presents a significant challenge for patients, providers, and the healthcare system. 33 Persistent opioid use after spine surgery has been associated with poor outcomes, including hospital readmission, emergency department utilization, and wound complications.10,14 The influence of persistent opioid use on PROMs after spine surgery remains unclear, with some research suggesting worse outcomes and some suggesting similar outcomes in certain metrics.3,11,27 In our cohort, patients with social vulnerability were nearly 3 times more likely to have persistent opioid use at 1 year postoperatively. Additionally, social vulnerability was associated with preoperative opioid use within 60 days of surgery, although this was not statistically significant. Although preoperative opioid use was associated with persistent postoperative opioid use, social vulnerability was independently associated with persistent opioid use on multivariate regression at 1 year postoperatively. This suggests that social determinants of health may be independent risk factors for postoperative opioid use. In a previous study, Wague et al. previously demonstrated that unemployment and lower community median income were strongly associated with opioid use after lumbar spine surgery. 28 Futhermore, Wague et al. found that Black patients more likely to use opioids before surgery, and that preoperative opioid use was associated with persistent opioid use postoperatively. 28 Additionally, Schoenfeld et al. reported that lower socioeconomic status was significantly associated with a decreased likelihood of discontinuing opioid use after spine surgery in a military health system study. 22 Our study found that the SVI metric can be independently predictive of persistent opioid use postoperatively. Identifying this risk preoperatively may help guide preoperative discussion around patient expectations and goals for opioid use in the postoperative setting. The authors view SVI and preoperative opioid use as reasonable screening tools to identify patients that may be at risk for opioid dependence postoperatively. Furthermore, patients with both social vulnerability and preoperative opioid use may be at even higher risk for persistent opioid use after surgery. It may be pertinent to involve a specific pain management team to help guide pre- and post-operative pain control, minimize the risk of opioid dependence, and set expectations prior to surgery.
Other social determinants of health, such as race/ethnicity, religious status, and insurance payor status have also been investigated as potential predictors of outcomes after spine surgery.3,23,25,28 In our study, patients in the social vulnerability group were more likely to have race/ethnicity reported as Black/African-American or Hispanic/Latino, and less likely to have race/ethnicity reported as White/Caucasian. Patients in the social vulnerability group were also more likely to have Medicaid and less likely to have private insurance as the insurance payor status. However, on multivariate analysis, neither race/ethnicity nor insurance payor status were associated with perioperative outcomes, healthcare utilization metrics, or PROMs in this cohort. Other studies have found association between race/ethnicity and insurance payor status and outcomes after spine surgery, however. For example, Shin et al. reported that Black patients experienced a greater LOS after surgery and that insured patients had shorter LOS and lower 90-day readmission rates after surgery. 23 Tang et al. reported that the presenting severity of symptoms of patients with spine tumors was elevated among non-White and non-private insurance patients. 25 The authors also found that Black race, Medicaid, and lower income were all associated with decreased odds of favorable discharge disposition. 25 Others have found that opioid prescribing patterns have been different among patients with different race/ethnicity. For example, Wague et al. found that Black patients were 6.3 times more likely to use opioids before surgery, with preoperative opioid use being associated with persistent opioid use after surgery. 28 Although our study did not find any association between race/ethnicity and insurance payor status and outcome measures, it should be noted that the majority of patients in our cohort were Caucasian/White (69.9%) and with private insurance (81.5%). Therefore, the study could certainly be underpowered to investigate the influence of race/ethnicity and insurance status on outcomes and healthcare utilization metrics after spine surgery.
This study also compared PROMs and MCID achievement in patients with social vulnerability. In our cohort, SVI was not associated with baseline PF and PI PROMs, overall improvement in PF and PI PROMs, nor the rate of MCID achievement. On subgroup analysis, all patients with persistent opioid use trended towards lower PROMs, but this did not achieve statistical significance. This may be due to the fact that there was an overall wide range of PROM scores and a relatively small number of patients with persistent opioid use, decreasing statistical power. Prior studies have had some conflicting results regarding the association between social variables and PROMs after spine surgery. Of note, prior literature has suggested that socioeconomic disadvantage may be a barrier itself to completion of PROM surveys after lumbar spine fusion. 8 Additionally, others have found that racial and socioeconomic disparities were associated with worse global physical health and VAS pain scores both pre- and post-operatively after spine surgery. 15 There is a lack of research investigating social determinants of health and patient-reported outcomes in spine surgery. Given the multifactorial nature of social barriers, further research investigating the relationship between specific social metrics and PROMs would be useful.
Although not specifically investigated in this study, we believe that there are multiple target areas for improvement in patient care. The authors view that the SVI metric could be used as a screening tool to identify patients in clinic that may be at higher risk for certain poor outcome measures after surgery. Once identified, these patients could be placed on a high-risk protocol that would involve multidisciplinary discussions with other team members to ensure efficient and effective care in the perioperative period. Involving social work providers and home health agencies prior to surgery would likely be beneficial for these patients. Specifically, it would be useful for home health nursing and/or home physical therapists to be setup prior to surgery, or at least prior to discharge from the hospital. Home health care can be a tool to provide consistent care and also detect issues or challenges as they arise in a more efficient and timely manner. For patients with pre-operative opioid use and/or social vulnerability, it would be useful to involve either the pain management or physiatry services to help guide a post-operative pain control regimen, with the goal of limiting long-term opioid use after surgery. Having a non-surgical provider contact for pain control management may be useful for these patients, as follow-up and continued contact with these providers may be easier. For patients who are traveling long distances for surgery, establishing care with 1 of these providers closer to their residency may be beneficial.
Patient experience is a challenging metric to measure, but it remains a crucial component of healthcare, particularly after a major surgery. 27 For example, understanding and meeting patient expectations is an important goal for successful outcomes in spine surgery.18,32 Although it was not specifically investigated in this study, the authors believe that social determinants of health likely play a significant role in patient experience in the perioperative period. For example, cultural and language barriers may play a significant role in understanding discharge instructions, expectations, and even PROM surveys. Although discharge instructions are translated to native language, there are often not in-person interpreters available to answer specific questions and communicate more effectively. As another example, transportation and housing barriers likely play a significant role in postoperative care – particularly at tertiary care centers, where patients may travel several miles for a complex spine surgery. These patients could certainly have challenges with post-operative follow-up visits and receiving more urgent perioperative care when issues arise. It is possible that these patients may ultimately turn to other healthcare providers in their area, whom may not have access to the same electronic health record and may not understand appropriate subspecialty-specific postoperative care. This could potentially lead to over-utilization of healthcare resources, unnecessary tests, and substandard care for patients. The exact influence and nuances of these barriers to care would be an important area of investigation for future studies on this topic.
This study does have limitations that should be considered in the context of its findings. Firstly, the study is a retrospective review of prospectively collected data, which is inherently subject to selection bias. All patients were treated at a tertiary care center, which may select for a certain patient population. Additionally, we did not collect data on how long patients had symptoms prior to surgery, which could certainly influence perioperative opioid use and potentially long-term outcomes. This would be an important variable to address in future studies. Patients without complete PROMs data at 1 year postoperatively were not included in the analysis, which can certainly introduce selection bias. Other authors have indeed reported that social determinants of health impact completion of PROMs – with the majority of patients completing PROMs residing in wealthier communities. 8 Further studies to identify specific barriers to PROMs and rectify this challenge within this patient population would be of value. Additionally, patients in the lower SVI cohort had some minor differences in other demographic variables – these patients were more likely to be female and to have ASA class 2. Efforts were made to control for these potential confounding variables using multivariate regression. Nonetheless, the results should be considered in the context that some baseline demographic variables were different between groups. Lastly, efforts were made to search for utilization of healthcare resources at outside institutions using the “Care Everywhere” tool in the electronic medical record. However, it is possible that episodes of postoperative care at non-participating institutions would not be detected. Nonetheless, the data discussed herein provide insight into healthcare utilization trends and highlight potential targets to optimize healthcare equity in socially vulnerable patients undergoing elective spine surgery.
Conclusions
Patients with social vulnerability – as defined by an upper quartile score on the SVI socioeconomic and housing subcategories – were more likely to utilize the emergency department and have persistent opioid use at 1 year postoperatively from elective lumbar decompression procedures. Social vulnerability was independently associated with postoperative emergency department utilization and persistent opioid use on multivariate analysis. Further prospective studies are warranted to investigate the relationship between specific social disparities and healthcare utilization after elective spine surgery.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.