
Abstract
Study Design
Retrospective review.
Objectives
This study aimed to assess and compare the clinical course and complications between surgical decompression and decompression with fusion in lumbar spine patients aged ≥80 years.
Methods
A retrospective review of electronic medical records at a single institution was conducted between September 2005 and December 2021. Logistic regression was used to identify potential risk factors for the occurrence of complications.
Results
Over a 16-year period, 327 patients were allocated to the decompression only group and 89 patients were allocated to the decompression and instrumented fusion group. The study had a mean follow-up duration of 36.7 ± 12.4 months. When assessing the CCI, patients of the instrumentation group had fewer comorbidities
Conclusions
Lumbar decompression and additional fusion in octogenarians are considerable treatment techniques; albeit associated with increased complication risks. Prolonged operative time and extent of surgery are critical confounding factors associated with higher rates of postoperative complications. Surgery should only be performed after careful outweighing of potential benefits and risks.
Introduction
As life expectancy is increasing owing to accelerating improvements in patients’ quality of life and in the health care system, it is expected that the proportion of the world’s population aged over 60 years will nearly double from 12% to 22% in 2025. 1 Natural aging can substantially affect all spine elements such as the intervertebral discs, facet joints, and supporting muscles and ligaments, thus leading to biomechanical alterations and anatomical changes. 2 Such degenerative changes may results in spinal and foraminal narrowing, thereby inducing significant compression of vascular and neural structures of the spinal cord, reflected clinically as neurogenic claudication or lumbar radiculopathy, which is a decrease in the mobility and quality of life of elderly patients.2‐4
In a randomized trial from 2016 on decompression with or without fusion for the treatment of degenerative lumbar stenosis with concomitant degenerative spondylolisthesis, the study group showed that decompression with fusion led to comparable outcomes at 3- and 5-years follow up with the decompression group alone. 5 The reoperation rates were similar between both groups at 20%. In line with these findings, a more recent randomized study showed similar results, although the decompression-alone group underwent reoperation more frequently (12.5% vs 9.1%) over a 2-year follow up. 6 However, a major limitation of these studies is that octogenarians were ruled out from the analysis, as the mean age of the patients in both studies was approximately 66 years.
Over the past few years, the prevalence of degenerative disorders of the lumbar spine, such as spinal stenosis or olisthesis, has rapidly increased worldwide, especially in aged 80 years and over. 7 Since this subset of patients is prone to predisposing and comorbid medical conditions, diagnosis and treatment may require complex strategies (Deyo et al., 2010; Machado et al., 2017; O’Lynnger et al., 2015). Surgical management of elderly patients might be viewed with trepidation by many surgeons due to a higher rates of morbidity and mortality owing to their prior baseline history3,11
In terms of octogenarians (patients aged ≥80 years), thus far, there is no clear consensus on optimal treatment, especially in cases of instability. Whether simple decompression or decompression with fusion should be performed in this frail cohort still poses a dilemma. Considering the unique needs of older patients and the multitude of age-related variables that impact the clinical course, a thorough investigation of this patient cohort should be conducted.
Given the lack of studies on this topic, we aimed to compare the clinical course and complications (including morbidity, mortality, and readmission rates) after surgical decompression only vs surgical decompression with instrumented fusion exclusively in octogenarians with spinal canal stenosis or spondylolisthesis.
Methods
Study Design, and Inclusion Criteria
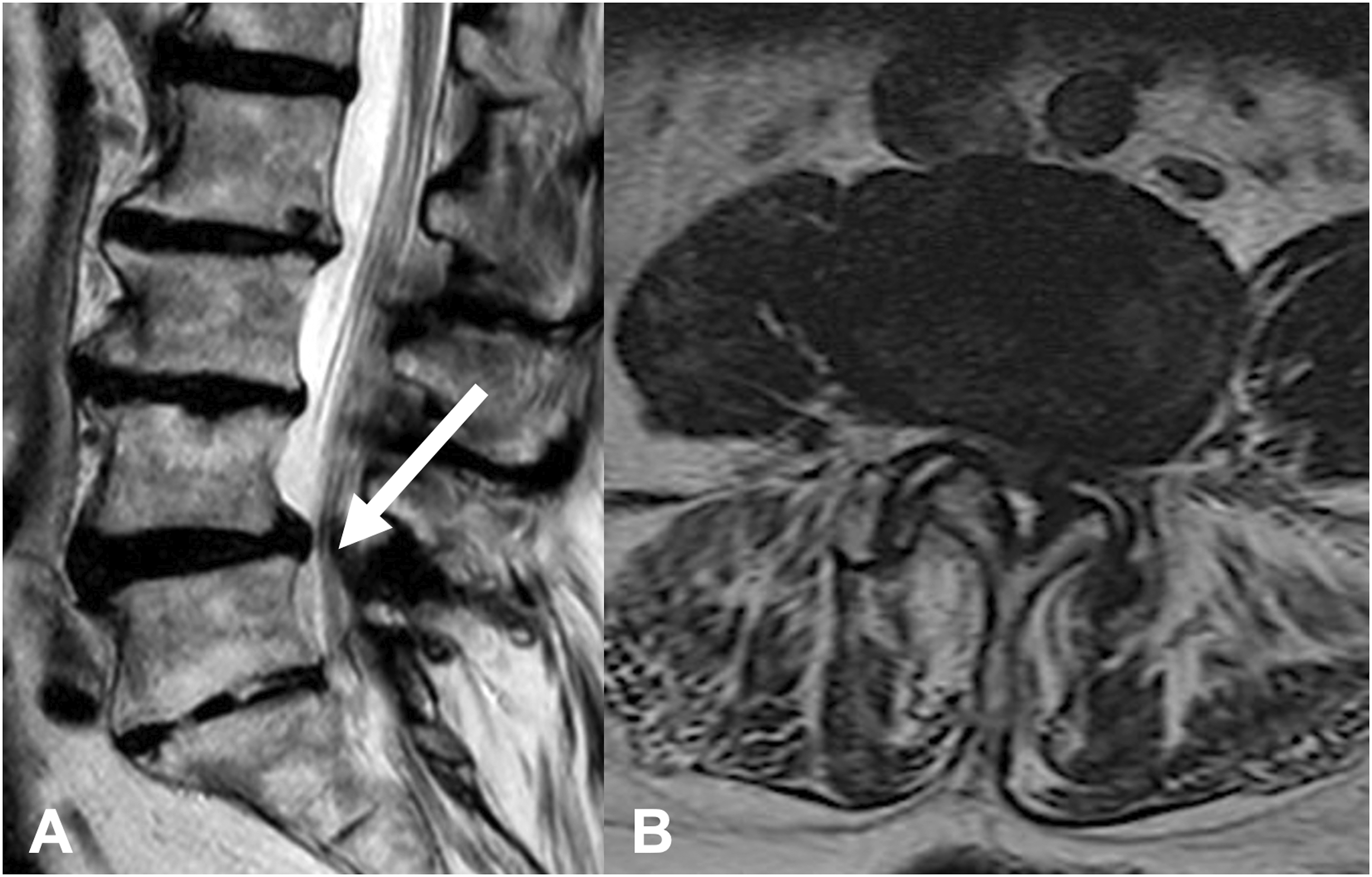
Clinical and imaging data were retrospectively collected over a 16-year period, (September 2005 to December 2021) from our institutional database. The present study was conducted in accordance with the Declaration of Helsinki and approved by the local ethics committee (approval no. S-723/2017). The requirement for informed consent was waived owing to the retrospective nature of the study. Patients aged ≥80 years with lumbar spinal canal stenosis with or without degenerative olisthesis were consecutively enrolled. Patient evaluations consisted of radiographs in the standing upright flexion/extension, computed tomography (CT) scan, and magnetic resonance imaging. Surgical candidates consisted of patients in whom conservative therapy had failed, including physical therapy, injections, and medical management, or those who presented with a neurological deficit, by whom a correlator in imaging was obtained. Exclusion criteria were as follows: age <80 years, concurrent intracranial or cervical pathology, spinal infection, progressive kyphotic deformity, and unavailable requisite data (Figures 1 and 2). Sagittal (A) and axial (B) lumbar spine magnetic resonance tomography of a 84-year-old patient with lumbar spine spondylolisthesis L4/L5 (white arrow). Mobile pathoanatomy anatomy on functional X-rays (C flexion, D extension). Sagittal (A) and axial (B) lumbar spine magnetic resonance imaging for an 86-year-old patient with lumbar spinal stenosis L4/L5 (white arrow) symptomatic with neurogenic claudication.
Patients’ Characteristics
Patient demographics, comorbidities, American Society of Anesthesiologists (ASA) scores, surgery duration, volume blood loss, number of treated spinal levels, perioperative and postoperative complications, hospital length of stay (LOS), intensive care unit (ICU) stay, readmission rate, reoperation rate, and mortality rate were retrieved from patients’ electronic medical records. Comorbidities were preoperatively assessed using the age-adjusted Charlson comorbidity index (CCI).9,12 The CCI score was calculated for each patient to classify comorbidities and was grouped as having no comorbidity (CCI = 0), minimal comorbidity (CCI = 1 or 2), moderate comorbidity (CCI = 3-5), or severe comorbidity (CCI > 6). Preoperative neurological condition was assessed using the motor score (MS) of the American Spinal Injury Association impairment grading system (MS = 0, no muscle strength; MS = 100, healthy). Postoperative MS was documented according to the last clinical and imaging follow-up examination. According to our institutional standards, routine clinical and radiological follow-up examinations were performed before discharge and 3 months after surgery. The final follow-up period was between 3 and 36.89 months postoperatively. Conventional radiographs in the anteroposterior and lateral views were obtained to evaluate screw position and fusion rates.
Procedures
Patients were allocated into 1 of 2 groups: (1) surgical decompression only and (2) surgical decompression with instrumented fusion. An MRI and a CT scanning of the lumbar spine were performed for the preoperative evaluation of each patient. MRI helped to confirm the diagnosis and assess the severity of lumbar spinal stenosis, define the location of the stenosis (eg central, foraminal, or lateral recess), evaluate the facet joint regarding osteoarthritis signs, and, most importantly, preclude symptoms that mimic lumbar spinal stenosis. 13 Moreover, based on MRI, we localized the of lumbar spinal stenosis for example, a bulging disc or thickened flaval ligaments. The CT scans enabled us to accurately evaluate the osseous dimensions of the canal, to delineate the posterior elements, visualize destructive changes of the facet joints, and differentiate between hard vs soft disc pathology. 14 The diagnosis of spondylolisthesis was confirmed by assessing radiographs in the standing upright flexion/extension position. Due to the poor baseline history of the examined cohort, each case was interdisciplinarily discussed by a multitude of healthcare professionals including neurosurgeons, neuroradiologists, and anesthesiologists in accordance with the clinical needs of each patient. The final decision was made by the senior spine surgeons. An optimal treatment plan was set based on the individual’s clinical All instrumented surgeries were performed in an open manner using a CT-based point-to-point navigation system to enhance maximal safety, as previously described by our study group. 15 Decompression was performed microsurgically, as routinely conducted at our institution. A microsurgical laminectomy was conducted for decompression of the spinal canal. As for fusion, transforaminal interbody fusion (TLIF) was conducted, which is routinely performed in our institution.
Statistical Analysis
For categorical variables, frequency counts were computed and presented along with their percentages. Continuous variables are presented as means ± standard deviations, as they were normally distributed, as verified using the Shapiro–Wilk test. Univariate analysis was used to compare groupwise baseline characteristics, surgery duration, blood loss volume, intraoperative and postoperative complications, LOS, ICU stay, readmissions, revision rates, and mortality. For categorical variables, the chi-square test was applied, while for continuous variables, the independent t-test was used. The Wilcoxon’s rank test was used to evaluate changes in neurological status (MS) of each group at discharge. Potential risk factors for complications were examined as independent variables in a bivariate logistic regression analysis model. To investigate a potential cut off for length of surgery and assess it as a risk factor for the occurrence of complications, we first defined the median of the length of surgery, which was 150 minutes. Then, we classified the duration of surgery into 2 groups: 0-150 minutes and 150.1-380 minutes. Finally, we performed univariate logistic regression analysis for the occurrence of complications and adjusted for the surgical duration. A P-value<.05 was considered to be statistically significant. All statistical analyses were performed using SPSS software, version 24.0.0.0 (IBM Corp., Armonk, NY, USA).
Results
Patients’ Demographics and Baseline Characteristics
Baseline Characteristics of Patients.
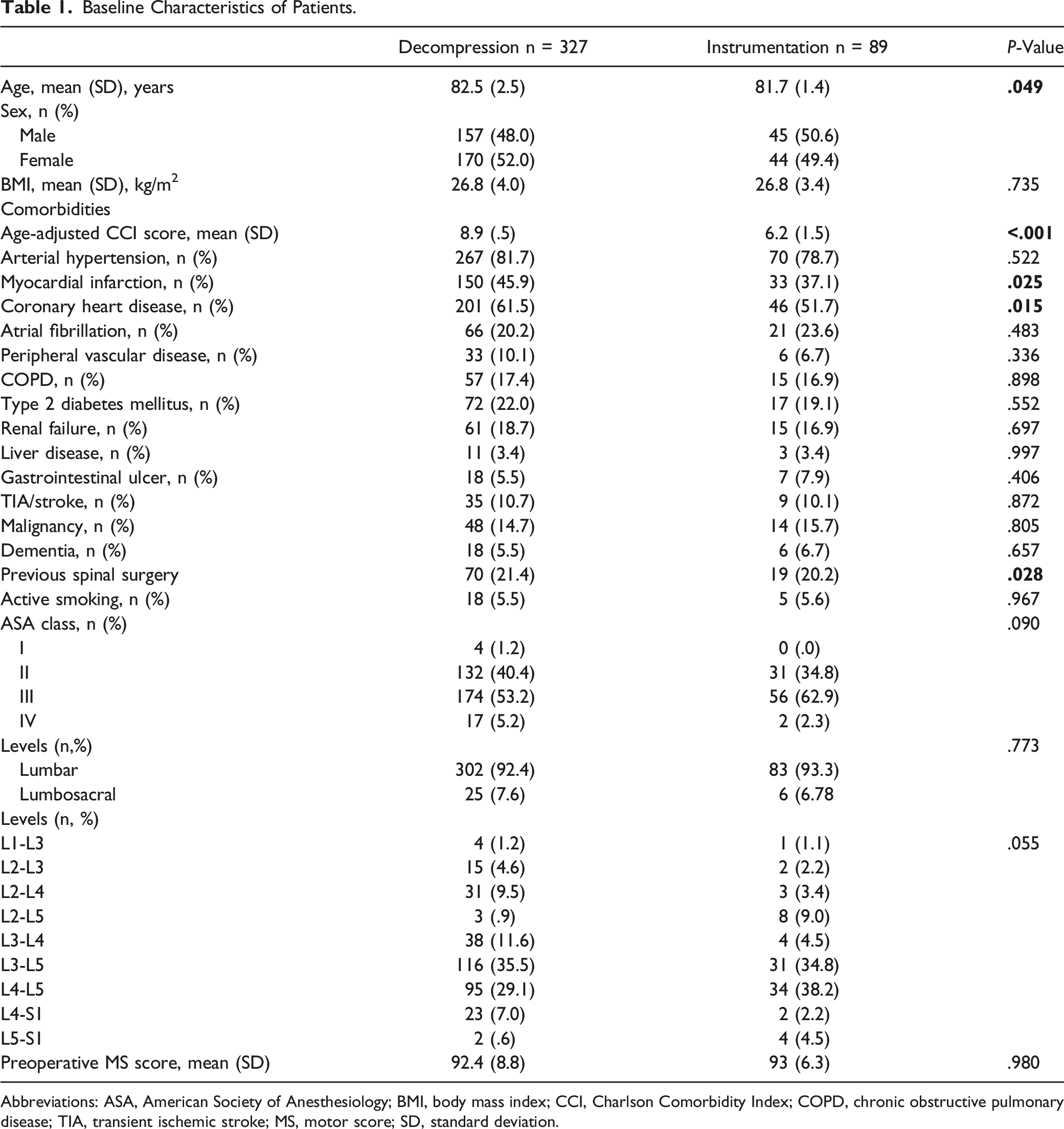
Abbreviations: ASA, American Society of Anesthesiology; BMI, body mass index; CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disease; TIA, transient ischemic stroke; MS, motor score; SD, standard deviation.
Surgical Characteristics, Clinical Course, and Revision Rates
Comparison of surgical characteristics and clinical course between the groups
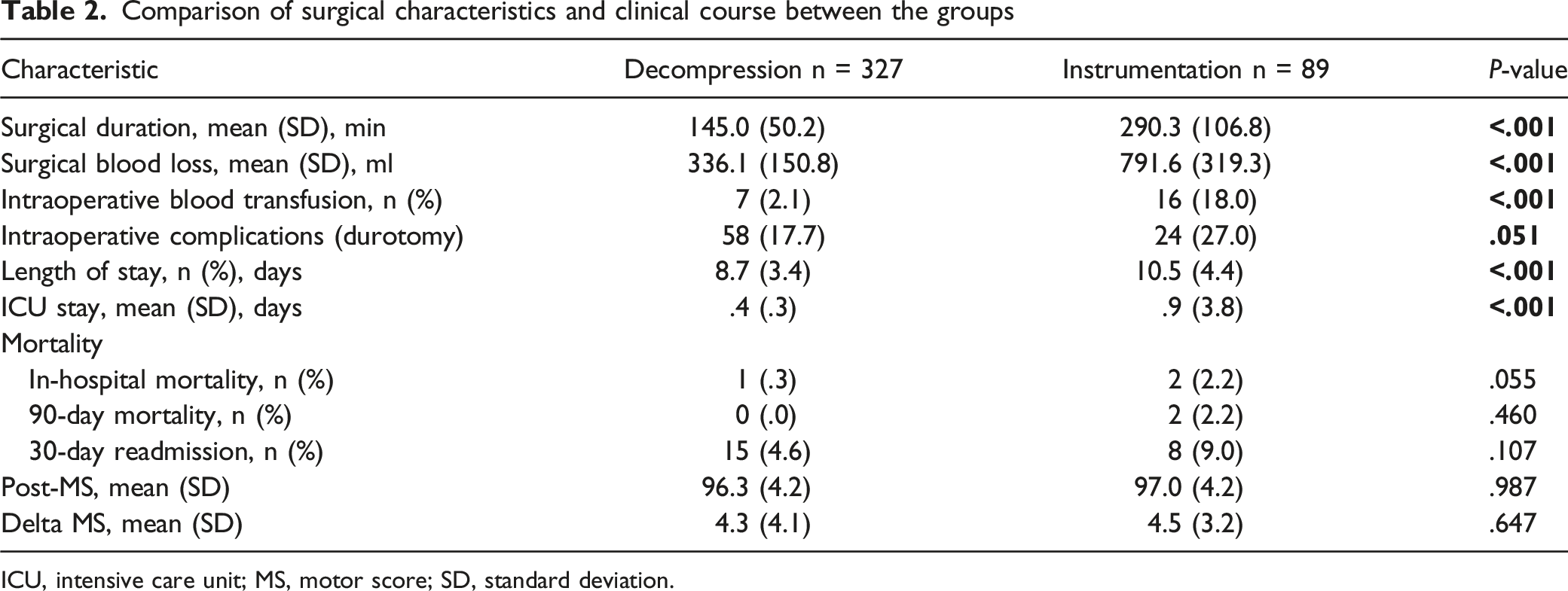
ICU, intensive care unit; MS, motor score; SD, standard deviation.
Comparison of Neurological Status Between Baseline (Before Surgery) and Discharge.

All data are mean (SD).
MS, motor score of the American Spinal Injury Association grading system.
Occurrence of Adverse Events and Potential Risk Factors
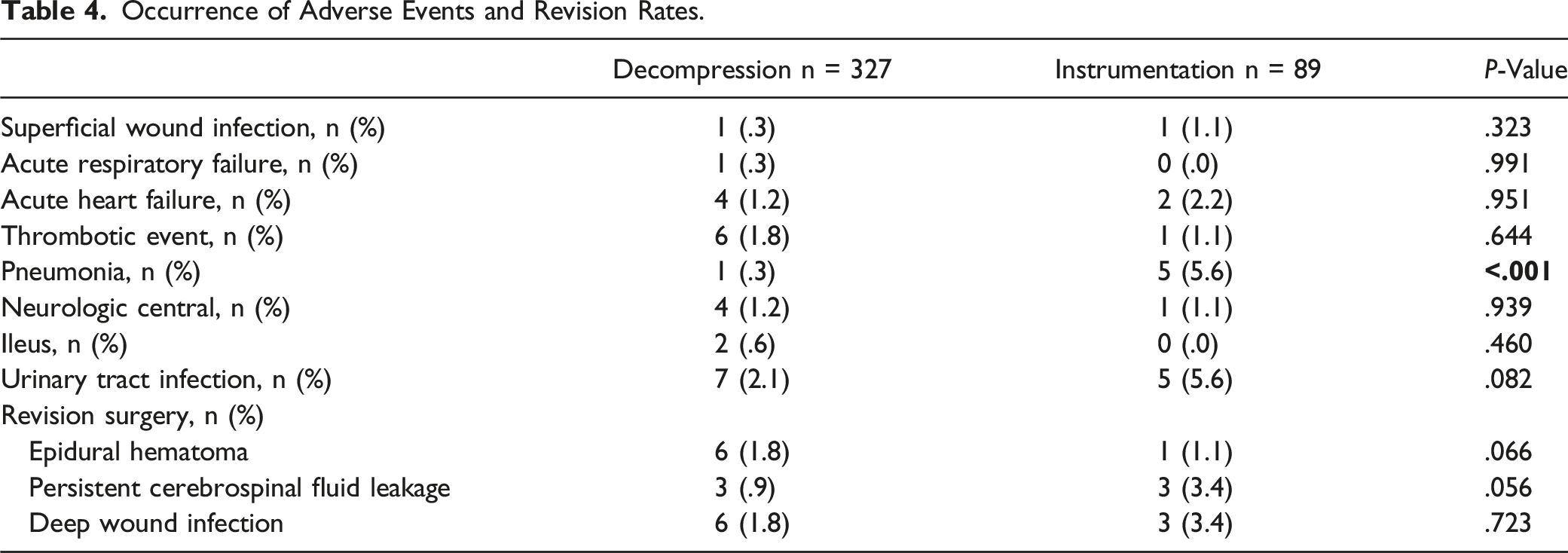
Occurrence of Adverse Events and Revision Rates.
Bivariate Logistic Regression Analysis for Definition of Potential Risk Factors for the Occurrence of Postoperative Complications.
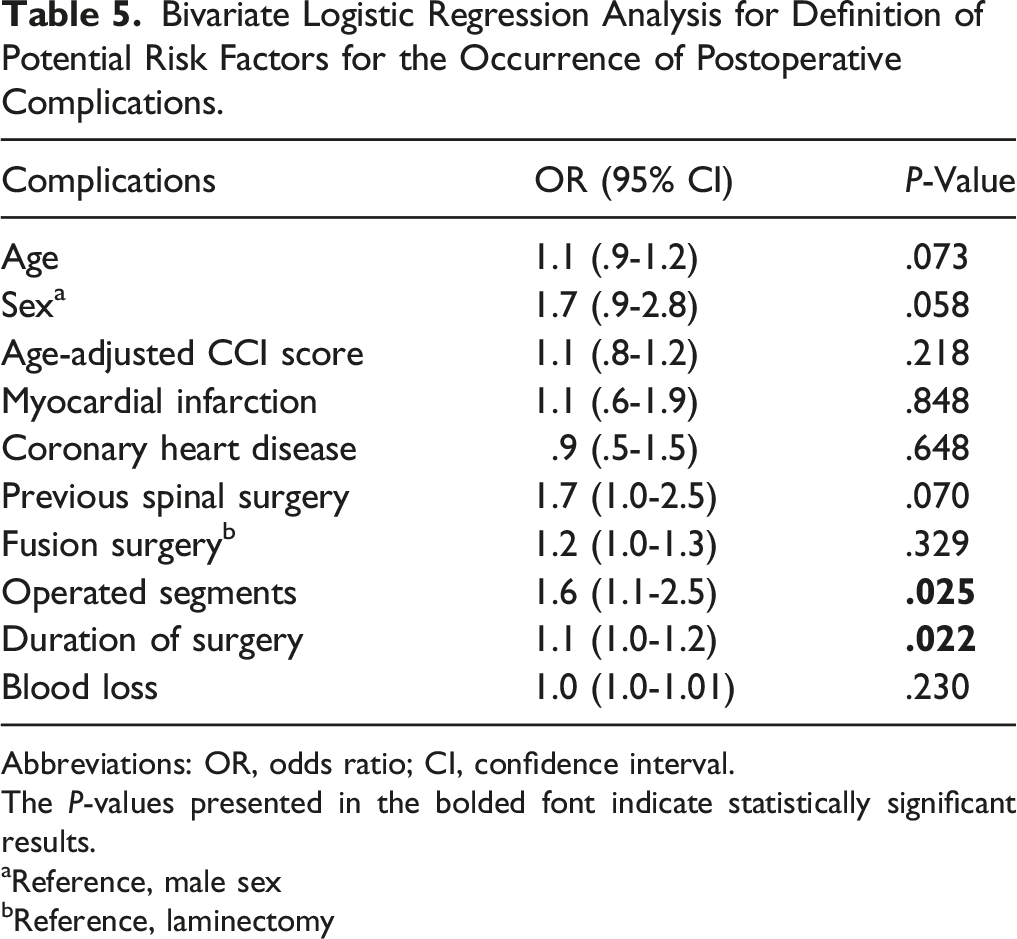
Abbreviations: OR, odds ratio; CI, confidence interval.
The P-values presented in the bolded font indicate statistically significant results.
aReference, male sex
bReference, laminectomy
Discussion
To the best of our knowledge, this is the first systematic analysis describing surgical strategies for the treatment of degenerative spinal diseases in a large sample of patients over 80 years of age. The current study investigated patient history and clinical status, with a special focus on assessing morbidity and mortality rates. Interestingly, we found a significant difference in age, wherein older patients of the instrumentation group were at least 2 years younger than those of the decompression group. When examining different underlying conditions, patients who underwent fusion surgery had a higher prevalence of cardiac diseases, such as previous myocardial infarction or coronary heart disease, and an overall substantially higher burden of comorbidities, whereas similar findings were seen concerning the pre- and postoperative neurological status. Notably, surgical duration, estimated blood loss volume, and intraoperative complications were higher in the fusion group. The in-hospital and 90-day mortality rates were low in both groups, ranging from 0% to 2.2%. Notably, only surgical duration was a unique risk factor for the occurrence of postoperative complications in octogenarians.
Preoperative evaluation of older patients converted to a surgical procedure should be thoroughly discussed, especially in the context of complication, morbidity, and mortality rates. 16 Wang et al. performed a retrospective analysis of 26 patients older than 85 years undergoing lumbar spine surgery, with 72% opting for fusion surgery. They escribed relatively low comorbidity rates with a mean ASA score of 2.6, indicating mild systemic disease, and a CCI score of 1.1, indicating moderate illness 17 A recent review and meta-analysis of 51 studies on degenerative spinal stenosis showed a higher prevalence of cardiovascular diseases, and in conjunction with the aforementioned study, the overall CCI was 1.2, which is much lower than those described in the present study. 18 In addition, Daubs et al., in their retrospective study of 46 patients older than 60 years undergoing lumbar spine fusion surgery, described the presence of 4 comorbidities in only 9% of the cases, while more than 20% had no underlying pathologies. 16 Herein, the age ranged between 60 and 85 years, while the number of octogenarians was not explicitly reported. Ong et al. analyzed claims data of older patients with lumbar spinal stenosis or spondylolisthesis undergoing a surgical procedure, and only 4% of the enrolled patients had a CCI of >5. 19 Notably, only 10%-13% of the examined cohort were over 80 years old, which might explain the low morbidity rates. Nevertheless, this discrepancy between our findings and those of the aforementioned studies concerning comorbidities might be attributable to the large number of patients enrolled in our study. Second, many cases were admitted to our hospital because of a new neurological deficit, and the surgical procedure was inevitable to improve the prognosis of patients independent of different underlying conditions that might be weighed under normal conditions. For example, Wang et al. reported that all surgical procedures were planned electively; thus, potential selection bias might be present. 17 Hence, we strongly believe that the preoperative condition of patients should be meticulously documented as, for example, poor renal function or a preexisting lung or heart disease could possibly impact peri- and post-operative monitoring due to volume dynamics. 20
In a retrospective analysis of 130 older patients, of whom only 30 patients were aged 80 years and higher, the study group of the octogenarians showed that the performance of lumbar decompression with fusion improved postoperatively (improvement of VAS 52.0% and of ODI 42.8). 21 However, data on neurological status for both before and after surgery were omitted. In line with these data, Shabat et al. advocated that laminectomy can lead to significant improvements in daily activity as well as a significant decrease in lumbar pain of octogenarians, as measured by the Barthel index (VAS: preoperative 8.8, postoperative 3.6; P < .001). 22 In another study on 121 octogenarians with lumbar degenerative spinal canal stenosis, laminectomy also led to substantial mitigation of pain (VAS: preoperative 7.2, postoperative 4.5; P < .001). 23 Furthermore, in another study on potential differences in functional outcomes between post-lumbar surgery patients <65 years (n = 189) and >65 years (n = 74), there were no significant differences in quality of life, indicating that age should be a contraindication for surgery in the aged population with degenerative lumbar spine pathologies. 24 Nevertheless, it should be emphasized that the above-mentioned studies are limited by a small sample size. In the present study, 417 patients who underwent lumbar surgery with a long-term follow up were examined, and we were able to show that the neurological status after surgery improved substantially. Therefore, 1 may deem that spinal surgery, even in this frail cohort, can be helpful to preserve the mobility and quality of life of the patients.
The logic of avoiding major surgical procedures in elderly patients because of potential complication rates is self-evident. However, due to improvements in spinal surgery, such as the development of microsurgical approaches or the implantation of pedicle screws by applying spinal navigation systems, which are associated with shorter operation times, octogenarians are considered candidates for such surgeries. Importantly, Wang et al. showed that complication rates were comparable to our findings at 19.2%. 17 The most prevalent unsolicited event was electrolyte imbalance, while minor complications occurred in over than 50% of the cases. Revision and readmission rates were not reported. Over the 42-month follow-up period, no deaths occurred. In conjunction with these findings, Saleh et al., in their retrospective analysis of 2320 patients aged over 80 years, found similar complication rates ranging from 3% to 16%. 4 The most common major complications were sepsis (1%) and the need for blood transfusion (10.1%). The mortality rate was .4%, similar to that found in our study. In another review focusing exclusively on patients older than 60 years, 11 articles reported inadvertent durotomy in 5%, while the mortality rates were similar to those reported by Saleh et al.. 25 Interestingly, in our study group, pneumonia was found to be significantly more frequent in patients who opted for instrumented fusion than in those who did not. A trend toward a higher prevalence of durotomy was observed in the instrumentation group; however, this did not reach statistical significance. Risk factors for the occurrence of complications seem to be surgical duration longer than 180 minutes4,17 as well as the number of operated levels, 26 which is in accordance with our results. Previous evidence suggests that the operative procedure (decompression only vs instrumentation), presence of comorbidities, or intraoperative blood loss volume do not have a substantial impact on patients’ clinical course.4,17,26 Nevertheless, these confounders can result in an extended hospitalization stay. For instance, Kobajyashi et al. reported significantly longer hospitalization rates (mean: 51 days) due to the occurrence of major complications, which is much higher than ours’. 27 One potential explanation might be that the cohort of Kojabashi et al. consisted mainly of nonagenarians (patients >90 years) who predominantly underwent cervical spine surgery because of higher grades of disability. 27 Notwithstanding also the more invasive nature of fusion surgery, patients who undergo such procedures might require more added postsurgical care.
In the present study, surgical duration, extent of surgery, intraoperative blood loss, transfusion, and length of hospital stay were significantly higher in patients undergoing posterior decompression and fusion than in patients receiving a simple decompression. In a retrospective analysis of 111 patients aged 70 years undergoing lumbar posterior decompression and pedicle screw fixation, Kong et al. found comparable surgical times and blood loss (256 minutes; 620 ml). 28 In line with our findings, larger extent of surgery was a significant risk factor for the occurrence of complications. Deyo et al. reported a higher in-hospital complication rate of 15.8% for older patients with laminectomy and fusion than for those with laminectomy alone (9.8%). 9 Son et al. showed in a comparative analysis of octogenerians vs patients aged ≥65 years similar operative times, blood loss, and blood transfusion and even longer hospitalization (33 days vs 10.5 days in the present study) after lumbar spinal fusion surgery. While it may seem surprising, these confounding factors did not differ significantly between the groups.
However, increasing age and blood loss were associated with higher risk for complications. Nevertheless, quality of life and functional outcomes ameliorated substantially in older adults. 21 Of note, in a large study of 4947 older patients undergoing posterior lumbar fusion based on claims data, Hersey et al. stated not only that longer surgical times are associated with a higher risk for the occurrence of postoperative complications but also that every increment of operative time results in an increased risk for adverse events. 29 Moreover, Wang et al. advocated that operative times longer than 180 minutes in older adults undergoing lumbar spine surgery are associated with increased risks of complications, which is similar to our findings. 17 Whereas randomized trials concentrated mainly on younger patients undergoing lumbar decompression with or without fusion, it bears noting that the length of surgery as well as the blood loss were significantly higher in patients who underwent fusion than in those who did not. 5 Hence, on the 1 hand, these findings endorse the performance of lumbar spinal fusion surgery, as the octo- and nonagenarians can maintain their quality of life, but 1 the other hand, careful perioperative management and short operation times are needed to prevent postoperative complications or even death.
In contrast to the findings of Carreon et al., the performance of instrumented fusion was not a significant risk factor for the occurrence of complications. However, longer ICU stays and overall hospitalization rates occurred in the instrumentation group compared with those in the decompression only group. Interestingly, the 30-day readmission rates did not differ significantly between the groups. However, patients in the instrumentation group had higher revision rates, mainly because of persistent cerebrospinal fluid leakage or screw displacement. In a long-term follow-up of >3 years, no death occurred, and additional instrumentation was not required because of secondary instability after surgical decompression. Previous evidence suggests that radiologically confirmed instability after spinal decompression should be treated using instrumented fusion. 30 Advances in surgical techniques over the past decade have allowed adequate decompression with minimal disruption to the surrounding stabilizing factors, and meticulous study of patients converted to surgical decompression might have potential reasons for the lack of secondary fusion surgery in such a frail cohort. Another factor to consider might be the spontaneous fusion of the spinal cord which might substantially contribute to a decrease in instability rates. 31
The main strength of the current study is that we are the first to examine the clinical course exclusively in octogenarians undergoing spinal decompression only vs decompression and instrumented fusion in such a large-sample cohort. However, this study has some limitations. First, this was a retrospective study, in which patient management was not randomized but the surgeon’s assessment was guided by individual patient characteristics. Notwithstanding, considering the vulnerability of this subset of patients, we believe that the treatment strategy was selected by considering patient history, neurological condition, and imaging parameters. One might argue that only a limited number of cases have been examined. However, because there is a lack of robust clinical evidence on the clinical course solely in octogenarians, we believe that our findings provide a real-world picture of optimal treatment for these patients. In total, 38 patients (9.1%) were lost to follow up examination after the regular 3 months outpatient visit in our institution for the postoperative evaluation. Herein, we want to accentuate that these 38 patients underwent microsurgical decompression, and the chance for a postoperative complication was much lower than that of the instrumentation group. Sixteen patients were lost after one-year follow up and 20 patients after 2-years follow up. Three-years follow up data could be extracted for 343 patients (82.2%). Overall, we feel that, despite the loss of patients to follow up, our cohort produces a real-world picture of the disease course. Furthermore, due to the retrospective design of the current study scores validating the clinical outcome could not be applied. Larger studies are needed to elucidate potential candidates for nonoperative management.
Conclusions
As life expectancy increases and the population continues to age, the number of elderly patients seeking surgical therapy is also expected to increase. Older patients undergoing lumbar spine fusion have longer hospitalization rates and higher revision rates than those undergoing decompression only. However, the mortality rates and neurological condition were similar in both groups. Unambiguously, the surgical time and extent of surgery should be preoperatively considered because they serve as potential confounders for the occurrence of complications. Careful attention to patients’ comorbidities is critical, and use of an anesthetic and operative duration should be kept to a minimum.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to Participate
The requirement for informed consent was waived on account of the retrospective nature of the study.
Ethics Approval
The local ethics committee approved this study (study ID: S-115/2015) and waived the requirement for informed consent because of the retrospective nature of the study.