
Abstract
Study Design
Retrospective study using the MarketScan database.
Objective
This study sought to investigate: (1) real-world surgical management, and (2) 5-year all-cause reoperation rates after index surgical treatment.
Methods
Patients 18 – 65 years old with 2-year minimum follow-up undergoing single-level lumbar decompression were included. Patients were stratified based on the presence of spondylolisthesis (+LISTH) and arthrodesis (+FUSION) during the index procedure. Those undergoing multi-level, endoscopic, revision, corpectomy/transpedicular, and thoracic/cervical decompression were excluded, as were those with infectious, traumatic, or neoplastic etiologies. The time elapsed between primary and any revision surgery was determined. Follow-up was terminated at 5 years post-operatively.
Results
In total, 86 708 adult patients undergoing single-level lumbar decompression were included. Spondylolisthesis was observed in 10.8%. Of + LISTH, 90.7% underwent additional arthrodesis. Of -LISTH, 89.8% underwent decompression alone. Among + LISTH, at 5-year post-operatively, 15.2% vs 20.3% of patients with +FUSION vs -FUSION had undergone surgical revision involving the lumbar spine (aHR 0.76, P = 0.009). Conversely, among those without spondylolisthesis (-LISTH), 17.6% vs 17.6% of those with +FUSION vs -FUSION had undergone revision at 5-year (aHR 0.94, P = 0.116). In the -LISTH group, patients demonstrated higher occurrence of revision over 2 – 5 years (aHR 1.43, P < 0.0001) among patients treated with additional arthrodesis.
Conclusions
In this retrospective cohort study of patients undergoing surgical treatment for single-level lumbar stenosis, patients with spondylolisthesis who underwent arthrodesis with decompression had lower revision rates at 5-year follow-up.
Introduction
Degenerative lumbar spondylolisthesis is a common lumbar disorder and involves the slippage of vertebral bodies due to underlying degenerative spinal pathology. 1 The current clinical paradigm is that the expected surgical treatment for single-level lumbar stenosis is usually decompression alone for patients without dynamic spondylolisthesis, and addition of arthrodesis for patients with dynamic spondylolisthesis. However, the literature is heterogeneous.
The Spine Patient Outcomes Research Trial (SPORT) demonstrated that surgical management of lumbar degenerative spondylolisthesis had superior outcomes when compared to those treated nonoperatively.2,3 Most patients in the surgical treatment group were treated with laminectomy and arthrodesis. One of this study’s limitations was that it did not provide substantial comparative data on laminectomy alone vs laminectomy and arthrodesis for patients with degenerative spondylolisthesis.2-4 Currently, the literature is inconclusive regarding whether laminectomy alone vs laminectomy with arthrodesis is superior in patients with lumbar spondylolisthesis. Försth et al found no difference in Oswestry Disability Index (ODI) scores at 2 and 5 years post-operatively in patients with and without spondylolisthesis who were randomized to decompression vs decompression with fusion groups.3,5 Ghogawala et al, 3 however, in the Spinal Laminectomy vs Instrumented Pedicle Screw (SLIP) trial found an increase in SF-36 scores at 3 and 4 years post-operatively in spondylolisthesis patients who underwent decompression and fusion compared to decompression alone. Chan et al aimed to investigate the difference between these 2 surgical treatment options by comparing 12-month outcome data for patients with degenerative lumbar spondylolisthesis who underwent laminectomy with or without fusion. They demonstrated that patients who underwent laminectomy and fusion had better ODI scores in 1 year. In addition, they looked at reoperation rates and found that even though patients who underwent laminectomy and fusion had lower reoperation rates, there was no statistically significant difference at 1 year. 6
Other studies have examined revision rates after decompression for lumbar stenosis, but those with long-term follow-up have generally been limited by low overall enrollment. The aims of the current study were to investigate: (1) rate of expected surgical treatment in the real-world, and (2) 5-year all-cause reoperation rates after index surgical treatment.
Methods
Data Source
This was a retrospective cohort study using the MarketScan Research Database (IBM Watson Health, Ann Arbor, MI). The MarketScan database contains >30 billion records of claims data from private insurers, including employees ≤65 years old of private, self-insured corporations, as well as COBRA enrollees and their dependents. As this study involved only deidentified and publicly available data, informed consent was not required, and this study was deemed exempt from Institutional Review Board (IRB) review.
Patient Selection
Patients age ≥18 years undergoing single-level lumbar decompression in either the inpatient or outpatient settings were identified using CPT codes (CPTs 63 005, 63 030, 63 047, 63 052). Those undergoing multi-level surgery (CPTs 63 017, 63 035, 63 044, 63 048, 63 053), revision surgery (63 042), endoscopic decompression (CPT 62380), and anterior, transpedicular, corpectomy, thoracic, and cervical decompression (CPTs 63 075, 63 076, 63 077, 63 078, 63 081, 63 082, 63 085, 63 086, 63 087, 63 088, 63 090, 63 091, 63 055, 63 056, 63 057, 63 064, 63 001, 63 003, 63 015, 63 016, 63 020, 63 040, 63 043, 63 045, 63 046) were excluded, as were those with infectious, traumatic, or neoplastic etiologies. Only patients with minimum 2-year follow-up were included. Follow-up was terminated at 5 years after the index surgery.
Dependent Variable
The primary dependent variable was revision surgery at 2-year follow-up, either with arthrodesis (CPTs 22 612, 22 630, 22 558, 22 586, 22 633, 22 808, 22 810, 22 812, 22 800, 22 802, 22 804) or decompression (CPTs 62 380, 63 005, 63 017, 63 030, 63 042, 63 044, 63 047, 63 052, 63 053, 63 056, 63 087, 63 088, 63 090, 63 091), occurring in either the inpatient or outpatient settings. Of note, patients with 24-h observational stays were considered outpatient for coding purposes.
Independent Variables
The primary independent variables were the presence of diagnosis codes for spondylolisthesis (ICD-9-CM [7384, 75 612], ICD-10-CM [M4315, M4316, M4317]), and the presence of procedure codes for arthrodesis (CPTs 22 612, 22 630, 22 558, 22 586, 22 633). Additional independent variables included age at surgery, sex, outpatient vs inpatient surgery, region, interbody use, and anterior approach for arthrodesis. Documented spondylolisthesis was assumed to be “dynamic” in nature for the purposes of the analysis.
Statistical Analysis
Descriptive statistics were generated. Bivariable analyses were conducted with Chi-Square tests and Wilcoxon-Mann-Whitney tests, as appropriate. Kaplan-Meier curves were generated. Multivariable analyses were conducted with Cox Proportional Hazard regression, and cases of non-proportionality were analyzed with piecewise regression. Statistical significance was considered P < 0.05. All analysis was completed with SAS 9.4 (SAS Institute, Cary, NC) and R 4.3.2 (R Foundation, Vienna, Austria).
Results
Study Population
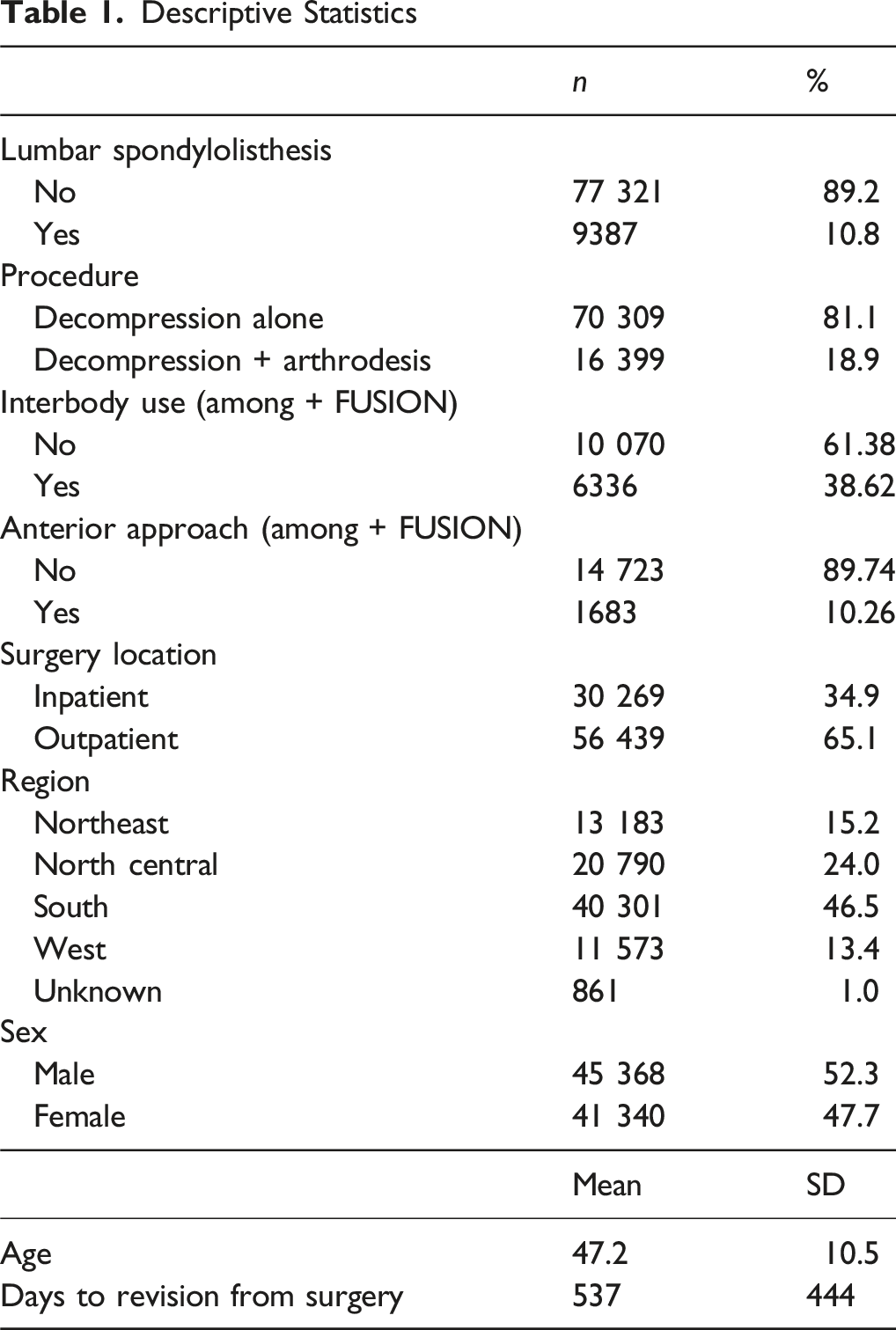
Descriptive Statistics
Expected Treatment
Descriptive Statistics (cont.)
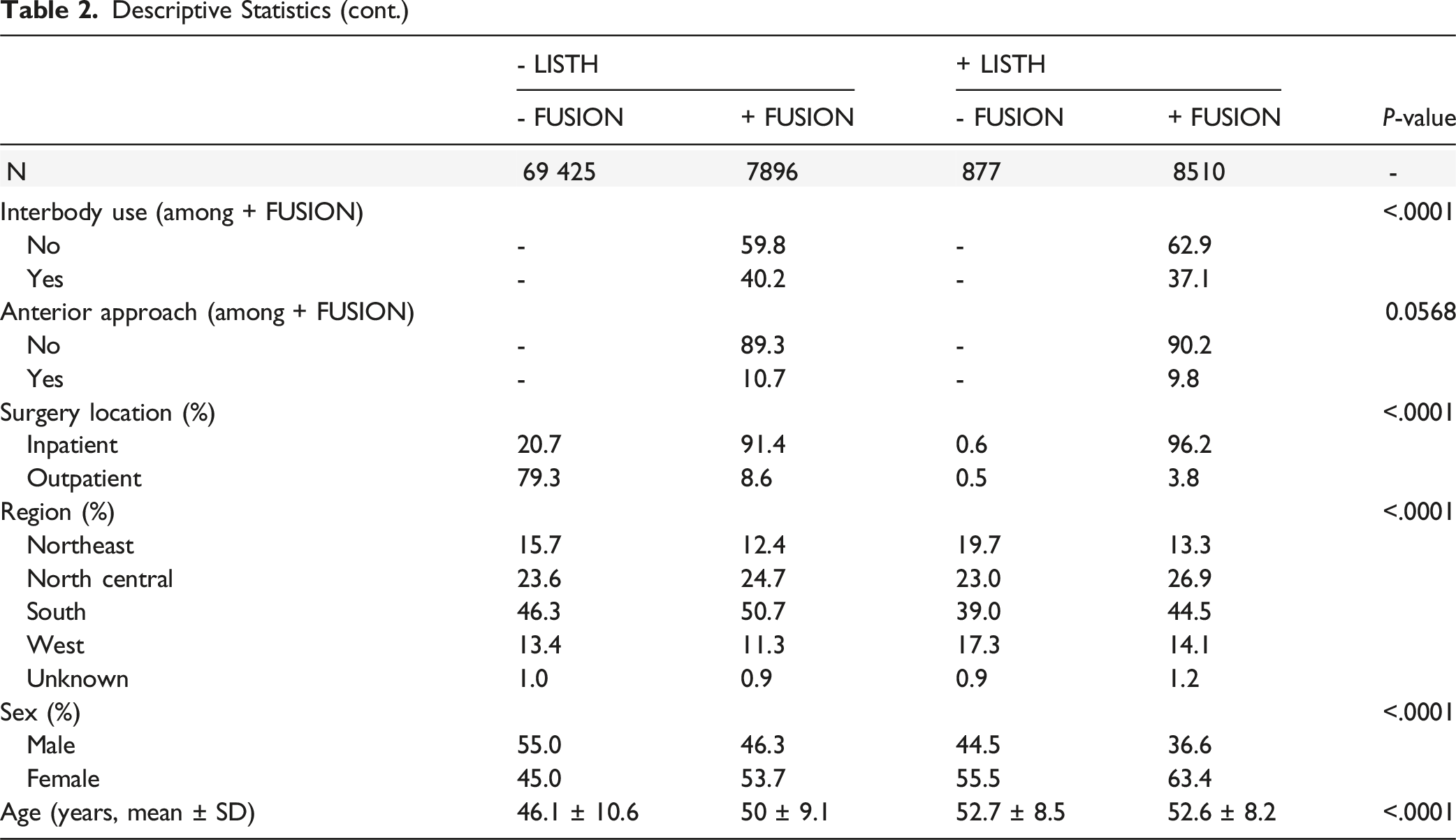
Patients undergoing arthrodesis were significantly more likely to have had surgery inpatient (93.9% inpatient for arthrodesis vs 21.2% inpatient for decompression alone, P < 0.0001), to be female (58.8% female for arthrodesis vs 45.1% female for decompression alone, P < 0.0001), and to be older (mean age 51.3 [SD 8.8] for arthrodesis vs 46.2 years [SD 10.6] for decompression alone).
Revision Rates
In Kaplan-Meier analysis, revision surgery at 2- and 5-year post-operatively occurred in 10.4% and 17.4% of patients overall, respectively. Among patients with spondylolisthesis, the revision rate at 5 years was 20.3% for patients who underwent decompression alone, vs 15.2% for those who underwent arthrodesis with decompression. Using proportional hazards regression, the occurrence of revision was significantly lower for those who underwent arthrodesis with decompression vs decompression alone in both unadjusted (HR 0.63, P < 0.0001), and adjusted analysis (aHR 0.76, P = 0.0094) (Figure 1). Revision Surgery by Listhesis and Arthrodesis Status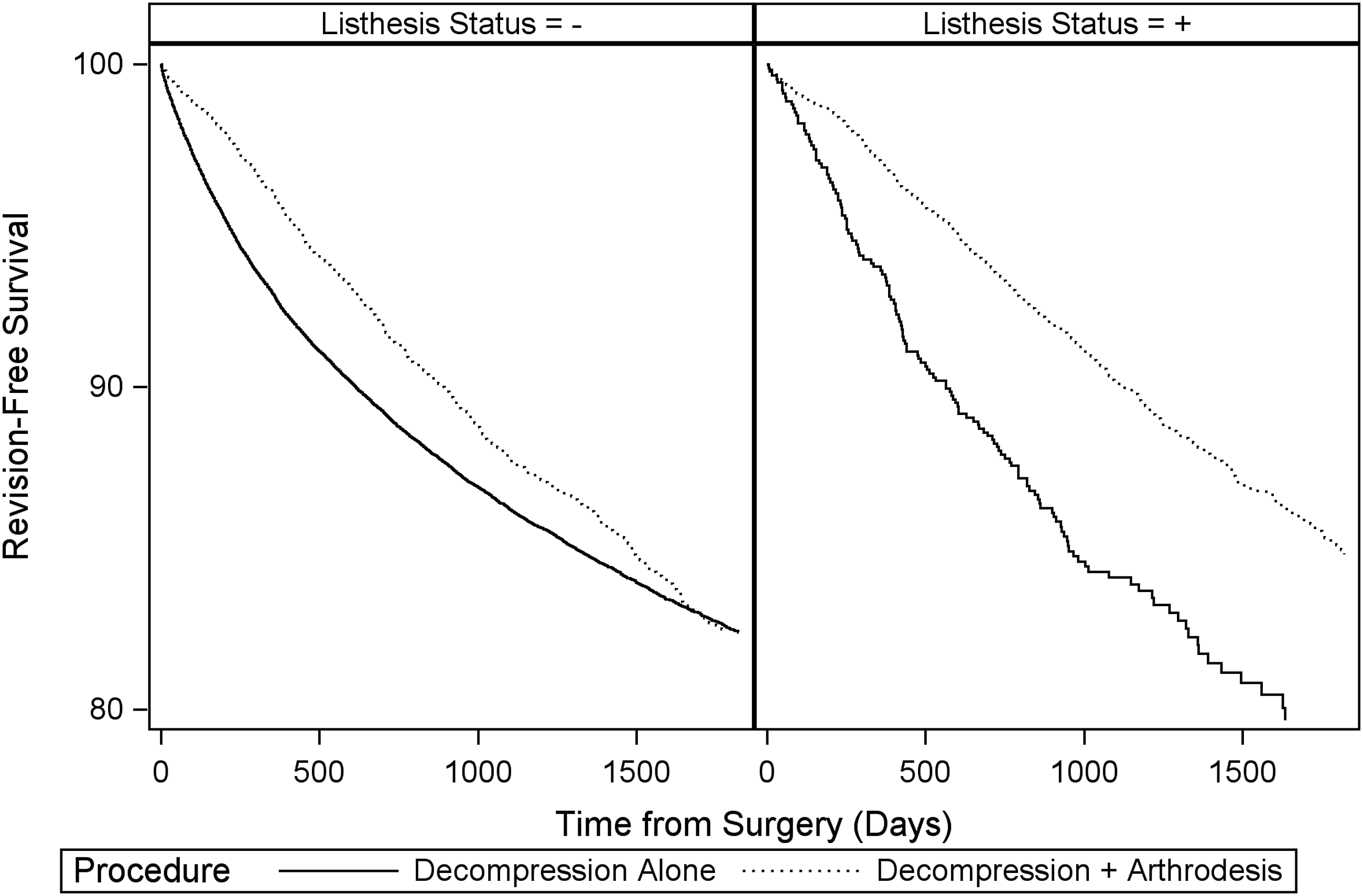
Among patients without spondylolisthesis, revision rates at 2 years post-operatively were 11.2% for -LISTH, -FUSION, and 8.6% for -LISTH, +FUSION. At 5 years post-operatively, revision rates were 17.6% for -LISTH, -FUSION, and 17.6% for -LISTH, +FUSION. In proportional hazards regression, no significant difference in revision occurrence was observed over the overall study period for -LISTH, +FUSION vs -FUSION (aHR 0.94, P = 0.1164). Examination of the Kaplan-Meier plot for patients without spondylolisthesis indicated initial divergence of revision rates, followed by convergence later in the study. Given this non-proportionality of hazards, we analyzed interval hazard ratios from 0 – 2 years and 2 – 5 years after surgery. We observed an initial lower occurrence of revision from 0 – 2 years among patients undergoing arthrodesis with decompression vs decompression alone (0 – 2 years, -LISTH, +FUSION vs -FUSION: aHR 0.77, P < 0.0001), but a higher occurrence of revision for the same comparison between 2 – 5 years (2 – 5 years, -LISTH, +FUSION vs -FUSION: aHR 1.43, P < 0.0001).
Discussion
In this study of patients with lumbar stenosis, approximately 90% received expected treatment: those with spondylolisthesis more likely underwent arthrodesis with decompression compared with patients without spondylolisthesis, who more likely underwent decompression alone. Among patients with spondylolisthesis, the revision rate at 5 years was lower in patients who underwent arthrodesis with decompression compared with decompression alone. Finally, in patients without spondylolisthesis, revision rates were higher starting year 2 and up to year 5, among those treated with additional arthrodesis despite no documented instability.
Our findings regarding revision rates among patients with spondylolisthesis corroborates a study by Ghogawal et al. 3 In their randomized controlled trial, they found that the rate of reoperation was significantly lower among patients with degenerative spondylolisthesis who underwent laminectomy with posterolateral instrumented fusion (14%) compared with those who only underwent decompressive laminectomy alone (34%). Additional investigations similarly found a lower reoperation rate among patients with lumbar stenosis who underwent fusion compared with decompression alone.7-9 Furthermore, several studies have demonstrated that the addition of arthrodesis with decompression for the treatment of spinal stenosis with spondylolisthesis results in improved clinical outcomes.3,10-13 Although Pieters et al 14 found that patients who underwent fusion for lumbar spondylolisthesis had a higher rate of unplanned return to the OR (3.0%) compared to patients who underwent decompression (1.0%), their study did not analyze minimally invasive techniques. This may have resulted in higher reoperation rates for their fusion group, as it failed to include patients who underwent indirect decompression from techniques such as minimally invasive transforaminal lumbar interbody fusion.15,16 While patients with spondylolisthesis are often treated with fusion to address potential progression of slip and dynamic instability, 17 Staartjes et al demonstrated that a decision-making protocol can be utilized to determine whether a patient should undergo decompression with or without arthrodesis to reduce the risk for complications and revision surgery. 7
The present study found that despite an initial divergence in revision rates at 2 years among patients without spondylolisthesis who underwent decompression alone vs decompression with arthrodesis, revision rates converged by 5 years. Notably, there was no significant difference in overall revision rates between our 2 cohorts. Moayeri et al similarly found an identical reoperation rate (7.5%) between patients who had undergone fusion or decompression alone for spinal stenosis without degenerative lumbar spondylolisthesis. 18 Additionally, Martin et al 19 reported an overall reoperation rate of 17.1% for patients with spinal stenosis without spondylolisthesis, which aligns with the results of our study. Several other investigations have also showed that the addition of arthrodesis in the treatment of lumbar stenosis without spondylolisthesis did not impact or reduce reoperation rates,5,20,21 with Grob et al 22 reporting no significant difference in clinical outcomes among patients receiving fusion vs decompression alone for the treatment of spinal stenosis without instability.
This study has several limitations. There is a notable absence of clinical details in the MarketScan database, and our analysis relies on appropriate diagnostic coding, which can be prone to data entry errors. Further, the dataset does not include information regarding specific surgical factors (eg, implant types, decompression technique, etc.) that could have impacted overall revision rates. Furthermore, the decision to perform a revision procedure ultimately falls upon surgeon discretion, with reoperation thresholds varying on a surgeon-to-surgeon basis. In particular, it is possible that there is increased surgeon predisposition to revise following decompression alone given the option of potential fusion, whereas there may be less predisposition to perform a revision arthrodesis. We also do not have the clinical reasons for revisions, and the revision rates are for all-causes. Additionally, we were unable to assess whether the revision is at the index level, a level adjacent to the index level, or further remote. These clinical details are unfortunately not included in the MarketScan database and would require retrospective or prospective clinical studies to assess. While we included age at surgery, sex, outpatient vs inpatient surgery, region, interbody use, and anterior approach for arthrodesis in our multivariable analyses, the possibility of unknown confounding variables remains, as is the case with all non-randomized retrospective studies. Finally, the MarketScan database is based on a large convenience sample and is limited to patients who have commercial insurance. This may affect the generalizability and applicability of our results, especially since a large cohort of the population is enrolled in Medicare or Medicaid insurances. The insurance plans included in the MarketScan database, while large, are not designed to be proportionally representative of the United States population, or even the population of commercially insured individuals. Given the potential impact of insurance coverage on access to care, it is highly likely that differential dynamics may be observed for patients with public insurance or, particularly, no insurance.
Despite these limitations, to our knowledge, this is the first study to characterize long-term revision rates in patients with and without spondylolisthesis undergoing single-level lumbar decompression with and without arthrodesis. Our study also identifies revision rate temporal trends associated with each procedure, which could help guide surgeons when recommending surgical treatment options to their patients. Future studies should prospectively examine the long-term operative courses for each procedure and identify potential risk factors in each cohort that increases the risk for revision surgery.
Conclusion
In this retrospective cohort study, among patients undergoing single-level lumbar decompression, the majority of patients without spondylolisthesis underwent decompression alone, and the majority of patients with spondylolisthesis underwent arthrodesis with decompression. Those with spondylolisthesis who underwent arthrodesis with decompression demonstrated lower revision rates at 5-year follow-up than decompression alone.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.