
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To assess for racial differences in opioid utilization prior to and after lumbar fusion surgery for patients with lumbar stenosis or spondylolisthesis.
Methods:
Clinical records from patients with lumbar stenosis or spondylolisthesis undergoing primary <3-level lumbar fusion from 2007 to 2016 were gathered from a comprehensive insurance database. Records were queried by International Classification of Diseases diagnosis/procedure codes and insurance-specific generic drug codes. Opioid use 6 months prior, through 2 years after surgery was assessed. Multivariate regression analysis was employed to investigate independent predictors of opioid use following lumbar fusion.
Results:
A total of 13 257 patients underwent <3-level posterior lumbar fusion. The cohort racial distribution was as follows: 80.9% white, 7.0% black, 1.0% Hispanic, 0.2% Asian, 0.2% North American Native, 0.8% “Other,” and 9.8% “Unknown.” Overall, 57.8% patients utilized opioid medications prior to index surgery. When normalized by the number opiate users, all racial cohort saw a reduction in pills disbursed and dollars billed following surgery. Preoperatively, Hispanics had the largest average pills dispensed (222.8 pills/patient) and highest average amount billed ($74.67/patient) for opioid medications. The black cohort had the greatest proportion of patients utilizing preoperative opioids (61.8%), postoperative opioids (87.1%), and long-term opioid utilization (72.7%), defined as use >1 year after index operation. Multivariate logistic regression analysis indicated Asian patients (OR 0.422, 95% CI 0.191-0.991) were less likely to use opioids following lumbar fusion.
Conclusions:
Racial differences exist in perioperative opioid utilization for patients undergoing lumbar fusion surgery for spinal stenosis or spondylolisthesis. Future studies are needed corroborate our findings.
Introduction
Racial disparities in the management of pain are pervasive within the American health care system. 1 A robust body of literature has demonstrated differential resource allocation along racial lines with regard to many treatment modalities. 2 -4 This includes the use of opioids, which remain commonly utilized agents in a variety of clinical settings. 4 -6 The reasons for this observed variance are thought to involve complex interactions between social, cultural, and contextual factors, 7 -9 with metabolism of opioids themselves having also been demonstrated to show racial differences. 10,11 While numerous studies have demonstrated that non-Hispanic whites receive more opioids for acute pain than other races, 12 -14 the directionality of racial differences in opioid use for chronic and perioperative pain is often less clear. 3,5,15,16 Better characterizing the relationship of race with chronic and perioperative opioid use acquires increasing importance at a time when policies for opioid prescriptions in noncancer pain are being reexamined.
Common indications for opioid use includes low back pain, 17 a condition that affects over 80% of the population at some point during their lifetime and is one of the most common reasons people pursue medical care in the United States. 18,19 The prevalence of chronic low back pain is increasing, and this rise is occurring across racial/ethnic groups. In a cross-sectional study of US households, Freburger et al 18 determined that over a 14-year period the prevalence of chronic impairing low back pain increased by 162% overall, with an increase of 155% seen in non-Hispanic whites, an increase of 226% seen in non-Hispanic blacks, and an increase of 120% seen in people identifying as other races. 18
Management of chronic low back pain, caused by underlying conditions such as symptomatic lumbar stenosis or spondylolisthesis, often involves a trial of nonoperative therapy with a subset of patients eventually requiring operative measures. 20 Opioids are a mainstay of treatment both during conservative therapy trials as well as throughout the perioperative period. 17,21,22 Whether racial variations exist in opioid use following lumbar fusion surgery for low back pain remains unknown.
To that end, the aim of this study was to evaluate for racial differences in the perioperative utilization of opioid medications in lumbar decompression and fusion surgery for patients diagnosed with lumbar stenosis or spondylolisthesis.
Methods
Data Source
The study population was retrieved from The Humana Ortho (HORTHO) database, which consists of 20.9 million private/commercially insured and Medicare Advantage beneficiaries with an orthopedic diagnosis. Patient information was accessed through a remote server hosted by PearlDiver (PearlDiver Technologies, Inc, Colorado Springs, CO). Clinical records were queried by International Classification of Diseases (ICD) diagnosis and procedure codes and generic drug codes specific to Humana.
Patient Sample
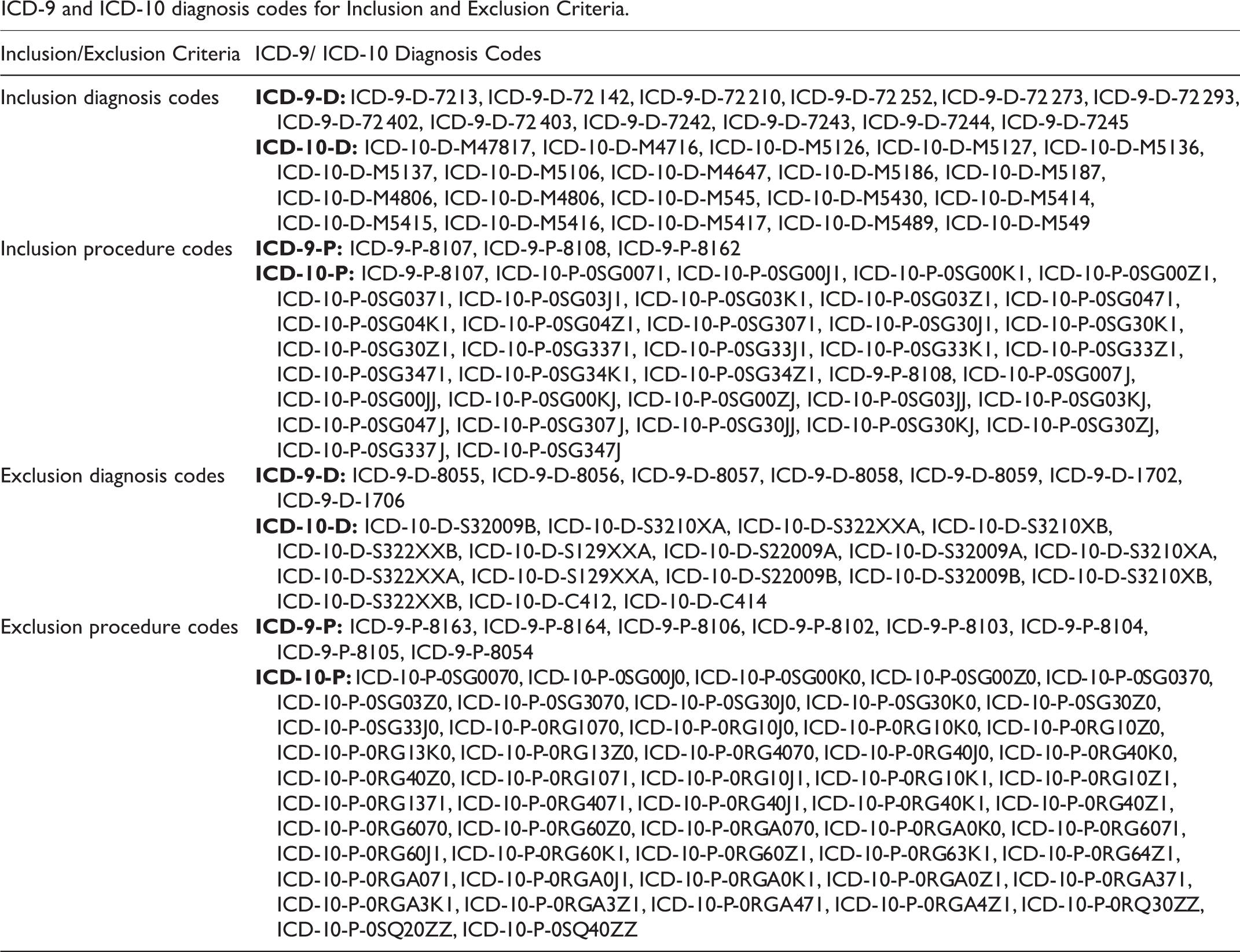
We considered adult patients (≥19 years old) with degenerative conditions of the lumbosacral spine who underwent an index lumbar decompression and fusion procedure between 2007 and 2016. More specifically, patients undergoing primary ≤3-level lumbar spinal fusion surgery (ICD-9: 8107, 8108, 8162) were collected. No distinction was made between traditional open and minimally invasive operative approaches. Only patients with a documented diagnosis of lumbar stenosis (ICD-9: 72 402, 72 403), spondylolisthesis (ICD-9: 7213, 72 142), intervertebral disc degeneration (ICD-9: 72 252, 72 210, 72 273, 72 293), or low back pain (ICD-9: 72 420, 72 440, 72 450) prior to their index fusion surgery were considered. Patients were omitted if they underwent >3 level lumbar fusions (ICD-9: 8163, 8164), an anterior fusion technique (ICD-9: 81.06), or had a history of cervical (ICD-9: 8102, 8103) or thoracic fusion (ICD-9: 8104, 8105). Moreover, patients with a concurrent diagnosis of spinal fracture (ICD-9: 8054, 8055, 8056, 8057, 8058, 8059) or spinal malignancy (ICD-9: 1702, 1706) were excluded. For each of the aforementioned ICD-9 codes, the relevant corresponding ICD-10 codes were incorporated into the patient selection/exclusion criteria (Appendix A).
Opioid Use
Opioid use 6 months prior to index surgery through 2 years after surgery was considered for analysis. Generic opioid codes specific to Humana were used to capture prescriptions of interest before and after surgery (Appendix B). Specifically, the most frequently prescribed opiate formulations were queried, including oxycodone hydrochloride, hydrocodone/acetaminophen and oxycodone/acetaminophen, which were prescribed in the majority (>80%) of patients. For perioperative narcotic utilization comparisons, opioid use was normalized to number of pills per opioid user per month.
Baseline Demographics and Comorbidities
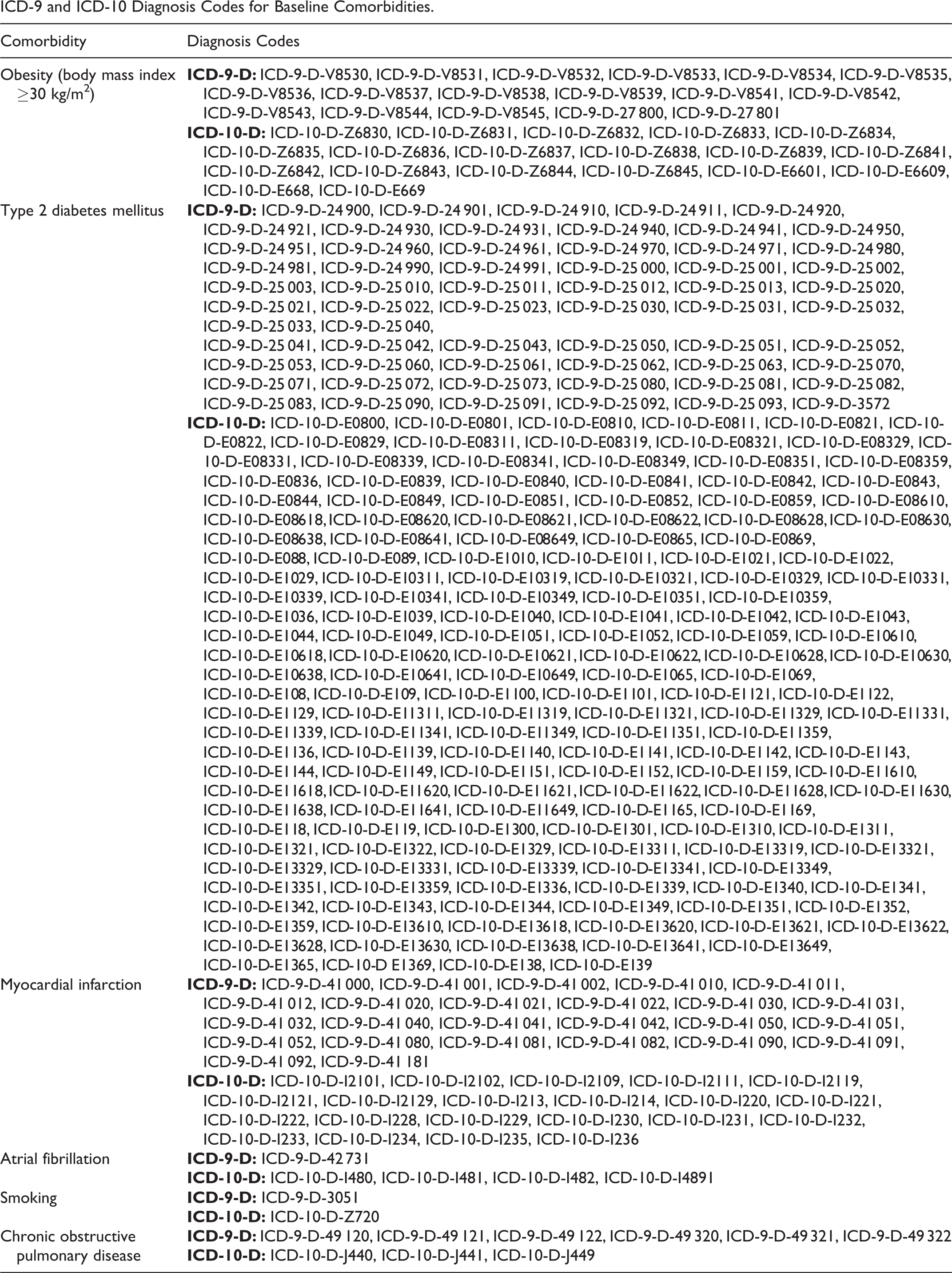
Demographic information including age, gender, geographical region, and ethnicity was captured. As a patient privacy measure, the HORTHO patient age data is binned into buckets consisting of 5-year intervals. Patient ethnicity identification groups were as follows: white, black, Asian, Hispanic, North American Native, and Other. Additionally, a designation of “Unknown” was assigned to patients opting not to make a selection. Patient geographic region was separated into 4 regions (Midwest, Northeast, South, West) consistent with US census bureau definitions, and was based on the location from where the insurance claim was initiated. Additionally, ICD-9 and ICD-10 diagnosis codes were used to collect preoperative comorbidities known to influence outcomes in spinal surgery, which included obesity (body mass index ≥30 kg/m2), type 2 diabetes mellitus (DM), smoking status, atrial fibrillation, myocardial infarction, and chronic obstructive pulmonary disease (COPD) (Appendix C). As an additional variable, hospital length of stay (LOS) associated with the index lumbosacral fusion was obtained.
Data Analysis
The primary objective of this study was to evaluate for racial differences in opioid utilization before and after primary lumbar decompression and fusion surgery. Direct statistical comparisons of opioid use were performed between demographic cohorts via chi-square tests when appropriate, with P < .05 considered statistically significant. The secondary aim was to investigate for independent predictors of postoperative opioid use. Demographic variables and preoperative comorbidities including age, gender, race, geographic region, obesity, hospital LOS, and a history of narcotic use 6 months prior to fusion served as covariates in the regression model. Multivariate logistic regression analysis was completed to identify independent predictors of any postoperative opioid use up to 2 years after surgery. The analysis was performed in R (The R Project for Statistical Computing) via the PearlDiver platform. It should be noted that patient age 20 to 24 years, female gender, white race, and Midwest region were used for the multivariate baseline comparison group for age, gender, race, and region, respectively. The term “cost,” was used to represent the actual amount paid by insurers.
Results
Patient Sample
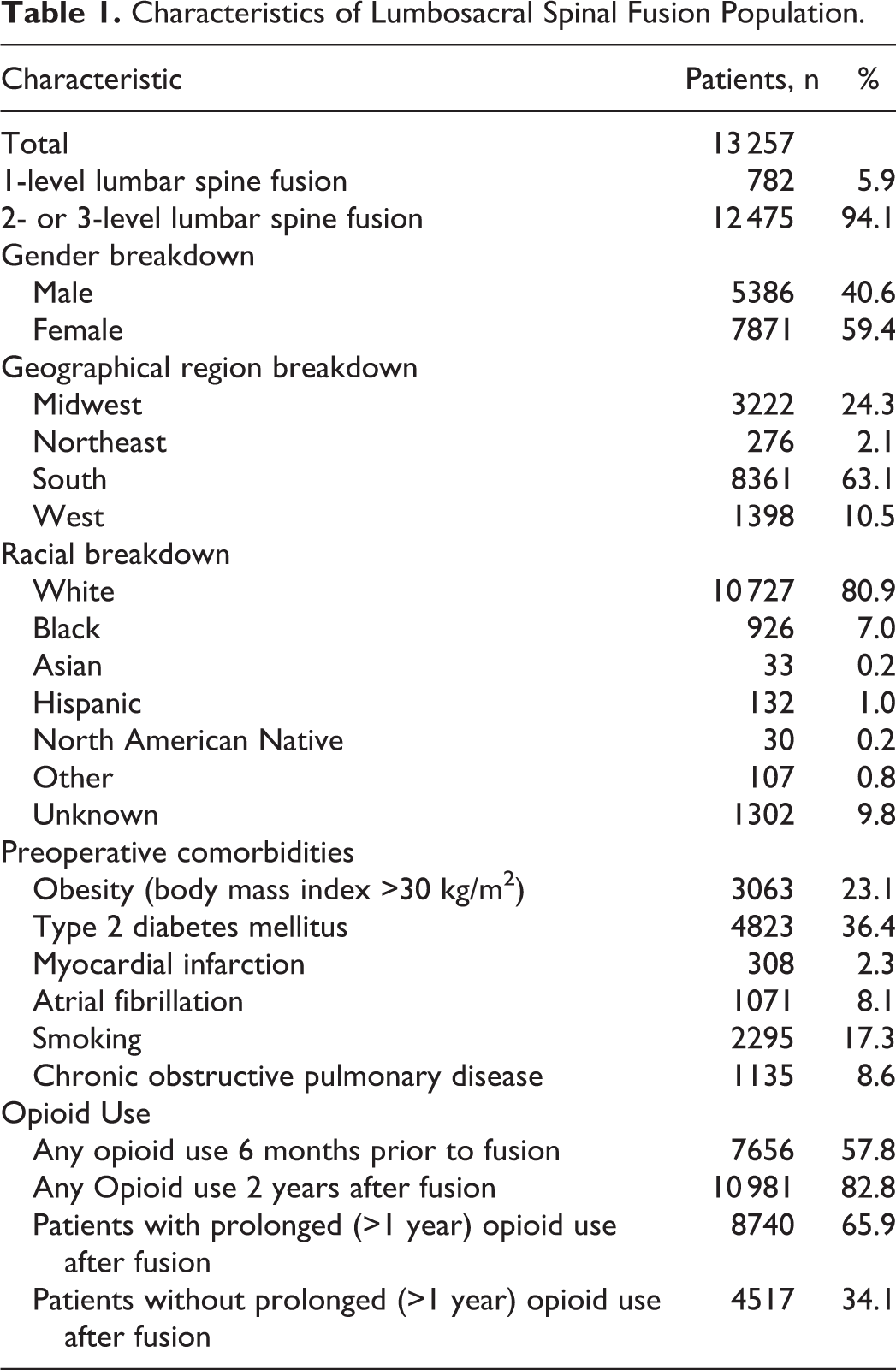
A total of 13 257 patients underwent a 1-, 2-, or 3-level posterior lumbar decompression with instrumented fusion and fulfilled the inclusion criteria (Table 1). Females (59.4%) and patients from the South (63.1%) comprised the majority of the population. The racial distribution was as follows: 80.9% white, 7.0% black, 1.0% Hispanic, 0.2% Asian, 0.2% North American Native, and 0.8% other. Additionally, 9.8% of the population did not identify with any particular race (Unknown) (Table 1). Type 2 DM (36.4%), obesity (23.1%), and smoking history (17.3%) were the most prevalent preoperative comorbidities (Table 1).
Characteristics of Lumbosacral Spinal Fusion Population.
Preoperative Opioid Use
Overall, 7656 (57.8%) patients had a history of opioid use prior to the index surgery (Table 1). Looking at the percentage of patients from each racial affiliation group with preoperative opioid utilization, 58.1% of whites, 61.8% of blacks, 60.6% of Asians, 54.5% of Hispanics, 36.7% of North American Natives, 49.5% of other, and 53.8% of unknown cohorts had documented narcotics use (Table 2). Over the 6-month preoperative period, a total of 2 368 008 opioid pills were billed for. Average pill count was highest in Hispanics (228.8 pills/patient) followed by whites (183.0 pills/patient) and blacks (174.9 pills/patient) (Table 3). When normalized by actual opioid users per month, North American Natives had the highest utilization (71.1 pills/opioid user/month) followed by Hispanics (69.9 pills/opioid user/month) and whites (52.5 pills/opioid user/month) (Table 3). The Asian cohort had the lowest average pill count and opioid user normalized pill count (102.1 pills/patient and 28.1 pills/opioid user/month, respectively). The total costs of opioids billed over a 6-month period prior to index surgery was $737 215. Hispanics on average billed the most for preoperative opioids ($74.67/patient), followed by the unknown cohort ($62.00/patient) and the Black population ($57.70/patient) (Table 4). Normalizing by dollars billed per opioid user per month, the Hispanic population remained the highest at $22.82/opioid user/month.
Racial Demographic Comparison of Perioperative Opioid Utilization, n (%).

Racial Demographic Comparison of Perioperative Opioid Pills Billed.a
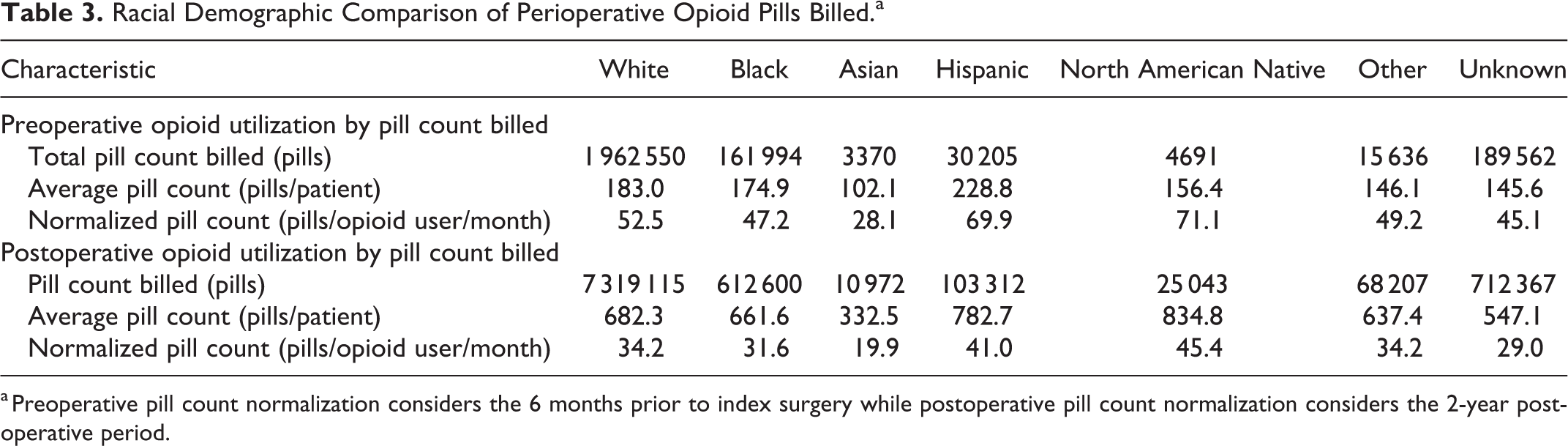
a Preoperative pill count normalization considers the 6 months prior to index surgery while postoperative pill count normalization considers the 2-year postoperative period.
Racial Demographic Comparison of Perioperative Dollars Billed for Opioids.a
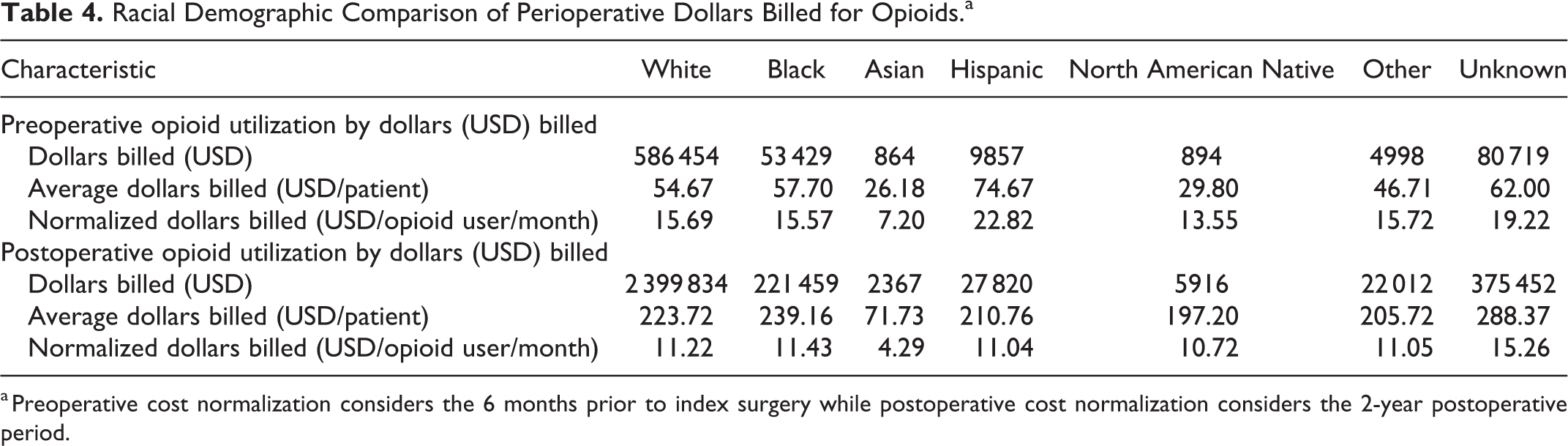
a Preoperative cost normalization considers the 6 months prior to index surgery while postoperative cost normalization considers the 2-year postoperative period.
Postoperative Opioid Use
Overall, 82.8% of our cohort utilized opiates within the 2-year postoperative period (Table 1). Additionally, 65.9% of our patients were identified to have continuous opioid use at 1-year postoperatively. The racial cohort breakdown for prolonged postoperative opioid use was as follows: black 72.7%, North American Native 70.0%, white 66.6%, Hispanic 65.2%, other 59.8%, Asian 57.6%, and unknown 55.9% (Table 2). Patients of North American Native race had the largest average pill count billed per month (834.8 pills/month) followed by Hispanics (782.7 pills/month) (Table 3). Similarly, when normalized by number of opioid users per month, the highest pill counts were derived from the North American Native (45.4 pills/opioid user/month) and Hispanic (41.0 pills/opioid user/month) racial cohorts (Table 3). Considering the average and normalized dollars billed cohort comparisons, patients of unknown ($288.37/patient and $15.26/opioid user/month, respectively) and black ($239.16/patient and $11.43/opioid user/month, respectively) race had the highest costs (Table 4). Patients of Asian descent had the least postoperative opioid utilization across all measured pill count and dollars billed metrics.
The results indicate that all racial cohorts had an increase in opioid use following lumbar spinal fusion (Table 2). Similarly, all racial cohorts except for Asians saw an increase in the proportion of patients with prolonged opioid use compared with the percentage of patients with any preoperative opioid use. However, comparing the pill counts and dollars billed when normalized per opioid user per month, it can be seen that there is a decrease in both metrics across all racial cohorts (Tables 3 and 4).
Predictors of Postoperative Opioid Use After Surgery
In a multivariate logistic regression analysis, patients of Asian (odds ratio [OR] 0.422, 95% confidence interval [CI] 0.191-0.991) racial identification were less likely than white patients to use opioids following lumbar decompression and fusion surgery (Table 5). Additionally, patients with a history of obesity (OR 1.198, 95% CI 1.058-1.358), preoperative opioid use (OR 5.847, 95% CI 5.254-6.517), patients receiving treatment in the South (OR 1.228, 95% CI 1.096-1.374), West (OR 1.362, 95% CI 1.139-1.634), and age groups 25-29, 35-39, and 45-49 years old were more likely to use postoperative opioids compared with their baseline comparative cohort (Table 5).
Multivariate Regression Results.a
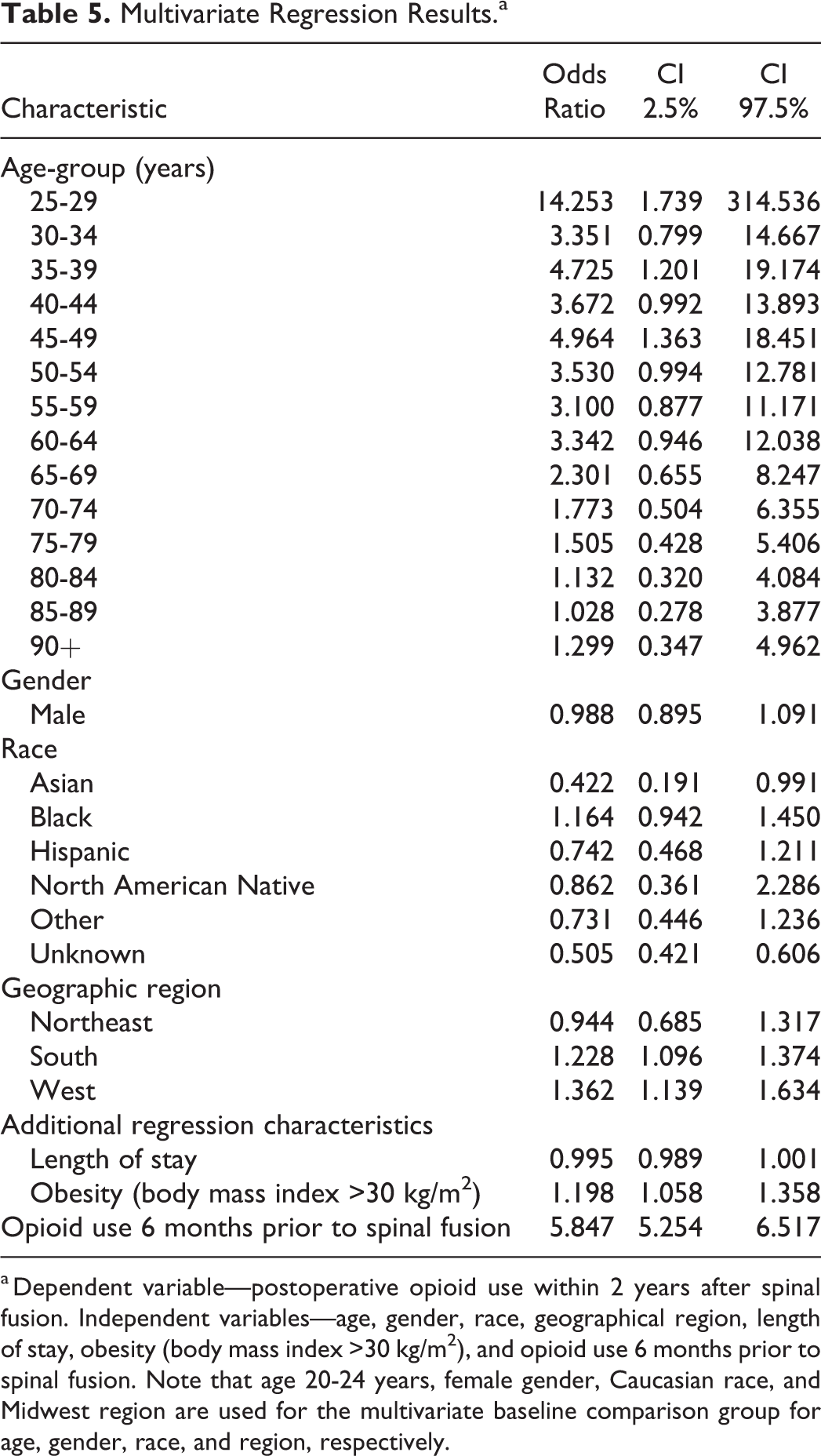
a Dependent variable—postoperative opioid use within 2 years after spinal fusion. Independent variables—age, gender, race, geographical region, length of stay, obesity (body mass index >30 kg/m2), and opioid use 6 months prior to spinal fusion. Note that age 20-24 years, female gender, Caucasian race, and Midwest region are used for the multivariate baseline comparison group for age, gender, race, and region, respectively.
Discussion
In this retrospective study of 13 257 patients undergoing 1-, 2-, or 3-level posterior lumbar instrumented fusion for symptomatic lumbar stenosis or spondylolisthesis, we demonstrated that overall 7656 (57.8%) patients had a history of opioid use prior to index surgery, 10 981 (82.8%) patients used opioids within 2 years after surgery, and 8740 (65.9%) patients had prolonged (>1 year) usage of opioids following surgery. In terms of racial distribution of opioid use, the black cohort had the largest proportion of patients using opioids preoperatively (61.8%), the largest proportion who used opioids within 2 years after surgery (87.1%), as well as the largest proportion with long-term continuous opioid use following surgery (72.7%). Preoperatively, Hispanics were found to have the highest average pill count (222.8 pills/patient) as well as the highest amount billed for opioids ($74.67/patient). Postoperatively, multivariate logistic regression demonstrated that Asian patients (OR 0.422, 95% CI 0.191-0.991) were less likely than white patients to use opioids following lumbar decompression and fusion surgery.
Our findings are consistent with previous studies that have demonstrated racial differences in perioperative opioid use. In a retrospective study of chronic opioid use in 79 123 surgical patients, Jiang et al 15 found that African Americans (OR 1.59, 95% CI 1.49-1.69) and Hispanic Latinos (OR 1.38, 95% CI 1.11-1.70) were more likely to become chronic opioid users than Caucasians. These authors also found that Asian surgical patients (OR 0.63, 95% CI 0.48-0.82) were less likely to become chronic opioid users than Caucasians. 15 Additionally, in a retrospective study of 578 patients undergoing spine surgery, Walid and Zaytseva 16 found that significantly more African American patients undergoing lumbar decompression and fusion procedures used opioids than did Caucasian patients (69.2% vs 40.6%, P < .01). The results from these studies are similar to our findings, in which the black cohort had the highest proportion of opioid users both before and after lumbar decompression and fusion surgery, and the Asian cohort was significantly less likely than whites to receive opioids postoperatively.
There are multiple factors that may contribute to the racial variation in opioid use in chronic and perioperative pain demonstrated in the literature. Pain sensitivity/thresholds are one such factor that have been shown to differ based on race. In a systematic literature review and analysis of ethnic group responses to painful stimuli, Rahim-Williams et al 23 found consistent evidence that across different stimulus modalities African Americans had lower pain tolerance and rated suprathreshold stimuli higher than non-Hispanic white counterparts. A prospective study by Campbell et al 24 also determined that African Americans had lower tolerance to heat, cold pressor, and ischemic pain than whites. Similar findings of lower pain threshold and reduced tolerance to pain have been demonstrated in Asians compared with non-Hispanic whites as well. 25 The underlying mechanisms for such differences have not been fully elucidated; however, cultural factors are thought to play a role. For example, Chan et al 26 found that when examining first- and second-generation Asian Americans versus their European American counterparts, that only the first-generation Asian Americans had heightened pain response, thus suggesting that acculturation may play a role in pain sensitivity.
Efficacy and response to opioid medications have also been shown to vary by race/ethnicity. Commonly utilized opioid medications including morphine, codeine, and hydrocodone have all been shown to exhibit altered metabolism in populations of Asian or African descent based on different rates of clearance as well as frequencies of CYP2D6 enzyme polymorphisms. 10,11 In the clinical setting, a prospective observational study examining the effect of race on analgesia requirements by Sadhasivam et al 6 demonstrated that African American children undergoing tonsillectomy had greater postoperative morphine requirements as well as higher postoperative pain scores than Caucasian children following administration of similar intraoperative doses. African American children were also found to better tolerate high doses of morphine and experienced fewer side effects than Caucasians. 6 In a prospective matched cohort study of 68 Caucasian patients and 68 Chinese patients undergoing major abdominal surgery, Konstantatos et al 27 determined that the average opioid requirement following surgery was significantly less in Chinese patients compared with Caucasian patients when both cohorts were given access to patient controlled analgesia. This was despite Chinese patients reporting higher pain levels. The authors determined through questionnaires that patient expectations and preferences regarding treatment also differed significantly between Chinese and Caucasian patients, further demonstrating the complex interplay of numerous biopsychosocial factors in the experience of pain and response to therapy. The collective findings that African Americans may have increased opioid requirements after surgery compared with Whites, while Asians may have decreased requirements, could contribute to the racial variance in opioid use observed in our study.
The results from the current study are particularly germane in the setting of recent health initiatives and policy trends. Disparities in healthcare delivery have been identified as critical areas for improvement in the US health care system, with initiatives such as Healthy People 2010 by the US Department of Health and Human Services having sought to eliminate racial and ethnic health inequalities as primary targets. 1 Additionally, the World Health Organization has stated that access to adequate pain relief is a fundamental human right. 4 Balancing these concepts at a time when responsible stewardship of opioids in noncancer pain is also being emphasized requires thorough elucidation of where disparities in opioid use lie. While oligoanesthesia in minorities, particularly African Americans, has been demonstrated numerous times in the literature, our current study found no significant difference in opioid use following lumbar decompression and fusion surgery between whites and blacks on multivariate analysis. Furthermore, higher proportions of African Americans utilized opioids both prior to and following index surgery than any other race. Our study additionally adds to recent literature suggesting Asians may receive less opioids following surgery than other races. 15 It is important to recognize that numerous other cultural, social, and contextual factors may also influence racial variations in opioid use. Structural barriers to accessing opioids in the United States have additionally been demonstrated. These include that pharmacies serving primarily minority neighborhoods may carry smaller supplies of opioids, as well as that ethnic minorities may have limited access to pain specialists. 4,7,28 Further studies are needed to corroborate our findings in perioperative settings.
Limitations
The results and implications of this study should be considered within the context of its limitations. First, the HORTHO database consists only of private/commercially insured patients and Medicare Advantage beneficiaries. Consequently, Medicaid patients with a potentially differing demographic profile were precluded from this investigation. Our racial cohort breakdown includes a significant percentage of patients who opted to withhold their racial affiliation and were consequently identified as “Unknown.” This has the potential to alter the results of our analysis, especially if a considerable proportion derived from less represented minority cohorts. It is important to note that the HORTHO database only documents claims that are filed through the Humana insurance system. Consequently, any prescription and/or therapy activity rendered outside Humana such as over-the-counter analgesic therapies, holistic pain management strategies, or personally-financed nonoperative treatments were not considered in the current analysis. Additionally, when investigating racial demographic differences in treatment utilization, it is difficult to analyze the quantity of therapy use in isolation from access to clinical care. Unfortunately, there were no available variables that comprehensively characterized patient socioeconomic status or access to medical services. Last, we utilized a large administrative database which lacks patient-level diagnostic and clinical context that could influence our findings. Despite these limitations, this study demonstrated that racial differences exist in perioperative opioid utilization for patients undergoing lumbar decompression and fusion surgery for symptomatic stenosis or spondylolisthesis.
Conclusion
This study suggests that racial differences exist in perioperative opioid utilization for patients undergoing lumbar decompression and fusion surgery for symptomatic stenosis or spondylolisthesis. Future studies are needed to corroborate our findings.
Footnotes
Appendix A
ICD-9 and ICD-10 diagnosis codes for Inclusion and Exclusion Criteria.
| Inclusion/Exclusion Criteria | ICD-9/ ICD-10 Diagnosis Codes |
|---|---|
| Inclusion diagnosis codes |
|
|
|
|
| Inclusion procedure codes |
|
|
|
|
| Exclusion diagnosis codes |
|
|
|
|
| Exclusion procedure codes |
|
|
|
Appendix B
Humana Generic Drug Codes for Inclusion Narcotics.

| Inclusion Medications | Humana-Specific Generic Drug Codes |
|---|---|
| Opioids |
|
Appendix C
ICD-9 and ICD-10 Diagnosis Codes for Baseline Comorbidities.
| Comorbidity | Diagnosis Codes |
|---|---|
| Obesity (body mass index ≥30 kg/m2) |
|
|
|
|
| Type 2 diabetes mellitus |
|
| ICD-9-D-25 041, ICD-9-D-25 042, ICD-9-D-25 043, ICD-9-D-25 050, ICD-9-D-25 051, ICD-9-D-25 052, ICD-9-D-25 053, ICD-9-D-25 060, ICD-9-D-25 061, ICD-9-D-25 062, ICD-9-D-25 063, ICD-9-D-25 070, ICD-9-D-25 071, ICD-9-D-25 072, ICD-9-D-25 073, ICD-9-D-25 080, ICD-9-D-25 081, ICD-9-D-25 082, ICD-9-D-25 083, ICD-9-D-25 090, ICD-9-D-25 091, ICD-9-D-25 092, ICD-9-D-25 093, ICD-9-D-3572 | |
|
|
|
| Myocardial infarction |
|
|
|
|
| Atrial fibrillation |
|
|
|
|
| Smoking |
|
|
|
|
| Chronic obstructive pulmonary disease |
|
|
|
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.