
Abstract
Study Design
Retrospective study.
Objective
This study aimed to investigate the association between preoperative patient expectations and postoperative satisfaction in elderly patients with adult spinal deformity (ASD), with particular emphasis on identifying potential dose-response relationships.
Methods
We conducted a retrospective cohort study of elderly patients (aged ≥65 years) with ASD undergoing thoracolumbar fusion surgery at our institution. Participants were stratified into satisfied and dissatisfied cohorts based on postoperative the North American Spine Society (NASS) satisfaction scores assessed at follow-up. Comprehensive data collection included demographic characteristics, radiological parameters, surgical variables, and perioperative outcomes. Propensity score matching using the nearest-neighbor method was applied to both groups of patients. Conditional logistic regression models adjusted for confounders were employed to assess associations. Nonlinear relationships were investigated through smoothed curve fitting with covariate adjustment. Threshold effects were analyzed using piecewise regression models, with receiver operating characteristic (ROC) curve analysis validating optimal cutoff values.
Results
In our study involving 234 elderly patients with ASD undergoing thoracolumbar fusion surgery between September 2019 and September 2022, we analyzed statistically significant differences between a case group (patient dissatisfied) and a control group (patient satisfied). We matched 82 patients in each group using nearest-neighbor matching. Despite this matching, there were still significant differences in key variables such as American Society of Anesthesiologists (ASA), Age-adjusted Charlson Comorbidity Index (ACCI), complications, previous spine surgery, perioperative outcomes, and preoperative expectation (P < .05). In our fully adjusted model, we found that higher expectation scores were associated with lower satisfaction levels. Our curve-fitting analysis revealed that the risk of decreased patient satisfaction increased notably when the expectation score exceeded 53 points. Two-piecewise regression confirmed this threshold (OR = 0.29, 95% CI 0.17 ∼ 0.38, P < .001), corroborated by Receiver operating characteristic (ROC) analysis (AUC = 0.808, sensitivity 83.6%, specificity 63.2%).
Conclusion
Our findings identify 53 points as the critical threshold on preoperative expectation scales where satisfaction risk markedly escalates in elderly spinal deformity patients undergoing thoracolumbar fusion. The demonstrated dose-response relationship underscores the clinical importance of preoperative expectation management in this population.
Introduction
Healthcare satisfaction, increasingly recognized as a key quality indicator influencing hospital and physician reimbursement, is becoming a crucial parameter for assessing patients undergoing spine surgery.1,2 Patient satisfaction, defined as the degree to which patients are content with their treatment outcomes, assists surgeons in evaluating the effectiveness of care. 3 Achieving satisfactory outcomes is among the primary goals in spine surgery.
With the rapid development of medical technology, more and more patients have high expectations for major surgeries such as thoracolumbar fusion surgery, especially for elderly patients.4,5 Currently, some studies have shown that preoperative expectations have a significant effect on postoperative adverse outcomes in elderly patients with adult spinal deformity (ASD). Hanci Zhang, MD, et al showed that patients’ preoperative expectations affect patient satisfaction and that high preoperative expectations were associated with lower satisfaction as well as increased length of stay and readmission rates. 5
Several studies have identified associations between preoperative expectations and patient satisfaction, typically employing generalized linear models.6,7 These studies often dichotomized patient expectations into “high” and “low” categories, overlooking continuous variables and potential nonlinear relationships. 8 The limitations inherent in generalized linear models may restrict the detection of curvilinear relationships and dose-response effects, phenomena frequently observed in medical research. Consequently, this study aims to explore the association between preoperative expectations and satisfaction among elderly patients with ASD undergoing thoracolumbar fusion surgery.
Materials and Methods
Study Design
The study received approval from our hospital’s Institutional Review Board (IRB#2024-010-002). We retrospectively collected data on all elderly patients (aged ≥65 years) with ASD who underwent thoracolumbar fusion at our institution between September 2019 and September 2022. Postoperative patient-reported outcomes were assessed using the North American Spine Society (NASS) questionnaire at the routine 2-year follow-up. Questionnaires were completed either during scheduled outpatient clinic visits or via standardized remote follow-up methods (eg, telephone). Based on the satisfaction outcomes, patients were categorized into two groups: the dissatisfied group (case group) and the satisfied group (control group). Propensity score matching using the nearest-neighbor method was applied to both groups of patients. We investigated the correlation between preoperative expectations and postoperative satisfaction in these patients. The study cohort was established according to the following inclusion principles: (1) Participants meeting diagnostic criteria for ASD necessitating surgical treatment were required to demonstrate at least one radiographic parameter from: (1) Pelvic incidence-lumbar lordosis (PI-LL) ≥ 10°, (2) Pelvic tilt (PT) ≥ 25°, (3) Sagittal Vertical Axis (SVA) ≥ 5 cm, (4) Thoracic kyphosis (TK) ≥ 60°, and (5) Coronal Cobb angle ≥ 20° 9 ; (2) Individuals aged 65 years or older; (3) Those undergoing posterior thoracolumbar fusion procedures encompassing 5 or more vertebral segments; and (4) Availability of comprehensive postoperative follow-up records spanning a minimum 2-year period. Patients were excluded if they met the following criteria: (1) were younger than 65 years; (2) patients with a history of prior spinal surgery for tumors, trauma, or infection were excluded; (3) had concurrent cervical or coccygeal spinal interventions; or (4) patient with the percentage of missing data that exceeds 10%.
Measurement of Expectations and Satisfaction of With Spine Surgery
The comprehensive 20-item Hospital for Special Surgery Lumbar Spine Surgery Expectations Survey was administered to all patients to assess their preoperative expectations.10–12 These well-established surveys assess patients’ expected improvements in symptom relief, physical function, and psychological well-being.13,14 The questionnaire was administered only after obtaining the patient’s informed consent and was completed before surgery. Patients were instructed to respond to each item by indicating their expected level of improvement using a scoring system ranging from “back to normal or completely improved” (4 points) to “I do not have this expectation or this expectation does not apply to me” (0 points). The total score, obtained by summing the scores for all items, ranged from 0 to 80, with higher scores reflecting more positive and higher expectations. 10 Patient satisfaction was assessed in the 2-year follow-up through the NASS. 15 NASS consists of the following items: The treatment met my expectations (a score of 1); I did not improve as much as I had hoped, but I would undergo the same treatment for the same outcome (a score of 2); I did not improve as much as I had hoped, and I would not undergo the same treatment for the same outcome (a score of 3); I am the same or worse than before treatment (a score of 4). The “satisfied patients” were defined as a score of 1 or 2. 16
Data Collection
We evaluated a variety of demographics, radiological parameters, surgical factors, and perioperative outcomes using the patients’ electronic medical records. Demo graphic variables encompassed age, sex, body mass index (BMI), smoking status, drinking, Age-Adjusted Charlson Comorbidity Index (ACCI), American Society of Anesthesiologists (ASA) classification, Marital status, symptom duration, and predominant pain symptom. Patients also completed several patient-reported outcome measures, including the Oswestry Disability Index (ODI version 2.0, scored 0-100 with higher scores indicating greater disability) to assess baseline functional status, the Geriatric Depression Scale (possible score of 0-30, ≥11 is a positive screen for depression) and the Spielberg State Anxiety Inventory (possible score of 20-80, population norms are available for comparison). Preoperative radiological parameters such as TK, LL, PT, PI, T1 pelvic angle (TPA), SVA were assessed using standard standing lateral whole-spine radiographs from all eligible patients. All radiographic measurements were independently performed by 2 fellowship-trained spine surgeons who were blinded to clinical data and postoperative satisfaction outcomes. Interobserver reliability was evaluated using the intraclass correlation coefficient (ICC) and an ICC of ≥ 0.75 was considered indicative of high reliability, 17 based on repeated measurements in a randomly selected subset, with all parameters demonstrating excellent agreement. Discrepancies were resolved by consensus. Surgical factors included the number of fused levels, Schwab grade, and estimated blood loss (EBL). Postoperative complications were quantified using the Comprehensive Complication Index (CCI), the CCI quantifies the cumulative burden of postoperative complications by weighting and summing all complications experienced by a patient. Scores range from 0 (no complications) to 100 (death) and categorized into 3 severity levels: mild complications (CCI 0-20), and severe complications (CCI >20). 18 Most importantly, we used the 20-item Hospital for Special Surgery Lumbar Spine Surgery Expectations Survey to assess patients’ preoperative expectations and NASS to assess patient satisfaction. The Expectations Survey was administered preoperatively as part of the standard pre-surgical assessment, after completion of surgical decision-making and patient counseling, and prior to the index operation. The Expectations Survey was administered preoperatively as part of the standard pre-surgical assessment, after completion of surgical decision-making and patient counseling, and prior to the index operation. We also correlated patient satisfaction with estimated blood loss, postoperative drain retention, and length of stay (LOS). Predominant pain symptoms, specifying that this term refers to the primary pain characteristics (eg, location, intensity, frequency) reported by participants as most bothersome or frequent during the study period.
Statistical Analysis
Histograms and the Shapiro-Wilk test were used to assess the distribution of numerical variables. The mean and standard deviation of continuous variables were used to describe demographic, clinical, and surgical characteristics, and Student’s t-test or Mann-Whitney U test was used to compare differences between groups. Propensity score matching was performed using age, sex, body mass index (BMI), and preoperative psychological factors (anxiety and depression). Nearest-neighbor matching without replacement was applied in a 1:1 ratio to improve intergroup comparability. To exclude the influence of preoperative functional status on patient satisfaction, we included the preoperative Oswestry Disability Index (ODI) score and expectation level as covariates in the multivariate regression model. The model was adjusted for baseline differences to assess the independent effect of expectation on patient satisfaction. Adhering to the guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, we presented the outcomes from 3 models: the crude model, a minimally adjusted model, and a fully adjusted model. We examine the nonlinear relationship by smoothing the curves. If a nonlinear relationship is observed, a two-segment regression model is applied to calculate the threshold effect based on the smoothed curve. Receiver operating characteristic (ROC) curve analyses were performed to determine the optimal expectation cutoff value based on the Youden index.
A two-tailed P < .05 was considered statistically significant. All analyses were performed with the Statistical Package for Social Sciences version 26 (SPSS, version 22.0, Inc., Chicago, IL, USA) and R version 4.3.1 for Windows (R Foundation for Statistical Computing, Vienna, Austria).
Results
In the initial cohort, 234 patients were available for analysis (Figure 1). 89 patients in the case group and 145 in the control group. The two groups of similar patients were matched by the nearest neighbor method. Nearest-neighbor matching paired 82 patients who were satisfied with 82 similar patients who were dissatisfied. Flowchart for patient inclusion and screening
Subject Characteristics for Cases and Matched Controls
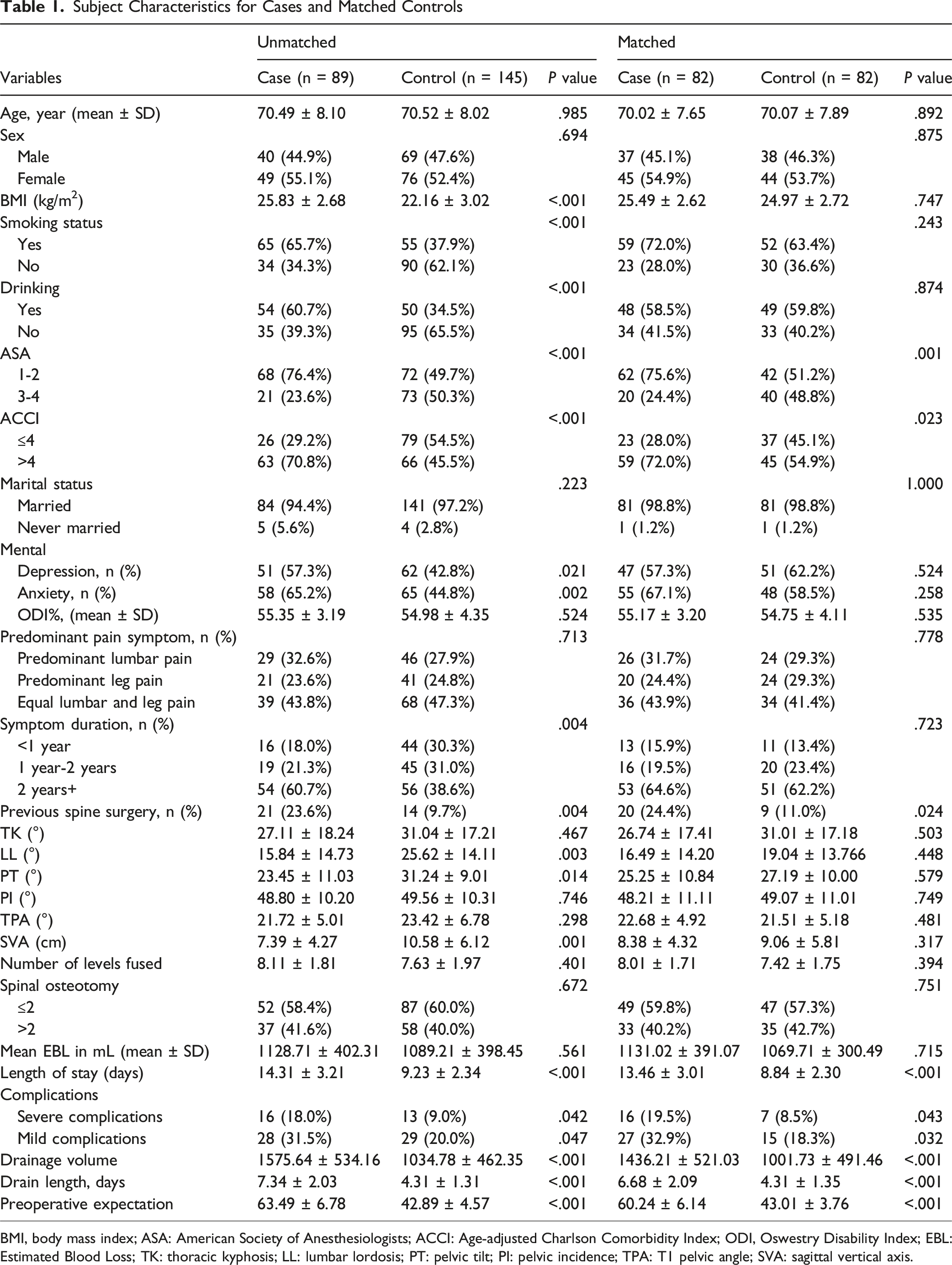
BMI, body mass index; ASA: American Society of Anesthesiologists; ACCI: Age-adjusted Charlson Comorbidity Index; ODI, Oswestry Disability Index; EBL: Estimated Blood Loss; TK: thoracic kyphosis; LL: lumbar lordosis; PT: pelvic tilt; PI: pelvic incidence; TPA: T1 pelvic angle; SVA: sagittal vertical axis.
Univariate Conditional Logistic Regression Analysis of Variables Associated With Satisfaction
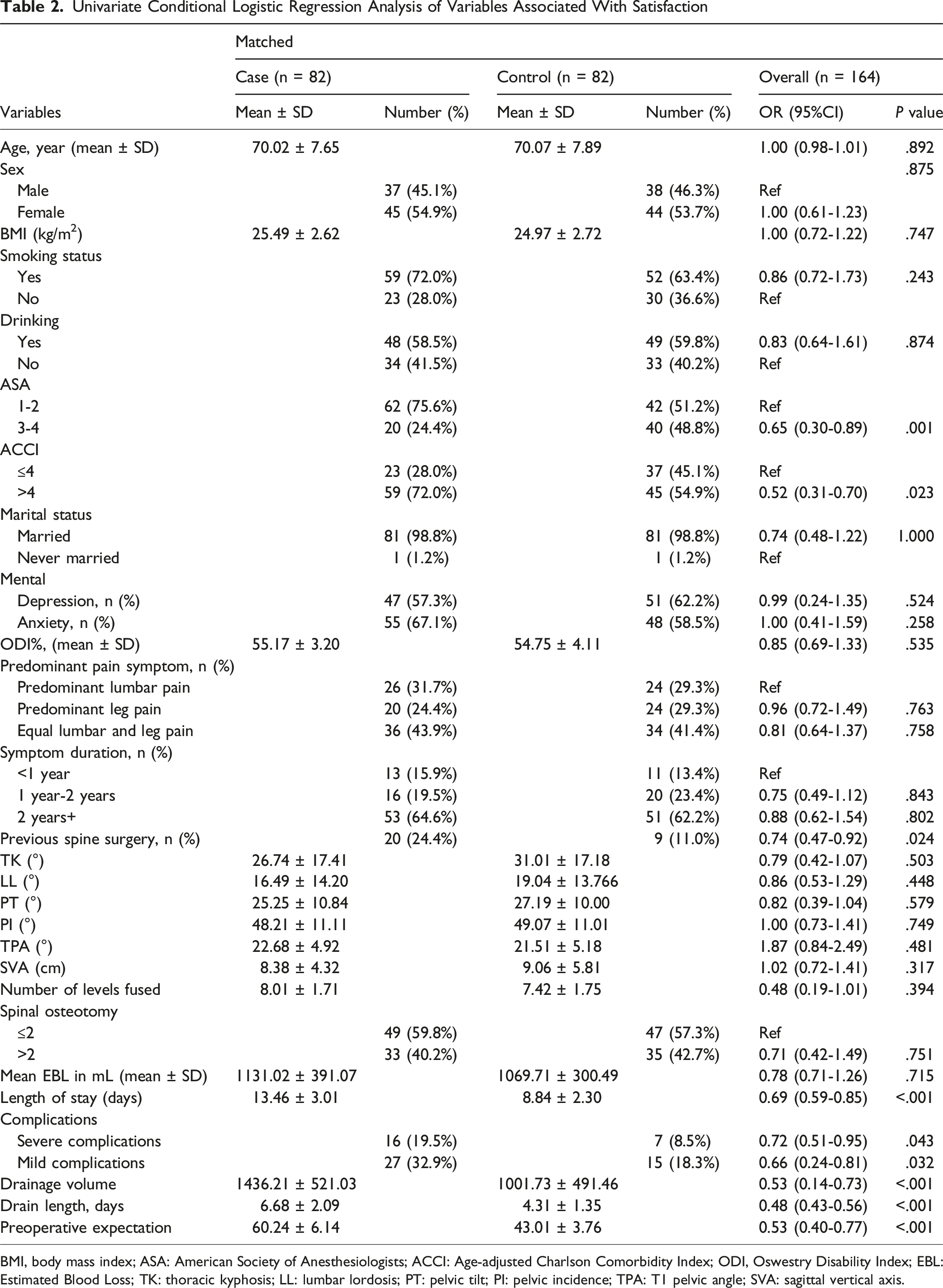
BMI, body mass index; ASA: American Society of Anesthesiologists; ACCI: Age-adjusted Charlson Comorbidity Index; ODI, Oswestry Disability Index; EBL: Estimated Blood Loss; TK: thoracic kyphosis; LL: lumbar lordosis; PT: pelvic tilt; PI: pelvic incidence; TPA: T1 pelvic angle; SVA: sagittal vertical axis.
Relationship Between Preoperative Expectation and Satisfaction. Values are Odds Ratio (OR) (95% CI)
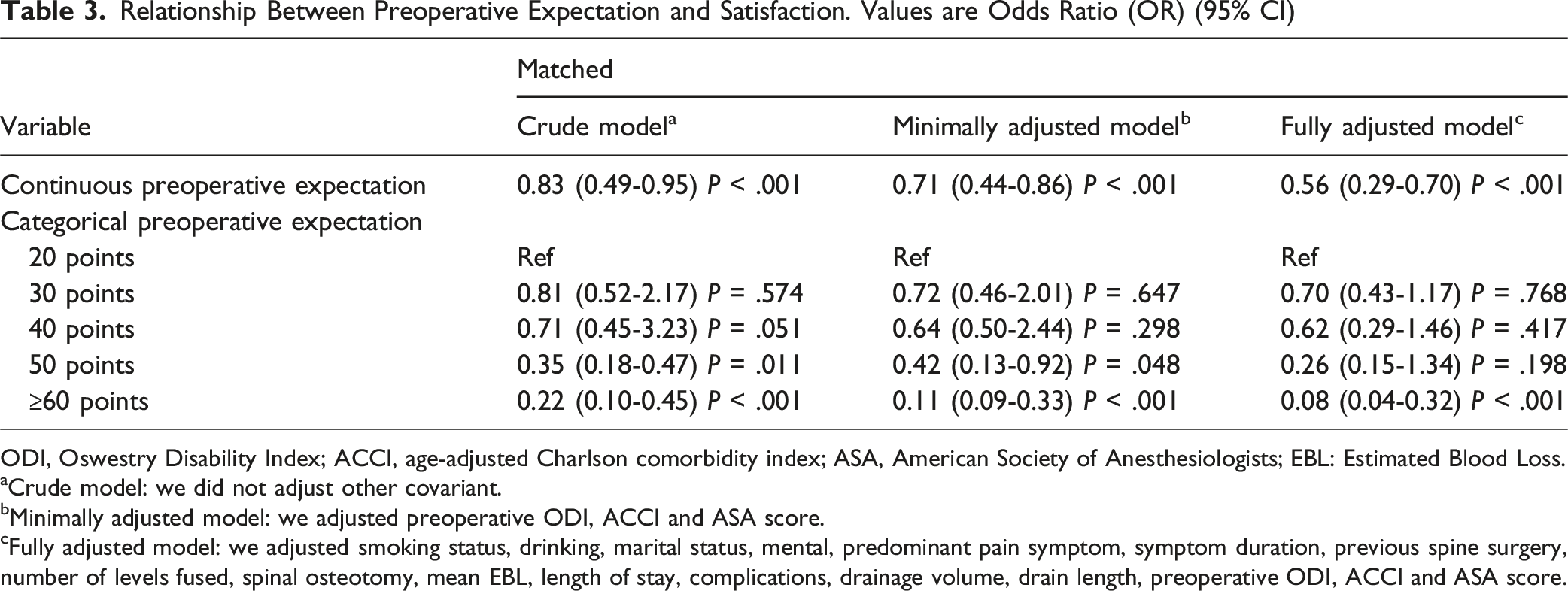
ODI, Oswestry Disability Index; ACCI, age-adjusted Charlson comorbidity index; ASA, American Society of Anesthesiologists; EBL: Estimated Blood Loss.
aCrude model: we did not adjust other covariant.
bMinimally adjusted model: we adjusted preoperative ODI, ACCI and ASA score.
cFully adjusted model: we adjusted smoking status, drinking, marital status, mental, predominant pain symptom, symptom duration, previous spine surgery, number of levels fused, spinal osteotomy, mean EBL, length of stay, complications, drainage volume, drain length, preoperative ODI, ACCI and ASA score.
Two-Piecewise Regression Model
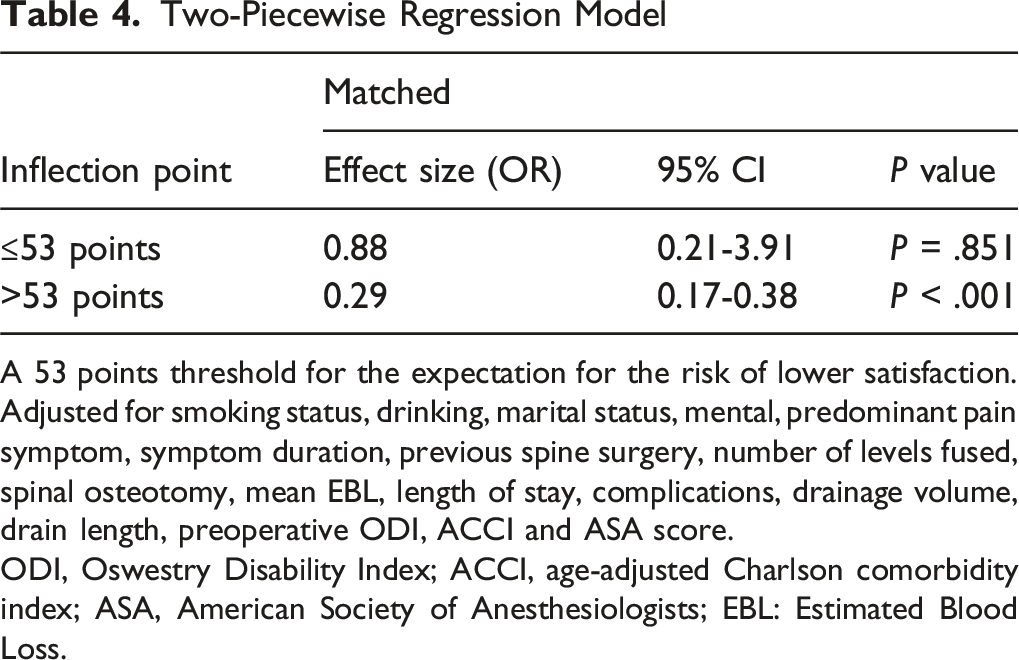
A 53 points threshold for the expectation for the risk of lower satisfaction.
Adjusted for smoking status, drinking, marital status, mental, predominant pain symptom, symptom duration, previous spine surgery, number of levels fused, spinal osteotomy, mean EBL, length of stay, complications, drainage volume, drain length, preoperative ODI, ACCI and ASA score.
ODI, Oswestry Disability Index; ACCI, age-adjusted Charlson comorbidity index; ASA, American Society of Anesthesiologists; EBL: Estimated Blood Loss.
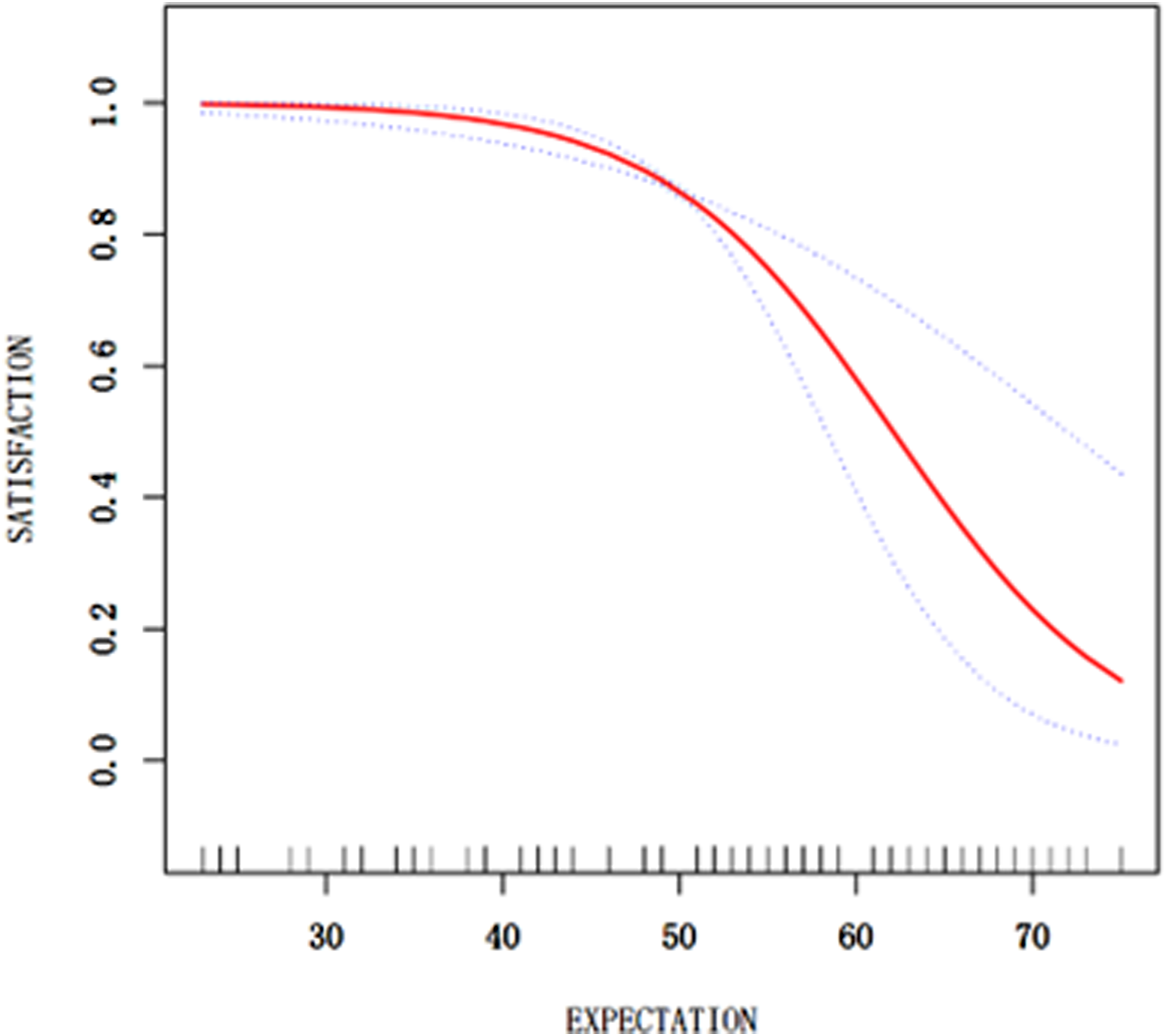
Curve fitting plot of the preoperative patient expectations and the risk of satisfaction. A non-linear relationship between preoperative patient expectations and the risk of satisfaction was observed after confounding variables fully adjusted
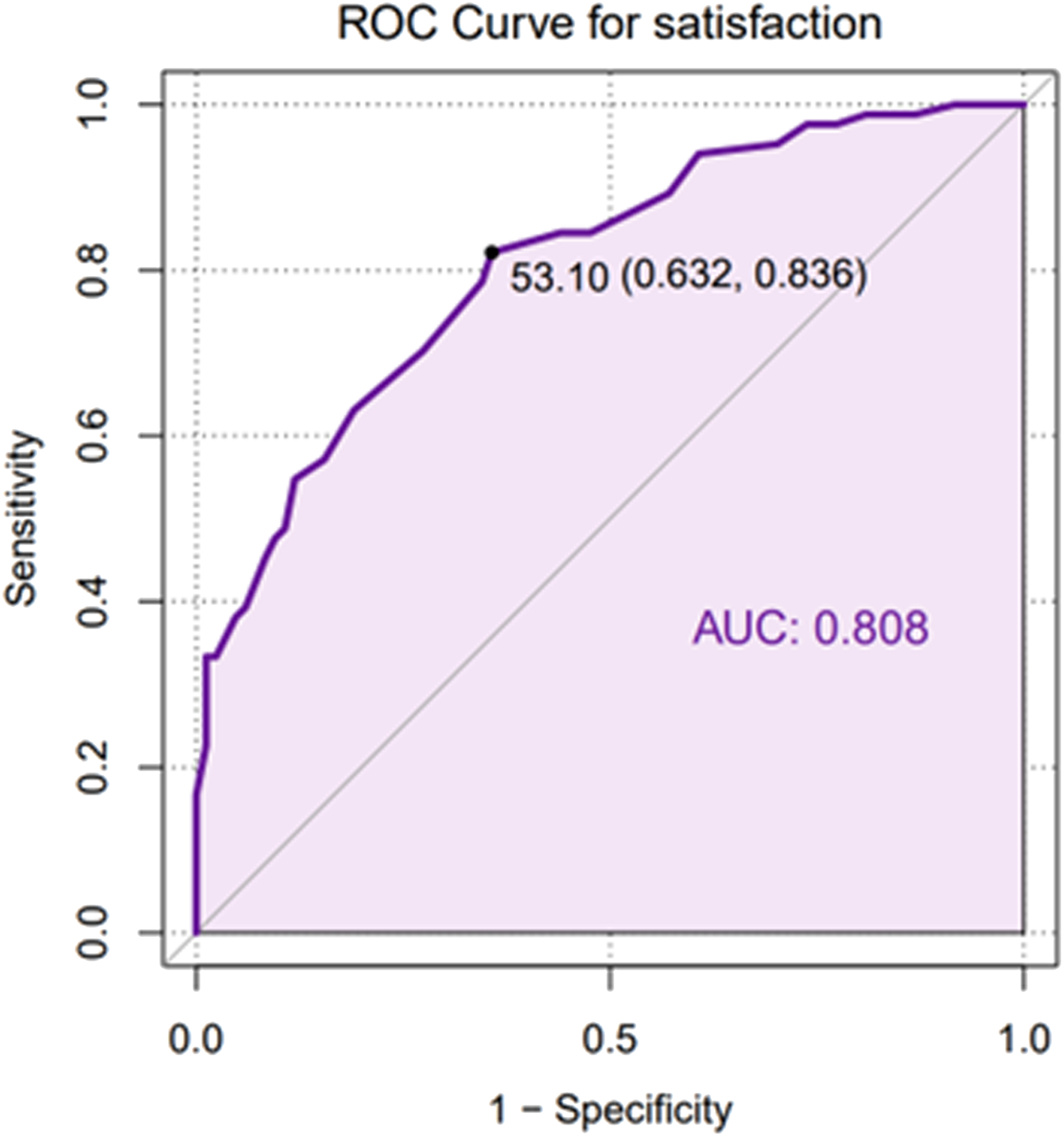
Determination of preoperative patient expectations thresholds based on ROC (receiver operating characteristic) curve analyses. The optimal cutoff value for the preoperative patient expectations score is presented as the threshold with the specificity and sensitivity in parentheses. AUC = area under the ROC curve
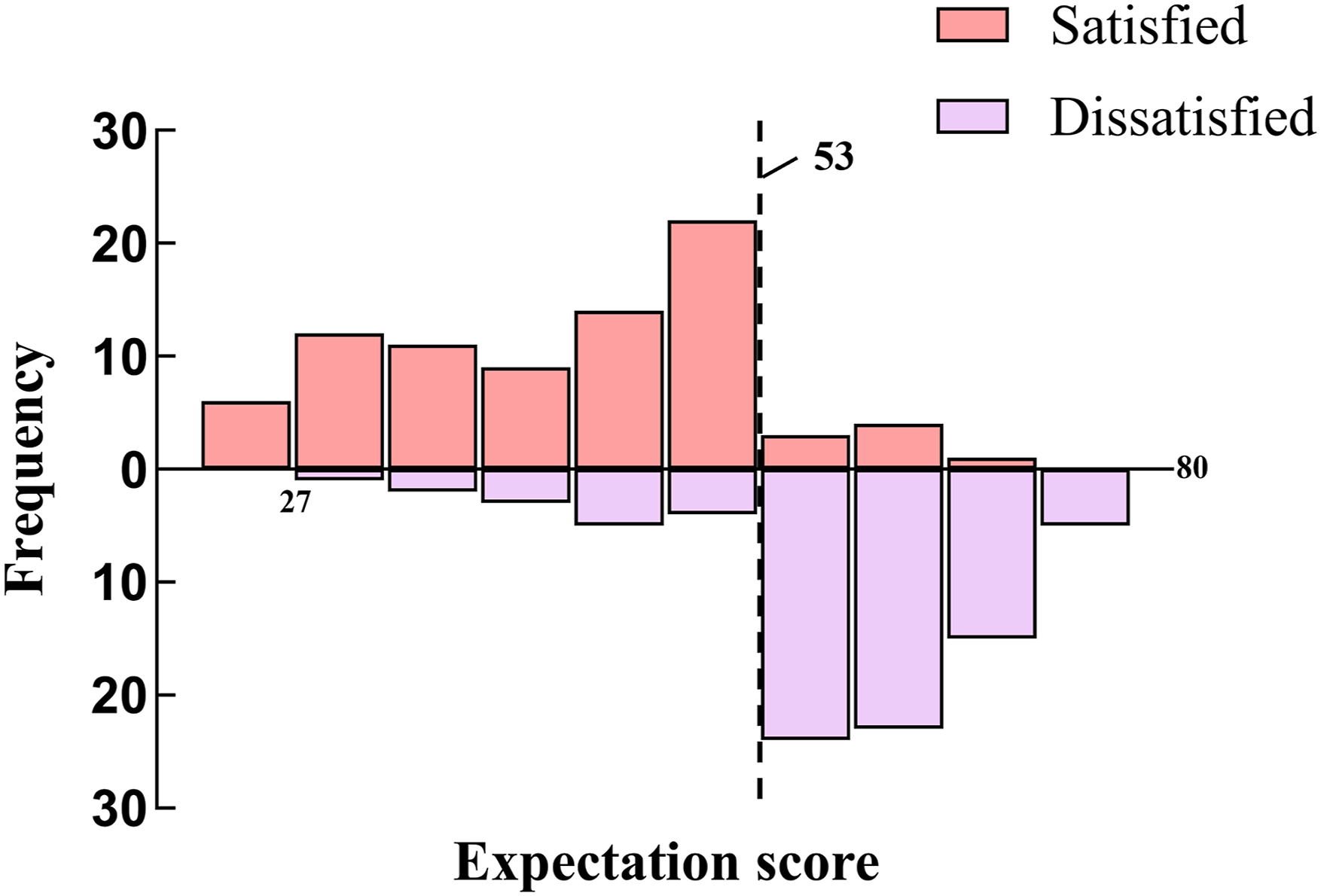
Distribution of satisfaction for the critical threshold on preoperative patient expectations. The dashed vertical lines represent the thresholds of expectations. Each rectangle in the histogram represents a 10% interval of the preoperative patient expectations
Discussion
Elevated preoperative expectations may negatively influence patient satisfaction among elderly individuals with ASD.19,20 Although prior studies have generally suggested a negative association between higher preoperative expectations and postoperative satisfaction, the precise structure of this relationship has remained insufficiently characterized. This uncertainty provided the primary rationale for the present study, which aimed to explore whether the association between expectations and satisfaction follows a uniform linear pattern or varies across different levels of preoperative expectations. Our study found that patients with high preoperative expectations experienced significantly lower satisfaction levels postoperatively. This outcome aligns with existing research, such as the study by Jordan et al, which demonstrated that higher preoperative expectations were linked to length of stay and lower satisfaction following lumbar fusion surgery. 21 Simultaneously, by modeling preoperative expectations as a continuous variable and applying nonlinear analysis methods, we found that this relationship is threshold-dependent, rather than purely negatively correlated.
We conducted a single-center retrospective cohort analysis involving 234 elderly patients who underwent long-segment thoracolumbar fusion. Our study aimed to augment existing descriptive statistics and explore potential associations between preoperative expectations and patient satisfaction. We found that elevated preoperative expectations were significantly associated with decreased patient satisfaction and extended hospital stays. Notably, even after adjusting for various intraoperative variables through univariate and multivariate analyses, high preoperative expectations remained a significant risk factor for reduced satisfaction. Furthermore, our fitted curve analysis indicated that patient satisfaction notably declined when preoperative expectations exceeded 53 points. At the moment, the ROC analysis demonstrated good discriminative performance of the expectation score (AUC = 0.808). The identified 53-point cutoff should not be interpreted as a definitive clinical decision threshold, but rather as a pragmatic, cohort-specific reference that may facilitate preoperative risk stratification and guide targeted expectation management. Importantly, the generalizability of this cutoff requires confirmation through larger, prospective, multicenter studies involving diverse patient populations before it can be routinely applied in clinical practice. These findings underscore the importance of managing patient expectations to enhance satisfaction and optimize postoperative outcomes.
Patient expectations are a crucial aspect of shared decision-making, particularly for individuals undergoing complex surgeries.22,23 While these expectations are believed to influence clinical outcomes, existing research presents mixed findings regarding their correlation with actual results. For instance, a systematic review highlighted that positive expectations were associated with improved patient-reported outcomes in 47% of the studies, whereas 15% reported poorer outcomes. 24 Additionally, a study focusing on spinal surgery patients found that preoperative expectations often exceeded long-term achievements, yet satisfaction levels remained high despite unmet expectations. 25 In contrast, our study demonstrates a dose-response relationship between preoperative expectations and patient satisfaction with surgical outcomes. Specifically, we observed that higher preoperative expectations were associated with lower postoperative satisfaction. This finding aligns with the results of Jacob KC et al, who reported that lower preoperative expectations led to a higher rate of fulfilled expectations, thereby increasing patient satisfaction. 26
Patient satisfaction is particularly important in elderly patients with ASD undergoing thoracolumbar fusion.27,28 A study by Canizares et al demonstrated that high preoperative expectations were significantly associated with postoperative adverse events and influenced patient satisfaction. 29 Similarly, our data corroborate these findings. To address this, our institution has implemented a comprehensive perioperative intervention program aimed at aligning preoperative expectations with realistic outcomes to enhance patient satisfaction. We recommend improved preoperative education for elderly spinal deformity patients, particularly those with expectations exceeding 53 points, as our study identified this threshold as critical. Understanding the specifics of high patient expectations and making appropriate adjustments to lower preoperative expectations can improve patient satisfaction. This approach aligns with existing literature emphasizing the importance of managing expectations to achieve better postoperative satisfaction.
Limitations
This study is the first to examine the relationship between preoperative expectations and postoperative satisfaction in ASD patients. It provides strong data to support perioperative interventions for ASD patients. However, the study has limitations: (1) Despite employing PSM, some covariates remained imbalanced between groups. We addressed this through double-adjustment in our regression analyses, but acknowledge that residual confounding may persist. Also, our analyses are limited to observed variables. Unmeasured factors, such as patient motivation or social support, could influence satisfaction outcomes and were not accounted for in our models. (2) Despite refinement of the propensity score matching strategy, a residual imbalance remained in the proportion of patients with a history of previous spine surgery between groups. Prior operative experience may influence patient expectations and perceptions of surgical outcomes, potentially predisposing these patients to postoperative dissatisfaction. Although this variable was included in the fully adjusted multivariable regression model, this imbalance represents an inherent limitation of observational matching and should be considered when interpreting the results. (3) This study was a single-center, retrospective cohort analysis, which limits the generalizability of the suggested results. The retrospective nature of this study also limits this study because the described benchmarks were unable to assess efficacy. Therefore, further studies are needed to develop and disseminate protocols that use the benchmarks described above to determine their efficacy. (4) Propensity score matching limited the number of patients in each group to 82, which reduces the statistical power of the suggested results. Therefore, in future studies, we will aim to expand the sample size to conduct a prospective study with a large sample size for further research. (5) The present study focused on elderly patients undergoing extensive thoracolumbar surgery for ASD, a population characterized by high surgical complexity and heterogeneity. Direct comparison with studies involving less invasive spinal procedures may be limited. Although a comprehensive set of demographic, clinical, radiographic, and patient-reported variables was analyzed, unmeasured confounders related to surgical complexity, perioperative care, or psychosocial factors may still have influenced postoperative satisfaction. The cutoff value of 53 points for preoperative expectations was identified within this specific cohort and may vary in larger or more homogeneous populations with minimal baseline differences in demographic parameters or PROMs. Therefore, this threshold should be interpreted cautiously and requires validation in broader patient populations.
Conclusion
In this cohort of patients, we successfully correlated preoperative expectations involving 53 points or greater as a significant predictor of reduced postoperative satisfaction in elderly patients with spinal deformity undergoing thoracolumbar fusion surgery. However, this cutoff was derived from a single cohort and should be regarded as exploratory. Further large-scale, prospective studies with external validation are warranted to confirm the generalizability and clinical applicability of this finding.
Footnotes
Acknowledgements
We thank the Department of Orthopedics, Xuanwu Hospital Capital Medical University staff and all the patients who participated in the study.
Ethical Considerations
The study protocol was validated by the institutional review board in Xuanwu Hospital Capital Medical University (2018086). A written informed consent was obtained from all the participants in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Capital’s Funds for Health Improvement and Research (No. 2024-1-2012), the Beijing Hospitals Authority’s Ascent Plan [No. DFL20190802], National Key Research and Development Program of China (No. 2020YFC2004900), and Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support [No. XMLX202116]. The funders played no role in the design of this study, the collection, analysis and interpretation of data or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.