
Abstract
Study Design
Retrospective cohort study.
Objectives
Frailty and nutritional status are predictors of adverse spine surgery outcomes. This study evaluated the predictive utility of a combined Risk Analysis Index (RAI) and Geriatric Nutritional Risk Index (GNRI) model, and introduced a compound score integrating RAI, GNRI, American Society of Anesthesiologists (ASA) classification, and Preoperative Acute Severe Condition (PACS). To develop the CGARP score, we performed multivariable logistic regression with 30-day mortality as the dependent variable and GNRI, RAI, ASA, and PACS as independent variables.
Methods
Using the National Surgical Quality Improvement Program (NSQIP) database (2015-2020), we assessed predictive performance for mortality, morbidity, and length of stay in spine surgery patients. Demographics, comorbidities, and surgical risk factors were analyzed across RAI quartiles. Model performance was measured using area under receiver operating characteristic curve (AUROC).
Results
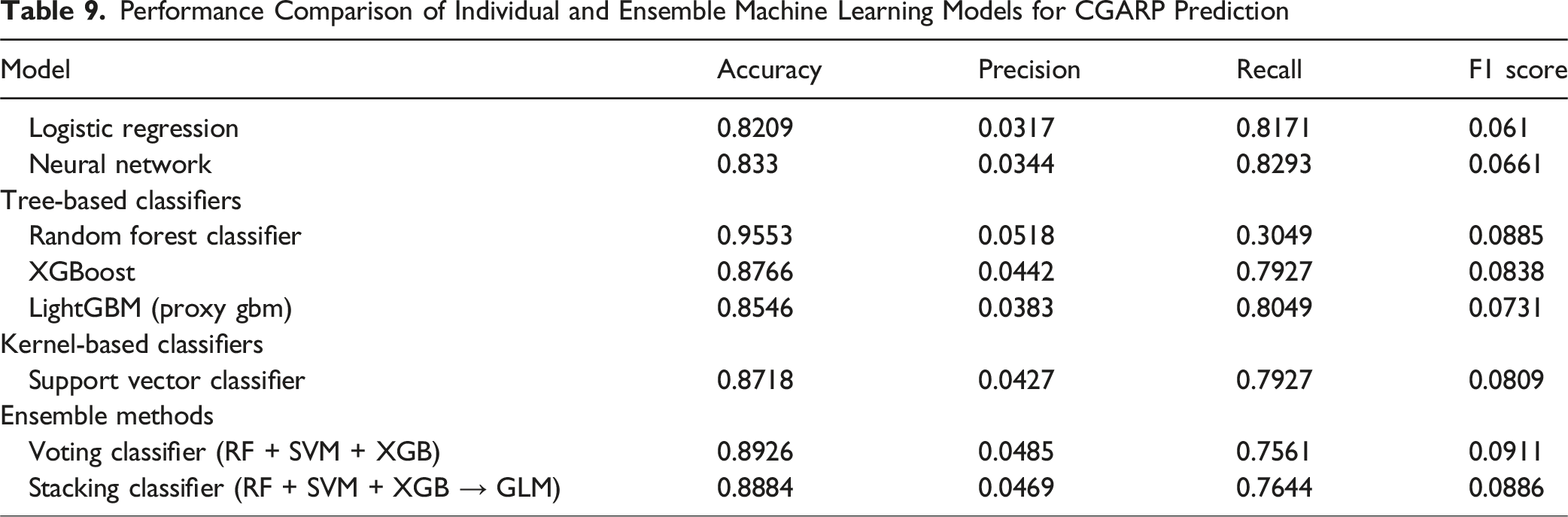
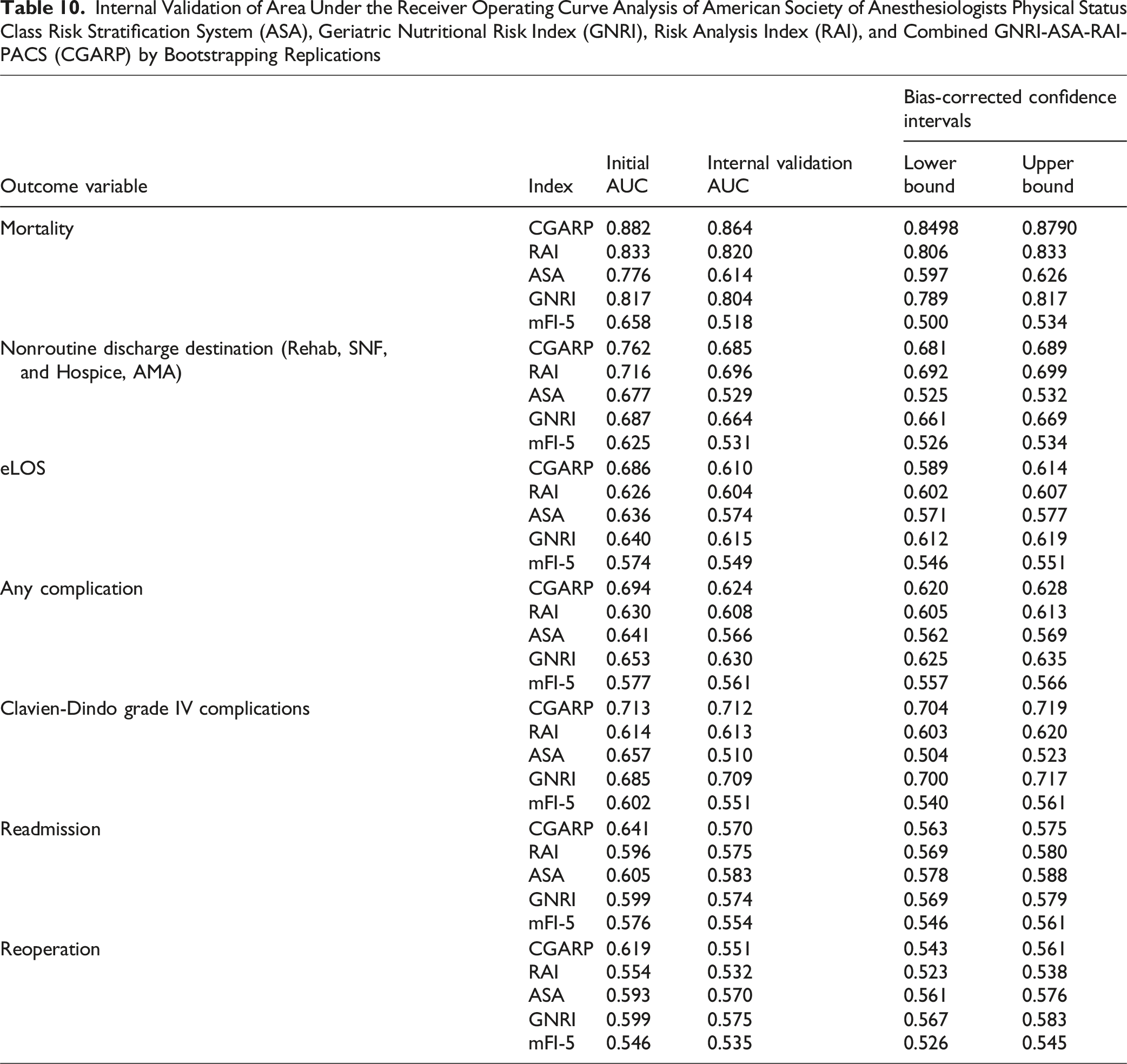
Among 360 133 patients, increasing frailty and malnutrition were independently associated with worse postoperative outcomes. The RAI-GNRI model showed outcome-specific discrimination, C-statistics 0.619 (reoperation) to 0.882 (mortality). The CGARP compound model outperformed individual predictors across all outcomes, with AUROCs of 0.882 (mortality), 0.762 (non-home discharge), 0.686 (extended length of stay), 0.694 (any complication), and 0.641 (readmission). Internal bootstrapping confirmed model stability. Random Forest was the most predictive machine-learning algorithm (AUC = 0.9553). Threshold analysis using Youden’s J statistic identified 4 risk categories, correlating with stepwise increases in mortality, complications, and non-home discharge.
Discussion
Frailty and nutritional risk are independently predictive of adverse spine surgery outcomes. The CGARP model demonstrated superior predictive performance and provides clinically actionable risk stratification.
Introduction
Every year, approximately 900 000 adults in the United States undergo spine surgery for various pathological entities, including infections, neoplasms, deformity, and degeneration, aiming to enhance quality of life.1,2 With an aging population, spine surgeries are increasingly common among patients over 65 years of age. 3 Thus, judicious patient selection in older patients is critical, considering comorbidities, functional and nutritional status, and the growing recognition of frailty.
Frailty, or decreased baseline physiologic reserve, is an independent risk factor for adverse postoperative outcomes following spine surgery.4-6 The Risk Analysis Index (RAI) has emerged as a leading frailty index, demonstrating strong predictive capability for spine surgery outcomes. Similarly, nutritional status has been evaluated using the Geriatric Nutritional Risk Index (GNRI), which correlates serum albumin and body weight.7,8 In recent lumbar spine fusion studies, infection and mortality rates were linked to malnourishment. While both the RAI and GNRI are useful for predicting outcomes, their combined impact on risk stratification remains unexplored.
The present study sought to assess the impact of patient frailty and nutritional status using a combined RAI-GNRI model to improve risk stratification of patients undergoing spine surgery using a national, prospective registry.
Methods
Data Source and Patient Consent to Procedure
Patient data was extracted from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database from 2015 to 2020. This validated database, involving over 700 hospitals, collects more than 200 variables on surgical patients. 9 The study was HIPAA-compliant and exempt from institutional review board approval. Informed consent was waived due to the retrospective design of the study.
Patient Selection
Current Procedural Terminology (CPT) codes were used to identify adult (18 years and older) patients in the ACS NSQIP database who underwent spine surgery between 2015 and 2020. Patients were identified using CPT codes 22 010-22855 and 62 380-63707 for spinal instrumentation and spinal procedures, respectively. Patients 90 years and older, as well as those who had missing outcome data (mortality, unknown discharge destination, etc.), unknown transfer status, and unknown functional status were excluded.10-13
Risk Analysis Index (RAI)
The RAI was developed to optimize preoperative screening based on frailty stratification in patients undergoing elective surgery.
14
The RAI evaluates a diverse set of patient factors and therefore more accurately captures the multidimensionality of frailty. The RAI incorporates variables such as age, sex, renal impairment, dyspnea, cancer status, weight loss, and functional status. Of note, cognitive deterioration, originally coded in the RAI scoring with
American Society of Anesthesiologists (ASA) Physical Status Classification
ASA is a risk assessment tool to preoperatively stratify patients based on overall health status. It contains 5 main categories: ASA I (healthy patient), ASA II (mild systemic disease), ASA III (severe systemic disease), ASA IV (severe systemic disease that is a constant threat to life), and ASA V (moribund patient with a guarded prognosis absent surgery). High ASA grades have been established in the literature as strongly correlating with poor postoperative outcomes across various surgical specialties, including spine surgery. ASA was thus additionally included as a component of the CGARP model.
Geriatric Nutritional Risk Index (GNRI)
The GNRI was originally developed using variables collected by the ACS-NSQIP database, including sex, weight (kg), height (cm), and preoperative albumin level. GNRI is calculated using the formula outlined by Bouillanne et al: GNRI = (1.489 × serum albumin [gram per liter]) + (41.7 × [weight/WLo]). 17 The weight/WLo ratio was capped at 1 for patients with weight exceeding their ideal weight, in order to capture overweight/obese patients who may be malnourished. WLo is the ideal weight, calculated by the Devine formula: men as 50 + (0.91 × [height in centimeters −152.4]) and women as 45.5 + (0.91 × [height in centimeters −152.4]).
GNRI values were stratified into clinically relevant categories: no nutritional risk (GNRI scores >98), low risk (GNRI scores 92-98), moderate risk (GNRI scores 82-91), and major nutritional risk (GNRI scores <82).
Preoperative Acute Severe Condition (PACS)
PACS reflects the cumulative burden of acute preoperative conditions and is calculated by summing binary NSQIP “present at time of surgery” flags for sepsis, SIRS, acute renal failure, ventilator dependence, or pneumonia.
Combined GNRI-ASA-RAI-PACS (CGARP) Score
To develop the CGARP score, we performed multivariable logistic regression with 30-day mortality as the dependent variable and GNRI, RAI, ASA, and PACS as independent variables. The resulting adjusted odds ratios were used to derive weightings proportional to each variable’s relative contribution to risk. These coefficients were normalized and scaled for practical use, yielding the final formula: CGARP = (3 × GNRI group) + (2 × RAI group) + (2 × ASA class) + (1 × PACS). This approach allowed for data-driven, interpretable weighting while preserving clinical relevance.
Population Characteristics and Complications
The baseline study variables included in the present study are age, sex, BMI, hospital length of stay (LOS), and total operation time. Previous medical comorbidities including dyspnea, hypertension functional status, COPD, CHF, smoking status, DM, disseminated cancer, steroid use, weight loss, and bleeding disorders were also included. Preoperative Acute Severe Condition (PACS) was included as an additional risk variable, reflecting the cumulative burden of acute preoperative conditions. PACS is a simple variable that is the sum of all conditions a patient has on surgery, calculated using Present at Time of Surgery variables from the ACS NSQIP database. 18
Outcomes and Complications
Outcomes of interest included 30-day mortality, overall complication rates, Clavien-Dindo grade IV (CDIV) complications, 30-day unplanned readmission, 30-day unplanned reoperation, extended LOS (eLOS), and nonhome discharge destination (NHD). Complications consisted of 1 of the following: prolonged intubation exceeding 48 hours, unplanned reintubation, sepsis, septic shock, pneumonia, deep vein thrombosis/thrombophlebitis, pulmonary embolism, acute cerebrovascular accident or stroke with neurological deficit, acute renal failure, myocardial infarction, cardiac arrest requiring cardiopulmonary resuscitation, superficial surgical site infection (SSI), deep incisional SSI, organ space SSI, wound disruption, intra- or postoperative blood transfusion, renal insufficiency, or urinary tract infection. CDIV complications are defined by the presence of life-threatening complications defined by single or multiple organ dysfunction requiring intensive care unit management. 19 eLOS was defined as > 75th percentile of length of stay of all patients, which was equal to 4 days of stay or longer in our cohort.
Statistical Analysis
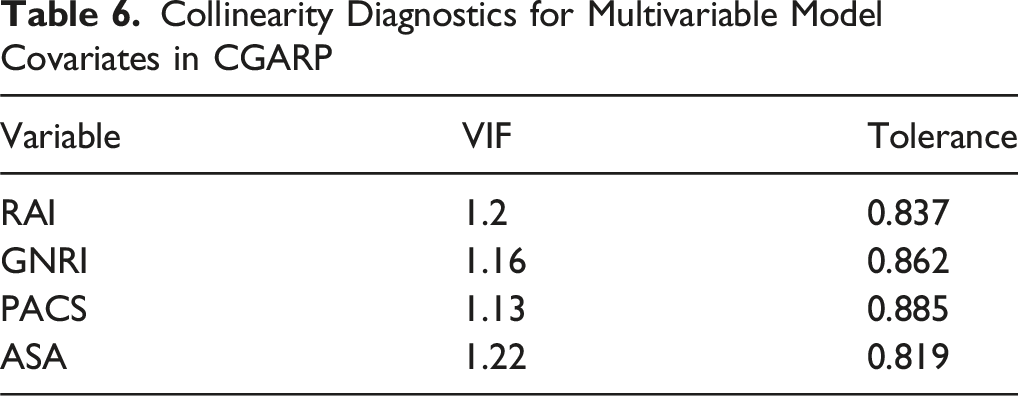
Non-normally distributed interval data were presented as median with Interquartile Range (IQR). The distribution of the data was assessed using the Kolmogorov-Smirnov test. Kruskal-Wallis test was utilized to analyze non-normally distributed continuous variables, while Chi-square was used to analyze categorical variables. Multivariable logistic regression analyses on ASA, GNRI, and RAI and 30-day mortality were carried out to arrive at the coefficients for the development of compound score index. Effect sizes for dichotomous outcomes were expressed as Odds Ratio (OR) with corresponding 95% Confidence Interval (CI). To ensure model stability and eliminate multicollinearity concerns, Variance Inflation Factor (VIF) was calculated for each input variable, with VIF values below commonly accepted thresholds (VIF <3) indicating low collinearity. Receiver Operating Characteristic (ROC) curve analysis was performed, incorporating Area Under the Curve (AUC)/C-statistics calculations to assess the discriminative ability ASA, GNRI, RAI, and the new compound score. The DeLong test was applied to analyze the differences in discrimination performances (C-statistic). Youden’s J statistic was employed to determine optimal thresholds for stratifying the CGARP into 4 distinct categories. Internal validation of the new compound score was carried out using 100 bootstrapping replications with replacement. The 4 CGARP component variables (RAI, GNRI, ASA, and PACS) were used as inputs to train multiple machine learning classifiers to assess their predictive value for 30-day postoperative adverse outcomes. Models included tree-based classifiers (Random Forest, XGBoost, and LightGBM), a kernel-based classifier (Support Vector Classifier), a neural network model, and ensemble methods (voting and stacking classifiers), in addition to a logistic regression model for baseline comparison. Predictive performance was assessed using 5-fold cross-validation and confusion matrix-derived metrics, with accuracy, precision, recall, and F1-score serving as primary evaluation criteria. Feature importance scores were extracted from tree-based models and normalized to enable direct comparison of the relative contribution of each CGARP component to outcome prediction. Statistical analyses were carried out using Excel (Microsoft, Redmond, WA, USA), IBM SPSS Statistics ver. 27.0 (IBM Co, Armonk, NY, USA), and STATA 12.0 (StataCorp, College Station, TX, USA). A P-value <0.05 was considered statistically significant.
Results
Patient Characteristics
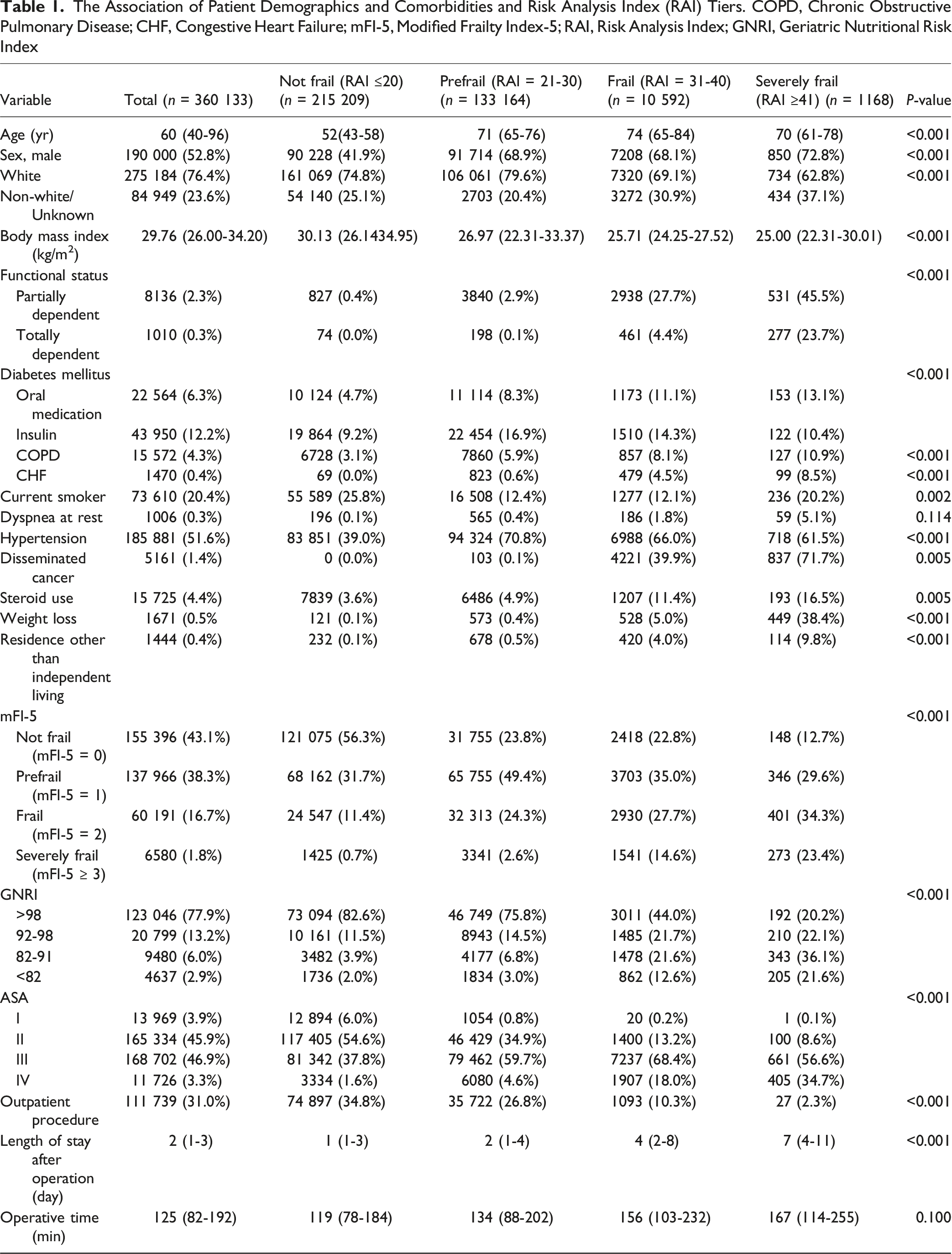
The Association of Patient Demographics and Comorbidities and Risk Analysis Index (RAI) Tiers. COPD, Chronic Obstructive Pulmonary Disease; CHF, Congestive Heart Failure; mFI-5, Modified Frailty Index-5; RAI, Risk Analysis Index; GNRI, Geriatric Nutritional Risk Index
RAI and GNRI 30-Day Outcomes
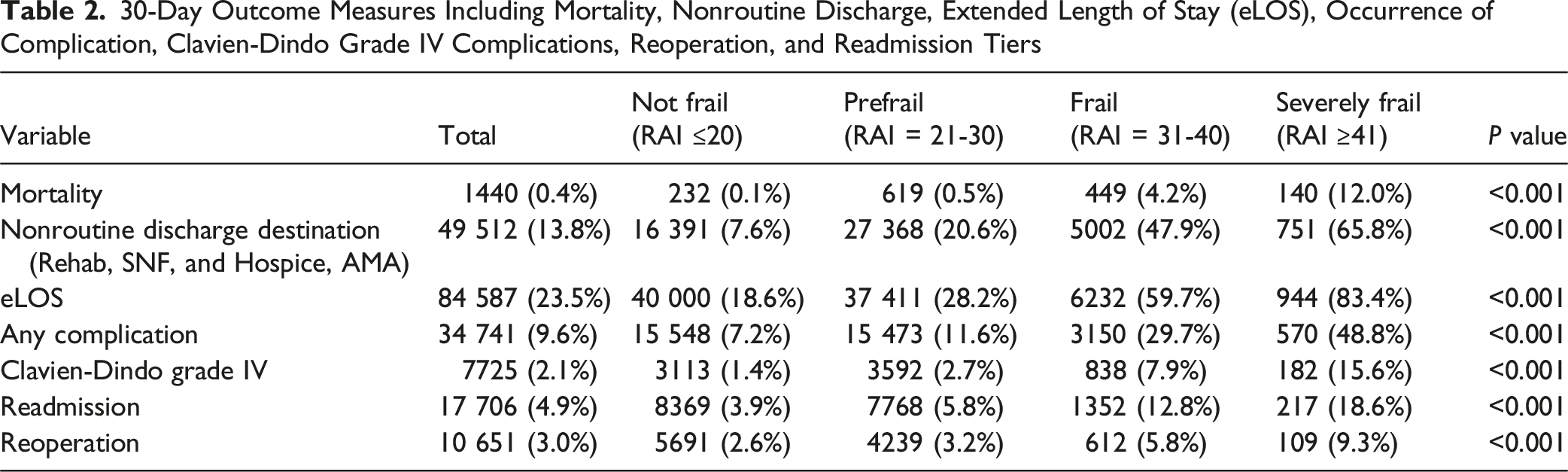
30-Day Outcome Measures Including Mortality, Nonroutine Discharge, Extended Length of Stay (eLOS), Occurrence of Complication, Clavien-Dindo Grade IV Complications, Reoperation, and Readmission Tiers
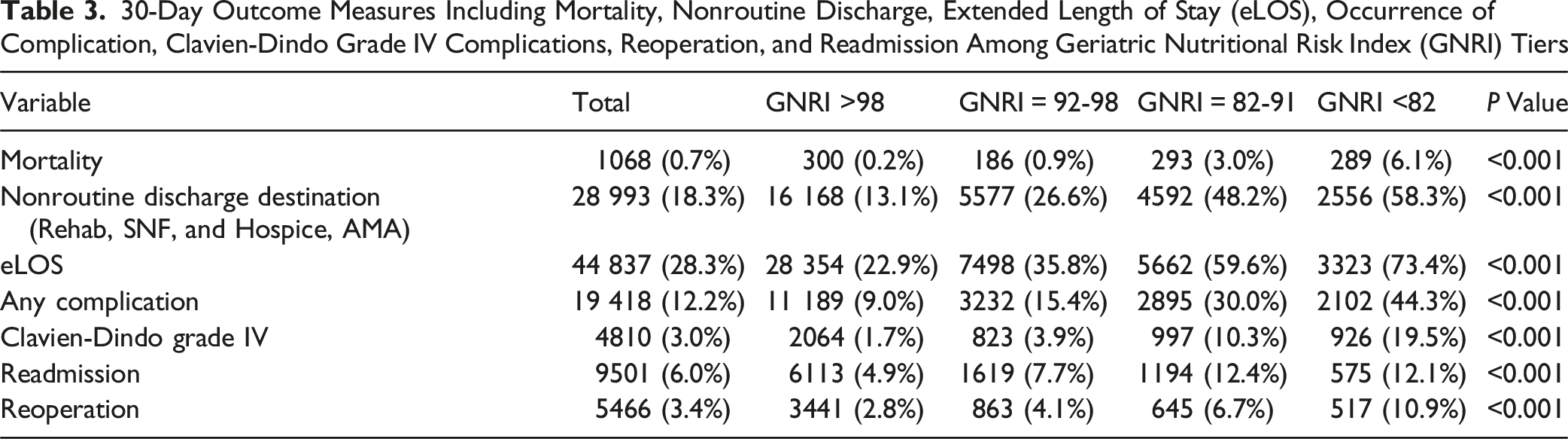
30-Day Outcome Measures Including Mortality, Nonroutine Discharge, Extended Length of Stay (eLOS), Occurrence of Complication, Clavien-Dindo Grade IV Complications, Reoperation, and Readmission Among Geriatric Nutritional Risk Index (GNRI) Tiers
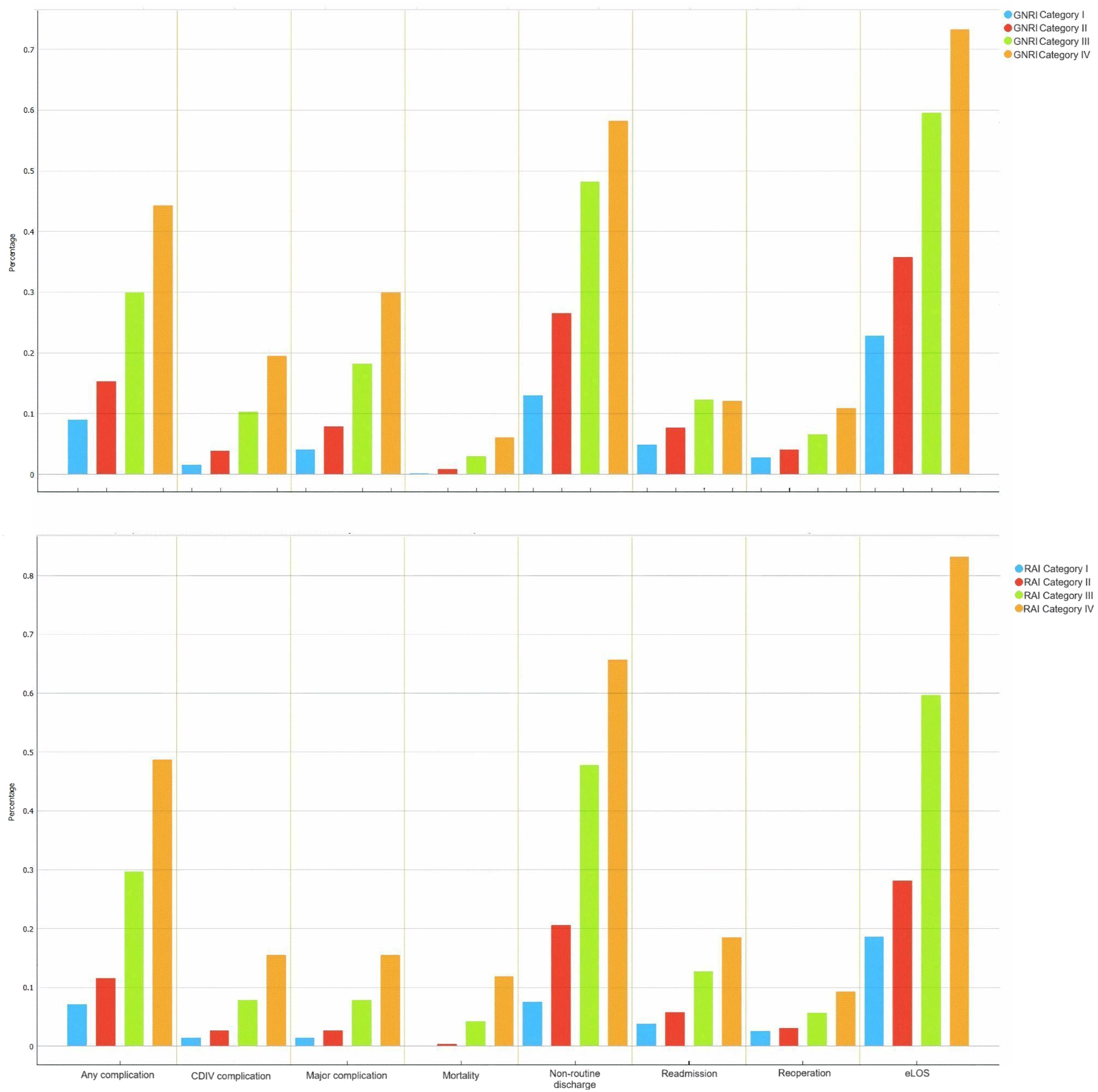
Rates of Adverse Outcomes Stratified by Categories of Geriatric Nutritional Risk Index (GNRI; Top) and Risk Analysis Index (RAI; Bottom). CDVI; Clavien-Dindo Class IV, eLOS; Extended Length of Stay
Major Postoperative Outcomes
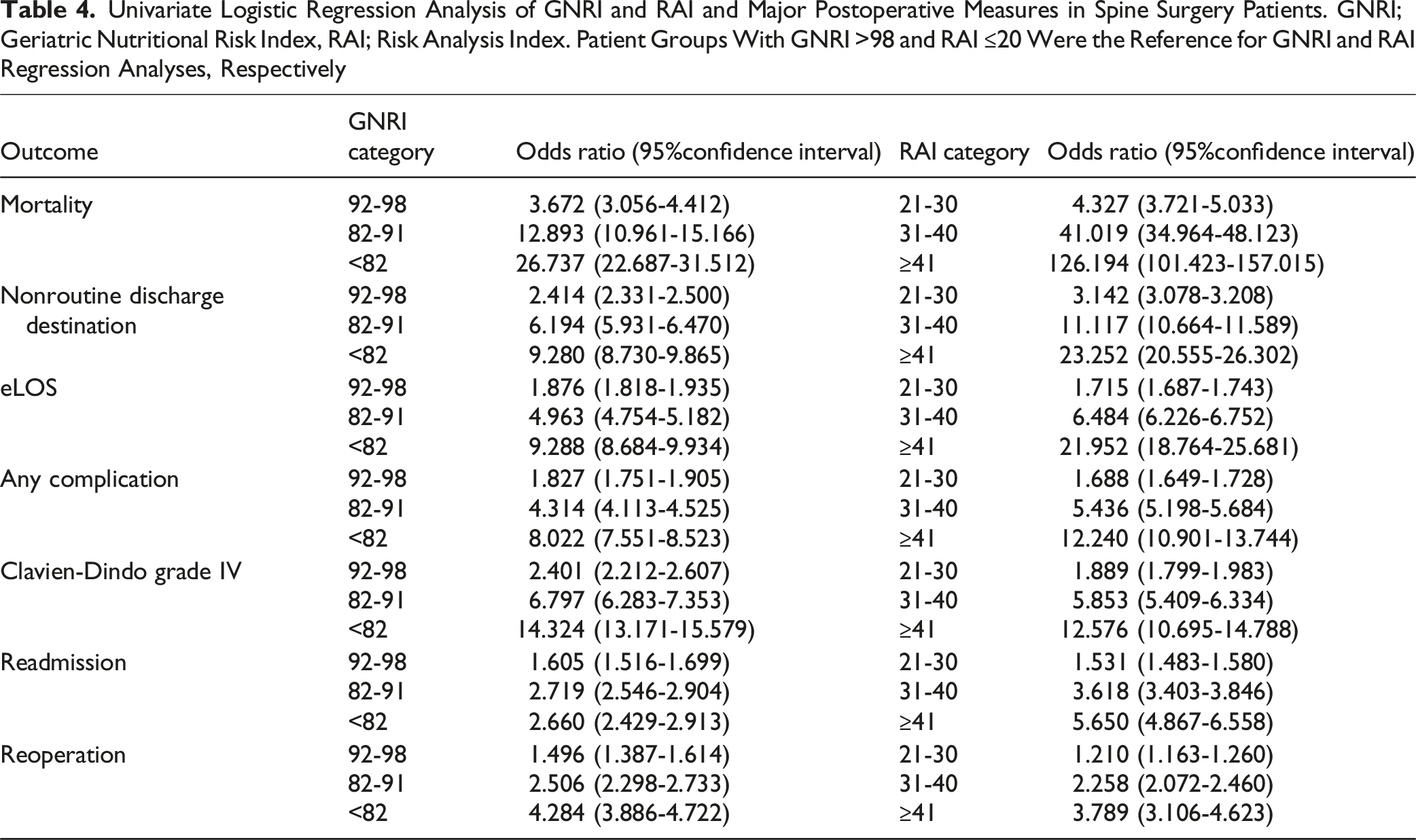
Univariate Logistic Regression Analysis of GNRI and RAI and Major Postoperative Measures in Spine Surgery Patients. GNRI; Geriatric Nutritional Risk Index, RAI; Risk Analysis Index. Patient Groups With GNRI >98 and RAI ≤20 Were the Reference for GNRI and RAI Regression Analyses, Respectively
Novel Score
Multivariable Regression Analysis of Mortality and American Society of Anesthesiologists Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and Preoperative Acute Severe Condition (PACS)

Collinearity Diagnostics for Multivariable Model Covariates in CGARP
Main Results
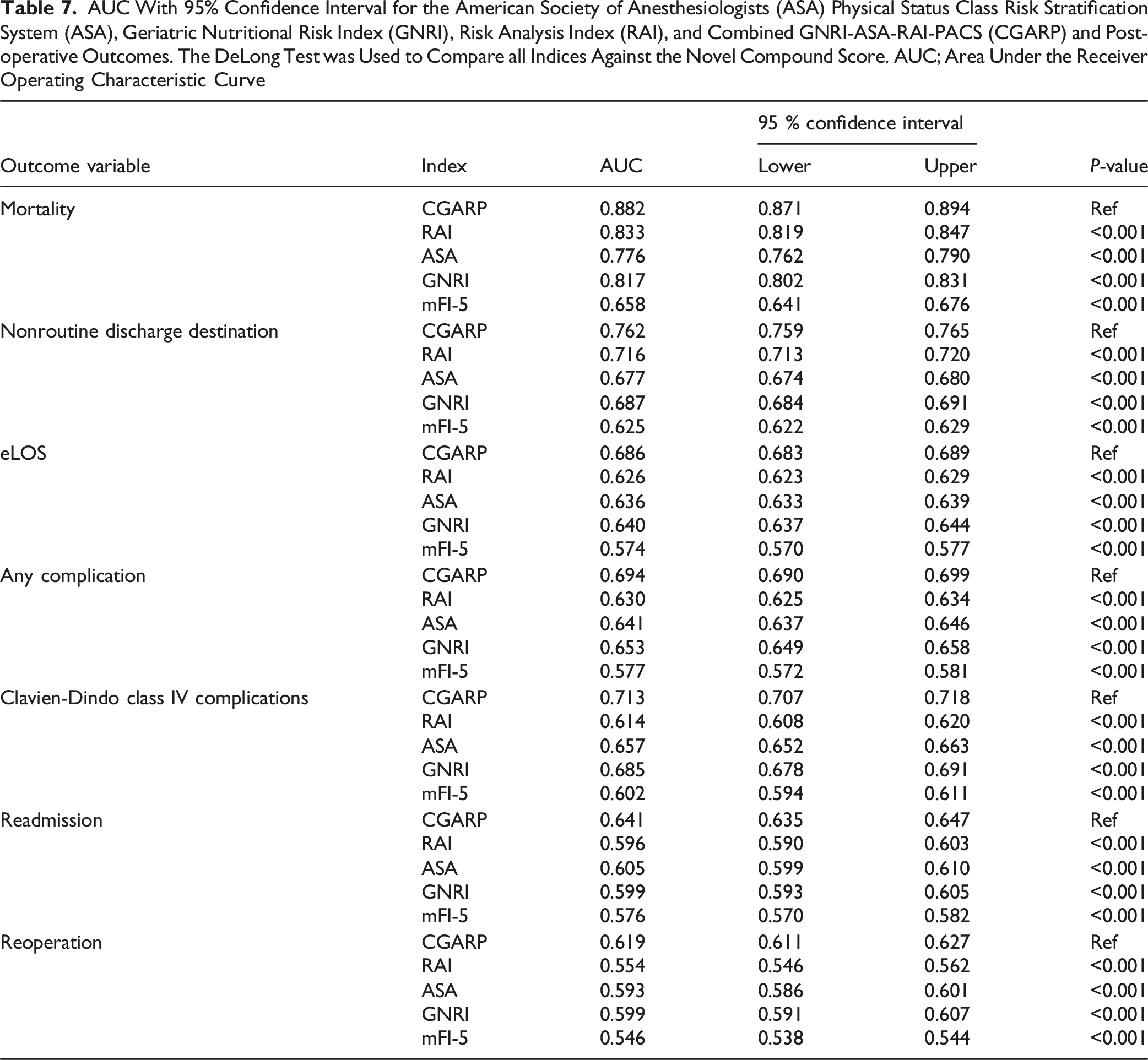
AUC With 95% Confidence Interval for the American Society of Anesthesiologists (ASA) Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and Combined GNRI-ASA-RAI-PACS (CGARP) and Post-operative Outcomes. The DeLong Test was Used to Compare all Indices Against the Novel Compound Score. AUC; Area Under the Receiver Operating Characteristic Curve
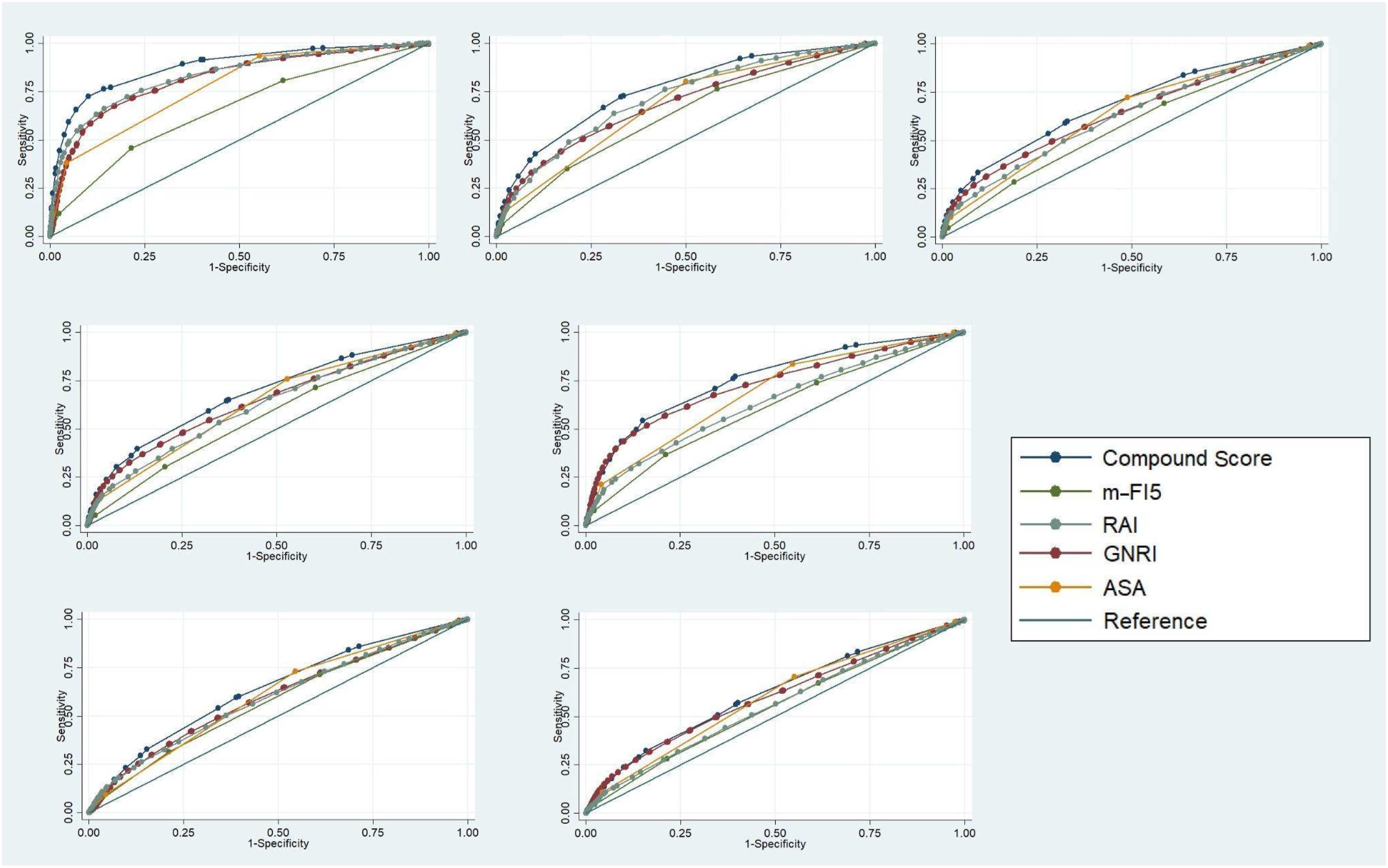
Receiver Operating Characteristic Curve of the American Society of Anesthesiologists Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and the Compound Score for Major Postoperative Outcomes. Mortality (A), Discharge to Non-routine Destination (B), Extended Length of Stay (eLOS) (C), Any Complication (D), Clavien-Dindo Physical Status Classification IV Complication (E), Readmission (F), and Reoperation (G) in Patients Who had Spine Surgery From National Surgical Quality Improvement Program Database 2015-2020
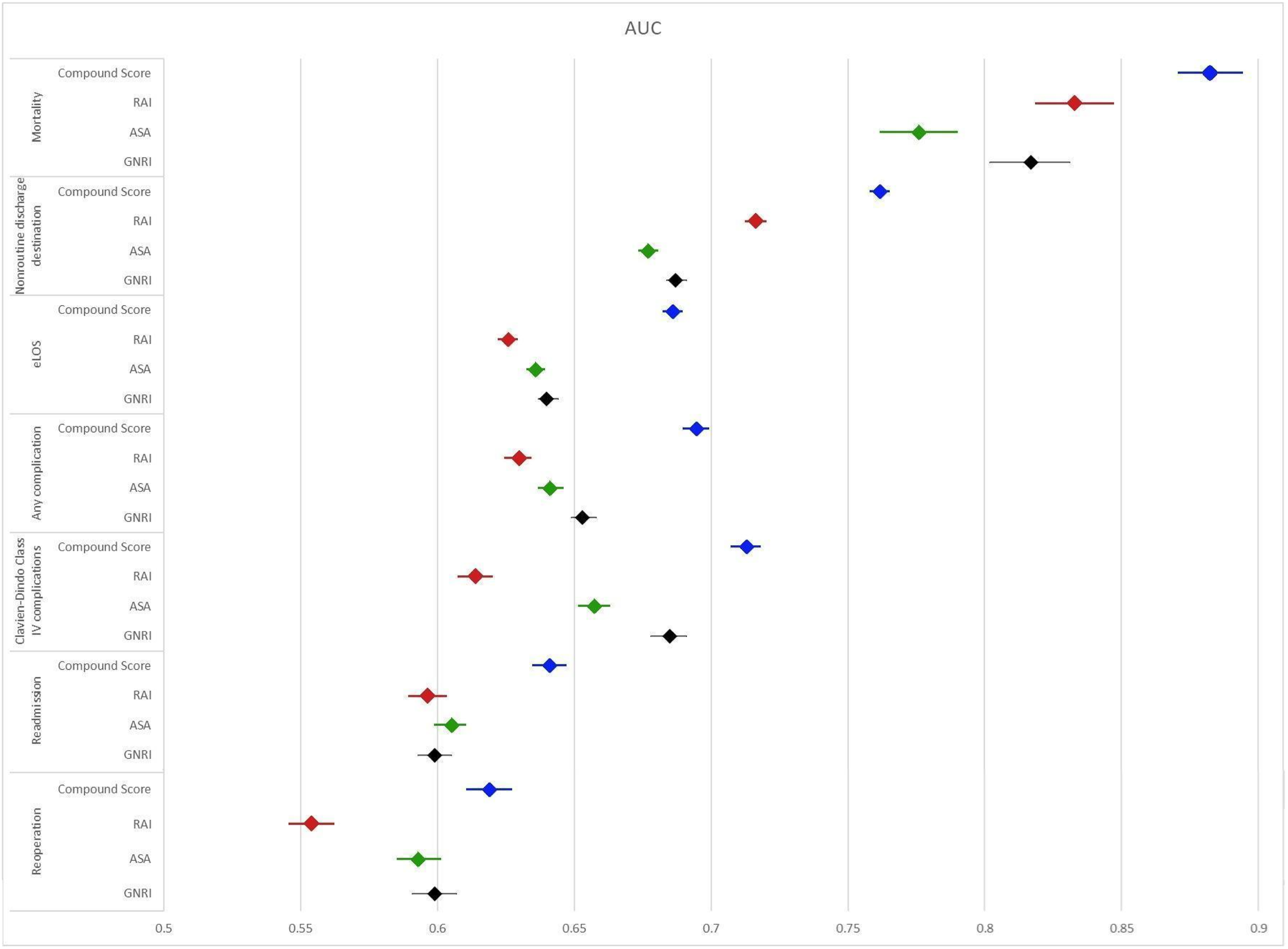
Forrest Plot of Area Under the Receiver Operating Characteristic Curve (AUC) of the American Society of Anesthesiologists Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and Combined GNRI-ASA-RAI-PACS (CGARP) for Major Postoperative Outcomes in Patients Who had Spine Surgery. Extended Length of Stay; eLOS
Postoperative Outcome Rates Stratified by CGARP Risk Category Based on Youden’s J Statistic

Machine Learning Model Performance Comparison
Performance Comparison of Individual and Ensemble Machine Learning Models for CGARP Prediction
Variable Importance Analysis
Feature importance scores were extracted from tree-based classifiers and normalized for direct comparison (Figure 4). The Risk Analysis Index (RAI) demonstrated the highest predictive contribution, followed by GNRI, ASA, and PACS. These results underscore the dominant influence of RAI and GNRI in CGARP-based predictive modeling of postoperative outcomes. Variable Importance Scores for RAI, GNRI, ASA, and PACS in CGARP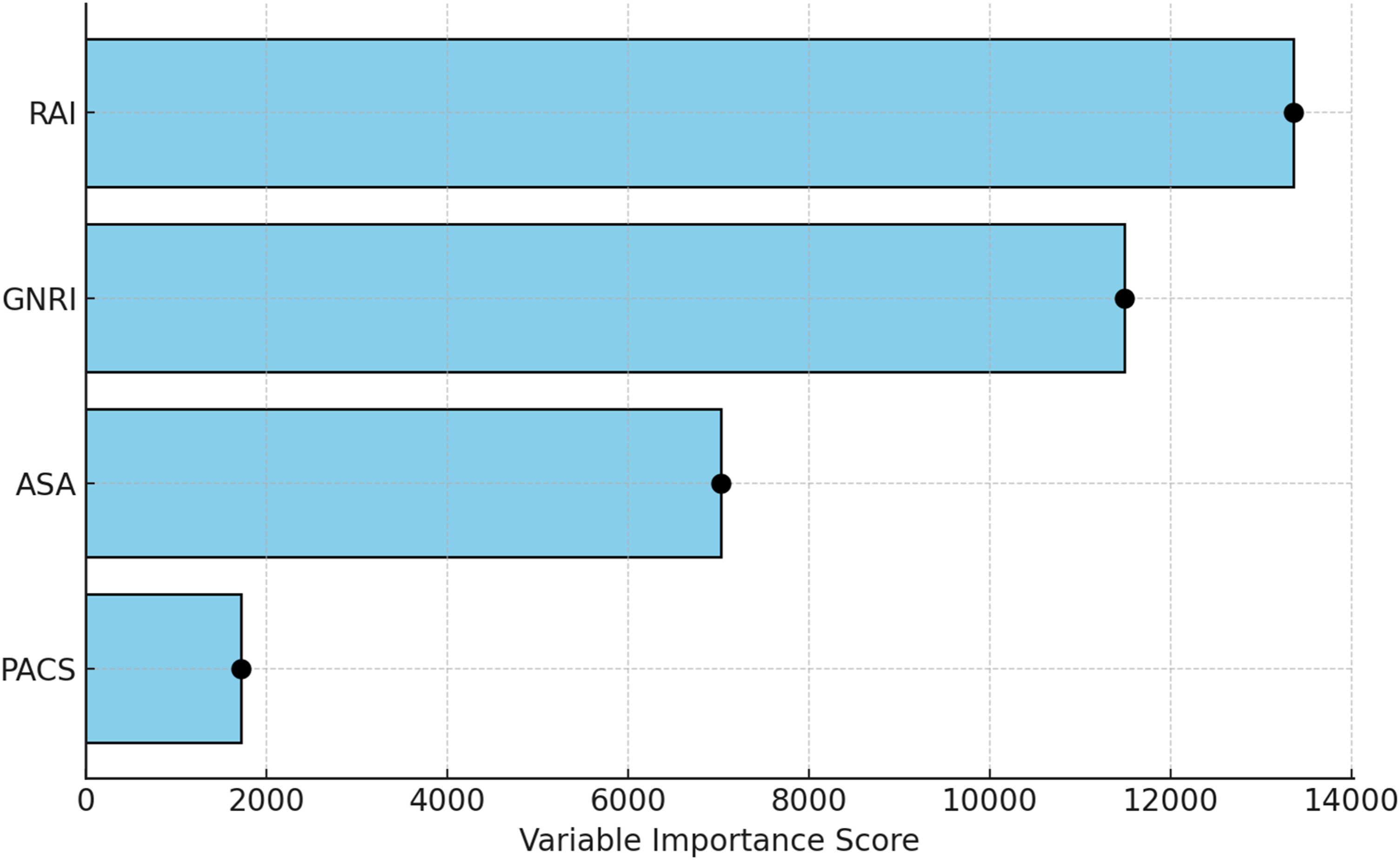
Internal Validation
Internal Validation of Area Under the Receiver Operating Curve Analysis of American Society of Anesthesiologists Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and Combined GNRI-ASA-RAI-PACS (CGARP) by Bootstrapping Replications
Discussion
In this study, the RAI, GNRI, PACS and ASA indices were evaluated for both individual and combined use as a novel compound score, the CGARP (Combined GNRI-ASA-RAI-PACS), to predict postoperative adverse outcomes in spine surgery NSQIP patients from 2015-2020. This study contributes to a more robust understanding of the intersectionality between patient frailty and nutritional status, underscoring the importance of frailty and nutritional status in informing spine surgery candidate selection and guiding perioperative risk stratification.
Interpretation of Results
Our dataset consisted of older patients with a median age of 60 years. Notably, this advanced age is associated with increased frailty levels, which complicates perioperative recovery and heightens unfavorable outcomes.5,6,20-22 Moreover, the compound score revealed that frail patients have the worst outcomes on all fronts—accounting for mortality, non-routine discharge, length of stay, complications, readmissions, and reoperations—compared with patients who are non-frail and those who are only at risk for being frail. These findings are in line with dozens of recent publications by our research group and by others demonstrating frailty as an independent predictor of adverse outcomes after brain and/or spine surgery22-24 A significant gender discrepancy was also noted, with males comprising 53% of the cohort and being more frail on average than females. Males had a higher risk of worse postoperative outcomes—including longer hospital stays, higher complication rates, and increased mortality. Underlying reasons for the sex differences in frailty among the original cohort could include different body compositions, as well as differing health-related behaviors not directly measured by RAI or GNRI including smoking, alcohol use, or obesity status that have been strongly associated with frailty and adverse spine surgery outcomes.25-30
Significant disparities across race and body weights were also observed in frailty. Patients who tended to be frail and required hospitalization for their surgical care had lower average BMI and tended to be non-white. These findings may emphasize the intersection of nutritional status and sociodemographic factors that are a critical driver of existing health disparities for both minority and frail patients.31,32
Implications of the CGARP Score
Interestingly, the application of the compound CGARP score showed superior prognostic ability in predicting discharge destination than the use of any 1 individual metric. The consistency of the composite score in predicting outcomes such as mortality is consistent with a theoretical framework of frailty: by representing more approaches to measuring frailty across these available tools, there is a more granular risk characterization compared to analysis via any 1 tool alone. The weighting of CGARP was intentionally derived from regression-based risk estimates, and sensitivity analyses confirmed that equal weighting resulted in diminished discriminatory performance. This suggests that the differential impact of frailty, nutritional status, and surgical risk factors should be accounted for in composite risk stratification models.33-35
The new composite score using RAI, GNRI, PACS, and ASA predicts postoperative outcomes with higher accuracy than any of the individual indices alone. GNRI alone predicted mortality, nonroutine discharge, eLOS, complications, Clavien-Dindo grade IV, readmission, and reoperation. RAI predicted mortality and Clavien-Dindo grade IV complications more accurately than ASA. The composite score showed stable prediction accuracy after internal validation, covering a wider scope of risk factors for better risk stratification and comprehensive patient management. The higher incidence of invasive surgery in this population necessitates the importance of accurate risk management. The greater gap between composite and individual scores highlights the improved discriminatory power of the composite score. Bowers et al demonstrated that the RAI-rev outperforms the mFI-5 in predicting 30-day mortality, Clavien-Dindo grade IV complications, nonhome discharge, and reoperation after ACDF. Covell et al found that the mASD-FI is effective for preoperative risk assessment in ASD surgery, predicting longer lengths of stay, higher complication rates, and inferior postoperative outcomes. While these studies have continued to validate the RAI as the premier frailty scale in spine surgery, improvements in outcome prognostication through frailty and nutritional status quantification may be a natural next step in risk stratification models.
The risk stratification table based on CGARP thresholds provides a practical and intuitive framework for clinical implementation. By categorizing patients into 4 tiers—Low, Medium, High, and Very High Risk—this analysis translates complex predictive modeling into accessible decision-making tools for clinicians. The identified cutoffs demonstrate a clear stepwise increase in the incidence of mortality, complications, and resource-intensive outcomes, such as NHD and extended LOS, across escalating CGARP strata. 36 These gradients not only validate the discriminatory accuracy of CGARP but also support its potential role in preoperative counseling, triage for enhanced recovery after surgery (ERAS) protocols, and identifying candidates for prehabilitation or nonoperative management. 37 While preliminary, this stratification framework offers actionable guidance and a foundation for future validation efforts aimed at threshold optimization and integration into perioperative workflows.
Other studies have found similar results utilizing the RAI framework., Bowers et al revealed in other spine and neurosurgical contexts like metastatic brain tumor resections that a higher RAI score is associated with increased risks of 30-day mortality, Clavien-Dindo grade IV complications and non-routine discharges across.5,30,38-40 Frailty scores can potentially be mitigated by preoperative identification, as surgeons may identify frail patients and tailor perioperative management to minimize associated risks. Similarly, the GNRI, demonstrates the impact of nutritional status on perioperative outcomes. Patients with malnutrition are at risk of higher rates of complications, longer lengths of stay and mortality. Moreover, preoperative nutritional supplementation is associated with reduced postoperative spine surgery complications.1,41-43 RAI-GNRI combines aspects of disease and nutritional status to enable an improved degree of risk stratification that allows for personalized interventions and higher quality care for each patient.
The results of this investigation also demonstrate that malnutrition or suboptimal nutritional status reduces the already impaired and reduced physiological reserve that characterizes frail patients and increases the physiological stress of surgery. This can further impede recovery, resulting in increased length of hospital stays and complication rates. This association between diminished GNRI score and increased complications parallels similar findings in previous literature, reinforcing the essential role nutrition has in achieving a successful postoperative recovery.20,24-27
Limitations
The present study has several limitations. The retrospective design may have subjective biases, resulting in inaccurate data entries or inconsistencies in the study parameters. We acknowledge that our analysis did not include calibration metrics or external validation, which limits its immediate clinical implementation. As such, we emphasize the need for future prospective validation in multicenter and non-NSQIP datasets. This would enhance generalizability and allow formal calibration analysis, such as calibration plots or Hosmer-Lemeshow tests, to better guide clinical decision-making. External validation of the CGARP score’s translational usefulness across various surgical groups and healthcare settings is essential. Therefore, future studies need to assess its effectiveness in real-world clinical settings and non-spine surgery populations to validate its wider application and scalability. Additionally, the large national database may not capture specific institutional protocols for measuring frailty indices, which could affect individual results. No tool can fully encompass the nuances of frailty and nutritional status. Although many of these indexes focus on functional ability, cognition, and exposure to factors predicted to increase mortality and morbidity, they predominantly assess frailty based on physical performance and health deficits. Nutritional assessments are primarily based on serum albumin and weight loss, overlooking the importance of specific nutrient adequacy and overall diet quality, which can significantly influence frailty and postoperative recovery. 44
Conclusion
This large data study reveals the synergistic effect of both frailty and impaired nutritional status in predicting postoperative adverse outcomes in patients undergoing spine surgery. The proposed compound CGARP score, which combines RAI, GNRI, PACS, and ASA classifications, demonstrated superior discrimination in predicting adverse outcomes in spine surgery. This innovation refines the ability to identify spine surgery patients at high-risk for adverse outcomes, allowing for personalized interventions to improve outcomes for these patients.
Supplemental Material
Supplemental Material - Predictive Value of Geriatric Nutritional Risk Index and Risk Analysis Index for Post-operative Outcomes in Spine Surgery Patients: A Comprehensive Analysis
Supplemental Material for Predictive Value of Geriatric Nutritional Risk Index and Risk Analysis Index for Post-operative Outcomes in Spine Surgery Patients: A Comprehensive Analysis by Stefan T. Prvulovic, BS, Sina Zoghi, MD, Aryan Gajjar, Cameron J. Sabet, Michael M. Covell, BA, Bhavya Pahwa, Nithin Gupta, BS, Meic H. Schmidt, MD, MBA, Marc D. Moisi, MD, Johnny Delashaw MD, and Christian A. Bowers, MD in Global Spine Journal.
Footnotes
Ethics Considerations
IRB approval was not required for this study as all patient information provided by the ACS-NSQIP is de-identified and publicly available.
Author Contributions
STP: conceptualization, methodology, data collection, formal analysis, writing – original draft, writing – review & editing; SZ: data collection, formal analysis, writing – original draft; AG: writing – original draft; CS: writing; - original draft; MMC: writing – review & editing; BP: data collection; NG: data collection; MHS: writing – review & editing, supervision; MDM: writing – review & editing, supervision; JD: writing – review & editing, supervision; CAB: conceptualization, methodology, formal analysis, writing – review & editing, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used to produce this manuscript are available from the corresponding author upon reasonable request.
Presentation Disclaimer
The following findings were presented at the Congress of Neurological Surgeons 2024 Annual Meeting in Houston, Texas. These findings were shared during our 6-minute oral presentation in the Sunrise Session on October 1st, 2024.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.