
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To evaluate the predictive performance of the Risk Analysis Index (RAI) and Modified 5-Item Frailty Index (mFI-5) in identifying risk for adverse postoperative outcomes in patients undergoing occipitocervical fusion (OCF).
Methods
The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database was queried for patients who underwent OCF from 2015 to 2020. Frailty was measured using both the RAI and mFI-5. The primary outcome was 30-day mortality. Secondary outcomes included major complications, minor complications, unplanned readmission, extended length of stay (eLOS), and non-home discharge (NHD). Multivariable logistic regression was used to assess associations, while receiver operating characteristic (ROC) curve analysis evaluated model discrimination.
Results
A total of 1637 patients were included (median age 68 years; 51.4% male). Higher frailty scores on both RAI and mFI-5 were associated with increased odds of mortality, major complications, and NHD. However, the RAI demonstrated superior discrimination for predicting mortality (C-statistic: 0.79 [95% CI: 0.75-0.83]) compared to mFI-5 (0.57 [95% CI: 0.53-0.61], P < .001), as well as for major complications (RAI: 0.64 vs mFI-5: 0.57, P = .01) and NHD (RAI: 0.73 vs mFI-5: 0.65, P < .001).
Conclusions
The RAI outperformed the mFI-5 in predicting key adverse outcomes following OCF. Incorporating RAI into preoperative evaluation may improve frailty-based risk stratification and guide surgical decision-making in vulnerable patients.
Introduction
Occipitocervical fusion (OCF) is a surgical procedure that seeks to stabilize the craniovertebral junction and is often performed to address instability arising from trauma or degenerative disease.1,2 This distinction is clinically important, as trauma-related instability is often associated with acute presentations requiring urgent surgical intervention, whereas degenerative disease is more frequently managed through elective procedures. 2 The primary objective of OCF is to restore structural stability, alleviate pain, and prevent neurological decline, which is crucial in conditions that impair the upper cervical spinal cord integrity. 3 Existing literature supports the efficacy of OCF, with high rates of neurological improvement, favorable fusion rates, and reduced postoperative complications.4,5 However, performing OCF in older patients necessitates a careful evaluation due to increased complication rates, with some studies reporting operative morbidity and mortality in up to 27% of patients, necessitating the value of accurate preoperative risk assessment tools, such as frailty metrics.1-3,6,7
Frailty, a multifactorial syndrome marked by reduced physiological resilience across bodily systems, poses significant challenges for OCF patients by increasing susceptibility to surgical stress and complicating recovery. The Risk Analysis Index (RAI) has emerged as a valuable tool for preoperative risk stratification and predicting postoperative adverse outcomes in spine surgery.8-10 Further, a growing body of evidence has repeatedly demonstrated the superior predictive capability of the RAI in predicting adverse outcomes compared to the commonly used Modified 5-Item Frailty Index (mFI-5). The RAI offers a more complete assessment of frailty by incorporating weighted factors across multiple domains. Conversely, the mFI-5 has been repeatedly criticized as a measure of multimorbidity, rather than true physiologic frailty.9,11
Despite the relevance of frailty metrics in surgical care, no studies have examined their specific application to OCF, underscoring a gap in targeted research for this high-risk population. 12 As such, this study sought to evaluate the impact of frailty, as measured by the RAI and mFI-5, on mortality rates following OCF.
Methods
Data Source
This study utilized data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. The NSQIP is a validated, multi-institutional database that captures detailed pre-, intra-, and postoperative outcomes for surgical patients across numerous surgical subspecialties, sourced from over 700 hospitals nationwide. Data entry is performed by ACS-trained clinical reviewers to ensure accuracy and consistency. 13 This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
Patient Selection
Patients ≥18 years who underwent OCF between 2015 and 2020 were identified using Current Procedural Terminology (CPT) codes 22 590 and 22 595. Exclusion criteria included patients >90 years old, missing discharge or transfer status, incomplete functional status data, absent ICD codes, and patients who left against medical advice. The rationale for restricting this study to OCF procedures was to ensure focus on pathologies specifically involving the occipitocervical junction. Other related procedures, such as C1-C2 fusion, were excluded in order to avoid heterogeneity in indications and anatomy across fusion levels; thus, this study specifically represents outcomes in patients undergoing OCF.
Frailty Metrics
Frailty was evaluated using the methodology previously established for the RAI and mFI-5.9,15,16 Briefly, the RAI includes weighted factors across multiple domains of frailty, such as age, sex, nutritional status, and physical performance and is scored from 0 to 81. 11 The RAI tier categorizations were as follows: 0-20 robust, 21-30 normal, 31-40 frail, and >40 very frail.
The mFI-5 is scored from 0-5 and is assessed by assigning 1 point for each of the following variables: functional status, diabetes, COPD, hypertension, and heart failure. 10 mFI-5 tier categorizations were as follows: 0 robust, 1 normal, 2 frail, & 3-5 very frail.
Outcomes and Complications
The primary outcome was 30-day mortality and secondary outcomes included incidence of major and minor complications, Clavien-Dindo Physical Status (PS) classification grade IV complications (CDIV), 30-day readmissions, 30-day reoperations, non-home discharge (NHD), and extended length of stay (eLOS) as described in prior literature.9,15,16 Major complications encompassed prolonged intubation exceeding 48 h, unplanned reintubation, sepsis, septic shock, pneumonia, deep vein thrombosis (DVT)/thrombophlebitis, pulmonary embolism (PE), acute cerebrovascular accident or stroke with neurological deficit(s), acute renal failure, myocardial infarction (MI), cardiac arrest requiring cardiopulmonary resuscitation, superficial surgical site infection (SSI), deep incisional SSI, organ space SSI, or wound disruption. CDIV were characterized by life-threatening organ dysfunction requiring intensive care, namely sepsis or septic shock, acute renal failure, pulmonary embolism (PE), myocardial infarction (MI), cardiac arrest requiring cardiopulmonary resuscitation, ventilation >48 h, and unplanned reintubation. eLOS was defined as hospital stays exceeding the 75th percentile of the study population (>8 days). Discharge designations were categorized into home and a facility that is home, or NHD, namely rehabilitation facility, skilled nursing facility, hospice care, and patients leaving against medical advice.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Software. Univariate and multivariate analyses were employed, with effect sizes reported as odds ratios and 95% confidence intervals. Receiver operating characteristic (ROC) curve analysis was used to assess the predictive power of each model. Comparisons of C-statistics between RAI and mFI-5 was performed using DeLong’s test. 17 A P-value of <.05 was considered statistically significant.
Results
Study Population Characteristics
Baseline Demographics, Clinical Characteristics, Hospital Characteristics, Peri/Post-Operative Complications, and Short-Term Outcomes of Patients Undergoing OCF (N = 1637)
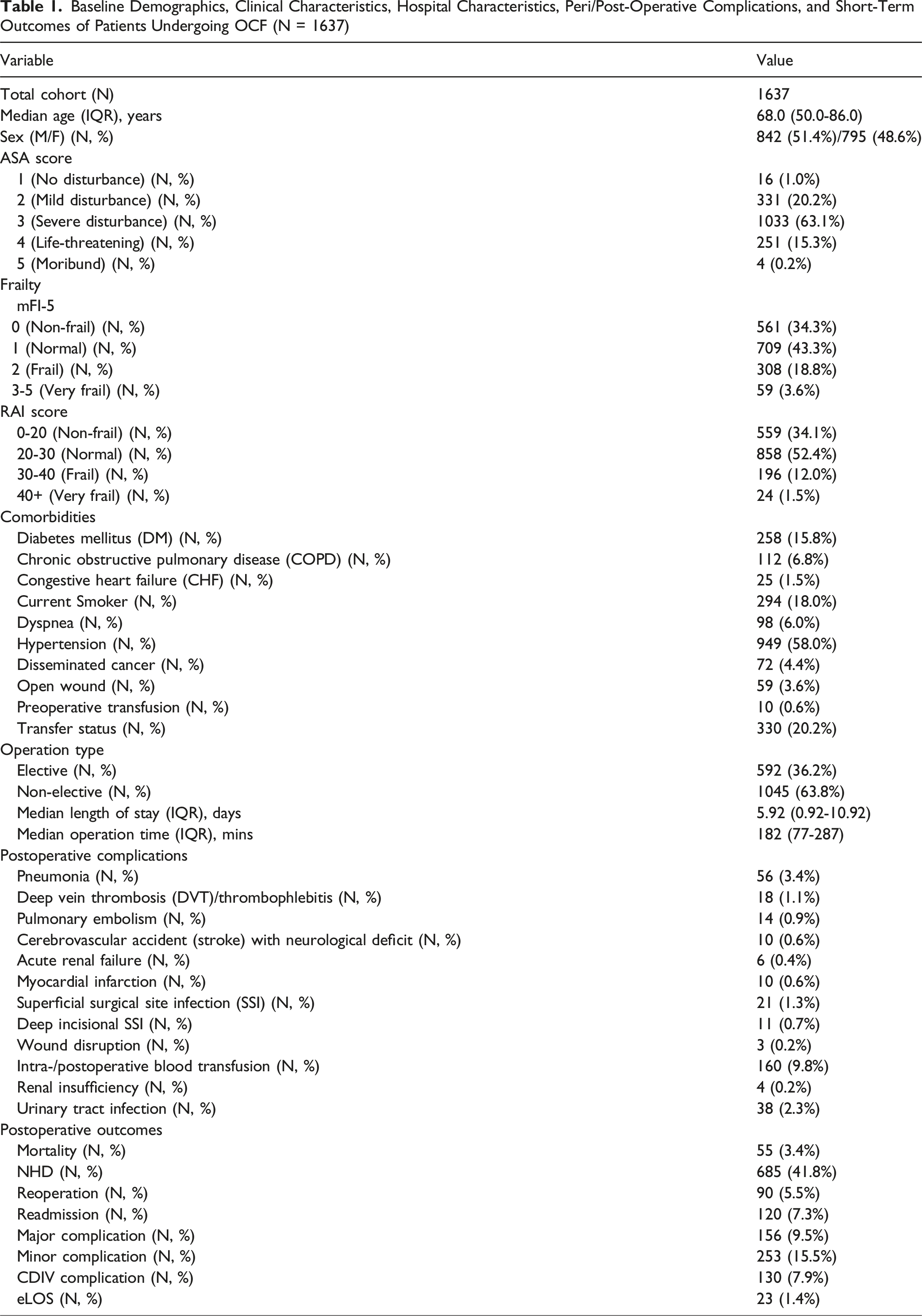
The modified frailty index (mFI-5) stratification demonstrated 34.3% (N = 561) of patients as robust, 43.3% (N = 709) normal, 18.8% (N = 308) frail, and 3.6% (N = 59) as very frail. The RAI score distribution indicated 34.1% (N = 559) as robust, 52.4% (N = 858) normal, 12.0% (N = 196) frail, and 1.5% (N = 24) very frail. The most common preoperative comorbidities were hypertension (58.0%, N = 949), diabetes mellitus (15.8%, N = 258), and current smoking status (18.0%, N = 294).
The most common major complications were pneumonia (3.4%, N = 56), deep vein thrombosis (1.1%, N = 18), and pulmonary embolism (0.9%, N = 14). The most common minor complication was intra- or postoperative blood transfusion (9.8%, N = 160). The median length of stay was 5.9 days (IQR: 0.9-10.9 days). NHD was reported for 41.8% of patients (N = 685) and major complications were reported for 9.5% (N = 156). There were 55 (3.4%) deaths overall within 30 days.
Multivariate Analysis
Multivariate Analysis Odds Ratios (OR) RAI Frailty Tier and Postoperative Outcomes for Patients Who Underwent OCF in the ACS NSQIP Database (2015-2020)
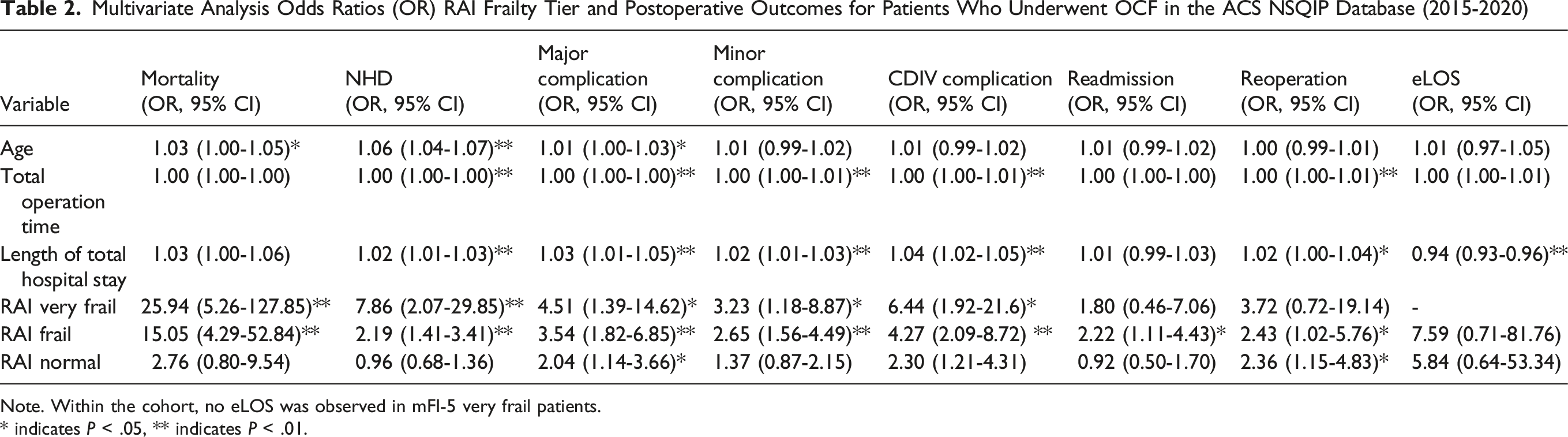
Note. Within the cohort, no eLOS was observed in mFI-5 very frail patients.
* indicates P < .05, ** indicates P < .01.
Multivariate Analysis Odds Ratios (OR) mFI-5 Frailty Tier and Postoperative Outcomes for Patients Who Underwent OCF in the ACS NSQIP Database (2015-2020)
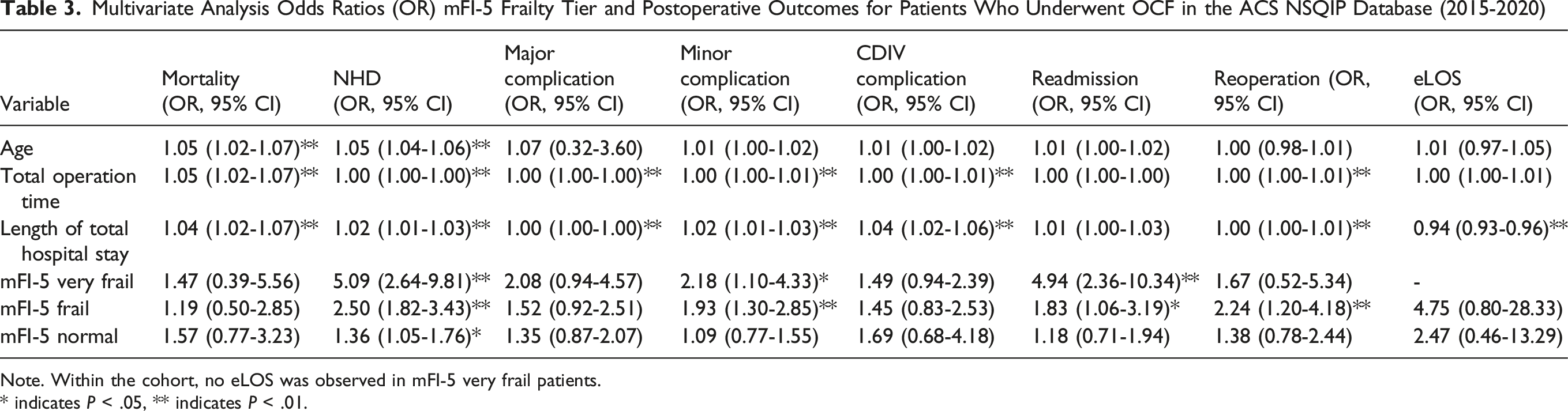
Note. Within the cohort, no eLOS was observed in mFI-5 very frail patients.
* indicates P < .05, ** indicates P < .01.
Increasing frailty also independently predicted major complications (mFI-5 Very Frail = OR: 2.08, 95% CI: 0.94-4.57, P = .177; RAI Very Frail = OR: 4.51, 95% CI: 1.39-14.62, P < .01), minor complications (mFI-5 Very Frail = OR: 2.18, 95% CI: 1.10-4.33, P < .05; RAI Very Frail = OR: 3.23, 95% CI: 1.18-8.87, P < .05) CDIV complications (mFI-5 Very Frail = OR: 1.49, 95% CI: 0.94-2.39, P = .25; RAI Very Frail = OR: 6.44, 95% CI: 1.92-21.6, P < .05), and NHD (mFI-5 Very Frail = OR: 5.09, 95% CI: 2.64-9.81, P < .01; RAI Very Frail = OR: 7.86, 95% CI: 2.07-29.85, P < .01). No significant associations were found for reoperation, readmission, or eLOS across frailty tiers for either measure. Collinearity analysis demonstrated no evidence of problematic multicollinearity among the variables included in the multivariable regression models. The variance inflation factor (VIF) values ranged from 1.03 to 1.37, and tolerance values ranged from 0.73 to 0.98 for age, operation time, total length of stay, and RAI. All values were well within acceptable limits, supporting the stability and reliability of the regression models.
AUROC Analysis
AUROC analysis was conducted to assess the discriminatory accuracy of the mFI-5 and RAI for the primary endpoint, 30-day mortality, and the secondary outcomes in patients undergoing OCF (Figure 1). The RAI demonstrated superior discrimination compared to the mFI-5 for predicting 30-day mortality (RAI: C-statistic = 0.79, 95% CI 0.72-0.86 vs mFI-5:C-statistic = 0.57, 95% CI 0.50-0.63) (P < .001, DeLong test). RAI demonstrated superior discrimination predicting secondary outcomes compared to the mFI-5 in predicting major complications, CDIV complications, and NHD only (Supplementary Table 1). ROC Curves for Predictive Performance of the Retrospective RAI and mFI-5 for Postoperative Outcomes for Patients Who Underwent OCF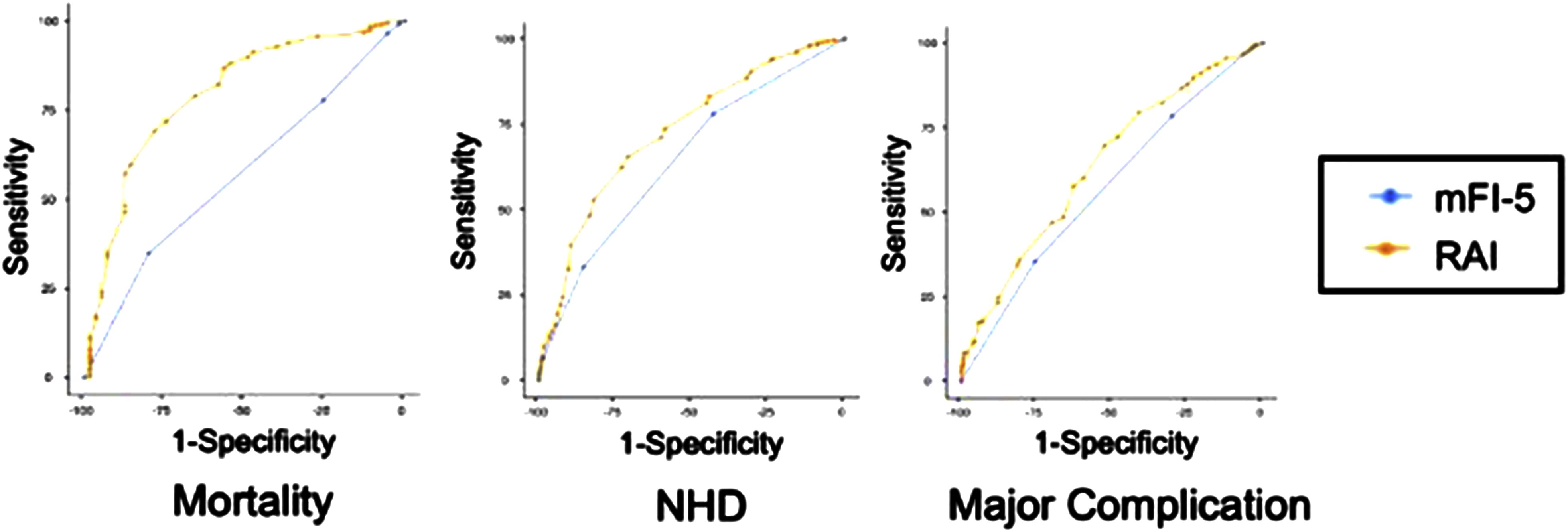
Discussion
In this large database cohort study of 1637 OCF patients, the RAI demonstrated superior discrimination compared to the mFI-5 in predicting adverse outcomes. Increasing patient frailty, as measured by the RAI, was an independent predictor of 30-day mortality, with 25.94 greater odds than the mFI-5. Furthermore, increasing RAI score also independently predicted major complications and NHD with greater odds than mFI-5. Importantly, RAI demonstrated superior discrimination compared to the mFI-5 for 30-day mortality, highlighting its value as a risk stratification tool in this high-risk population; however, while statistically significant (P = .01), the difference in discrimination between RAI and mFI-5 for major complications was less pronounced than for mortality (P < .001). Thus, this finding should be considered moderately superior rather than unequivocal. To the authors’ knowledge, this is the first RAI OCF study, clearly establishing the utility of the RAI compared with the mFI-5 as a preoperative risk stratification instrument to predict adverse outcomes in patients undergoing OCF.
Previous OCF outcomes studies have described varying mortality rates following OCF. Previous studies have reported a 30-day mortality rate of 3.75%–4.3%, similar to the 3.4% mortality rate reported in our study.2,18 Interestingly, 2-year mortality rates exceeding 25% have been reported in patients ≥65 years old, presumably due to the impact of greater comorbidity burden combined with a higher incidence of frailty in this cohort of substantially older patients.19,20 These findings support the premise that multiple contributors to patient frailty status play a pivotal role in adverse outcomes in OCF, bolstering our findings demonstrating the superior discrimination by the RAI compared to the mFI-5 in predicting 30-day mortality.
While both the mFI-5 and RAI correlated significantly with 30-day mortality and secondary outcomes such as major complications and NHD, the RAI consistently possessed increased odds and superior discrimination, highlighting the critical limitations inherent to mFI-5 as a solitary frailty variable. Our findings align with the avalanche of accumulating evidence in the spine surgery literature, demonstrating the RAI’s superior discrimination in predicting adverse outcomes, such as with ACDF, spinal deformity surgery, spinal metastasis surgery, and lumbar interbody fusion.15,16,21-27 The mFI-5 has been increasingly recognized as a unidimensional measure of multimorbidity, rather than a metric accounting for true decreased physiologic reserve.9,15,16,19 The 25.94 times greater odds and superior discrimination that the RAI demonstrated in predicting 30-day mortality, results from the RAI’s improved ability to consistently and precisely quantify decreased physiologic reserve. Unlike the mFI-5, the RAI incorporates deficits across 5 essential domains of frailty: functional, cognitive, nutritional, psychological, and physiological. 10 This multidimensional concept of domains of frailty has been utilized in prior studies specifically evaluating upper cervical spine procedures identifying the RAI as a powerful predictor of adverse outcomes, including complications, NHD, and mortality, aligning with our OCF findings in this study.15,28,29 These results are particularly relevant for OCF patients, who represent a unique surgical cohort due to complex airway management and higher rates of non-elective presentation, all of which compound surgical risk and may exacerbate frailty-related vulnerabilities.30-34 To further contextualize the role of frailty in OCF and trauma surgery, recent systematic reviews have emphasized frailty’s prognostic value in trauma populations. Notably, Roohollahi et al (2023) and Roohollahi et al (2024) found frailty to be strongly predictive of adverse outcomes in traumatic spinal injury and traumatic brain injury, respectively, further supporting the incorporation of frailty screening tools in acute surgical decision-making.35,36
The associated risks inherent to OCF are amplified in older and medically complex patients, in whom decreased respiratory reserve, altered airway anatomy, and sarcopenia impair the body’s ability to tolerate the significant stressors of prolonged anesthesia, prone positioning, and perioperative instability.30-34 In particular, age-related pulmonary changes such as reduced vital capacity and impaired mucociliary clearance increase vulnerability to postoperative pneumonia and prolonged ventilation. 37 Altered upper airway anatomy and cervical deformity can complicate intubation and airway maintenance, raising the likelihood of perioperative airway compromise. 38 Sarcopenia and diminished cervical musculature reduce physiologic reserve and limit postoperative functional recovery. 39 Therefore, adopting the RAI into routine clinical perioperative practice offers substantial advantages, particularly given its validated ease of use and brief bedside administration (often completed within 1 minute), facilitating rapid and accurate identification of higher-risk patients for adverse outcomes.40,41 Clinically, the RAI’s accuracy predicting OCF mortality informs preoperative risk discussions, including discussion of the informed consent process, perioperative optimization strategies, and postoperative resource allocation. 42 Implementing targeted interventions, such as pulmonary rehabilitation protocols, early mobilization initiatives, enhanced nutritional support, and aggressive management of perioperative respiratory mechanics and airway patency, can be prioritized for patients identified as frail by the RAI, potentially mitigating complications and reducing mortality risk. 40 However, given the retrospective design, short-term outcome window, and relatively low event number for mortality, conclusions regarding immediate clinical adoption should be tempered. Prospective validation studies are required prior to broader integration of the RAI into standard perioperative pathways for OCF. Additionally, the wide confidence intervals observed for the “very frail” subgroup warrant cautious interpretation.
Limitations
Limitations of this study are primarily attributed to its retrospective design and dependence on the ACS-NSQIP administrative database, which, although standardized and high-quality, lacks granular clinical, radiographic, and surgical details. Outcome assessments were limited to 30 days postoperatively, precluding longer-term analyses such as functional recovery or fusion success rates. This distribution of elective to non-elective cases suggests that the majority of cases likely represent trauma, or acute pathology-driven instability, whereas a smaller subset more likely reflects degenerative disease. Although subgroup analysis by etiology was not feasible due to coding constraints within NSQIP, we acknowledge that trauma and degenerative OCF patients may have distinct frailty and outcome profiles, an important area for future investigation. Further, the relatively low mortality event rate raises the possibility of model instability or overfitting. Although age, operative time, and length of stay were controlled in multivariable regression, residual confounding from unmeasured surgical factors, such as blood loss, approach, or intraoperative airway complexity, may persist. Collinearity was assessed and found acceptable. Calibration statistics are reported, but further external validation is warranted. Additional considerations include potential selection bias given the NSQIP sampling methodology and uncertain generalizability beyond U.S. NSQIP centers. An additional limitation stems from the low number of OCF patients identified in the database. Despite these limitations, our robust findings demonstrate that the RAI’s comprehensive representation of frailty provides significantly superior discrimination compared to mFI-5 in predicting mortality in OCF patients. Future prospective studies should validate these findings specifically for OCF populations, further establishing the RAI’s clinical utility, thus informing best practices in surgical risk stratification.
Conclusion
This study is the first to apply large-scale evidence comparing the RAI and mFI-5 in patients undergoing OCF. Our findings demonstrate that the RAI significantly outperforms the mFI-5 in predicting 30-day mortality, major complications, and NHD in OCF patients. These results suggest that frailty, as measured by the RAI, is a useful predictor of adverse outcomes in OCF. The RAI offers a clinically validated framework for identifying high-risk patients, informing preoperative discussions, and optimizing perioperative planning for prospective OCF patients. Routine clinical implementation of the RAI in OCF should be supported by prospective validation to confirm its predictive accuracy and generalizability in this unique population.
Supplemental Material
Supplemental Material - Comparison of the Risk Analysis Index and the Modified 5-Item Frailty Index in Predicting 30-Day Morbidity and Mortality After Occipitocervical Fusion
Supplemental Material for Comparison of the Risk Analysis Index and the Modified 5-Item Frailty Index in Predicting 30-Day Morbidity and Mortality After Occipitocervical Fusion by Omar Sbaih, Nithin Gupta, Dilibe Ekowa, Stefan Prvulovic, Kush Modi, Mark Miller, Rohin Singh, William DiCiurcio, Ruchir Nanvati, Matthew H. Meade, Jonathan Stone, and Christian Bowers in Global Spine Journal
Footnotes
Ethical Considerations
This study utilized a de-identified national database (ACS-NSQIP) and did not involve direct patient interaction; therefore, ethical approval and informed consent were not applicable.
Author Contributions
Omar Sbaih contributed to study conception and design, data analysis, interpretation of results, and drafting of the manuscript. Nithin K. Gupta contributed to data interpretation, clinical validation, drafting of the manuscript and critical revision of the manuscript. Dilibe Ekowa and Stefan Prvulovic assisted with data collection, literature review, and drafting of the manuscript. Kush Modi and Ruchir Nanavati contributed to statistical analysis and figure/table preparation. Mark Miller, Rohin Singh, William DiCiurcio, and Matthew Meade provided clinical insight, reviewed the manuscript for important intellectual content and critically revised the manuscript. Jonathan Stone provided senior statistical guidance, supervised the project, and critically revised the manuscript. Christian Bowers conceived the study, provided neurosurgical expertise, oversaw project execution, and contributed to final manuscript approval. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are derived from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP), which is a publicly available, de-identified dataset. As such, a formal data availability statement is not applicable.
Supplemental Material
Supplemental material for this article is available online.