
Abstract
Study Design
Observational Retrospective Cohort Study.
Objectives
To compare the discriminatory abilities of the Revised Risk Analysis Index (RAI-Rev) and the 5-Factor Modified Frailty Index (mFI-5) to predict major postoperative outcomes in DCM patients overall, and by anterior (ADF) or posterior (PDF) approaches for decompression and fusion.
Methods
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried for DCM patients undergoing ADF or PDF from 2015-2020. Logistic regression and Receiver Operating Characteristic analysis were used to compare the predictive and discriminatory value of mFI-5 and RAI-Rev for 30-day outcomes.
Results
18,138 DCM patients were included (median age: 61 years). Both RAI-Rev and mFI-5 predicted 30-day outcomes; however, increasing frailty as measured by RAI-Rev demonstrated greater odds ratios. RAI-rev demonstrated superior discrimination for non-fatal adverse outcomes, notably non-home discharge (NHD) [C-statistic 0.72 (95% CI 0.71-0.73, P < 0.001)], and for all non-fatal measures except major complications (P < 0.05). Sub-analysis by approach showed frailty had greater predictive accuracy for adverse outcomes in ADF compared to PDF.
Conclusions
The RAI-Rev demonstrated superior discrimination predicting non-fatal outcomes following DCM when compared to the mFI-5, with equivalent mortality prediction. Further, frailty plays a stronger role in predicting mortality and morbidity in ADF compared to frailty’s impact on predicting outcomes with PDF. This finding demonstrates the utility of the RAI-Rev in preoperative risk stratification with an increasingly frail patient population and provides initial evidence for selecting posterior approaches for DCM patients as frailty increases.
Introduction
Degenerative cervical myelopathy (DCM) is a degeneration of the cervical spine with subsequent symptomatic compression of the spinal cord, which has increasingly affected aging populations. 1 As the elderly population is expected to almost double from 58 million in 2022 to 82 million in 2050, the incidence of DCM will continue to rise. 2 Surgical decompression of the spinal cord is the mainstay of treatment in moderate-to-severe disease, with data to suggest benefits in earlier disease as well.3,4 Older patients frequently have more advanced disease, require higher risk surgical approaches, and have lower functional scores postoperatively; although, the functional improvement with surgery is comparable to younger patients. 5
Frailty, or decreased baseline physiologic reserve, is a multifaceted syndrome that manifests across multiple organ systems and reflects a patient’s vulnerability to internal and external stressors, resulting in adverse postoperative outcomes.6,7 Previously, the modified frailty index-11 (mFI-11) or its abbreviated form, the modified frailty index-5 (mFI-5), were used to measure frailty.8-11 However, the mFI has been critiqued in recent years for more so resembling a comorbidity index rather than a measure of true frailty, especially when compared to the Risk Analysis Index (RAI).12-14 The RAI was developed by Hall et al to more effectively capture the factors influencing frailty.15,16 There is now a growing body of evidence, especially regarding spinal pathologies, to support superior outcome discrimination when using the Revised Risk Analysis Index (RAI-Rev).17,18
As of this time, there is no current literature assessing discrimination of the RAI-Rev for predicting adverse outcomes for anterior (ADF) compared to posterior (PDF) approaches for decompression and fusion in degenerative cervical myelopathy. This study evaluates the discriminative thresholds of the RAI-Rev and mFI-5 on 30-day major postoperative outcomes in DCM patients using data from a large national cohort drawn from American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) and analyzes subgroups by anterior vs posterior approach. 19
Methods
Data Source
The present study investigated the ACS-NSQIP database, in keeping with the NSQIP Data Use Agreement. Established within the Veterans Health Administration in 1994, the NSQIP was designed to moderate and improve healthcare quality. Following its effective implementation within the Veterans Health Administration, it became available to the private sector in 1999. We utilized the NSQIP data from 2015 to 2020, with approximately six million patient records, comprising over 200 variables including patient demographics, comorbidities, and postoperative outcomes. To maintain data integrity, onsite surgical clinical reviewers are employed alongside regular internal audits to ensure inter-rater reliability.
Patient Population and Baseline Characteristics
Patients eligible for this study were those diagnosed with DCM who underwent cervical decompression and fusion surgery. This procedure included anterior approaches and/or posterior approaches (both instrumented and non-instrumented). Supplemental Table 1 summarizes the specific ICD-9/10-CM and CPT codes utilized in this study.
The study examined various demographic and baseline variables such as age, gender, height, weight, Body Mass Index (BMI), length of hospital stay, transfer status, operation time, and history of medical conditions including diabetes mellitus, Chronic Obstructive Pulmonary Disease (COPD), Congestive Heart Failure (CHF), dyspnea, hypertension, cancer, open wounds, steroid use, significant unintentional weight loss (>10%), bleeding disorders, preoperative transfusion, sepsis, systemic inflammatory response syndrome (SIRS), functional dependence, and smoking status.
Frailty Indices
Frailty was assessed using the RAI-Rev scoring system, adapted from previous studies by Hall et al and Arya et al12,14 RAI incorporates sex, age, cancer diagnosis (excluding melanoma), weight loss (unintentional weight loss of 4.5 kg over 3 months), renal failure, CHF, poor appetite, shortness of breath at rest, residence status (independence of living), cognitive decline, and activities of daily living (Supplemental Table 2). However, preoperative cognitive decline, another variable originally included in RAI, was not included in the present study due to NSQIP data limitations. Scores were categorized into robust, normal, frail, and very frail tiers based on specific score ranges. Score stratification of the RAI-Rev is as follows: robust ≤10, normal 11-20, frail 21-30, and very frail ≥31 RAI-Rev scores.
The modified frailty index was initially developed with 11 variables (mFI-11). 20 However, it was later modified to include only five variables as a result of changes in reporting requirements. 21 These variables include history of diabetes, hypertension, functional dependence, COPD, and CHF, with one point attributed to each condition. The mFI scores range from 0 to 5, and the tiers are as follows: nonfrail 0, prefrail 1, frail 2, and severely frail ≥3.
Outcome Measures
The primary outcomes included 30-day mortality, non-home discharge (NHD), extended length of stay (eLOS), minor complications, major complications, Clavien-Dindo Physical Status (PS) classification grade IV complications (CDIV), 30-day unplanned readmission, and 30-day unplanned reoperation. Minor complications included intra-/postoperative blood transfusion, renal insufficiency, or urinary tract infection (UTI). Major complications encompassed prolonged intubation exceeding 48 hours, unplanned reintubation, sepsis, septic shock, pneumonia, deep vein thrombosis (DVT)/thrombophlebitis, pulmonary embolism (PE), acute cerebrovascular accident or stroke with neurological deficit(s), acute renal failure, myocardial infarction (MI), cardiac arrest requiring cardiopulmonary resuscitation, superficial surgical site infection (SSI), deep incisional SSI, organ space SSI, or wound disruption. CDIV were characterized by life-threatening organ dysfunction requiring intensive care, namely sepsis or septic shock, acute renal failure, pulmonary embolism (PE), myocardial infarction (MI), cardiac arrest requiring cardiopulmonary resuscitation, ventilation >48 hours, and unplanned reintubation. eLOS was defined as hospital stays exceeding the 75th percentile of the study population. Discharge designations were categorized into home and a facility that is home, or NHD, namely rehabilitation facility, skilled nursing facility, hospice care, and patients leaving against medical advice.
Statistical Analysis
Continuous variables with non-normal distribution are reported as median with Interquartile Range (IQR). The distribution of the data was determined by employing the Kolmogorov-Smirnov test. Comparisons of medians of non-normally distributed continuous variables were carried out using Kruskal-Wallis test while the categorical variables were analyzed using Chi-square tests. Univariable and multivariable logistic regression analyses were performed for mFI-5, and RAI-Rev, and the following outcomes: 30-day mortality, NHD, eLOS, minor complications, major complications, CDIV, 30-day unplanned readmission, and 30-day unplanned reoperation. The effect sizes for dichotomous outcomes were presented as odds ratio (OR) and 95% Confidence Interval (CI). Receiver Operating Characteristic (ROC) curve analysis including the Area Under the ROC Curve (AUC)/C-statistics calculations were used to evaluate the discriminatory accuracy of the mFI-5 and RAI-Rev for primary outcomes. The DeLong test was used to compute the significance of the C-statistic difference between the frailty indices. Statistical analyses were carried out using Excel (Microsoft, Redmond, WA, USA), IBM SPSS Statistics ver. 27.0 (IBM Co., Armonk, NY, USA), and STATA 12.0 (StataCorp, College Station, TX, USA). P < 0.05 was considered statistically significant.
Results
Study Population Characteristics
A total of 18,138 patients with DCM who met the inclusion criteria were included in this study (Figure 1). The median age of the cohort was 61 years (IQR: 53 - 69 years) and 56.4% were male. The median BMI was 29.45 kg/m2 (IQR: 25.75 - 34.01 kg/m2) and the most common comorbidities within the cohort were hypertension (56.7%), smoking (25.3%) and diabetes mellitus (21.8%). Stratification of the cohort by frailty group as measured by the mFI-5 was as follows: robust 36.9%, normal: 39.9%, frail 20.1%, and very frail 3.1%. Distribution of frailty tiers as measured by RAI-Rev was as follows: robust: 5.6%, normal: 50.7%, frail: 40.7%, and very frail: 3.0%. Selection process for study cohort. Abbreviations: ACS-NSQIP; American College of Surgeons National surgical quality improvement program.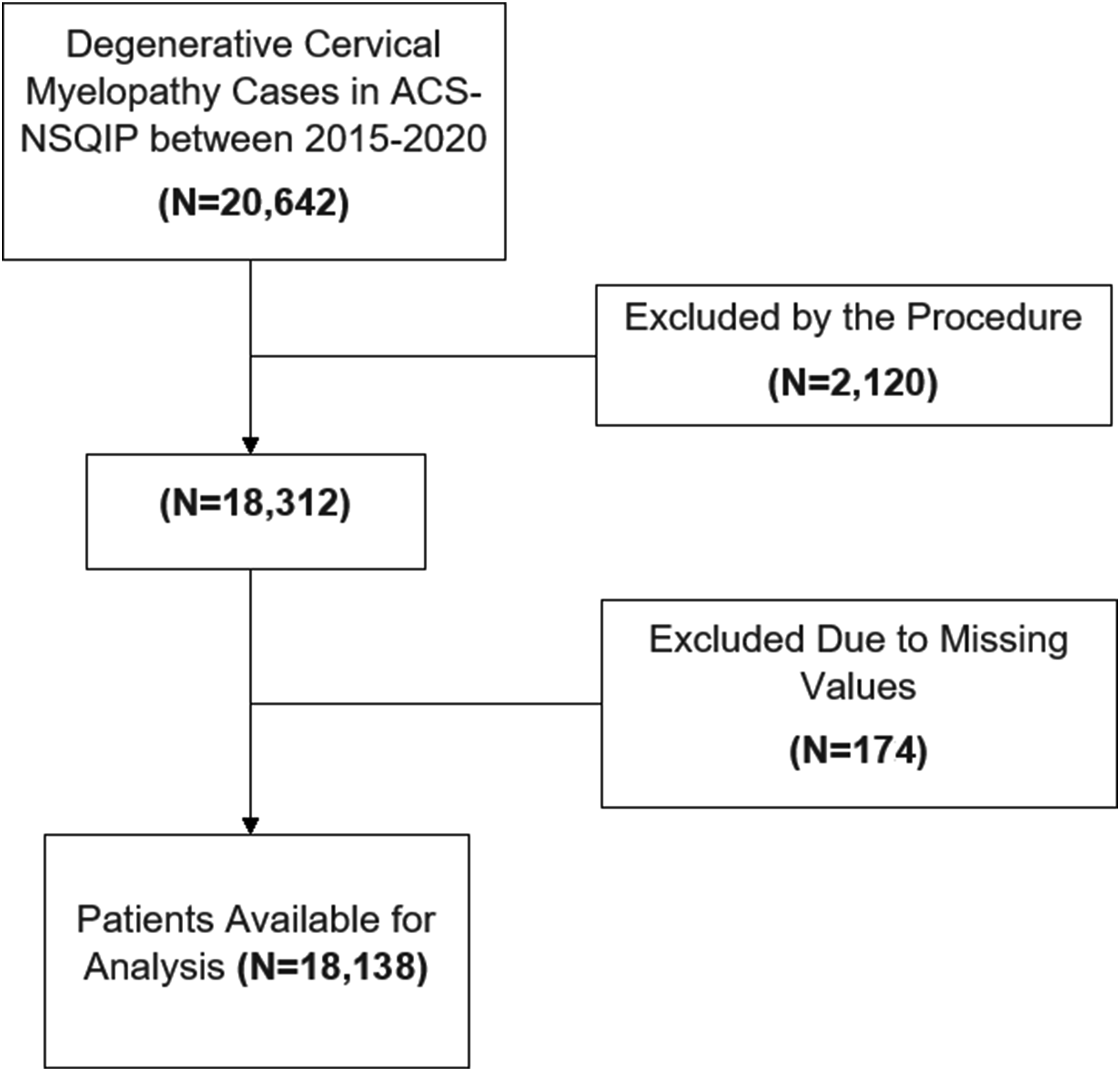
Overview of baseline, preoperative, intraoperative and postoperative characteristics of the study cohort, stratified by frailty tier as defined by the RAI-Rev.
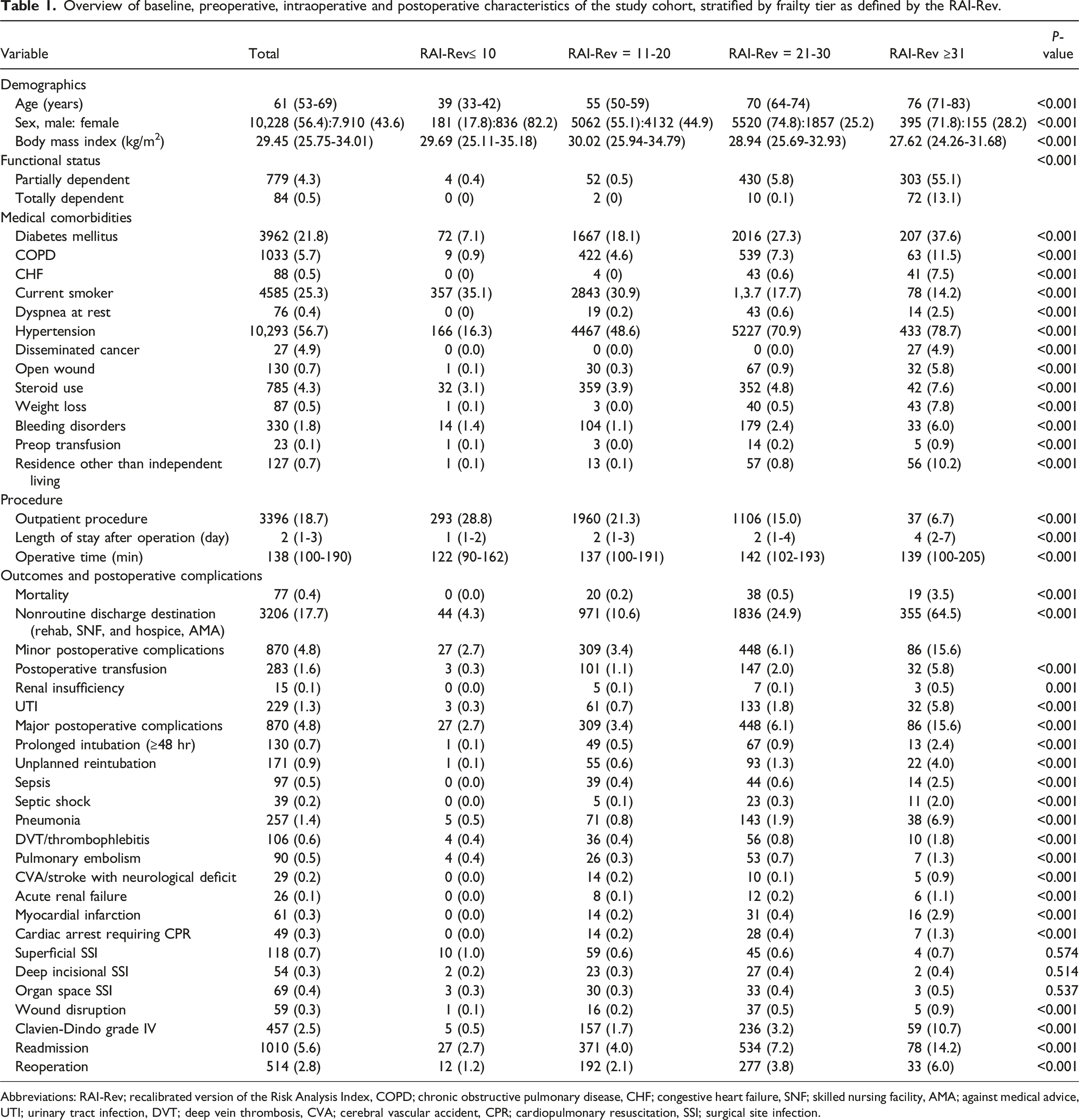
Abbreviations: RAI-Rev; recalibrated version of the Risk Analysis Index, COPD; chronic obstructive pulmonary disease, CHF; congestive heart failure, SNF; skilled nursing facility, AMA; against medical advice, UTI; urinary tract infection, DVT; deep vein thrombosis, CVA; cerebral vascular accident, CPR; cardiopulmonary resuscitation, SSI; surgical site infection.
Univariate Analysis of mFI-5 and RAI-Rev for 30-Day Postoperative Outcomes
Univariate analysis of the mFI-5 and RAI-Rev for 30-day postoperative outcomes in DCM patients.
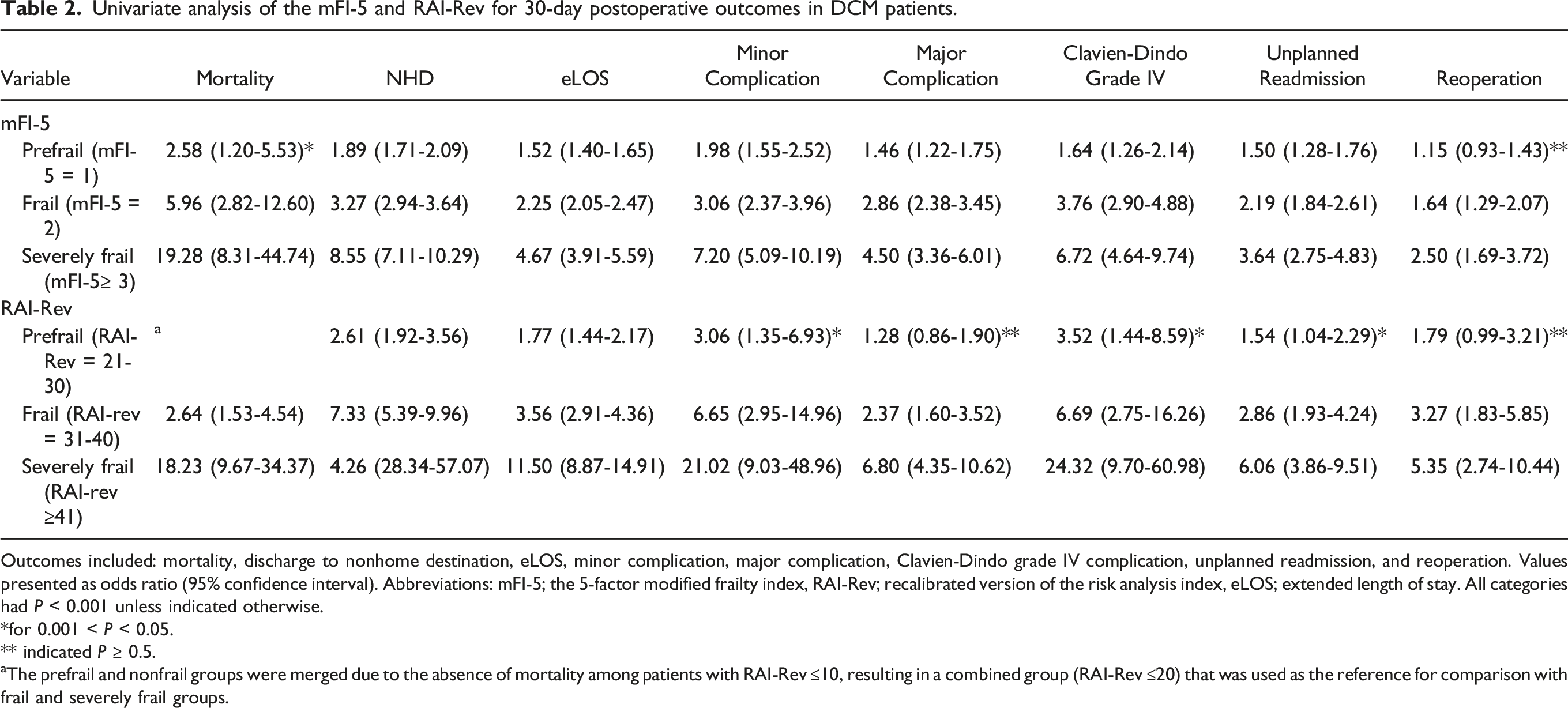
Outcomes included: mortality, discharge to nonhome destination, eLOS, minor complication, major complication, Clavien-Dindo grade IV complication, unplanned readmission, and reoperation. Values presented as odds ratio (95% confidence interval). Abbreviations: mFI-5; the 5-factor modified frailty index, RAI-Rev; recalibrated version of the risk analysis index, eLOS; extended length of stay. All categories had P < 0.001 unless indicated otherwise.
*for 0.001 < P < 0.05.
** indicated P ≥ 0.5.
aThe prefrail and nonfrail groups were merged due to the absence of mortality among patients with RAI-Rev ≤10, resulting in a combined group (RAI-Rev ≤20) that was used as the reference for comparison with frail and severely frail groups.
ROC Curve Analysis and C Statistic
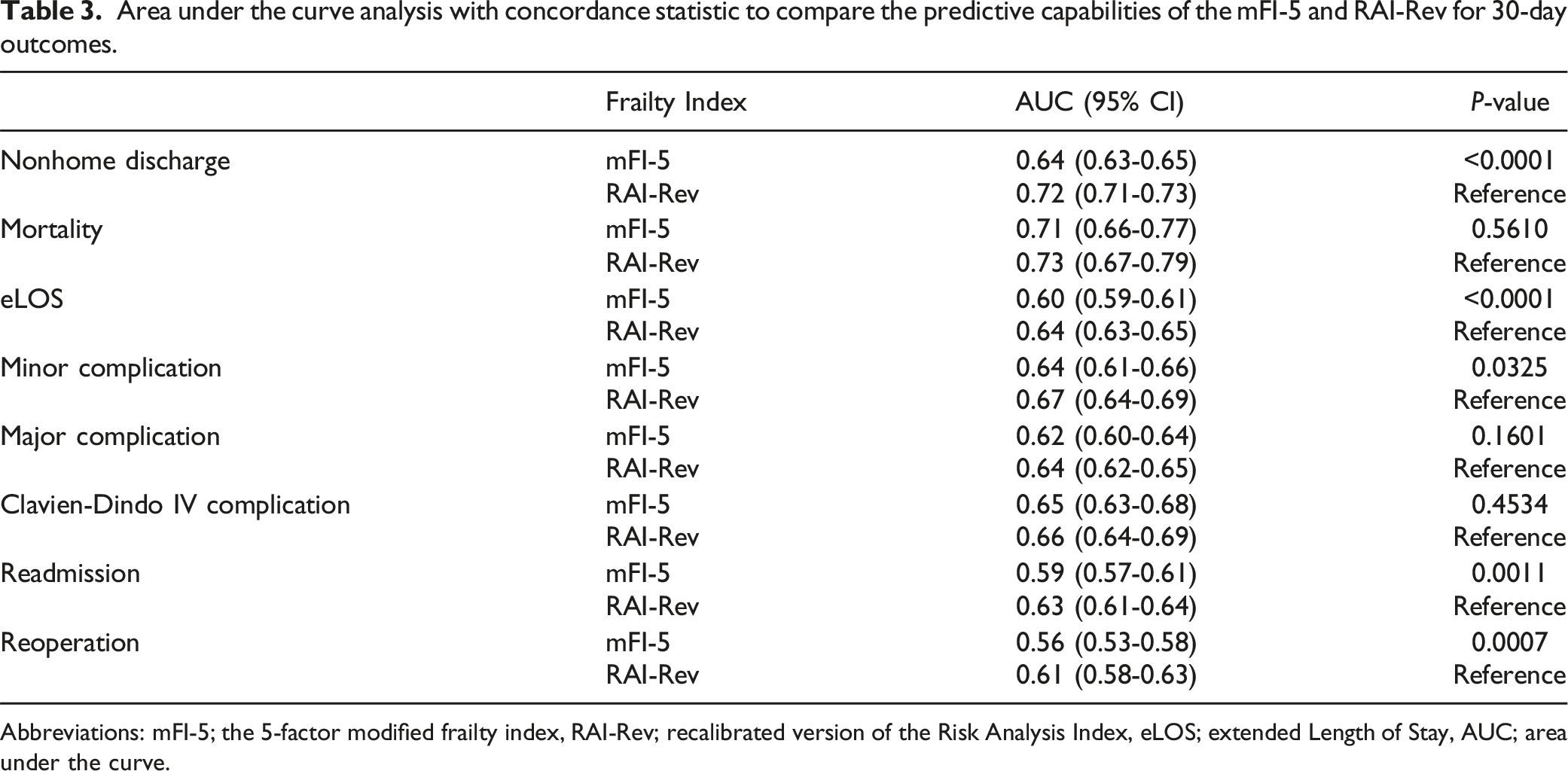
AUROC curve analysis was conducted for DCM patients to determine the discriminatory accuracy of the mFI-5 and RAI-Rev for predicting the primary postoperative outcomes (Figure 2 and Table 3). For NHD prediction, RAI-Rev had significantly greater performance (C-statistic = 0.72, 95% CI, 0.71 - 0.73) than the mFI-5 (C-statistic = 0.64, 95% CI, 0.63 - 0.65, P < 0.00. Similarly, for extended length of stay (eLOS), RAI-Rev significantly outperformed mFI-5 (RAI-Rev: C-statistic = 0.64, 95% CI, 0.63 - 0.65 vs mFI-5: C-statistic = 0.60, 95% CI, 0.59 - 0.61; P < 0.0001). RAI-Rev further outperformed the mFI-5 in predicting minor complications and readmission. It also demonstrated superior discrimination than mFI-5 only for reoperation (P = 0.0007). There was no significant difference in discriminative thresholds for predicting postoperative mortality. AUC curves [(a) mortality, (b) nonhome discharge, (c) eLOS, (d) minor complications, (e) major complications, (f) Clavien-Dindo IV complications, (g) readmission, (h) reoperation] and forest plot for prediction of 30-day outcomes after surgery for DCM by the mFI-5 and RAI-Rev. Area under the curve analysis with concordance statistic to compare the predictive capabilities of the mFI-5 and RAI-Rev for 30-day outcomes. Abbreviations: mFI-5; the 5-factor modified frailty index, RAI-Rev; recalibrated version of the Risk Analysis Index, eLOS; extended Length of Stay, AUC; area under the curve.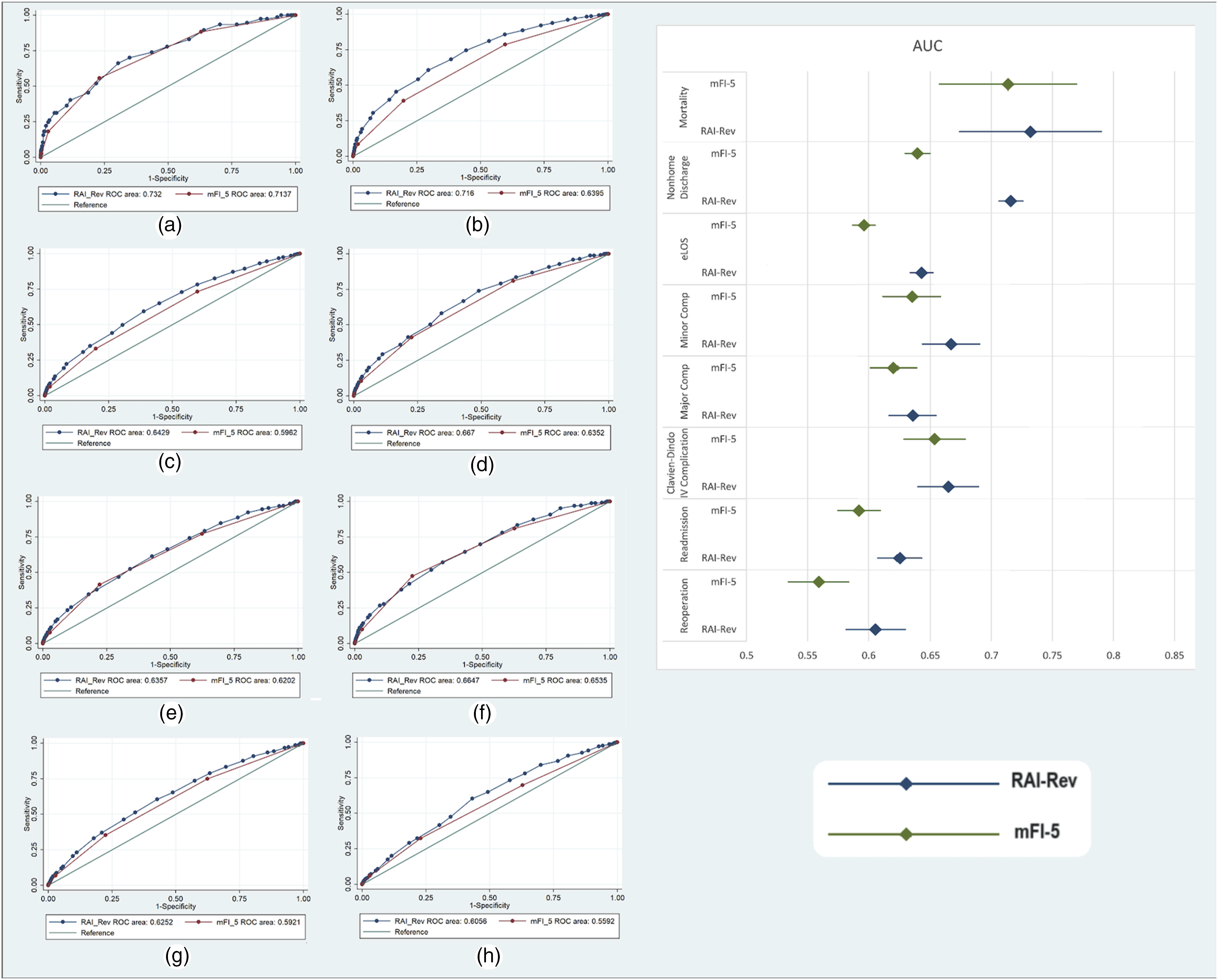
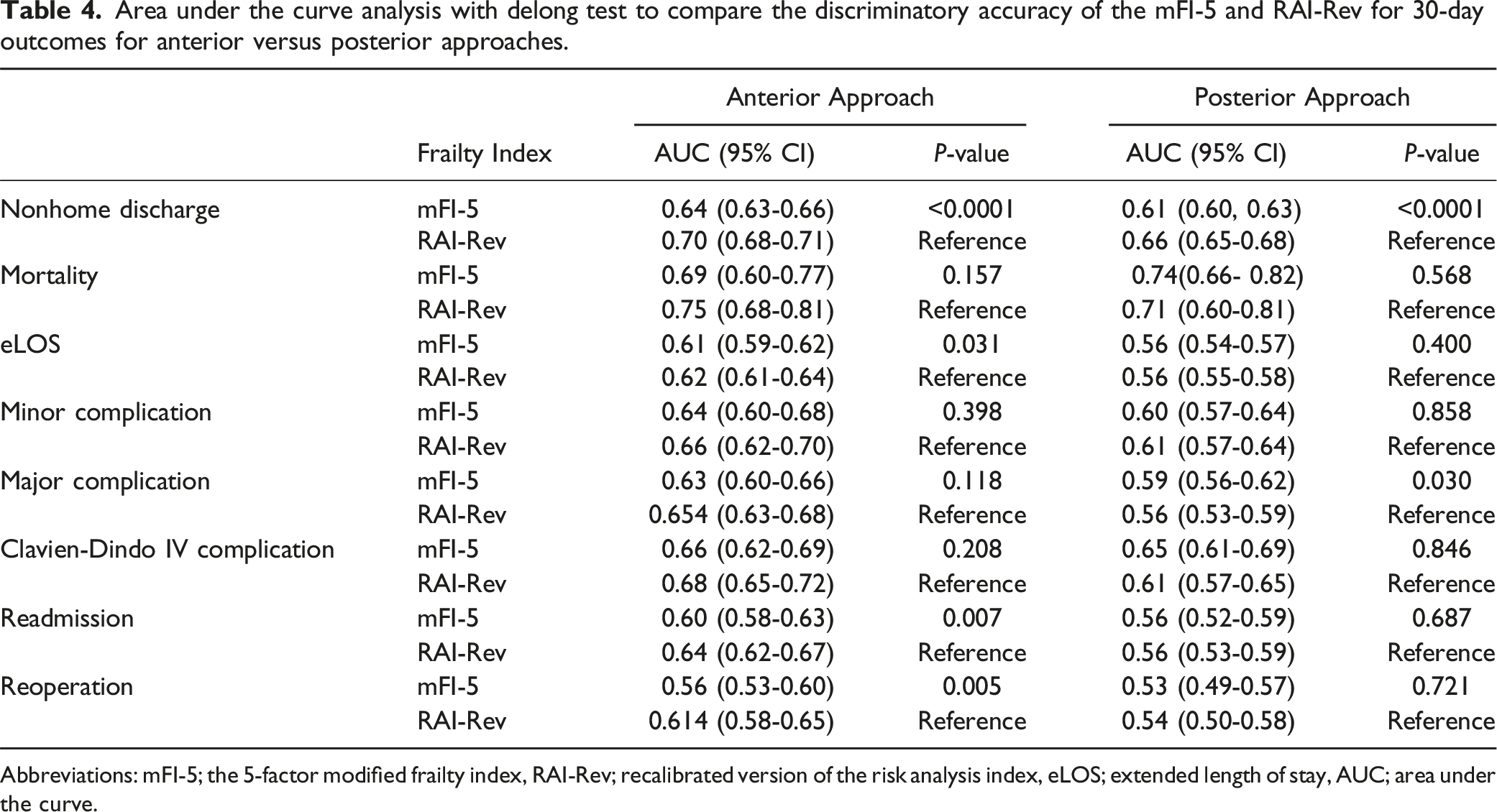
Area under the curve analysis with delong test to compare the discriminatory accuracy of the mFI-5 and RAI-Rev for 30-day outcomes for anterior versus posterior approaches.
Abbreviations: mFI-5; the 5-factor modified frailty index, RAI-Rev; recalibrated version of the risk analysis index, eLOS; extended length of stay, AUC; area under the curve.
For PDF, the RAI-Rev demonstrated superior discrimination compared to mFI-5 for NHD (RAI-Rev: C-statistic = 0.70, 95% CI, 0.68-0.71 vs mFI-5: C-statistic = 0.64, 95% CI, 0.63 - 0.66). There were no significant differences between frailty indexes for mortality, CDIV complications, readmission or reoperation. Further, discriminatory accuracy was poor with all measures demonstrating a C statistic ≤0.60 for all outcomes except NHD, minor complications, CDIV complications and mortality with the posterior approach.
Discussion
In this surgical registry analysis of 18,138 cervical decompression and fusion DCM patients, increasing patient frailty was associated with nonhome discharge, extended LOS, readmission, and minor complications. In AUROC curve analysis, the RAI demonstrated superior discrimination compared to the mFI for predicting NHD (C-statistic: 0.72 vs 0.65), extended LOS (C-statistic: 0.64 vs 0.60), minor complications, and readmission. When stratified by surgical approach, the RAI-Rev was superior to the mFI-5 in predicting outcomes following ADF, while all frailty metrics demonstrated poor discrimination with PDF.
The incidence of age-related diseases, including DCM, is increasing in proportion with the increasingly aging and frail population. Surgical treatment for DCM is relatively safe with in-hospital mortality ranging from 0.03 - 1.33%; however, complication rates are as high as 14.1%.22,23 To the authors’ knowledge, this is the first study which directly analyzes the discriminatory threshold of two commonly used frailty indices in DCM patients. These findings support the RAI as the leading frailty index to aid in preoperative risk stratification of DCM patients. Furthermore, ADF for DCM patients may play a more important role in predicting surgical outcomes in increasingly frail patients, PDF may be the most risk-averse option for frail DCM patients. Adverse outcomes are expected in patients with decreased baseline physiologic reserve; however, the accurate quantification of a patient’s frailty is critical. The present findings support the RAI as the most practical frailty index, as it is used at the point of care, with the best discrimination and suggest its utility in identifying the more high-risk DCM patients for improved risk-benefit discussion preoperatively.
Frailty in spine disorders is well described within the literature; however, there are no studies which examine RAI as a measure of frailty in the context of only DCM. Wilson et al demonstrated the impact of frailty on functional and quality of life metrics following surgery in DCM patients using the 5-factor modified frailty index (mFI-5). 24 Multiple studies demonstrated the utility of the 11-factor modified frailty index (mFI-11) and mFI-5 in predicting mortality and morbidity across a host of spinal pathologies.10,11,18,25-27 For DCM specifically, studies have shown that the mFI predicts adverse outcomes better than age alone and may have clinical utility in understanding improvement in quality of life measures following surgical treatment of DCM. However, the mFI have been increasingly scrutinized in recent years for resembling comorbidity indices rather than measures of true decreased baseline physiologic reserve.14,28 The RAI has emerged as a more quantitatively robust frailty scale and has demonstrated superior outcome discrimination compared to the mFI across a range of cranial and spinal pathologies.13,17,18,29-31 The present results corroborate these findings as the RAI outperformed the mFI in predicting NHD, eLOS, minor complications and readmission following decompression and fusion in DCM patients.
In addition to consideration of a patient’s frailty status, a surgeon’s decision regarding anterior vs posterior surgery is a critical aspect of the preoperative decision-making process. ADF and PDF are performed at similar rates in DCM patients. 32 ADF is associated with decreased blood loss, shorter LOS, lower odds of infection and C5 palsy, and superior outcomes in robust patients. 33 However, ADF is associated with higher odds of dysphagia. 32 Interestingly, frailty has been investigated as a predictor of adverse outcomes in DCM, however much of the current literature focuses on ADF. Further, the few studies examining frailty in the context of PDF did not perform an analysis of discriminatory accuracy, necessary for risk stratification.8,33 One explanation for a general lack of literature on this topic may be that frailty does not effectively predict outcomes in PDF, like the results presented in this study. The present results suggest that ADF in frail DCM patients is more influential in leading to adverse postoperative outcomes. The association between dysphagia and frailty is well-established, with some studies suggesting inclusion of dysphagia in baseline frailty assessment. 34 Posterior approaches in older patients are often selected by surgeons to avoid dysphagia.35-37 Additionally, posterior approaches to decompression are associated with significantly superior neurological and clinical improvement than anterior in cervical spondylotic myelopathy.38,39 Our findings support the understanding that patient frailty is superior to patient age in predicting surgical adverse outcomes, while independently supporting the association between a posterior approach to DCM results in a lower incidence of adverse outcomes in frail patients. These results offer quantitative evidence of frailty’s greater impact on ADF outcomes for DCM patients and support the commonly observed surgeon preference of selecting posterior approaches for DCM as patient frailty increases.
Limitations
The present study utilized a large, multicenter national database, which limits the granularity of the results and relies solely on the variables coded within the NSQIP. Specifically, the NSQIP does not include variables related to preoperative cognitive status, and therefore these variables were excluded from the RAI-Rev frailty calculations. Additionally, the NSQIP does not differentiate between “poor appetite” and “weight loss,” which are both reported in the database under “WTLOSS.” These limitations are similarly reported in previous studies which show that even with variable modifications to the RAI-Rev, there is still excellent discriminative ability of these frailty measures. Finally, unlike previous studies which used conventional RAI frailty tiers (robust: 0-20; normal, 21-30; frail, 31-40; very frail, 41+), our study utilized robust ≤10, normal 11-20, frail 21-30, and very frail ≥31, as the patient cohort when utilizing 41+ for very frail was minimal. This suggests that patients undergoing decompression for DCM are not as frail as other spine surgery populations, and a larger patient cohort may be necessary to capture outcomes in very frail patients.
Conclusion
The RAI-Rev demonstrated superior discrimination for predicting NHD, eLOS, readmission, and minor complications in DCM patients undergoing decompression and fusion compared to the mFI-5. Further, the role of frailty is less pronounced with posterior approaches compared to anterior approaches for DCM, providing evidence for utilizing PDF in increasingly frail DCM patients. The RAI-Rev may aid in surgical candidate selection and inform preoperative risk stratification of these patients based on frailty strata.
Supplemental Material
Supplemental Material - Discriminatory Value of the Risk Analysis Index Versus the 5-Factor Modified Frailty Index for Major Outcome Measures in Degenerative Cervical Myelopathy
Supplemental Material for Discriminatory Value of the Risk Analysis Index Versus the 5-Factor Modified Frailty Index for Major Outcome Measures in Degenerative Cervical Myelopathy by Nithin Gupta, Sina Zoghi, Michael M. Covell, Chase Smitterberg, Stefan T. Prvulovic, William T. DiCiurcio, Johnny Delashaw, Meic H. Schmidt, Marc D. Moisi, and Christian A. Bowers in Global Spine Journal.
Footnotes
Author Contributions
Conceptualization (NKG, SZ, CAB), Methodology (NKG, SZ, CAB), Formal Analysis (SZ), Writing - Original Draft (NKG, SZ, MMC, CS, STP), Writing - Review & Editing (NKG, MMC, WTD, JD, MHS, MDM, CAB), Supervision (WTD, JD, MHS, MDM, CAB), Project Administration (MHS, MDM, CAB).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data used to produce this manuscript are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.