
Abstract
Study Design
Retrospective Cohort Study.
Objectives
This study sought to analyze predictors of delayed spine surgery and their impact on postoperative adverse outcomes.
Methods
This retrospective cohort study analyzed patients who underwent spine surgery from the National Surgical Quality Improvement Program database from 2015 to 2020. Delayed spine surgery was defined as the interval from admission to operation exceeding the 95th percentile of the total population or lasting >3 days. Multivariate regression models were used to estimate probabilities of outcomes after adjusting for individual risk factors. The primary outcome included mortality, along with secondary measures including nonroutine discharge, extended length of stay (LOS), major and minor postoperative complications, Clavien-Dindo grade IV complications (CDIV), readmission, and reoperation rates.
Results
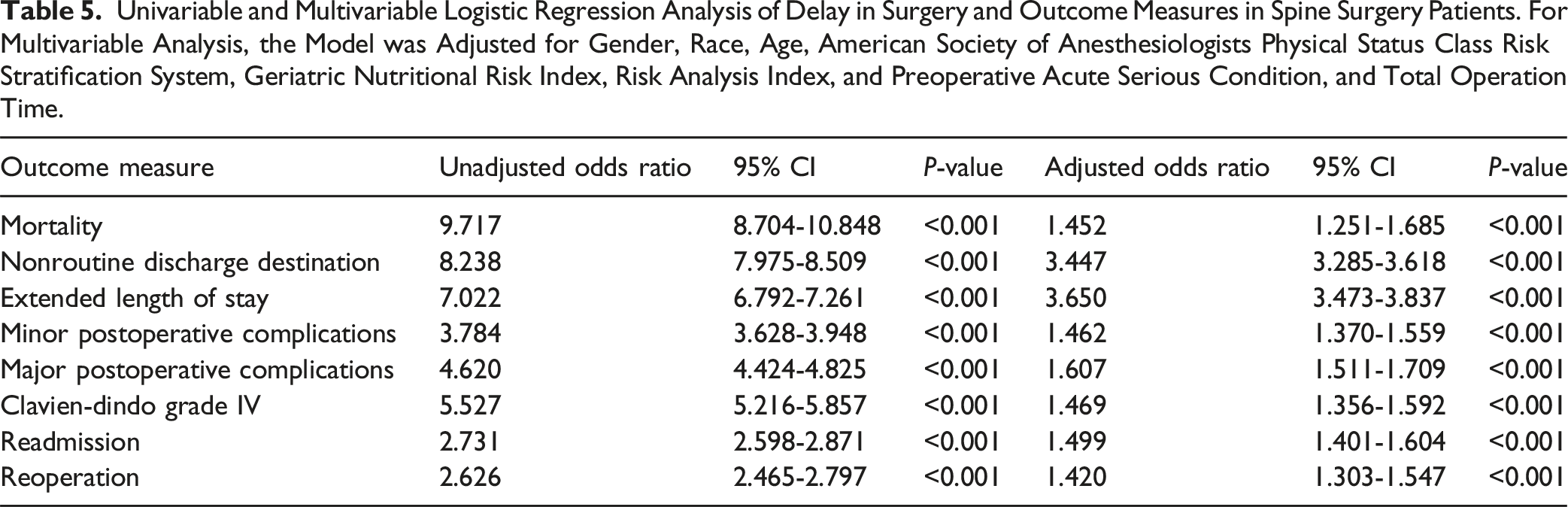
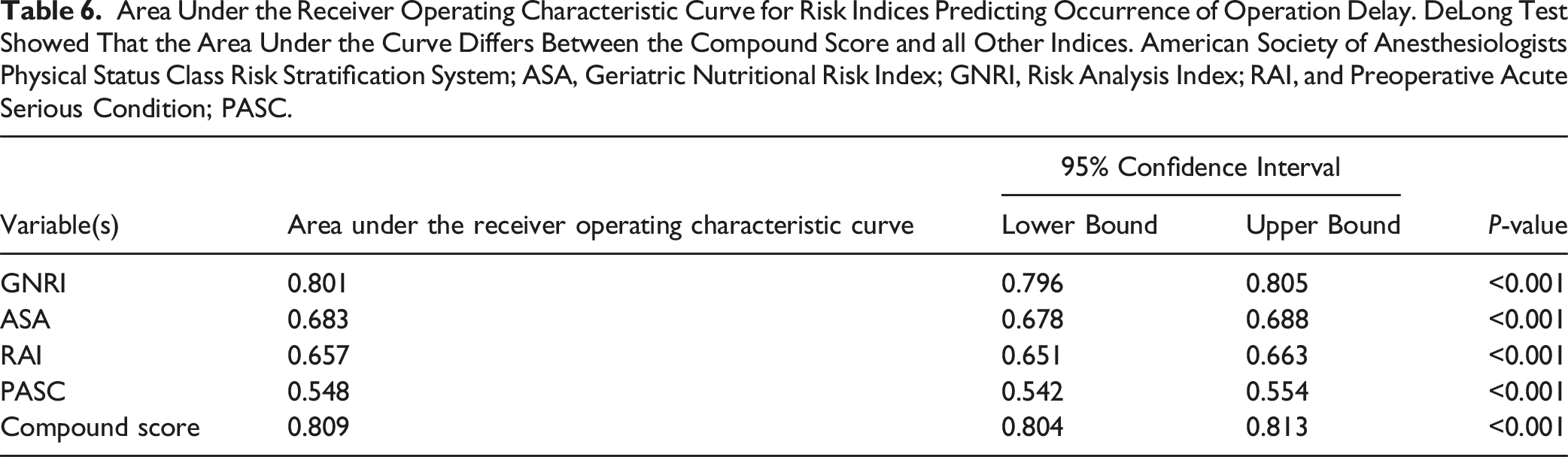
Of 362 788 patients, 16 664 (4.59%) experienced a delay in surgery. The adjusted odds ratios for outcomes predicted by delayed surgery were mortality (1.452, 1.251-1.685), nonroutine discharge destination (3.447, 3.285-3.618), extended LOS (3.650, 3.473-3.837), minor postoperative complications (1.462, 1.370-1.559), major postoperative complications (1.607, 1.511-1.709), Clavien-Dindo grade IV complications (1.469, 1.356-1.592), readmission (1.499, 1.401-1.604), and reoperation (1.420, 1.303-1.547). ROC analysis showed that GNRI has an excellent discriminative power (C-statistic = 0.801) for delayed surgery. There is little incremental gain from adding other indices including frailty and perioperative conditions and status to GNRI (C-statistic of the compound index = 0.809).
Conclusions
Pre-operative delays in spine surgery independently predict increased postoperative morbidity and mortality. Surgical delay was associated with higher GNRI. These findings highlight the importance of timely surgeries to minimize complications and reduce healthcare costs.
Keywords
Introduction
About 900 000 adults undergo spine surgery in the United States every year, with costs varying between 4500 and 30 000 USD per procedure. 1 Spine surgery contributes to over 86 billion USD of annual healthcare expenditure. 2 Previous literature on orthopedic surgery has shown that delayed surgery can amplify postoperative complication risks, augment patient distress, reduce hospital performance, and increase cost.3-5
Indeed, although many spine patients require urgent surgical intervention for their pathologies, data addressing the impact of delayed spine surgery on patient care at the population level are markedly lacking for different patient demographics and geographic areas in the US. Developing a better understanding of factors associated with delayed spine surgery could help identify targets for interventions to prevent such delays and improve the quality of care. Moreover, by specifically identifying patients at greatest risk for surgical delays and the specific reasons for these delays, patient burdens and unnecessary healthcare resource waste could be curbed. Herein, we aim to examine predictors of delayed spine surgery and its impact on postoperative outcomes after surgery.
Methods
Data Source
In this study, we utilized data from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database from 2015 to 2020. The ACS NSQIP is a validated national database with more than 700 participating hospitals, with more than 200 variables collected for the patients. ACS NSQIP data are reviewed and entered by trained reviewers ensuring consistency and reliability from the contributing institutions. 6 The present study was performed under a Health Insurance Portability and Accountability Act–-compliant Participant Use Data File and was considered exempt from our institutional review board. Given the de-identified nature of the information in the ACS NSQIP database, ethical approval from the institutional review board (IRB) was not required.
Patient Population
We used the Current Procedural Terminology (CPT) to identify patients 18 years or older in the ACS NSQIP database who had spine surgery between 2015 and 2020 including CPT 22010-22855 for spinal instrumentation and CPT 62380-63707 for spinal procedures. Patients older than 90 years of age, who had unknown discharge destination, unknown transfer status, unknown functional status, and missing outcome were excluded.
Preoperative Acute Serious Condition (PACS)
PASC was defined using 6 NSQIP Present at Time of Surgery (PATOS) variables and NSQIP variables defining preoperative acute renal failure and dialysis dependence as previously described by Yan et al.7,8 PASC can range from 0 to 8, with Increasing numbers indicating a higher number of PATOS and potentially inferior outcomes.
Risk Analysis Index (RAI)
The RAI was developed to optimize preoperative screening in patients undergoing elective surgery. 9 The RAI encompasses a diverse set of patient features and therefore can accurately capture the multidimensionality of frailty reasonably well. The variables included in RAI are patient demographics such as age and sex, history of medical comorbidities including heart failure, renal impairment, dyspnea, and cancer, nutritional status (as indicated by the weight loss), and a patient’s functional and cognitive status, reflected by their ability to live independently. RAI was developed using a sample of Veterans Affairs patients from the Veterans Affairs Surgical Quality Improvement Program and a mortality scoring model developed from nursing home patients.9,10 The RAI scoring cutoffs and variables are based on a previously reported algorithm.9 Of note, cognitive deterioration, originally coded in the RAI scoring system, was excluded in our study, due to reporting restrictions in the ACS NSQIP. Similarly, several of the ACS NSQIP variables have been phased out (eg, preoperative radiotherapy and chemotherapy) and are no longer recorded and as a result incorporated into the scoring system. It has been shown that the absence of these variables does not dramatically affect model performance.11,12 Patients in the present study were stratified into 4 frailty tiers: robust (RAI scores ≤20), normal (RAI scores 21-30), frail (RAI scores 31-40), and severely frail (RAI scores ≥41). 13
Geriatric Nutritional Risk Index (GNRI)
GNRI was developed using the ACS-NSQIP database variables, including sex, weight (kg), height (cm), and preoperative albumin level. The formula outlined by Bouillanne et al is utilized to calculate GNRI: GNRI = (1.489 × serum albumin [gram per liter]) + (41.7 × [weight/WLo]). 14 The weight/Ideal Body Weight (WLo) ratio was capped at 1 for patients with weight exceeding their ideal body weight, to avoid missing malnourished overweight/obese patients. Ideal body weight, calculated by the Devine formula: men as 50 + (0.91 × [height in centimeters −152.4]) and women as 45.5 + (0.91 × [height in centimeters −152.4]).
Population Characteristics
Baseline variables used in the present study are age, sex, BMI, hospital length of stay, and total operation time. Previous medical comorbidities including dyspnea, hypertension functional status, COPD, CHF, smoking status, DM, disseminated cancer, steroid use, weight loss, and bleeding disorders were also included and analyzed.
Surgery Delay
In the present study, surgery delay was defined using the “HtoODay” variable of the ACS NSQIP that measures the period of time elapsed from hospital admission until surgery in days. We defined surgery delay as the top 95th percentile of the longest periods of time from admission to operation. In our cohort, the cut-off for surgery delay was defined as any delay greater than 2 days.
Outcomes and Complications
Outcome measures examined in this study were 30-day mortality, occurrence of minor, major, or Clavien-Dindo grade IV (CDIV) complications, 30-day unplanned readmission, 30-day unplanned reoperation, prolonged LOS, and nonroutine discharge destination. Minor complications included Intra-/postoperative blood transfusion, renal insufficiency, or urinary tract infection, Major complications included prolonged intubation exceeding 48 hours, unplanned reintubation, sepsis, septic shock, pneumonia, deep vein thrombosis/thrombophlebitis, pulmonary embolism (PE), acute cerebrovascular accident or stroke with neurological deficit, acute renal failure, myocardial infarction (MI), cardiac arrest requiring cardiopulmonary resuscitation, superficial surgical site infection (SSI), deep incisional SSI, organ space SSI, or wound disruption. CD-IV Complications were defined as life-threatening complications resulting from dysfunction of one or more organs requiring treatment in the intensive care unit which included sepsis or septic shock, acute renal failure, PE, MI, cardiac arrest requiring cardiopulmonary resuscitation, ventilation >48 hours, and unplanned reintubation. 15 Extended LOS (eLOS) was defined as > 75th percentile hospital length of stay after surgery; in our cohort, eLOS was defined as a length of stay of at least 4 days.
Statistical Analysis
Data for non-normally distributed interval data were reported as the median interquartile range (IQR). The distribution of interval data was assessed using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to analyze non-normally distributed continuous variables, while the Chi-square test was used to analyze categorical variables. Multivariate logistic regression analyses of ASA, GNRI, and RAI and 30-day mortality were performed to obtain coefficients to develop a composite scoring index. Effect sizes for dichotomous outcomes were expressed as odds ratio (OR) with a corresponding 95% confidence interval (CI). Receiver operating characteristic (ROC) curve analysis was performed and included Area Under the ROC Curve (AUC)/C statistics calculations to assess the discriminative performance between ASA, GNRI, RAI and the novel composite score. The DeLong test was used to analyze differences in discrimination efficiency (C-statistics) of the indices. Statistical analyses were performed using Excel (Microsoft, Redmond, WA, USA), IBM SPSS Statistics 27.0 (IBM Co., Armonk, NY, USA), and STATA 12.0 (StataCorp, College Station, TX, USA). A P value <0.05 was considered statistically significant.
Results
Study Population Characteristics
The Association of Patient Demographics and Comorbidities and Delay in Surgery. COPD, Chronic Obstructive Pulmonary Disease; CHF, Congestive Heart Failure.
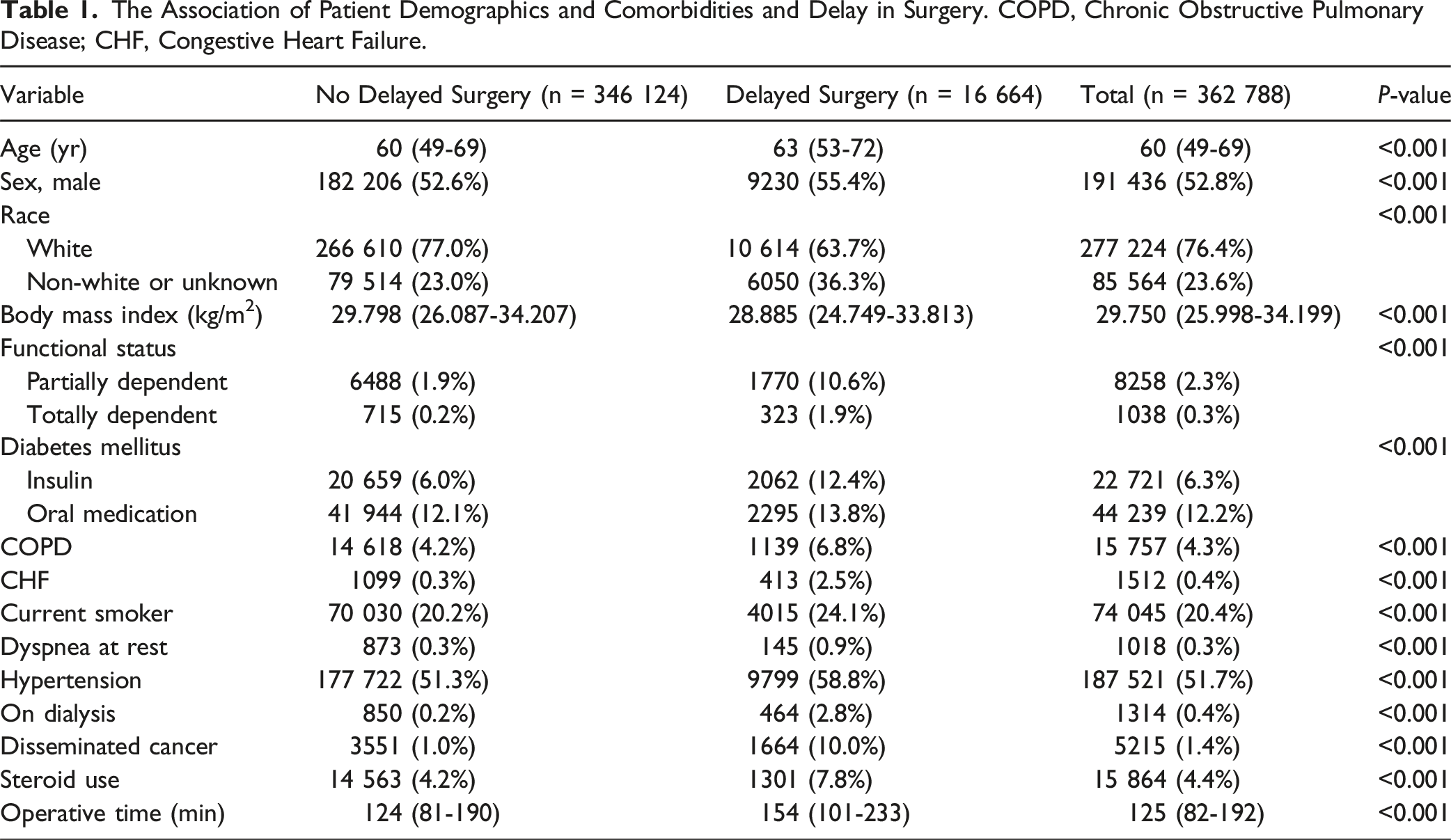
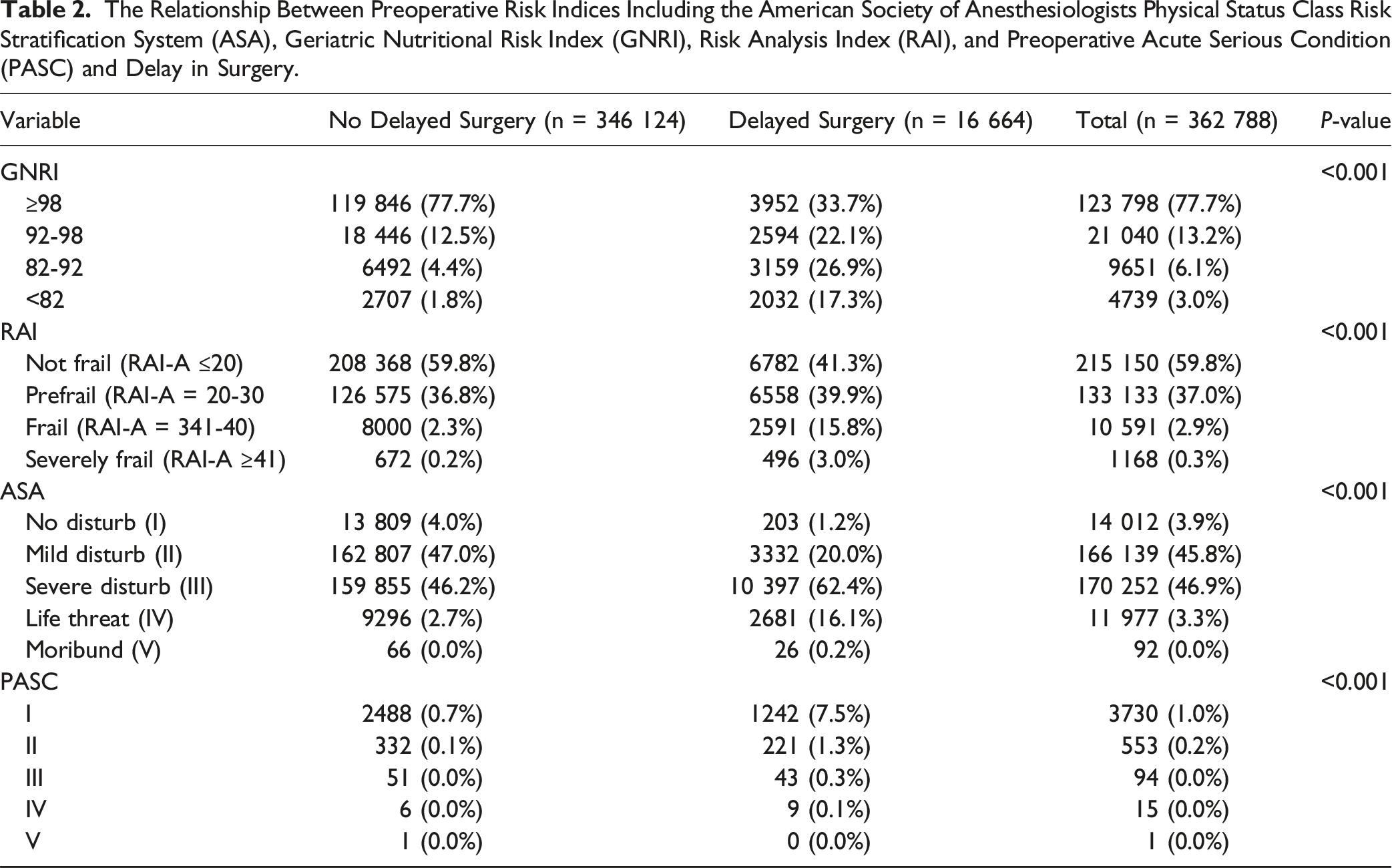
Regarding the distribution across preoperative risk assessment indices, 77% of the identified patients had a GNRI score ≥98, while only 3% of the patients had a GNRI score below 82. In a RAI frailty distribution analysis, 60% of patients were not frail, 37% of patients were prefrail, 2.9% were frail, and 0.3% were severely frail. Additionally, the majority of patients were classified as ASA stage III (46.9%) and PASC grade I (1%).
Analysis of Risk Factors
16 664 patients from our study population were reported to have delayed spine surgery. Compared to patients who had no delayed surgery, these patients were significantly older (P < 0.001) and were more likely to have predisposing comorbidities including diabetes mellitus, COPD, CHF, active smoking status, dyspnea, hypertension, disseminated cancer, steroid use, and increased operative time (P < 0.001).

The Relationship Between Preoperative Risk Indices Including the American Society of Anesthesiologists Physical Status Class Risk Stratification System (ASA), Geriatric Nutritional Risk Index (GNRI), Risk Analysis Index (RAI), and Preoperative Acute Serious Condition (PASC) and Delay in Surgery.
Multivariable Logistic Regression Analysis of Risk Indices and Operation Delay. The Odds Ratio From the Model Were Used to Compute an Novel Compound Index. American Society of Anesthesiologists Physical Status Class Risk Stratification System; ASA, Geriatric Nutritional Risk Index; GNRI, Risk Analysis Index; RAI, and Preoperative Acute Serious Condition; PASC.
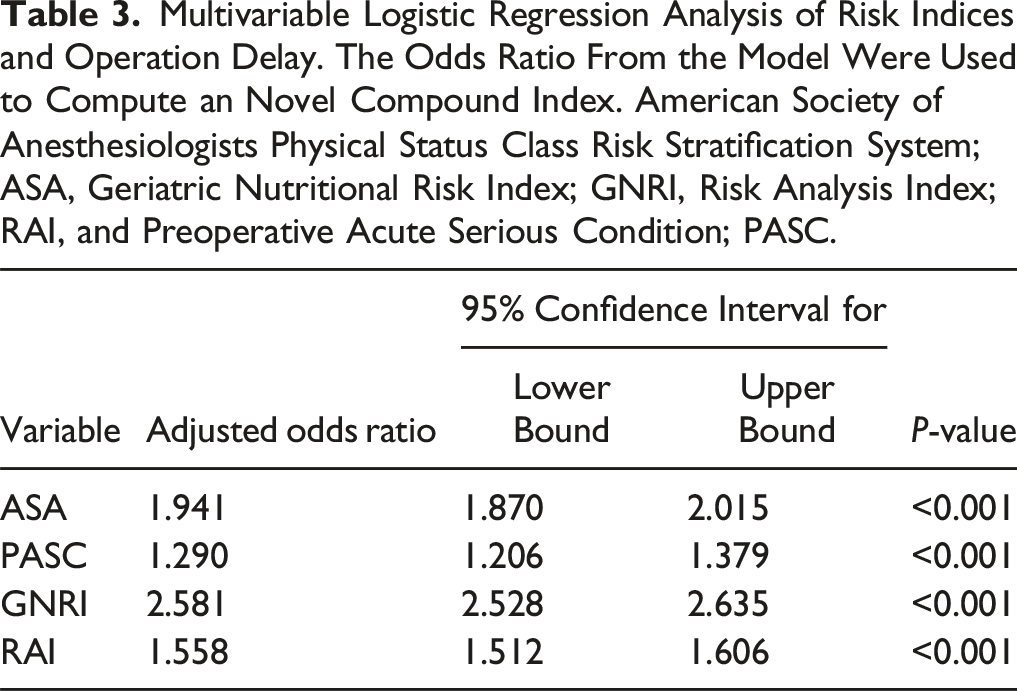
The possible scores for the CGARP index range from 8 to 38, where a score of 8 represents the lowest likelihood of operation delay, and a score of 38 indicates the highest likelihood.
Outcomes
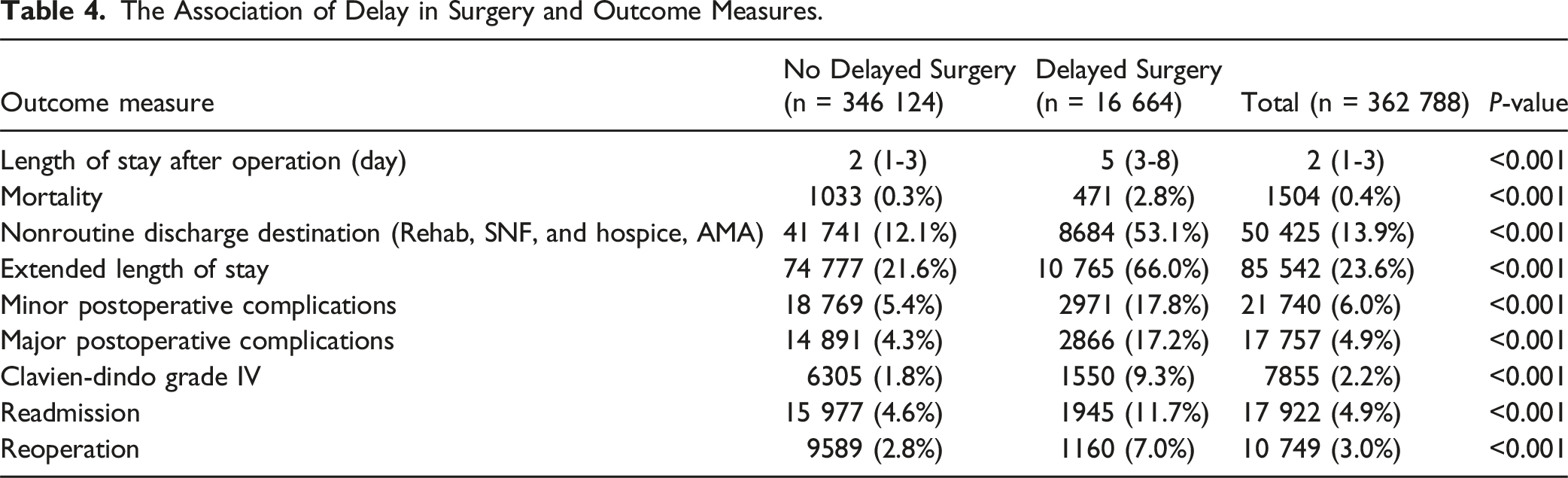
The Association of Delay in Surgery and Outcome Measures.
Univariable and Multivariable Logistic Regression Analysis of Delay in Surgery and Outcome Measures in Spine Surgery Patients. For Multivariable Analysis, the Model was Adjusted for Gender, Race, Age, American Society of Anesthesiologists Physical Status Class Risk Stratification System, Geriatric Nutritional Risk Index, Risk Analysis Index, and Preoperative Acute Serious Condition, and Total Operation Time.
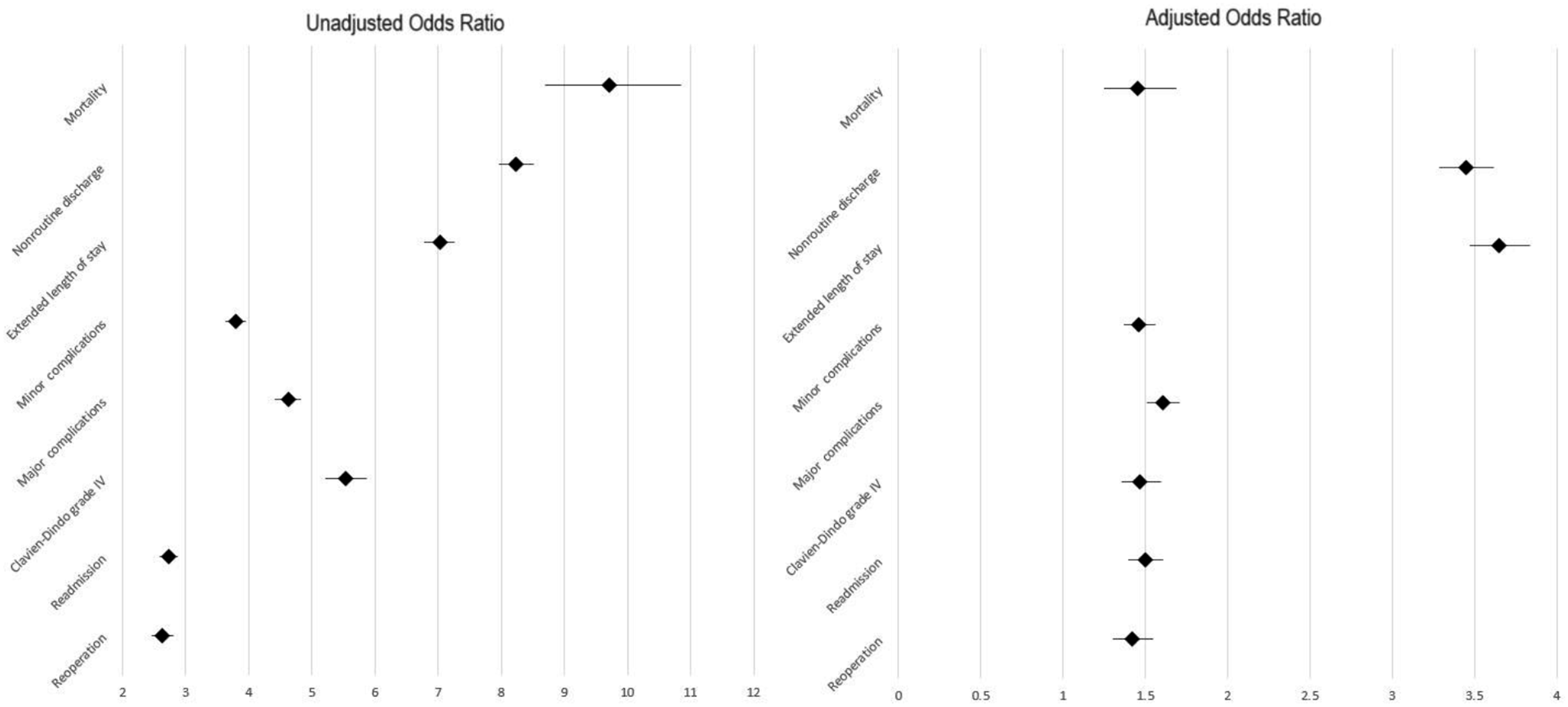
Forest plot of representation of odds ratios from Univariable and multivariable logistic regression analysis of delay in surgery and outcome measures.
ROC Curve Analysis
Area Under the Receiver Operating Characteristic Curve for Risk Indices Predicting Occurrence of Operation Delay. DeLong Test Showed That the Area Under the Curve Differs Between the Compound Score and all Other Indices. American Society of Anesthesiologists Physical Status Class Risk Stratification System; ASA, Geriatric Nutritional Risk Index; GNRI, Risk Analysis Index; RAI, and Preoperative Acute Serious Condition; PASC.
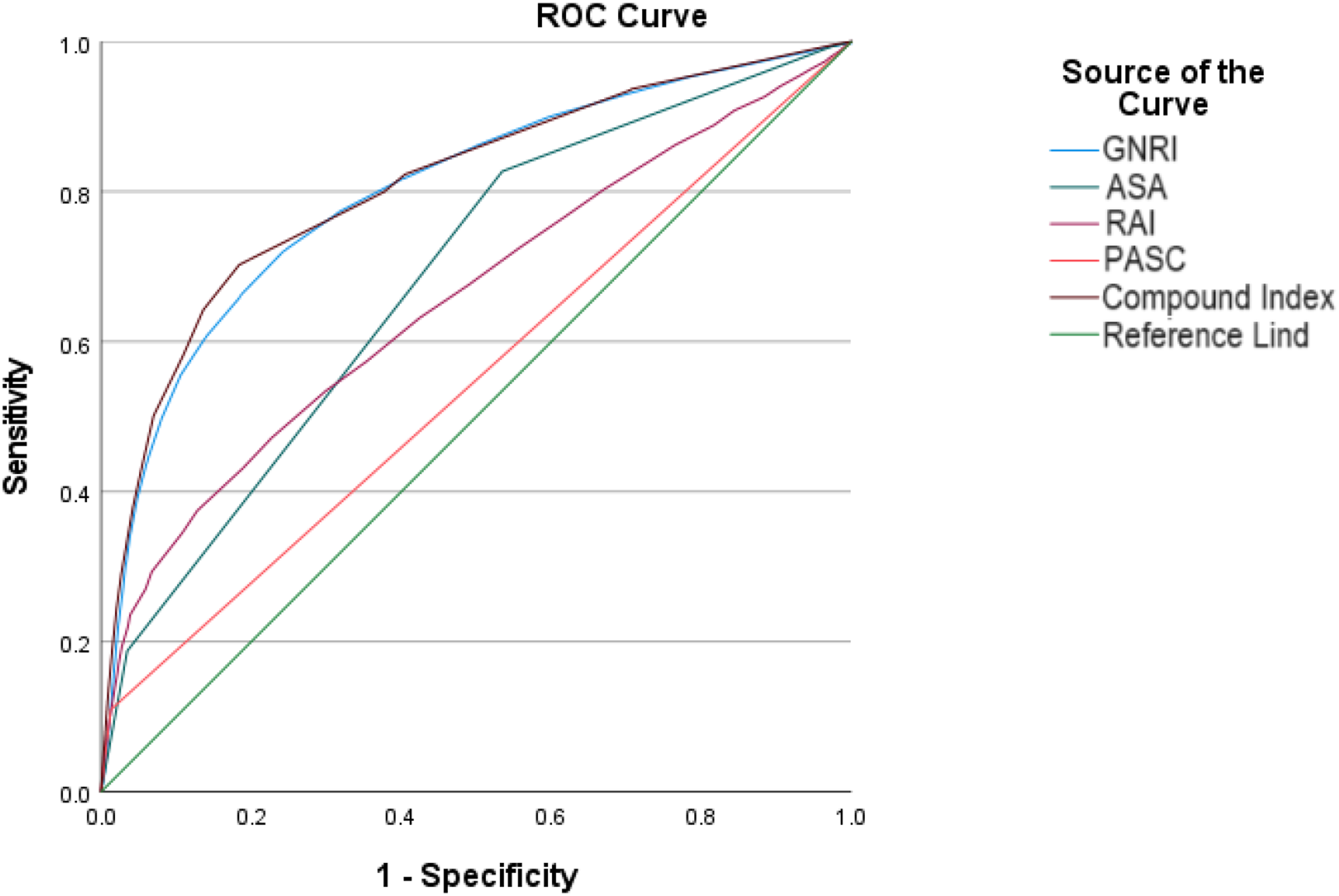
Receiver operating characteristic curve for risk indices predicting occurrence of operation delay. American Society of Anesthesiologists physical status class risk stratification system; ASA, Geriatric Nutritional Risk Index; GNRI, Risk Analysis Index; RAI, and Preoperative Acute Serious Condition; PASC.
Discussion
Our study analyzed data from 362 788 patients undergoing spinal surgical operations, focusing on the association between preoperative risk indices and delayed surgery outcomes. The population was predominantly older, white, and male, with a median age of 60 years and a significant prevalence of comorbidities, such as hypertension and diabetes mellitus.
Our analysis revealed that patients with delayed surgery were significantly older and had a higher incidence of comorbidities, including diabetes mellitus, COPD, and congestive heart failure, among others. These patients were also associated with worse outcomes, including extended length of stay, higher mortality rates, and increased rates of postoperative complications, readmission, and reoperation. The novel CGARP index, developed from the multivariable analysis, demonstrated superior predictive performance for delayed surgery compared to traditional indices like GNRI, ASA, RAI, and PASC, as evidenced by its higher C-statistic of 0.809. These findings underscore the importance of comprehensive preoperative risk assessment and the potential utility of the CGARP index in predicting surgical delays and improving patient outcomes.
Delays in spine surgery have been linked to worse postoperative outcomes and higher healthcare costs.16-19 However, there is a lack of literature on the burden of delayed spine surgery specifically across various demographics nationwide. Identification of which patients are likely to experience delay in surgery may help alleviate patient burden and unnecessary healthcare resource use.
Patients who were non-white were prone to surgical delay, with 36.3% non-white or of unknown race in the delayed group, and 23.6% in the non-delayed group. There are plausible explanations for the link between race and surgical delay that take root in socioeconomic factors. Obtaining timely access to care for non-white patients likely reflects disparities in access to care, insurance, income, and health literacy, all of which could, in turn, delay preoperative workups and surgery. Differences in the frequency of comorbidities between racial and ethnic groups could also explain some of the increased likelihood of surgical delay. Conditions such as diabetes and hypertension are more common in non-white patients, and their preoperative management could benefit from more careful approaches moving forward.20-27
In addition to race, comorbidities were correlated with delayed surgery. Each additional comorbidity raised both the odds of an operation occurring 7 days after or after surgery at 30 days; the effect remained significant (P < 0.001 in both comparisons) after adjusting for the general surgical score. Individuals with high scores on the American Society of Anesthesiologists (ASA) scale, or more severe systemic disease, had higher likelihoods of delayed surgery. In particular, patients undergoing delayed surgery accounted for 62.4% of those with an ASA III (severe systemic disease) score, compared with 46.9% in the control non-delayed group. Other comorbidities present in higher proportions among individuals experiencing delayed operations included diabetes, COPD, and CHF, which parallel other studies in the literature calling for greater attempts at preoperative screening, optimization, or stabilization.28-37 Individuals with disseminated cancer were also far more likely to undergo delayed surgery, reflecting the need for more intensive multidisciplinary care or simply stronger optimization for these conditions before, during, and after surgery.38,39
Nutritional status, measured using GNRI, was also a major determinant of delayed spine surgery. PASC, GNRI, and RAI had AORs of 1.290, 2.581, and 1.558 and AUCs of 0.683, 0.657, and 0.548, respectively. The compound score of 0.809 AUC outperformed all other models individually. Moreover, patients with a lower GNRI, which indicates a higher nutritional risk, were more likely to have their operations delayed with a 2.581 AOR and 0.801 AUC. Indeed, malnutrition increases the postoperative risk of morbidity and mortality. Previous studies have found that better pre-surgical patient nutrition status is associated with significant medical complications, wound dehiscence, infection, and even mortality.40-42 Importantly, the degree of the association between GNRI scores and delayed surgery is strong. This likely relates to the need to correct nutritional deficits in the preoperative period to minimize delays in surgery.
Another significant determinant of delayed operation was functional status. Patients who were partially or totally dependent were more likely to suffer a delay. For example, 10.6% of patients with delayed surgery were partially dependent, compared with 1.9% in the non-delayed group; 1.9% of patients who underwent delayed surgery were totally dependent, compared with 0.2% in the non-delayed group. Such dependence on external help with daily living often adds to the preoperative assessment and planning that is needed for perioperative care, which leads to delays.43,44 Also, patients with acute serious conditions, assessed by the Preoperative Acute Serious Condition (PASC) score, were at greater risk for delayed surgery. Whereas 7.5% of the patients with delayed surgery had a PASC score of I compared with 0.7% of the non-delayed, PASC scores were inversely associated with mortality. Acute serious conditions often call for urgent stabilization and robust preoperative work-up before the patient is ready for surgery, leading to surgery delays due to the need for multidisciplinary input and preoperative planning.
Delayed surgery was associated with inferior postoperative outcomes at each phase of hospitalization. Postoperative mortality was higher in patients who underwent delayed surgery (2.8% vs 0.3%), nonroutine discharge was more common (53.1% vs 12.1%), and lengths of stay were longer (66.0% vs 21.6%). Also, delayed surgery was associated with a higher overall incidence of postoperative complications, both minor (17.8% vs 5.4%) and major (17.2% vs 4.3%), and Clavien-Dindo grade IV complications were more common with delayed surgery (9.3% vs 1.8%). Rates of readmission were higher with delayed surgery (11.7% vs 4.6%), as were reoperation rates (7.0% vs 2.8%).
Interestingly, mortality had a 9.717 unadjusted odds ratio, but even after adjustment, aOR was found to be relatively high at 1.452. Similar or even higher aORs were found across minor and major postoperative complications, Clavien-Dindo grade IV, readmission, and reoperation categories, even though the unadjusted odds ratios were even lower than mortality. For instance, readmission had a low unadjusted odds ratio in comparison with mortality, at 2.731, but its AOR was higher than mortality at 1.499. Even more pronounced trends occurred with rates of non-routine discharge destination and extended length of stay, with unadjusted odds ratios of 8.238 and 7.022, and adjusted odds ratios of 3.447 and 3.650, respectively. The fact that surgical delay is still strongly correlated with the outcomes and AORs remain relatively large even after adjusting for these variables demonstrates the importance of timely spine surgery care for patients of all backgrounds. This longitudinal description of surgical outcomes illustrates the cascade of adverse events that patients undergoing operations experience due to surgical delays, potentially helping inform new guidelines on minimum clinical thresholds, maximum delay times, and other aspects to refine the care pathway for these spine patients.
Even more pronounced trends occurred with rates of non-routine discharge destination and extended length of stay, with unadjusted odds ratios of 8.238 and 7.022, and adjusted odds ratios of 3.447 and 3.650, respectively. The fact that surgical delay is still strongly correlated with the outcomes and aORs remain relatively large even after adjusting for these variables demonstrates the importance of timely spine surgery care for patients of all backgrounds. This longitudinal description of surgical outcomes illustrates the cascade of adverse events that patients undergoing operations experience due to surgical delays, potentially helping inform new guidelines on minimum clinical thresholds, maximum delay times, and other aspects to refine the care pathway for these spine patients.
Limitations
The present study has several limitations despite efforts to address them. As a retrospective study, there is potential for subjective biases, which may lead to inaccurate data entries or inconsistencies in the study parameters. Additionally, the use of a large national database may overlook specific protocols or practices unique to individual institutions, especially in terms of assessing frailty indices, which could influence the outcomes on an individual scale. Furthermore, no single tool can comprehensively capture all nuances of frailty and nutritional status. While many indices focus on functional ability, cognition, and exposure to risk factors that predict increased mortality and morbidity, they primarily assess frailty based on physical performance and health deficits. In the context of spine surgery, variations in institutional practices regarding surgical timing and postoperative care are not fully accounted for in this analysis, making the need for further studies inevitable.
Conclusion
In sum, delayed spine surgery is closely associated with older age, male sex, non-white race, and the presence of multimorbidity. Nutritional status and functional dependence, in particular, coupled with acute serious conditions, contribute to the likelihood of surgical delay. These often occur in the context of worsening clinical stability and thus carry significant adverse effects on postoperative outcomes, including higher rates of mortality, increased complications, prolonged length of stay, and higher rates of readmission and reoperation. There is a need to address the predictors of delayed surgery with perioperative optimization so that outcomes of care can be improved and allied healthcare costs reduced. Efforts to minimize surgical delay for spine surgery patients are of prime importance and should ideally commence from patient selection to when the patient undergoes surgery and considered after the surgery.
Footnotes
Author Note
Previous Presentations: 2024 CNS Annual Meeting.
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data was obtained through the ACS-NSQIP database and is used with the permission of The American College of Surgeons.