
Abstract
Study Design
Retrospective cohort study.
Objective
To describe the clinical characteristics and surgical outcomes of non-ambulatory patients with thoracic ossification of the posterior longitudinal ligament (T-OPLL), and to identify predictors of independent walking recovery.
Methods
This retrospective study analyzed 70 non-ambulatory T-OPLL patients treated with either circumferential decompression (CD) or posterior decompression with fusion (PDF) surgery at a single center over 10 years (2012-2022). Outcomes included neurological recovery rate, independent walking recovery, and complications.
Results
Overall, 71.4% of patients regained independent walking. The CD group showed superior functional outcomes (90% vs 64% walking recovery, P = 0.030) but higher complication rates (70% vs 38% CSF leakage, P = 0.015). Shorter disease duration (P = 0.018) and lower BMI (P = 0.027) independently predicted better walking recovery.
Conclusions
For non-ambulatory T-OPLL patients, CD surgery provides better functional recovery while PDF surgery offers a safer alternative. Early surgical intervention and individualized approach selection based on disease duration and BMI are critical for optimizing outcomes.
Keywords
Introduction
Thoracic ossification of the posterior longitudinal ligament (T-OPLL) is a progressive spinal disorder that frequently leads to severe myelopathy, resulting in debilitating outcomes such as loss of ambulation, sphincter dysfunction, and permanent neurological deficits.1,2 Epidemiological studies indicated that over 60% of patients with symptomatic T-OPLL experienced gait disturbances before surgical intervention, 3 underscoring the disease’s profound impact on quality of life.
Surgical decompression remains the primary treatment to halt neurological deterioration. The optimal approach, however, remains controversial. Posterior decompression with fusion (PDF) surgery offers a less invasive option but may provide incomplete relief for severe ventral compression. In contrast, circumferential decompression (CD) surgery achieves more extensive decompression through a posterior approach but carries higher risks, including cerebrospinal fluid (CSF) leakage (reported in up to 40% of cases 4 ) and transient neurological deterioration.4,5 This dichotomy underscores the need for an evidence-based framework to balance efficacy and safety.
Current literature predominantly focuses on ambulatory patients,5-7 leaving non-ambulatory patients who represent the most severe disease spectrum understudied. Recently, Aizawa et al. 8 reviewed nine non-ambulatory patients with thoracic OPLL and reported a neurological recovery rate of 71.3% among six patients who underwent anterior decompression via a posterior approach, offering a highly encouraging perspective. However, larger studies evaluating long-term surgical outcomes, risk-benefit trade-offs between PDF and CD surgeries, and predictors of recovery are lacking. To address these gaps, we conducted a retrospective analysis of 70 non-ambulatory T-OPLL patients treated at a high-volume center over a 10-year period (2012-2022). Our study aimed to describe the clinical characteristics and surgical outcomes of non-ambulatory patients with T-OPLL, and to identify predictors of independent walking recovery.
Materials and Methods
Study Design and Patients Recruitment
This retrospective study reviewed patients with thoracic spinal stenosis (TSS) treated at our center between July 2012 and November 2022. Our study was conducted according to the principles of the Declaration of Helsinki. 9 The inclusion criteria were as follows: (1) patients aged 18 years or older; (2) loss of walking ability due to thoracic OPLL; (3) complete clinical records, operative information, and imaging data; and (4) a minimum follow-up period of two years. Patients were excluded if they: (1) had thoracic myelopathy caused solely by other etiologies such as ossification of the ligamentum flavum (OLF), thoracic disc herniation, tumors, infections, or trauma; (2) presented symptoms and signs of coexisting cervical or lumbar degenerative diseases, confirmed by according radiological examinations. For patients presenting with concurrent OPLL and OLF, we specifically included only those where OPLL represented the dominant compressive pathology. Each case underwent thorough evaluation by our multidisciplinary team upon admission.
During the study period, our team performed surgery on 457 cases of TSS. Among these, 166 patients were non-ambulatory before surgery, and 74 were diagnosed with thoracic OPLL. Four patients were lost to follow-up, leaving 70 patients who met the inclusion criteria for the final analysis.
Data Collection and Study Outcomes
Patients' demographics, imaging features, and surgical outcomes were collected. Key demographic and clinical data included age, gender, body mass index (BMI), comorbidities (hypertension, diabetes mellitus). Imaging data were re-evaluated to confirm the diagnosis and identify the segments of OPLL. Surgical details such as the surgical approaches (CD or PDF), Number of decompressed segments, single segment estimated blood loss and single segment operation time were documented. Complications including perioperative and late complications were also recorded.
Primary outcomes were neurological recovery and independent walking recovery; secondary outcomes were complications. Neurological function was evaluated using the modified Japanese Orthopaedic Association (mJOA) score for thoracic myelopathy (range: 0 – 11). 10 The mJOA recovery rate was calculated using Hirabayashi’s formula: mJOA recovery rate (%) = (postoperative mJOA score– preoperative mJOA score) x100 / (11– preoperative mJOA score).10,11 Walking ability was assessed using the lower extremity motor function score from the mJOA scale, with a score of ≥ 3 indicating independent walking.
Radiological parameters to measure
The following radiological parameters were measured: • Thoracic kyphosis (TK) angle: Measured using the Cobb method on lateral radiographs from T4 to T12. • T-OPLL decompressed segments distribution: Classified as upper (T1-4), middle (T5-8), or lower (T9-12) thoracic spine. • T-OPLL configuration type: Categorized into flat or beak types based on Matsuyama et al.'s criteria.
10
• High-intensity area (HIA) on T2-weighted imaging (T2WI): Assessed via Magnetic resonance imaging (MRI). • Dura ossification: Evaluated by double-layer sign on axial bone window of computed tomography (CT) images.
Surgical Techniques
All surgeries were performed by the same surgical team. Surgical levels for fusion and decompression were determined based on a comprehensive assessment of preoperative symptoms, clinical signs, and imaging findings. Patients were placed in the prone position under general anesthesia. PDF surgery was achieved via laminectomy, with the lateral extent limited to the medial wall of the pedicles. The CD technique has been described in detail in our previous publications.
12
Intraoperative ultrasound was routinely employed to assess anterior spinal cord compression.
13
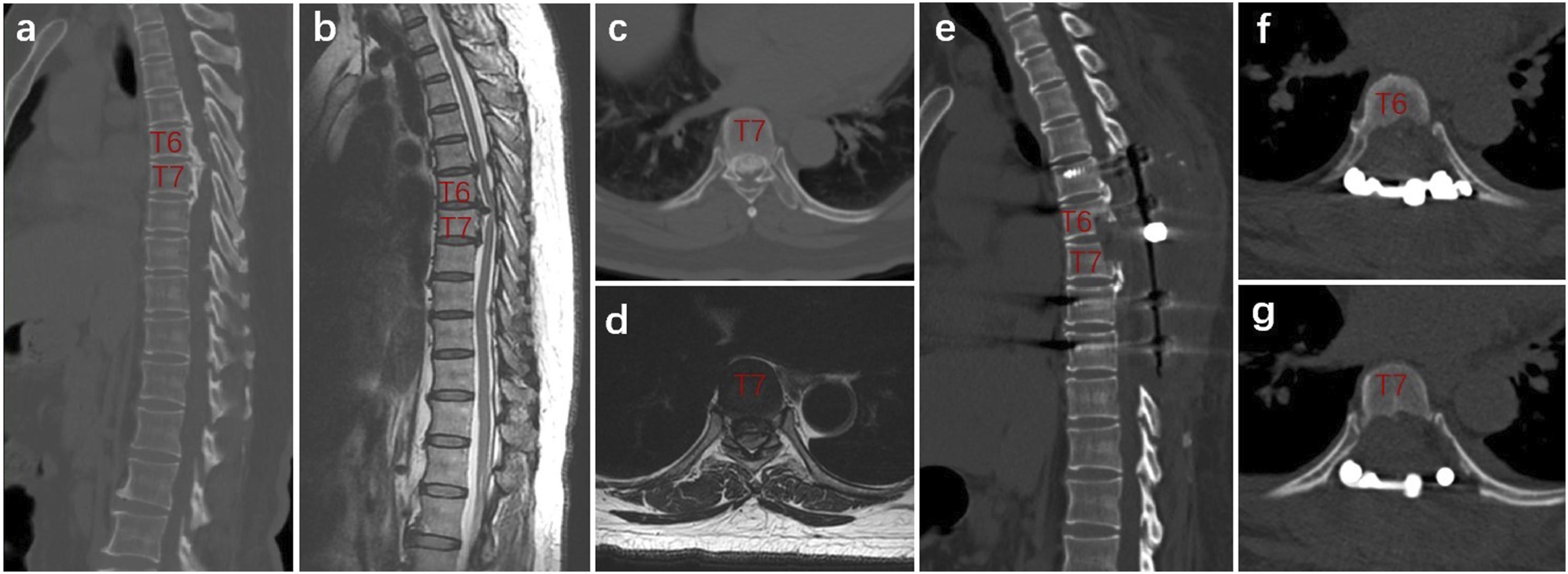
Whether selecting further CD mainly depended on the decompression adequacy, which was confirmed by observation of refilling and pulsating of the dura sac, feeling its tension manually, or real-time intraoperative ultrasound to detect the backward shift of the spinal cord and the space between OPLL and the dura sac. If there was suspicion or evidence of the remaining anterior compression, we proceeded with CD via a posterior transpedicular approach for these levels. In brief, the bilateral cancellous bone of one-third of the posterior vertebra was removed using a high-speed drill to create a ventral osseous cavity in the OPLL. The posterior vertebral cortex and OPLL were then carefully depressed and resected, achieving complete ventral decompression. However, if sufficient posterior shift and restoration of the spinal cord configuration were achieved, anterior manipulations were deemed unnecessary. A schematic diagram of transpedicular circumferential decompression via posterior approach was presented in Figure 1. Illustrative case was shown in Figure 2. Schematic Diagram of Transpedicular Circumferential Decompression (CD) via Posterior Approach. (a) A Beak Type Thoracic Ossification of Posterior Longitudinal Ligament (T-OPLL) Lesion; (b) Laminectomy were Firstly Made with High Speed Drill or Ultrasonic Scalpel; (c) The Bilateral Residual Facets and Pedicles were Resected; (d) A “culvert” is Made by Removing the Posterior Third of the Vertebral Cancellous Bone, and the OPLL Lesion is Pushed into the “Culvert”; (e) Complete CD was Realized Illustrative Case. A 59-Year-Old Female Patient was Admitted to Our Hospital with a Chief Complaint of Weakness in Both Lower Limbs for Over a Year and Non-Ambulatory Status for 1 Month. (a) Preoperative Sagittal CT Scan Showed a Beak Type Ossification of Posterior Longitudinal Ligament (OPLL) at T6-7 level; (b) Sagittal T2‐Weighted MRI Showed Significant Cord Compression at T5-8 levels; (c, d) Preoperative Axial CT and MRI Scan Showed Significant Compression by OPLL at the T7 Level, with a Spinal Canal Occupancy Rate Exceeding 50%;(e) Postoperative Sagittal CT at 3-Month Follow-Up Revealed T5-9 Laminectomy and Removal of T6-7 OPLL Lesion; (f, g) Postoperative Axial CT at 3-month Follow-Up Showed a Complete Resection of the OPLL at T6-7. One Year After Surgery, the Patient Regained Independent Walking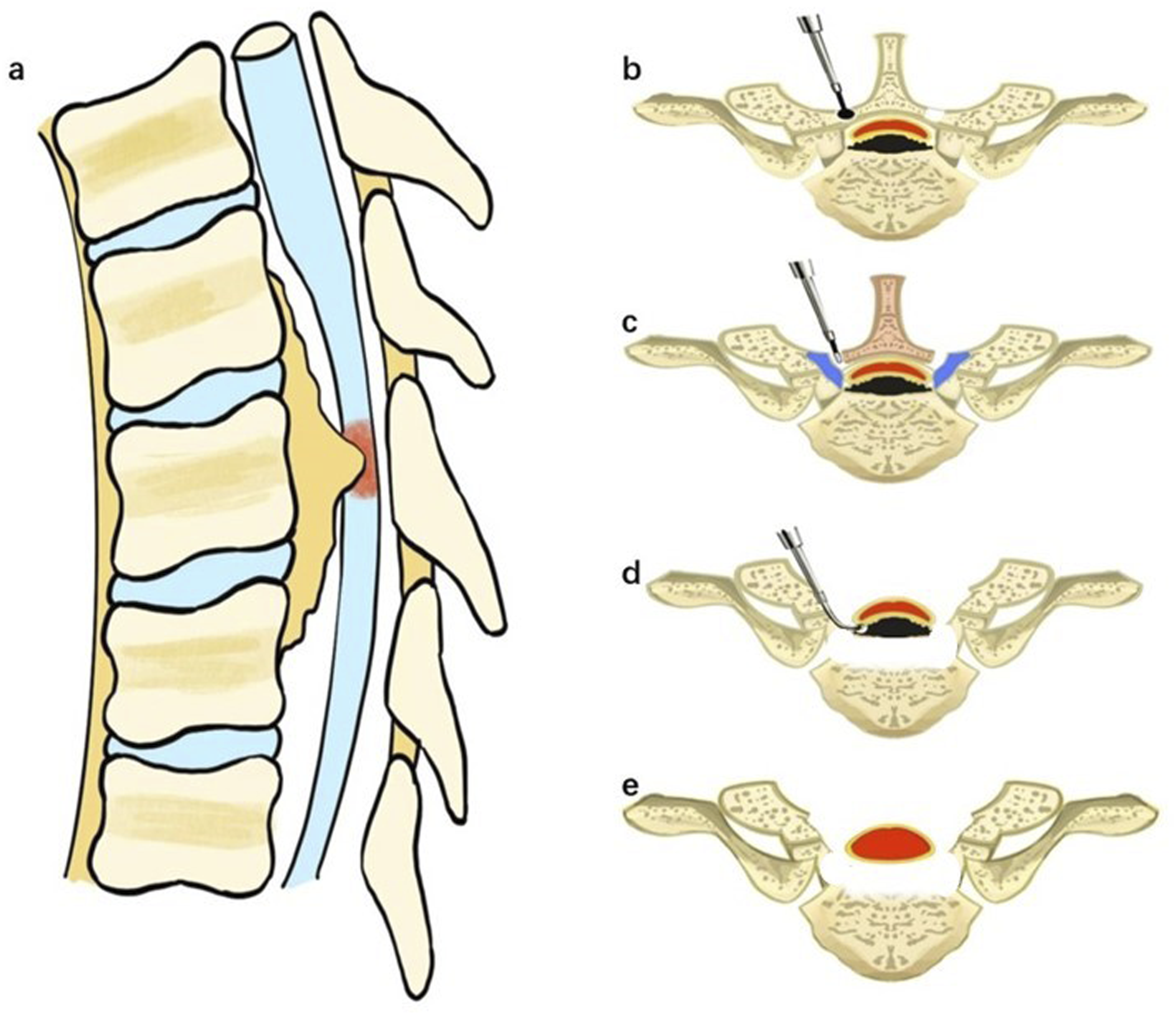
Statistical Analysis
IBM SPSS Statistics for Windows Version 27.0 (IBM Corp, Armonk, New York, USA) was utilized to process statistical analysis. Normal distribution of the data was assessed by Shapiro-Wilk test. The results were presented in the forms of mean ± standard deviation (SD) and median (Q1, Q3), accordingly. Unpaired Student t test and nonparametric Mann-Whitney U tests were used for continuous variables. Chi-square test or Fisher exact tests were used to compare categorical variables. Univariate logistic regression analyses were used to screen risk factors affecting the postoperative independent walking, and variables with P value < 0.1 were included in the multivariate logistical regression analysis, in order to determine independent factors affecting postoperative independent walking ability. Odds ratios (OR) and 95% confidence intervals (CI) were estimated for significant factors. Statistical significance was set at 0.05.
Results
Demographic and Clinical Characteristics
Demographic and Clinical Characteristics of the Cohort (N = 70)
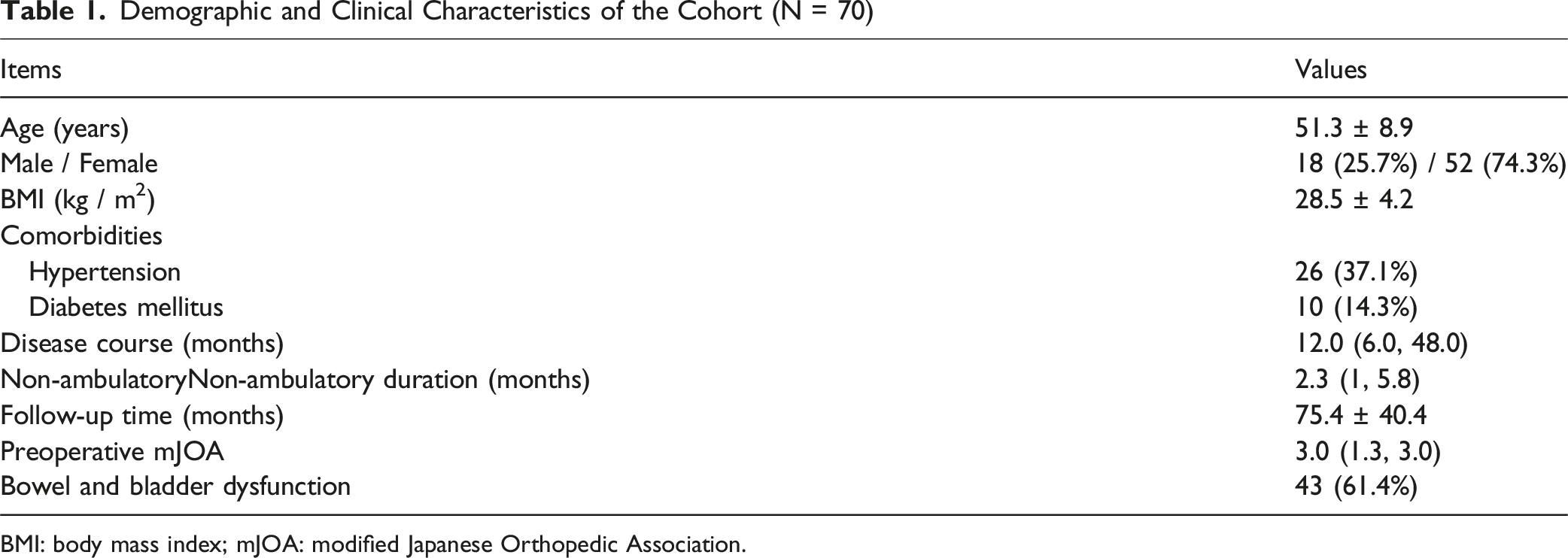
BMI: body mass index; mJOA: modified Japanese Orthopedic Association.
Imaging Measurements
Imaging Features of the Cohort (N = 70)
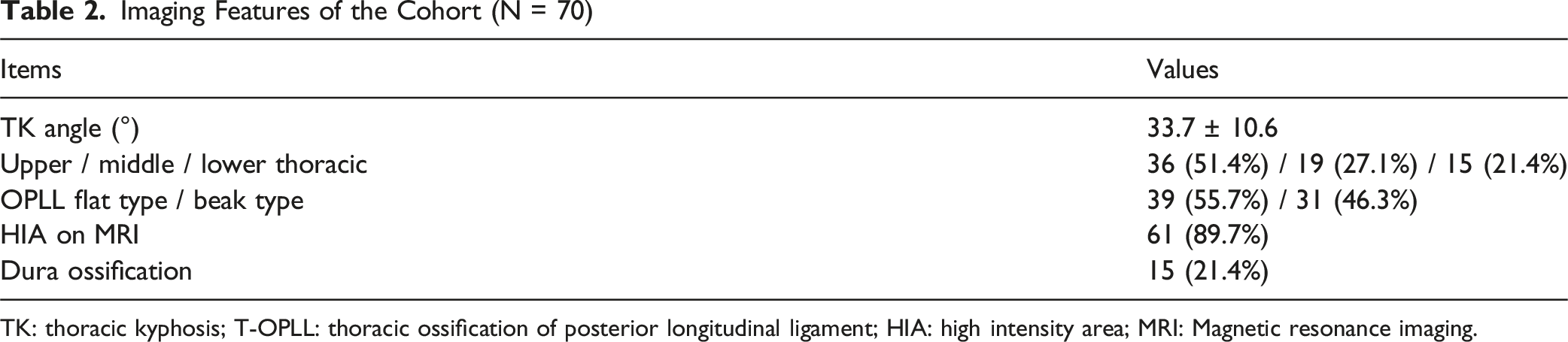
TK: thoracic kyphosis; T-OPLL: thoracic ossification of posterior longitudinal ligament; HIA: high intensity area; MRI: Magnetic resonance imaging.
Surgical-Related Data and Complications by Approach
A total of 50 patients underwent PDF surgery, while 20 patients received CD surgery performed via a posterior approach in our cohort. The median single segment operation time was 28.6 (22.4, 39.1) minutes, and the median single segment estimated blood loss was 100.0 (60.0, 133.3) ml.
A total of 63 surgical related complications were observed in 44 patients (62.9%). CSF leakage was the most common complication, occurring in 33 patients (47.1%). Transient neurological deterioration was noted in 16 patients (22.9%) and resolved within three months postoperatively under conservative management. Two patients developed epidural hematomas and one experienced complete lower limb paralysis and sphincter dysfunction. Following ultrasound-guided CSF aspiration, the patient’s muscle strength gradually improved, and independent walking was achieved three months postoperatively. Additionally, one patient sustained a postoperative vertebral fracture requiring revision surgery.
Surgery-Related Complications
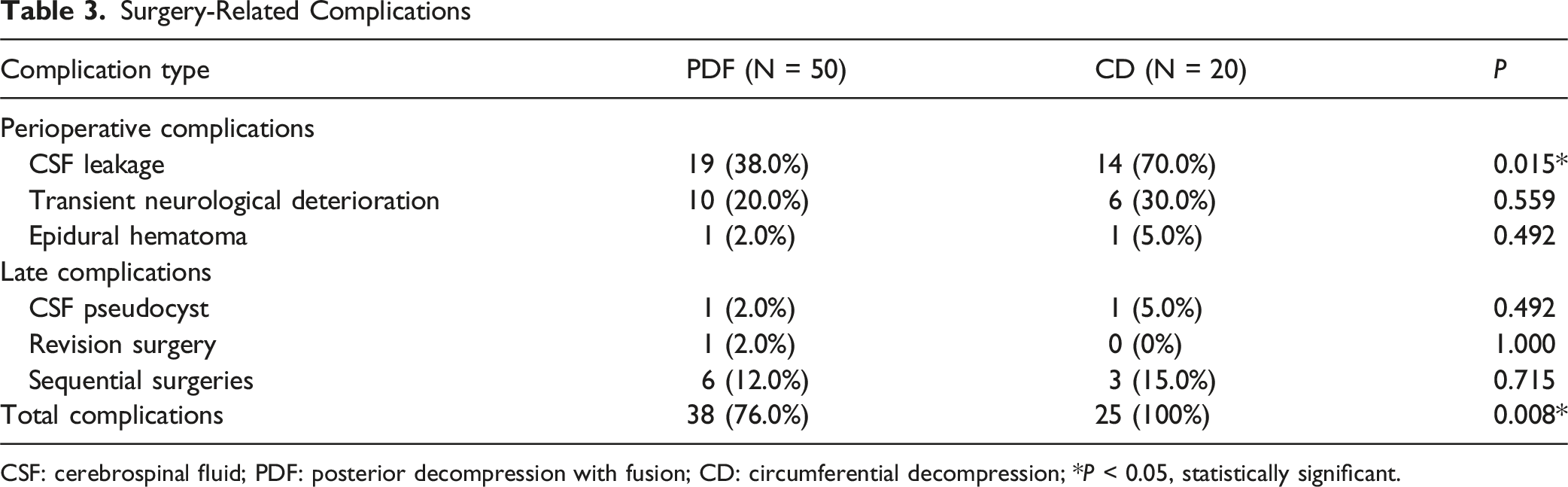
CSF: cerebrospinal fluid; PDF: posterior decompression with fusion; CD: circumferential decompression; *P < 0.05, statistically significant.
Neurological Recovery
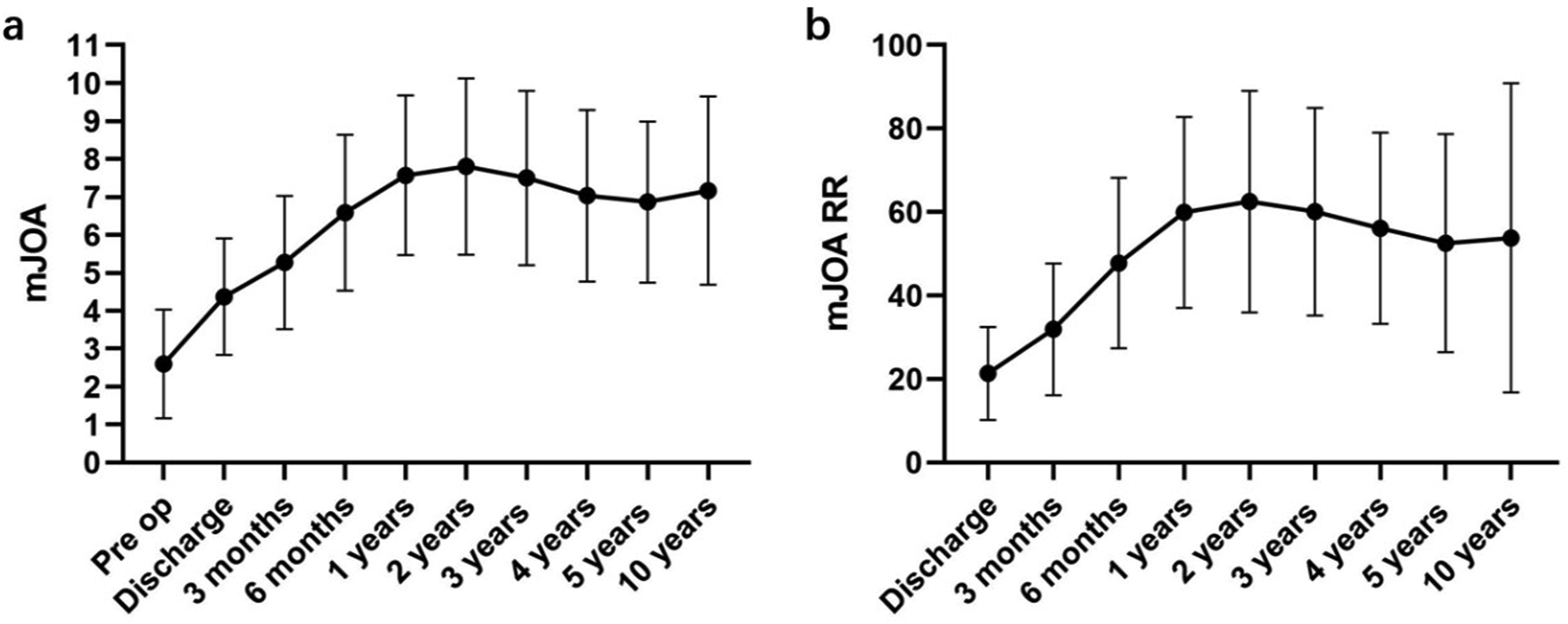
The median mJOA score significantly improved from 3.0 (1.3, 3.0) preoperatively to 4.0 (3.0, 5.0) at discharge (P < 0.001), and further to 8.0 (7.0, 9.8) at the final follow-up (P < 0.001) (Figure 3). The median recovery rate at the final follow-up was 62.5% (43.3%, 82.5%). By the final follow-up, only 5 patients had not regained motor function, while 50 out of the remaining 65 patients (71.4%) had regained the ability to walk independently. By reviewing outpatient medical records, we conducted an analysis of the patient’s neurological recovery rate and discovered a meaningful phenomenon that patients experienced continuous neurological improvement in the first two years after surgery and remained stable thereafter (Figure 4). Comparison of mJOA Between PDF and CD Groups. mJOA: Modified Japanese Orthopedic Association; PDF: Posterior Decompression with Fusion; CD: Circumferential Decompression; * Represented P < 0.05 Between the Two Groups The mJOA (a) and Neurological Recovery Rate (b) Changes at Different Stages. Pre op: Preoperative; mJOA: Modified Japanese Orthopedic Association; RR: Recovery Rate. (a and b) Represented mJOA Scores and Neurological Recovery Rate Changes Within Ten Years Postoperatively, Respectively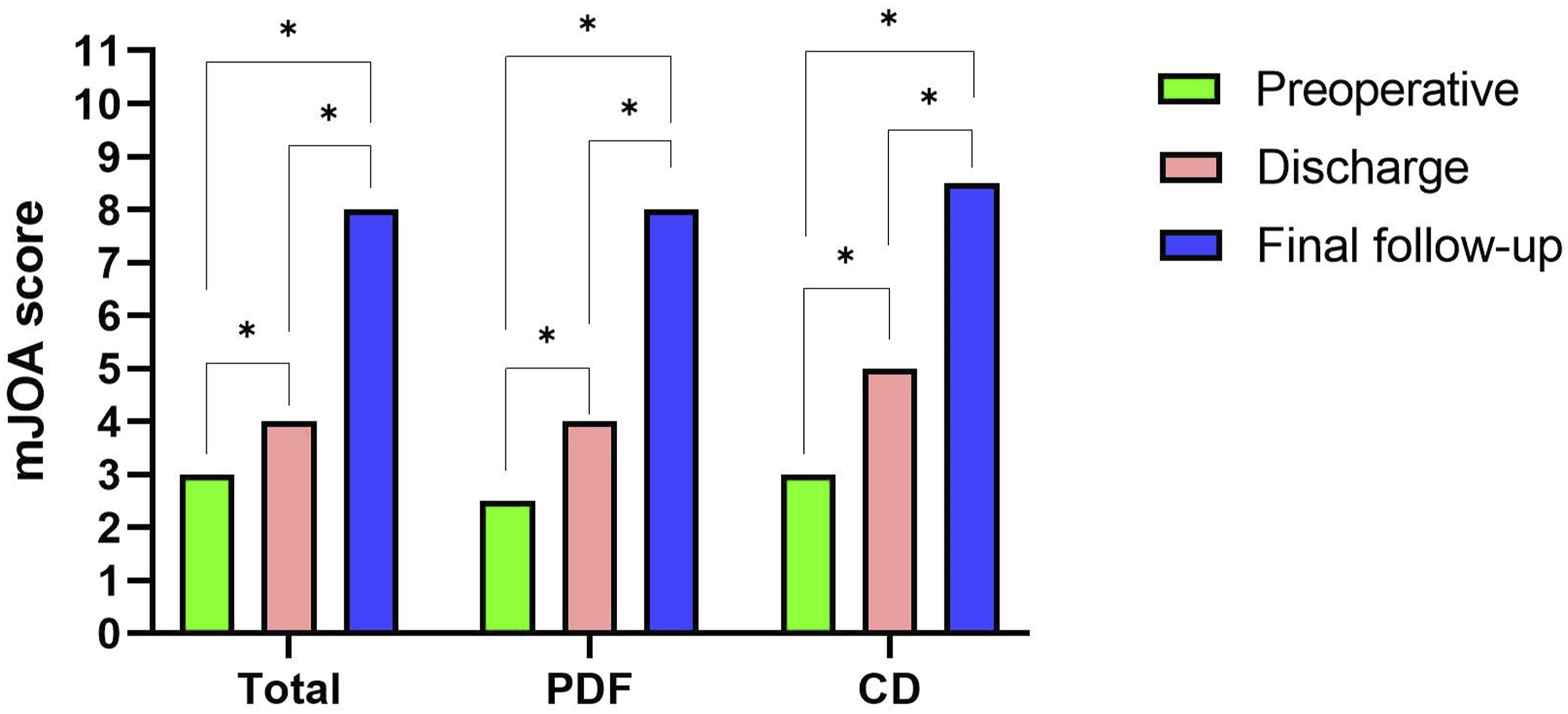
Multivariate Predictors of Walking Recovery
Analysis of Risk Factors Affecting Recovery of Independent Walking (N = 70)
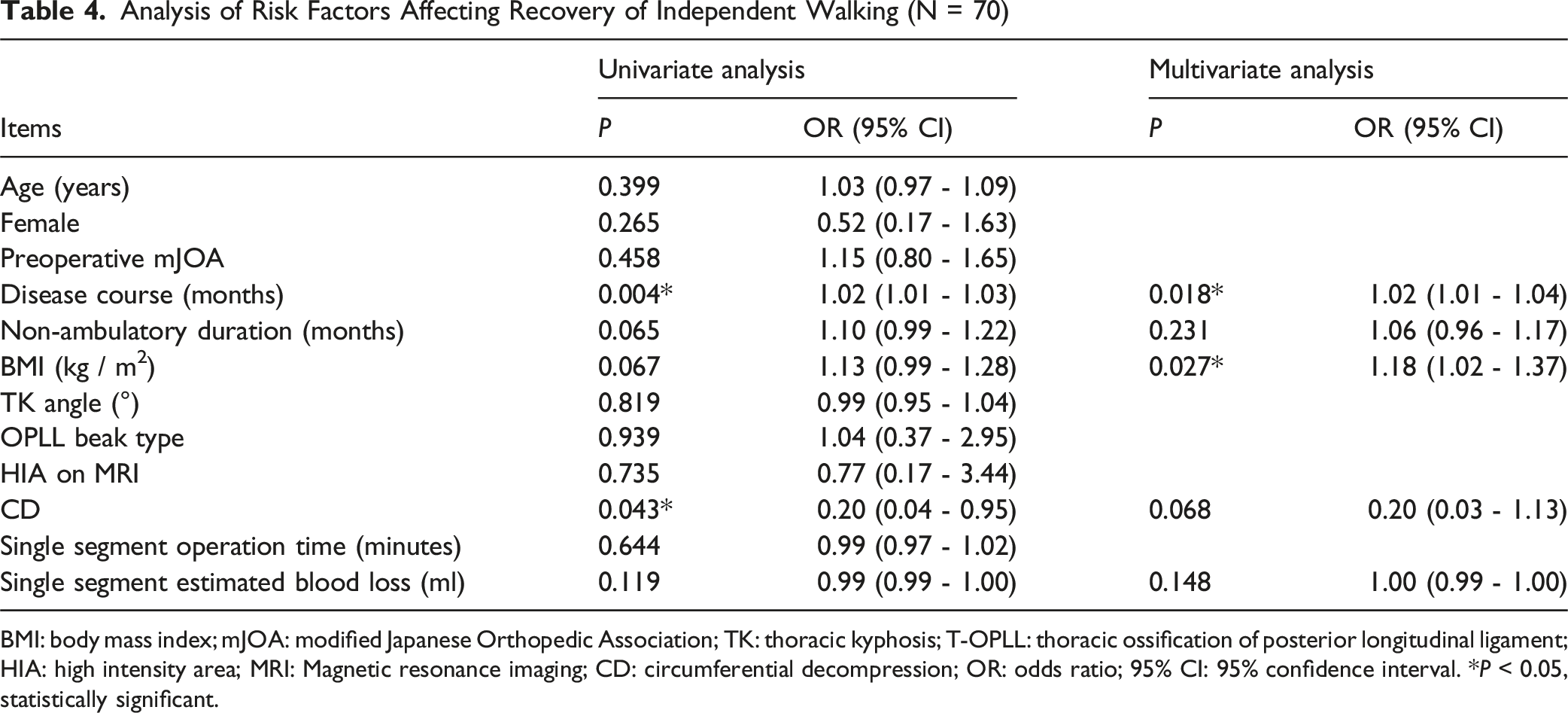
BMI: body mass index; mJOA: modified Japanese Orthopedic Association; TK: thoracic kyphosis; T-OPLL: thoracic ossification of posterior longitudinal ligament; HIA: high intensity area; MRI: Magnetic resonance imaging; CD: circumferential decompression; OR: odds ratio; 95% CI: 95% confidence interval. *P < 0.05, statistically significant.
Comparison of Demographic, Imaging Features, and Surgical Outcomes Between PDF and CD Groups
Comparative Analysis Between PDF and CD Groups
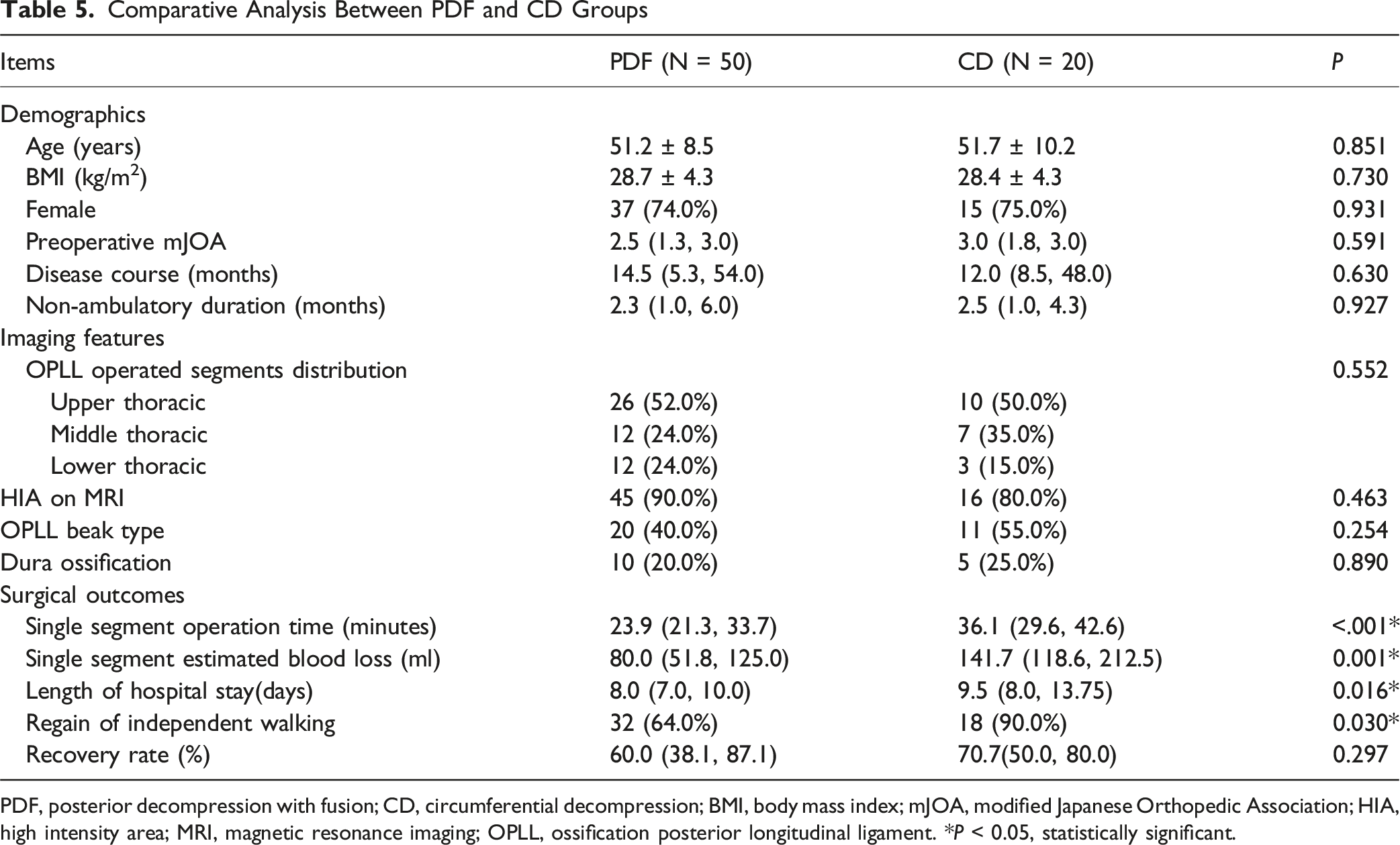
PDF, posterior decompression with fusion; CD, circumferential decompression; BMI, body mass index; mJOA, modified Japanese Orthopedic Association; HIA, high intensity area; MRI, magnetic resonance imaging; OPLL, ossification posterior longitudinal ligament. *P < 0.05, statistically significant.
Discussion
Few studies focusd on prognosis in non-ambulatory patients with T-OPLL, a condition associated with severe myelopathy and profound functional impairment. Our study is the first largest cohort to provide a comprehensive analysis of surgical outcomes in 70 non-ambulatory patients with thoracic OPLL, comparing CD and PDF. Our results demonstrate that decompressive surgery can lead to significant neurological recovery, with 71.4% of patients regaining independent walking ability at a mean follow-up period of 75.4 months.
Comparative Efficacy of CD and PDF
Prior studies11,14-16 have reported excellent clinical results in patients with T-OPLL, and our results were consistent with these studies. However, our results showed the PDF group achieved a higher recovery rate (60%) than Aizawa et al 8 reported, where only three patients underwent PDF. Such a small sample may have underestimated PDF’s efficacy. Moreover, in our study, the use of intraoperative ultrasound represents an important technical advancement, allowing for real-time assessment of decompression adequacy and potentially contributing to the favorable outcomes in both groups. This technology may be particularly valuable in determining when additional anterior decompression is necessary during posterior approaches, helping to avoid unnecessary aggressive maneuvers while ensuring adequate cord decompression. This challenges the notion that CD is universally superior and suggests PDF remains a viable option for select patients, particularly when considering its more favorable safety profile.
Complications and Risk-Benefit Balance
In our study, nearly 62.9% of patients had at least one complication, which was comparable to prior studies.17-19 While CD surgery offers superior functional outcomes, it is associated with higher perioperative risks, including increased single segment blood loss (141.7 mL vs 80.0 mL, P = 0.001), increased single segment operation time (36.1 minutes vs 23.9 minutes, P < 0.001), a longer length of stay (9.5 days vs 8.0 days, P = 0.016) and a significantly higher incidence of cerebrospinal fluid (CSF) leakage (70% vs 38%, P = 0.015). Our cohort identified 15 (21.4%) patients with dura ossification (10 cases in PDF group and 5 cases in CD group). All 5 patients with dura ossification in CD group experienced intraoperative dura tears. Moreover, the PDF group showed 4 (40%) cases of CSF leakage among their 10 dura ossification cases. Overall CSF leakage occurred in 33 (47.1%) cases in our study. Among CSF leakage cases, 9 (27.3%) patients demonstrated concurrent dura ossification. These findings are consistent with prior studies15,19-21 and emphasize the technical challenges inherent to CD. In contrast, PDF surgery presents a safer profile with shorter operative times and lower complication rates, making it a preferable option for high-risk patients, such as the elderly or those with multiple comorbidities. The decision to pursue CD should therefore be weighed carefully, considering the patient’s overall health and the surgeon’s expertise.
Predictors of Postoperative Walking Recovery
Multivariate analysis identified shorter disease duration (P = 0.018) and lower BMI (P = 0.027) as independent predictors of successful walking recovery. The association between shorter disease duration and better outcomes underscores the importance of early surgical intervention, as prolonged compression may lead to irreversible spinal cord damage. Similarly, lower BMI facilitates surgical exposure in the thoracic spine, particularly during circumferential decompression where visceral fat and epidural venous engorgement in obese patients significantly increase operative difficulty.
Clinical Decision-Making Framework
Based on our findings, we propose the following stratified approach to surgical selection: Surgical intervention should be considered early in the disease course for non-ambulatory T-OPLL patients. CD surgery should be prioritized for patients with shorter disease duration and lower BMI when maximal neurological recovery is the primary goal. PDF surgery represents a safer alternative for higher-risk patients or those with higher BMI. High-risk individuals where minimizing complications is critical.
Limitations
This study had several limitations. First, as a single-center study, there was a potential for selection bias. Second, the retrospective design restricted the ability to establish causal relationships. Third, we did not examine the timeline for postoperative recovery of walking ability, which could offer valuable guidance in surgical decision-making. Finally, although the follow-up period was moderate, longer-term outcomes remained unaddressed.
Conclusions
Our study presented a comprehensive analysis of surgical strategies for severe thoracic myelopathy caused by T-OPLL in a large cohort. Following decompression surgery, 71.4% regained the ability to walk independently over a mean follow-up period of 75.4 months. In non-ambulatory patients with thoracic OPLL, CD surgery offered superior walking recovery but carried higher perioperative risks, while PDF surgery provided a safer alternative with respectable outcomes. The choice of surgical approach should be individualized, considering disease duration and BMI. Early intervention remains a critical factor in optimizing neurological recovery. These insights provide a foundation for evidence-based surgical decision-making in this challenging patient population.
Footnotes
Ethical Considerations
Our study was approved by the ethics committee of the Peking University Third Hospital (No. M20241067) and conducted according to the principles of the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 82372451).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research data supporting this publication are available from the Peking University Third Hospital, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly.