
Abstract
Study Design
Literature Review.
Objective
Myelopathy affecting the thoracic spinal cord can arise secondary to several aetiologies which have similar presentation and management. Consequently, there are many uncertainties in this area, including optimal terminology and definitions. Recent collaborative cervical spinal research has led to the proposal and subsequent community adoption of the name degenerative cervical myelopathy(DCM), which has facilitated the establishment of internationally-agreed research priorities for DCM. We put forward the case for the introduction of the term degenerative thoracic myelopathy(DTM) and degenerative spinal myelopathy(DSM) as an umbrella term for both DCM and DTM.
Methods
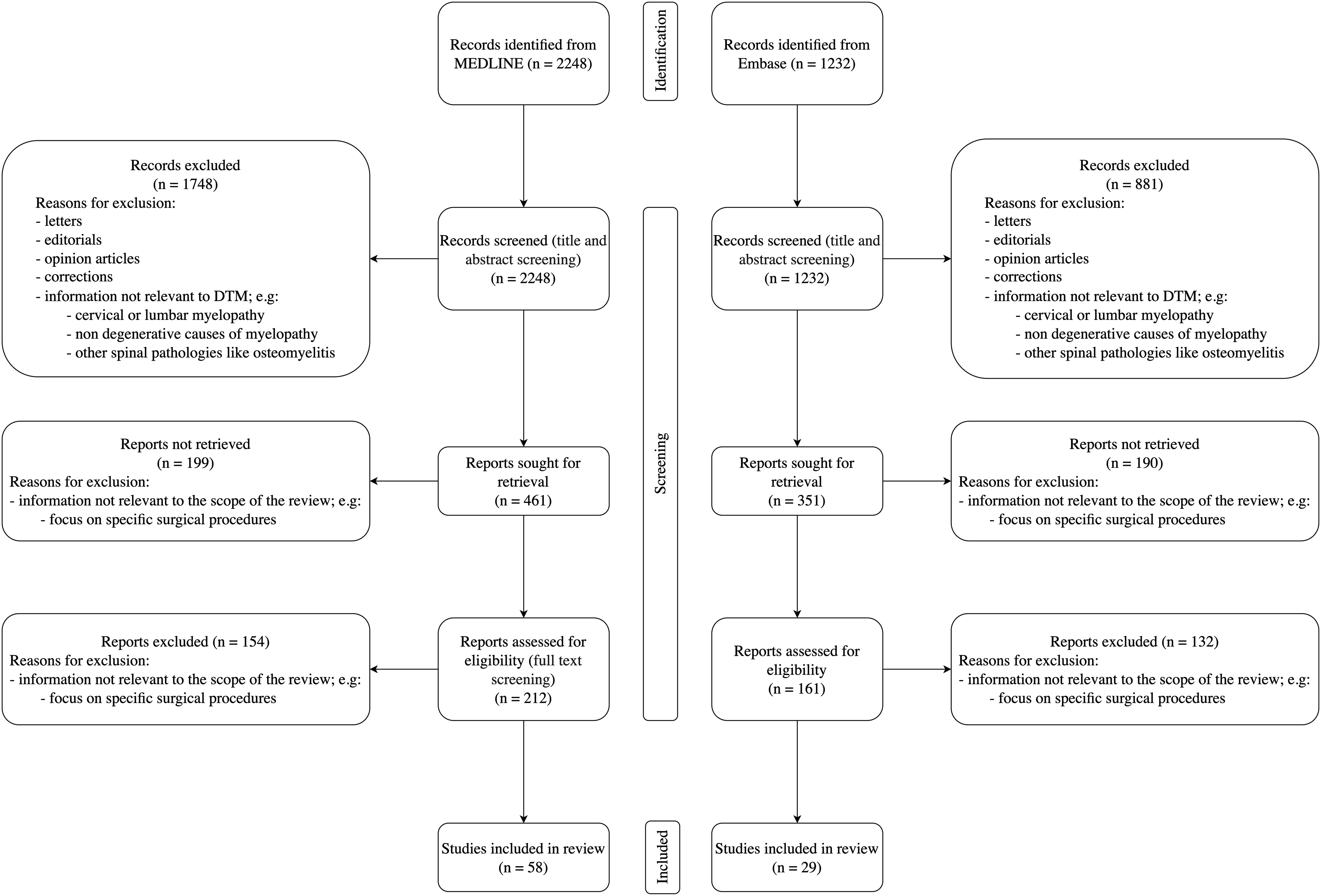
Following PRISMA guidelines, a systematic literature search was performed to identify degenerative thoracic myelopathy literature in Embase and MEDLINE.
Results
Conditions encompassed within DTM include thoracic spondylotic myelopathy, ossification of the posterior longitudinal ligament, ossification of the ligamentum flavum, calcification of ligaments, hypertrophy of ligaments, degenerative disc disease, thoracic osteoarthritis, intervertebral disc herniation, and posterior osteophytosis. The classic presentation includes girdle pain, gait disturbance, leg weakness, sensory disturbance, and bladder or bowel dysfunction, often with associated back pain. Surgical management is typically favoured with post-surgical outcomes dependent on many factors, including the causative pathology, and presence of additional stenosis.
Conclusion
The clinical entities encompassed by the term DTM are interrelated, can manifest concurrently, and present similarly. Building on the consensus adoption of DCM in the cervical spine and the recent proposal of degenerative cervical radiculopathy(DCR), extending this common nomenclature framework to the terms degenerative spinal myelopathy and degenerative thoracic myelopathy will help improve recognition and communication.
Keywords
Introduction
Myelopathy refers to a symptomatic spinal cord injury resulting from multiple causes, including degeneration, tumours, inflammation, infection, and vascular anomalies. It may occur at any spinal cord level, albeit most commonly at the cervical level. Myelopathies arise secondary to a range of aetiologies, however those resulting from degenerative spinal conditions are the most common. This review focuses on thoracic myelopathy and, in particular, myelopathy caused by degenerative conditions of the spine, which precipitate mechanical stress on the spinal cord.
The thoracic spine consists of 12 vertebrae from T1 to T12. Important distinguishing factors of the thoracic vertebrae include a body size that is larger than the cervical vertebrae but smaller than the lumbar vertebrae, pointed and downward-angled spinous processes, and articulation with the ribs. The latter is responsible for the reduced mobility of the thoracic spine compared to the cervical spine, which is thought to contribute to the lower prevalence of degenerative spinal myelopathy at the thoracic compared to the cervical level.1,2
Myelopathy from thoracic spondylotic myelopathy, and other forms of thoracic spine degeneration, including ossification of the posterior longitudinal ligament (OPLL),
3
ossification of the ligamentum flavum (OLF),4-6 calcification of ligaments,5,7 hypertrophy of ligaments,
5
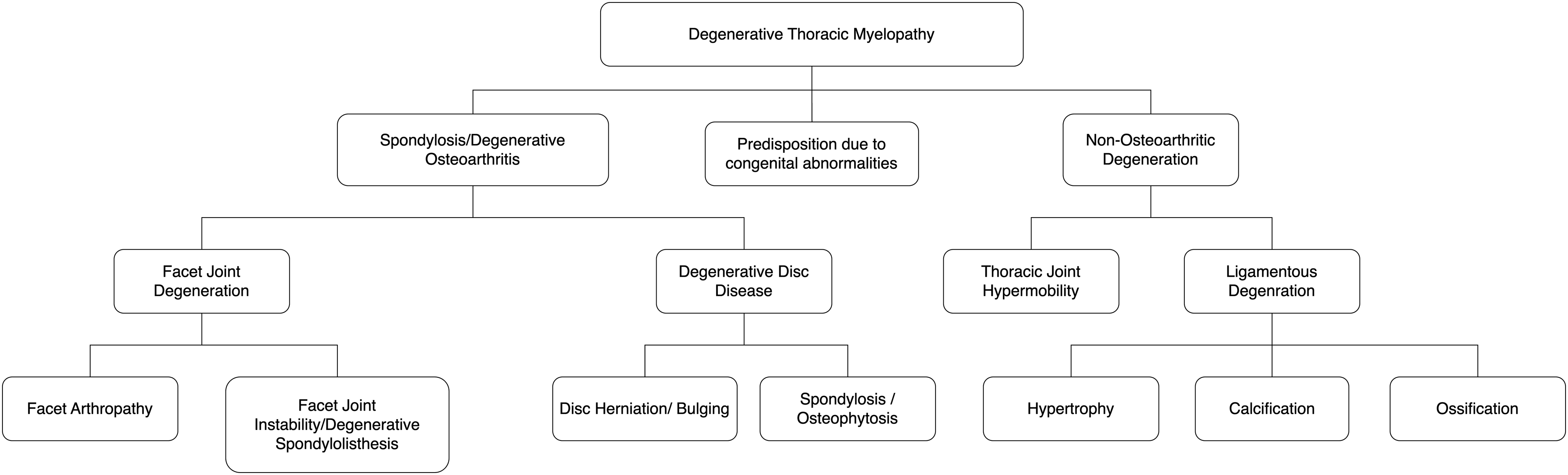
degenerative disc disease (DDD), thoracic osteoarthritis, intervertebral disc herniation (with the exception of acute herniation)8,9 and posterior osteophytes10,11 (Figure 1) share similarities in presentation and management. They trigger an uncommon, but disabling form of ‘slow motion’ spinal cord injury. A sagittal view of the thoracic spine demonstrates several pathologies that can cause DTM, including spondylosis, degenerative disc disease, and ossification of the posterior longitudinal ligament.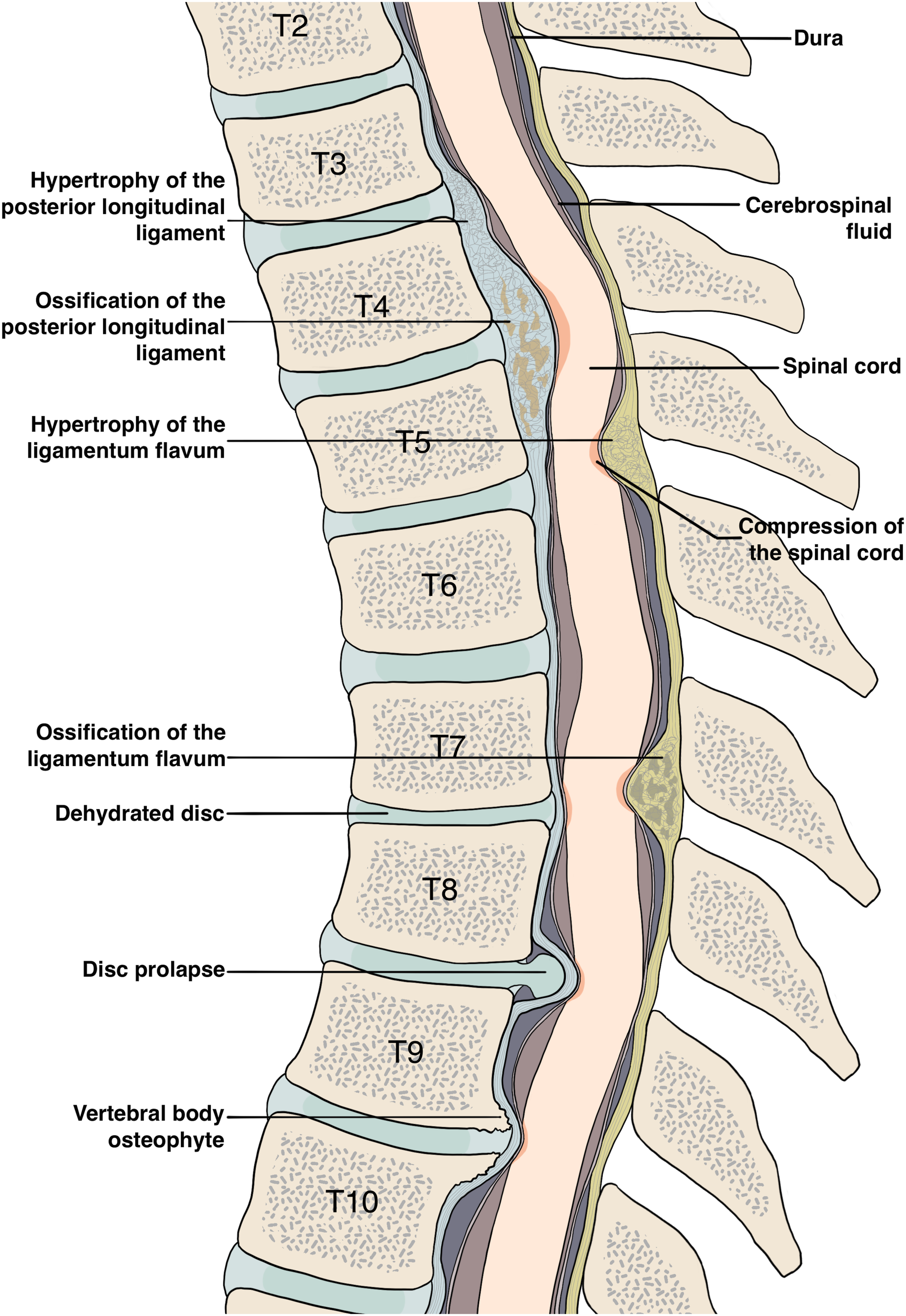
Many uncertainties challenge clinical care and research in this area, including significant heterogeneity in the use of terminology and definitions. Recent work in the cervical spine has resolved classification uncertainties with the proposal and subsequent community adoption of the term degenerative cervical myelopathy (DCM). DCM recognises that multiple degenerative spine pathologies converge on a common neurological phenotype, which is diagnosed and managed with similar approaches. This improvement in classification has also facilitated the establishment of common data elements and the definition of National Insitute for Health Research (NIHR) James Lind Alliance (JLA) research priorities.12,13
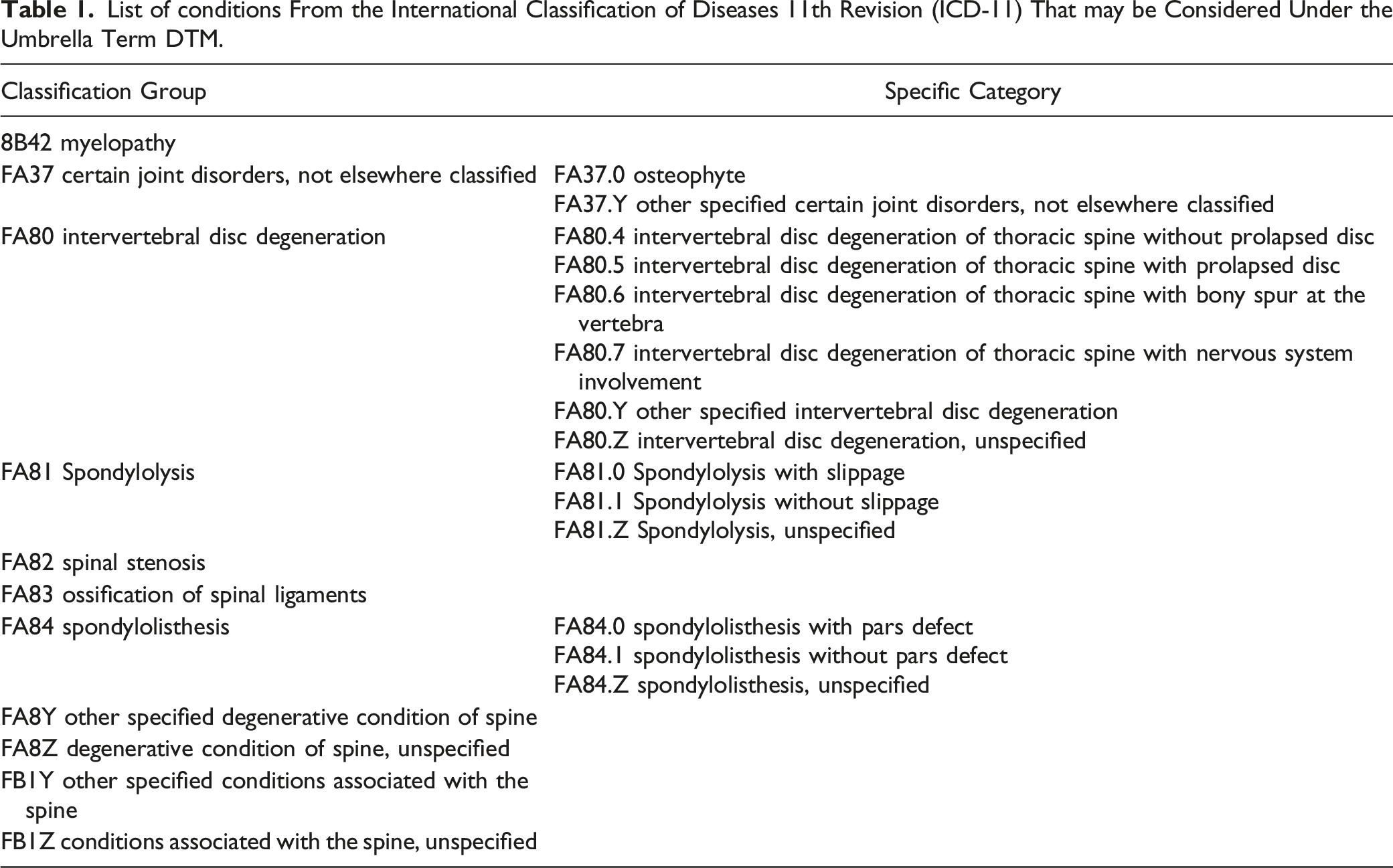
List of conditions From the International Classification of Diseases 11th Revision (ICD-11) That may be Considered Under the Umbrella Term DTM.
Methods
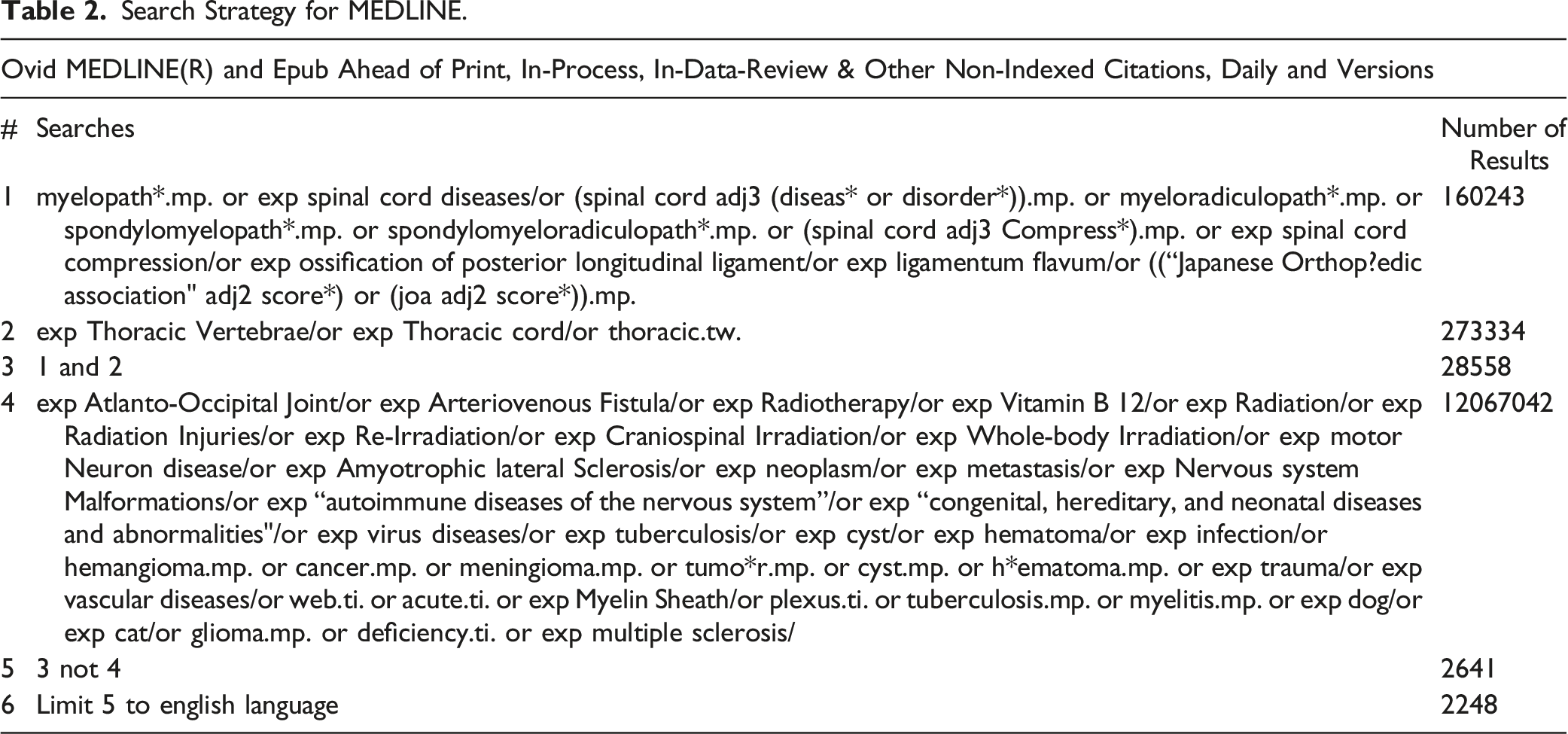
Search Strategy for MEDLINE.
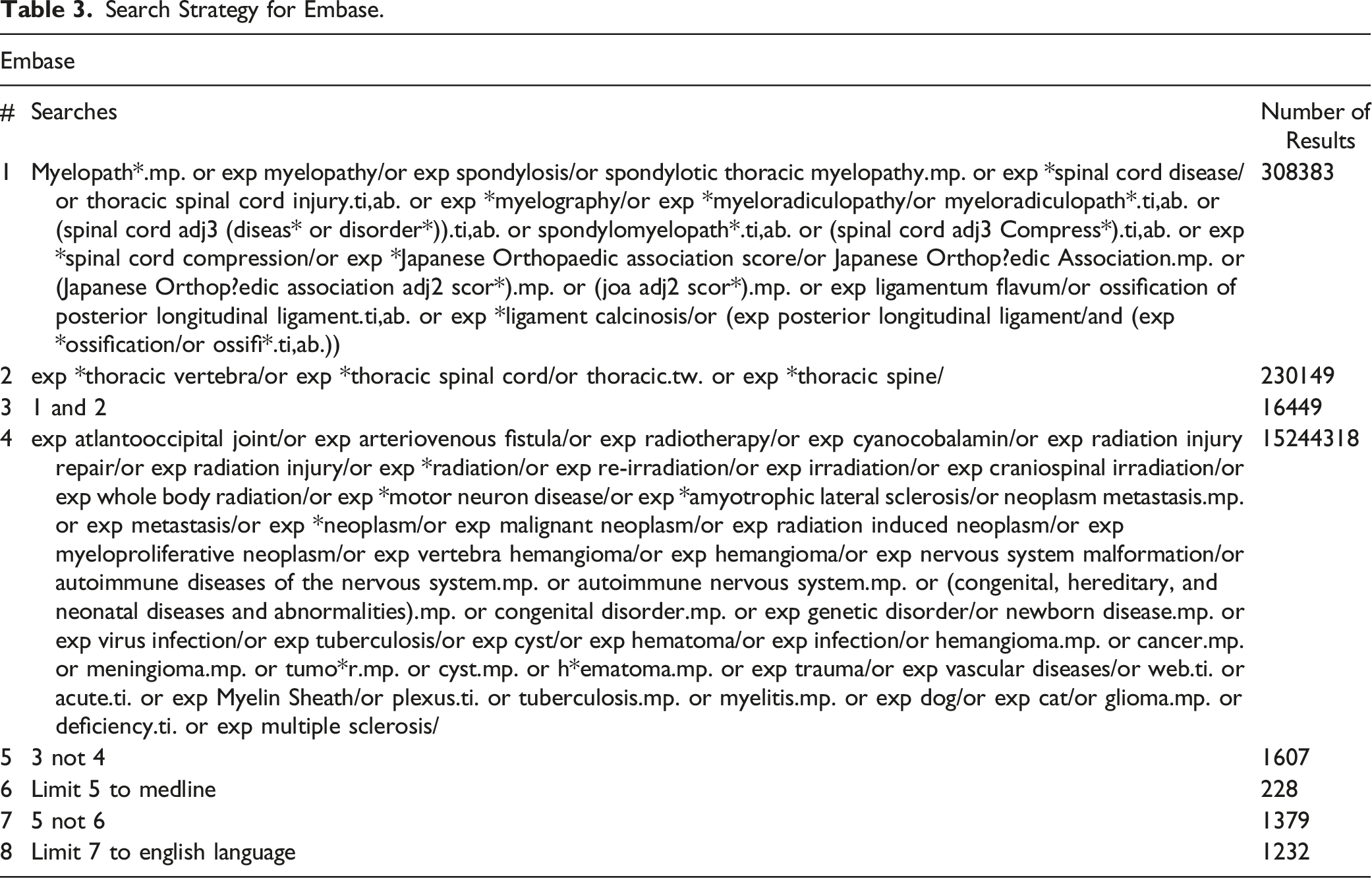
Search Strategy for Embase.
The majority of the screened papers had information irrelevant to DTM with a focus on topics such as cervical myelopathy, non-degenerative causes of myelopathy, and other spinal pathologies, such as osteomyelitis. Additionally, many papers focused on specific surgical procedures, which was outside the scope of this review. Papers meeting the inclusion criteria of a focus on degenerative pathology of the thoracic spinal column published in the English language were sought for retrieval. Retrieved papers were assessed for eligibility using a full-text review, and those that contained relevant information were included. The reference lists of included papers were also hand-searched to identify additional relevant studies. The search methodology is summarised in Figure 2. MEDLINE was searched first, with duplicate results from Embase automatically excluded from the search results. Included papers are listed in Supplementary Table 1. Most papers were published after 2010; 11 papers were published in 2021 and 8 in the first 6 months of 2022. A narrative synthesis of the identified literature is presented; no statistical analysis was performed. Search methodology flowchart based on PRISMA 2020 statement.
16
.
Discussion
Aetiology of DTM
Degenerative pathology in the thoracic spine that causes DTM can be divided into spondylotic (or osteoarthritic) and non-osteoarthritic (Figure 3). Both subcategories can compromise the spinal cord via exerting mechanical stress. In addition, certain congenital disorders can predispose to DTM. For example, Ehler-Danlos syndrome predisposes to thoracic instability and subsequent myelopathy
17
; Scheuermann’s disease is associated with thoracic disc herniation and OLF and is thus associated with at increased risk of DTM in affected individuals.18,19 Additionally, there may be a link between DTM and scoliosis, with a reported case of a patient with Klippel-Trenaunay-Weber syndrome having spinal stenosis and suffering from myelopathy.
20
However, due in part to the low incidence of thoracic myelopathy, research on predisposing factors is sparse. A conceptual differentiation of the constituents of degenerative thoracic myelopathy. DTM can be due to either osteoarthritic or non-osteoarthritic degeneration. In addition, certain congenital abnormalities can predispose individuals to DTM. Figure drawn with reference to Nouri et al 2015.
21
As recently outlined for DCM, 22 the pathophysiology of degenerative spinal myelopathy can be considered a function of mechanical stress, vulnerability and time, wherein mechanical stress consists of multiple mechanisms of loading, not just compression. Spinal cord vulnerability is influenced by cellular processes, and systemic factors, such as genetic and adaptive protective mechanisms, including autoregulation of spinal cord perfusion and nutritional status. 22 The association between obesity and smoking and both DCM and DTM, suggests similar pathogenesis may be exist for both DCM and DTM. 23 Moreover, the co-existence of DCM and DTM, such as by cervical and thoracic OLF and/or OPLL occurring concurrently, reinforces this hypothesis. 24
The aetiology of the mechanical stress that triggers DSM, i.e., whether it is due to static or dynamic mechanisms, can be used to subcategorise DTM. 25 Static spinal cord compression or spinal canal stenosis is the result of degenerative changes indenting the spinal cord, including osteophyte formation and ligament hypertrophy, calcification, and ossification. 25 Dynamic compression refers to compression as a result of movement, whether physiological or pathological. Due to the relatively reduced mobility of the thoracic spine, dynamic mechanisms are likely to be less important than in the cervical spine. Nevertheless, dynamic mechanisms may explain the increased rate of DTM in individuals with increased mobility and laxity of the thoracic spine. 17 Importantly, static and dynamic mechanisms of spinal cord stress may occur concomitantly. 22 Since dynamic mechanisms likely play a smaller role in DTM, a greater degree of static compression may well be needed compared to DCM to precipitate myelopathy.22,26 However, comparative analysis of the MRIs of patients with DCM and DTM and correlation with their presentations are needed to evaluate this hypothesis.
DTM Conditions
Comparison of Prevalence of Difference Causes of DTM

Furthermore, multiple degenerative changes often occur simultaneously. 32 For example, OLF and OPLL may present concomitantly, 31 and coexistent OPLL, OLF, and thoracic disc herniation have also been reported.29,31
Osteoarthritic Degenerative Conditions
Due to repetitive use, ageing, and environmental factors such as smoking, the proteoglycan composition of the nucleus pulposus changes, altering hydrostatic pressure, disc height, and subsequently force distribution.33-35 This can lead to a cascade of degenerative changes, which lead to osteophyte formation and intervertebral disc failure, such as disc bulging and herniation.25,36 Polymorphisms in several genes, such as those associated with cartilage and collagen formation like AGC1 and COL9A, have been associated with this degenerative process, 37 indicating a possible genetic vulnerability.
Thoracic disc herniation is a cause of myelopathy with an estimated frequency between 1 per 1000 and 1 per million.38-40 It is less common than cervical disc herniation, 41 which has an annual incidence of 18.6 per 100,000. 42 In fact, thoracic disc herniation accounts for only .15-4% of all disc operations.43,44 In approximately 40% of cases, the herniated disc is calcified. Typically, thoracic disc herniation occurs in middle-aged or older men and at levels below T8.9,41,45 The levels affected are classically at mechanical inflection points; increased mobility at these spinal levels is postulated to explain the increased prevalence of herniations. 41
Spondylosis is another osteoarthritic degenerative condition that can cause myelopathy. Here, protruding osteophytes, formed by the degenerative processes outlined above, compress the spinal cord. 46 This condition is infrequent in the thoracic spine compared to the cervical and lumbar regions 46 ; the low prevalence is partly explained by the high rate of misdiagnosis due to its co-occurrence with cervical and lumbar spondylosis. 46
In addition, another cause of thoracic myelopathy secondary to osteoarthritic pathology is degenerative spondylolisthesis. In this condition, an increased pedicle–facet joint angle and facet joint disruption has been observed. 47 Whilst far more common in the cervical and lumbar regions, 48 it can also occur in the thoracic region, often secondary to intervertebral disc degeneration. 48 Thoracic degenerative spondylolisthesis tends to occur in combination with lumbar spondylosis, which can lead to misdiagnosis and subsequently under-reporting. 48 Furthermore, it has also been associated with degenerative scoliosis. 49
Non-Osteoarthritic Degenerative Conditions
Changes in the spinal ligaments, notably the ligamentum flavum and the posterior longitudinal ligament, can lead to DTM. Although genetics may play a role in calcification, hypertrophy, and ossification of these ligaments, the fact that these phenomena usually manifest in older age implies a link with ageing and a likely degenerative aetiology.50-53
OLF is a condition whereby the ligamentum flavum undergoes progressive endochondral ossification.54,55 Ossification at multiple different spinal levels, i.e., tandem ossification, is a frequently recognised occurrence.3,25,31 OLF is more common in the thoracic spine compared to the cervical or lumbar spine, which may be due to the reduced mobility of this segment.56-58 The lower thoracic spine (T10-T12) is typically most affected.56,59-62 Thoracic OLF typically presents before 60 years of age 59 and is thought to be more prevalent in men,59-61,63,64 although this is inconsistent across studies.6,65,66 Genetic factors are believed to play a role in the development of OLF; an altered genome-wide DNA methylation profile has been reported in individuals with thoracic OLF. 67 Furthermore, overexpression of genes and transcription factors associated with the Notch and Wnt signaling pathways such as LGR5, ANGPT2, CX48, Runx2, and Osterix have also been associated with OLF in overexpression and knockdown experiments.54,68-71 Polymorphisms in the COL6A1 gene, which plays an important role in forming collagen, also appear to be associated with OLF. 72 Nonetheless, environmental factors are likely to play a role; mechanical stress has been shown to promote OLF by inducing the Notch and Wnt pathways. 73 Diet appears to be another important factor, 74 and fluoride intake is associated with risk of OLF. 75 There is also an association with obesity. 76
OPLL is another non-osteoarthritic degenerative precipitant of DTM. This is a condition whereby the posterior longitudinal ligament undergoes progressive thickening and endochondral ossification. 77 Similar to OLF, tandem ossification is frequent.3,25,31 OPLL is more common in the cervical spine. 78 In the thoracic spine, the mid-levels are typically affected.29,31 Thoracic OPLL is less common than OLF and is most commonly seen in Asian populations,31,79,80 with most studies conducted in Japan.80,81 The prevalence is much lower in North America and Europe. 80 Moreover, thoracic OPLL seems to be more often reported in males,31,82 although reports are inconsistent. 83 Similar to OLF, both genetic and environmental factors play a role in the development of the condition. Increased expression of IL17RC and COL6A1, two osteogenic genes, have been associated with OPLL.84-87 IGF-1 has been associated with ligament ossification, 88 which may explain the association between acromegaly and OPLL. 89 Hyperleptinemia and hyperinsulinemia are other factors involved in the development of OPLL, 90 as is obesity.78,90
Prevalence
DTM is less common than DCM. This may be due to the reduced range of motion in the thoracic spinal segment. 27 Nonetheless, accurate estimation of DTM prevalence is currently a challenge due to the heterogeneity in the classification of DTM as separate clinical entities, the paucity of literature on the topic, and the fact that studies have been mainly performed in Asian populations. Underdiagnosis is another challenge. 11 The incidence of surgical interventions is an important estimate of the prevalence of thoracic myelopathy. However, this is likely to be a substantial underestimate. Surgical intervention for thoracic myelopathy has a reported prevalence of approximately .9 per 100,000 population, which is less 10% of that of cervical myelopathy, according to a retrospective study in Japan. 91 These values were reported in studies of highly specific populations and are thus are not likely to be representative of the wider global epidemiology.
Presentation and Management
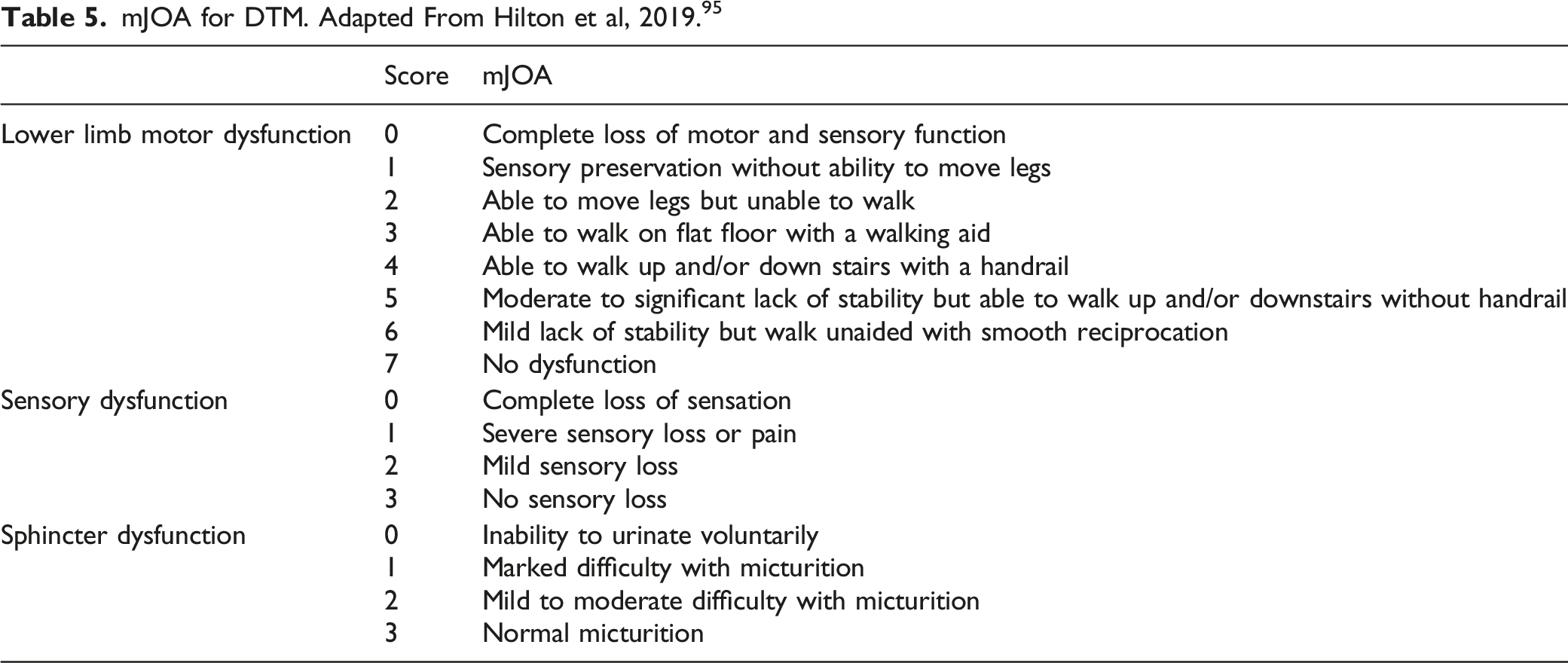
mJOA for DTM. Adapted From Hilton et al, 2019. 95
Furthermore, there are some rarer presentations of DTM. For example, high thoracic OLF may present with Horner’s syndrome, 96 whilst foot drop can be a symptom of calcified thoracic disc herniation at T11–L1 level. 97
The symptoms described are also often present when cervical or lumbar spinal disorders compress neural elements, which can result in misdiagnosis and delayed treatment.27,98 False localising levels, whereby the symptoms appear to emanate from a different anatomical location than their true origin,99,100 are another challenge that complicates diagnosis. For instance, cervical cord compression may present with a thoracic sensory level, and thoracic cord compression may present with a lumbar sensory level.92,99 Furthermore, it is relatively common for other neurological problems, such as peripheral neuropathy or lumbar and cervical spine disease, to occur concurrently with thoracic myelopathy, adding further diagnostic challenge.92,101 Radiculopathy and myelopathy also often occur simultaneously. 102 Finally, it is important always to consider the many non-degenerative conditions that can cause myelopathy, including autoimmune, inflammatory, and idiopathic causes.
Thoracic myelopathy tends to respond poorly to conservative management.103,104 Consequently, surgery is often required. Posterior decompressive laminectomy or laminoplasty and circumferential decompression via a posterior approach are the favoured approaches for posterior pathologies. 30 Posterior decompression is the most common operation for thoracic disc herniation, OLF, and OPLL, 30 whilst circumferential decompression is rarer and most commonly used in OPLL. 30 The preference for posterior decompression over circumferential decompression is related to factors such as reduced blood loss, lower complication rates, post-operation recovery rate, and less immediate neurologic deterioration. 30 Similar to the surgical approach for DCM, 105 there does not appear to be a clear difference between approaches with regard to long-term outcomes, 30 however conclusions are limited by a paucity of high quality comparative studies. Instrumented fusion may also be utilised alongside posterior decompression in OPLL, which has been associated with overall favourable outcomes. 106 Moreover, there appears to be a trend towards posterior instrumented fusion surgery for OLF, with 48.9% of cases in one prospective multicentre study being posterior decompression with instrumented fusion. 107
Anterior or lateral surgical approaches are performed less commonly but may be required for anterior compressive pathology; these come with the additional risks of damage to structures such as the aorta and oesophagus. 108 Nonetheless, anterior decompression for calcified discs may be associated with improved neurological outcomes. 109 Minimally invasive surgery has become increasingly common, particularly for disc herniations affecting a single thoracic level110,111; however, data on minimally invasive surgery is sparse.
Post-surgical outcomes in DTM depend on many factors, such as the operative approach, causative pathology, symptom duration, and presence of additional stenosis.30,104 For OLF, statistically significant improvements of JOA scores are reported, although recovery is typically incomplete.57,59,112,113 Recovery is dependent on several factors, such as preoperative neurological status, duration of symptoms, imaging findings, age, sex, number of levels involved, and type of OLF.52,57,66,113,114 However, the preoperative severity of myelopathy appears to be the most important factor.57,66,113 Outcomes for surgical management of thoracic disc herniations are generally poorer than those for cervical disc herniation. 115
Conclusion
Myelopathy of the thoracic spinal cord can be triggered by several interrelated, degenerative conditions that affect the thoracic spine, such as disc herniation, OLF, and OPLL. The paucity of published literature in this area is partly due to the relatively low prevalence of these conditions. The heterogeneity and inconsistency in the classification of DTM conditions as separate clinical entities further hinders synthesis of published data. Similar to the recent consensus process for DCM, we propose the introduction of the term degenerative thoracic myelopathy as an umbrella term for thoracic myelopathies triggered by degenerative conditions of the thoracic spine. Whilst there may be early hurdles in adoption, this terminology will improve recognition and communication as well as promote research efficiency and accelerate understanding of DTM. The present proposal represents current evidence-based expert consensus; future wider consultation may be necessary to refine it further.
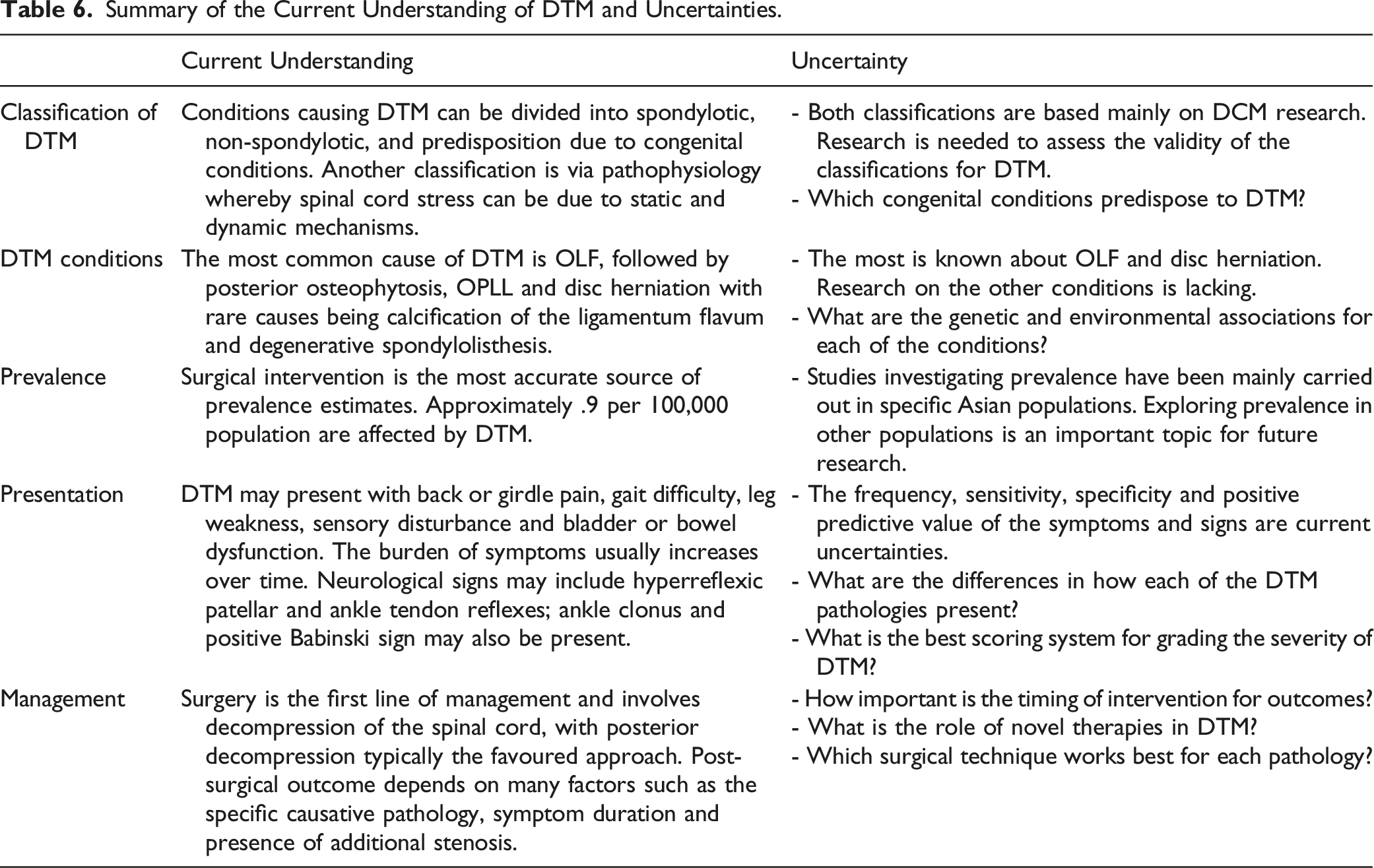
Summary of the Current Understanding of DTM and Uncertainties.
Supplemental Material
Supplemental Material - Degenerative Thoracic Myelopathy: A Scoping Review of Epidemiology, Genetics, and Pathogenesis
Supplemental Material for Degenerative Thoracic Myelopathy: A Scoping Review of Epidemiology, Genetics, and Pathogenesis by Tanzil Rujeedawa BA, Oliver D. Mowforth MA, MB, BChir, MSt, MRCS, Benjamin M. Davies BSc, MPhil, MRCS, Cylene Yang BSc MBBS, Aria Nouri MD, MSc, Jibin J. Francis MBBCh, FCNeurosurg FRCS, Bizhan Aarabi, MD, Brian K. Kwon, MD, PhD FRCSC, James Harrop MD, Jefferson R. Wilson, MD PhD, Allan R. Martin MD PhD, Vafa Rahimi-Movaghar, MD, James D. Guest, MD, PhD, Michael G. Fehlings, MD PhD FRCSC, Mark R. Kotter MD MPhil PhD in Global Spine Journal
Footnotes
Author Contributions
TR – conceptualization, manuscript drafting, and preparation, ODM – conceptualization, manuscript drafting, and preparation, BMD – conceptualization and manuscript review, CY – illustration and manuscript review, JF, BA, BKK, JH, MGF, JRW, ARM, VRM, JDG – manuscript review, MRK – conceptualization and manuscript preparation and review
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research in the MRK’s laboratory is supported by a core support grant from the Wellcome Trust and MRC to the Wellcome Trust-Medical Research Council Cambridge Stem Cell Institute. MRNK is supported by a NIHR Clinician Scientist Award, CS-2015-15-023. BMD is supported by an NIHR Clinical Doctoral Fellowship. ODM is supported by an Academic Clinical Fellowship at the University of Cambridge.
Disclaimer
The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.