
Abstract
Study Design:
Retrospective cross-sectional study.
Objectives:
There is insufficient data on the clinical features of ossification of the ligamentum flavum (OLF) of the thoracic spine and the risk of progression of ossified lesions. The link between obesity and ossification of the posterior longitudinal ligament (OPLL), which frequently coexists with OLF, has been demonstrated. However, the link between obesity and OLF has not been recognized. We aimed to determine the prevalence of obesity in thoracic OLF and whether the severity of OLF is associated with the degree of obesity.
Methods:
A total of 204 symptomatic Japanese subjects with thoracic OLF and 136 subjects without spinal ligament ossification as controls were included. OLF subjects were divided into 3 groups: 1) localized OLF (OLF <2-intervertebral regions); 2) multilevel OLF (OLF ≥3-intervertebral regions); and 3) OLF + OPLL. The severity of OLF was quantified using the OLF index using computed tomography imaging of the entire spine.
Results:
The proportion of severely obese subjects (BMI ≥ 30 kg/m2) was significantly higher both in the multilevel OLF group (25.5%) and the OLF + OPLL group (44.3%) than in the localized OLF group (3.6%) and the control group (1.4%) (P < 0.01). BMI, age, and coexistence of cervical OPLL and lumbar OLF were associated with thoracic OLF index in the multiple regression analysis.
Conclusions:
Our findings demonstrated that obesity is a distinct feature of multilevel OLF in the thoracic spine and that the severity of OLF is associated with the degree of obesity.
Keywords
Introduction
Ossification of the ligamentum flavum (OLF), which is a representative ossification disease of the spinal ligament along with the ossification of the posterior longitudinal ligament (OPLL), is relatively common in East Asia.1-9 The pathogenesis of OLF has not been studied as extensively as OPLL, and its causative mechanism remains uncertain. Several studies indicate that the degeneration of ligamentous attachments associated with mechanical factors and/or local instability is involved in the development of OLF,10-12 but there is insufficient evidence.
The ossification tendency of the entire spine also contributes to the development of OLF. 13 Patients with OPLL are known to have a high incidence of OLF.13,14 In addition, epidemiological studies have revealed that patients with thoracic OPLL have a high prevalence of morbid obesity and co-existing diffuse ossified lesions of the spinal ligaments, including OLF, suggesting an association between obesity and heterotopic ossification of the spinal ligaments.15,16 However, at present, the association between thoracic OLF and obesity is not recognized because it is not clear whether such patients are classified as OPLL or OLF. This has prompted us to investigate the association between OLF and obesity.
There is no effective treatment for OLF other than surgery. To develop a new therapeutic strategy against OLF, we need to clarify the patient’s background and explore the underlying etiology of OLF. Our objective was to investigate the prevalence of obesity in patients with symptomatic thoracic OLF and to evaluate whether the degree of obesity is associated with the severity of OLF.
Materials and Methods
Study Design
A cross-sectional study was conducted in accordance with the Declaration of Helsinki (1964), including patients between April 2015 and December 2020, and was approved by the ethics committees of the 2 participating hospitals. This study was approved by our institutional ethical review board (approval number: 2020-14) and the need for patient informed consent was waived owing to the retrospective nature of the study and deidentified data used.
Patients
A total of 242 patients with symptomatic thoracic OLF, who regularly visited our hospital and related institutions in the Hokkaido prefecture of Japan, were included. All patients were diagnosed and followed by a spine surgeon or radiologist based on clinical symptoms and X-ray or computed tomography (CT) images at the time of diagnosis. We excluded 20 patients who had comorbidities, such as cancer or gastrointestinal diseases, that might cause weight loss, or whose medical records clearly showed a weight loss of 5 kg or more within the preceding 6 months. We also excluded 18 patients who did not undergo whole-spine CT scans because we aimed to investigate the prevalence of heterotopic ossification of the entire spine. Finally, 204 patients (115 men, 89 women) aged from 29 to 88 years who underwent whole-spine CT scans were included in this study.
As controls, 415 subjects who underwent whole-spine CT scans from the cervix to the pelvis selected from 7860 subjects who visited one of the above institutions for health assessment between June and December 2020. Of these, 136 subjects with no ossification of the spinal ligaments as assessed by CT were finally included.
Grouping of Patients With Thoracic OLF According to OLF Type and Co-Existing Thoracic OPLL
Patients were classified into 3 groups based on the number of intervertebral regions with thoracic OLF and the presence or absence of co-existing thoracic OPLL: 1) the localized OLF group (OLF <2-intervertebral regions, n = 74); 2) the multilevel OLF group (OLF >3-intervertebral regions, n = 51); and 3) the OLF + OPLL group (OLF with OPLL, n = 79). The demographics and clinical characteristics of the patients in the 4 groups, including the control group, were compared.
Demographics, Comorbidities, and the Distribution of Spinal Ligament Ossification
Demographic data was obtained from all subjects
The body mass index (BMI) and comorbidities (hypertension, diabetes, hyperlipidemia, ischemic heart disease, hyperuricemia, kidney disease, and liver disease) were assessed. The distribution of spinal ligament ossification [i.e., cervical (C), thoracic (T), and/or lumbar (L)], including OLF, OPLL, and ossification of the anterior longitudinal ligament (OALL), was evaluated using axial and sagittal reconstruction CT images of the entire spine.
Image Acquisition
Non-contrast CT scans involving the entire spine were performed using the CT-Aquilion ONE™ / GENESIS Edition system (Canon Medical Systems Corporation, Tochigi, Japan).
The Severity of Spinal Ligament Ossification
To quantify the severity of OLF, the OLF index was calculated according to a previously described method.16,17 The analysis was performed independently by 3 board-certified spine surgeons. Before reviewing the images, readers interpreted the same images for 20 patients to determine the interobserver agreement. The interobserver intraclass correlation coefficient (ICC) was 0.90, and the 95% confidence interval (CI) was 0.77-0.96, indicating high interobserver agreement. The disagreement was resolved through discussion.
Statistical Analysis
Data was analyzed using the BellCurve for Excel software (version 3.10; Social Survey Research Information Co., Ltd., Tokyo, Japan). Three-group comparisons were evaluated using the Kruskal-Wallis test and Fisher’s exact test. The relationship between factors affecting the severity of spinal ligamentous ossification was analyzed by multiple regression analysis. The ICC was analyzed using a 2-way mixed-effect model. Statistical significance was basically set at P < 0.05; however, Bonferroni correction was performed for multiple testing and was set at P < 0.017 (0.05/3) for the 3-group comparison and P < 0.012 (0.05/4) for the 4-group comparison.
Results
Baseline Characteristics and Disease Status of Patients With Thoracic OLF
The characteristics of patients from each group and representative CT images are shown in Table 1 and Figure 1, respectively. Most patients with severe myelopathy had a history of spinal surgery. The age at investigation was significantly higher in the localized OLF group, multilevel OLF group, and OLF + OPLL group than in the control group. There were significantly more men in the multilevel OLF group than in the OLF + OPLL and the control group. Regarding comorbidities, the prevalence of hyperlipidemia in the OLF + OPLL group was significantly higher than that in the localized OLF and the control group. The prevalence of hypertension was significantly higher in the localized OLF group, multilevel OLF group, and OLF + OPLL group than in the control group. The prevalence of diabetes mellitus was significantly higher in the localized OLF group and OLF + OPLL group than in the control group. There was no significant difference in the prevalence of ischemic heart disease, hyperuricemia, renal disease, and liver disease among all groups. The prevalence of hypertension, diabetes mellitus, and hyperlipidemia in the OLF + OPLL group was relatively higher than that in the general population in Japan. 18
Clinical Characteristics of the OLF Groups.
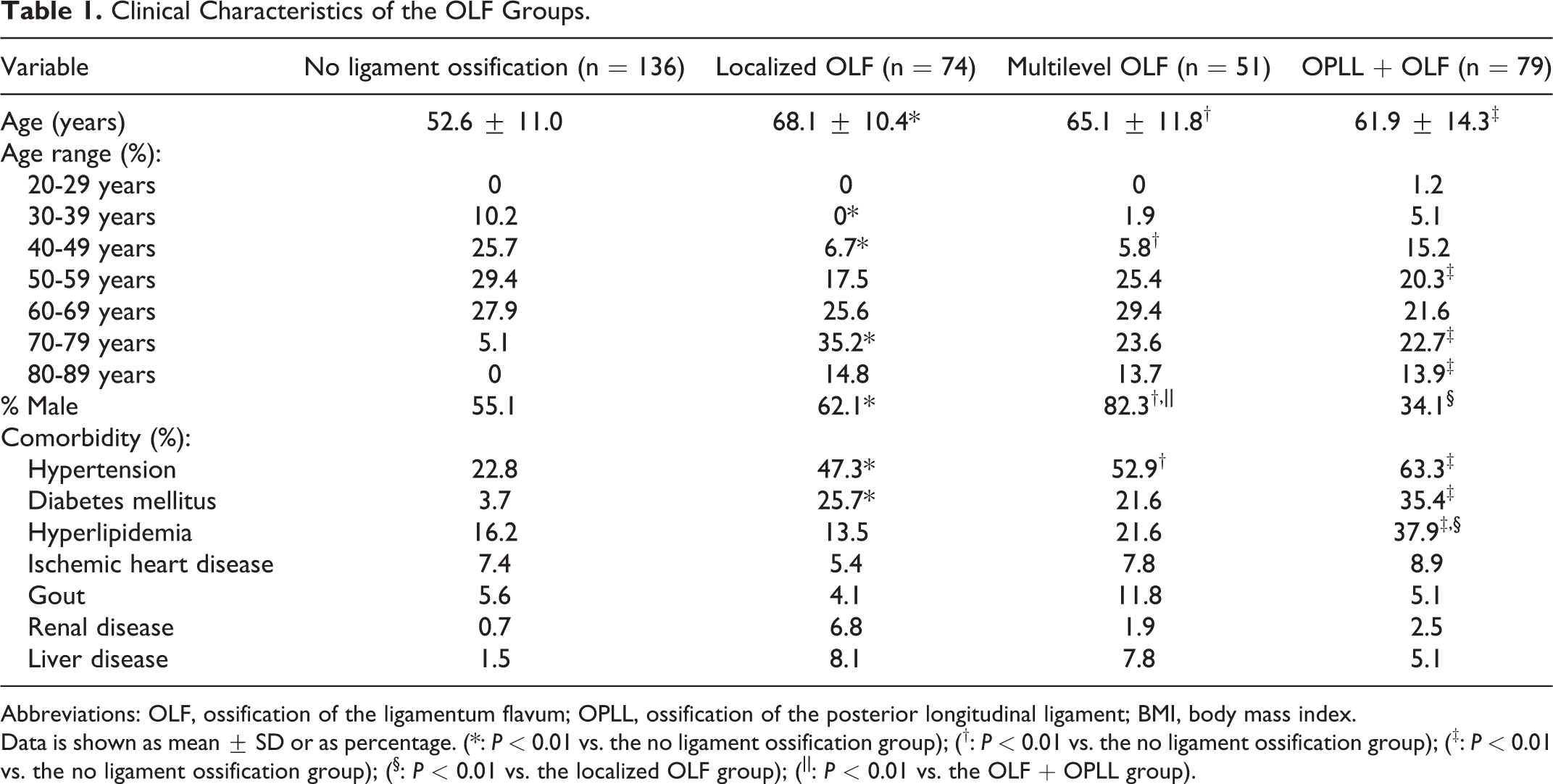
Abbreviations: OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index.
Data is shown as mean ± SD or as percentage. (*: P < 0.01 vs. the no ligament ossification group); (†: P < 0.01 vs. the no ligament ossification group); (‡: P < 0.01 vs. the no ligament ossification group); (§: P < 0.01 vs. the localized OLF group); (||: P < 0.01 vs. the OLF + OPLL group).
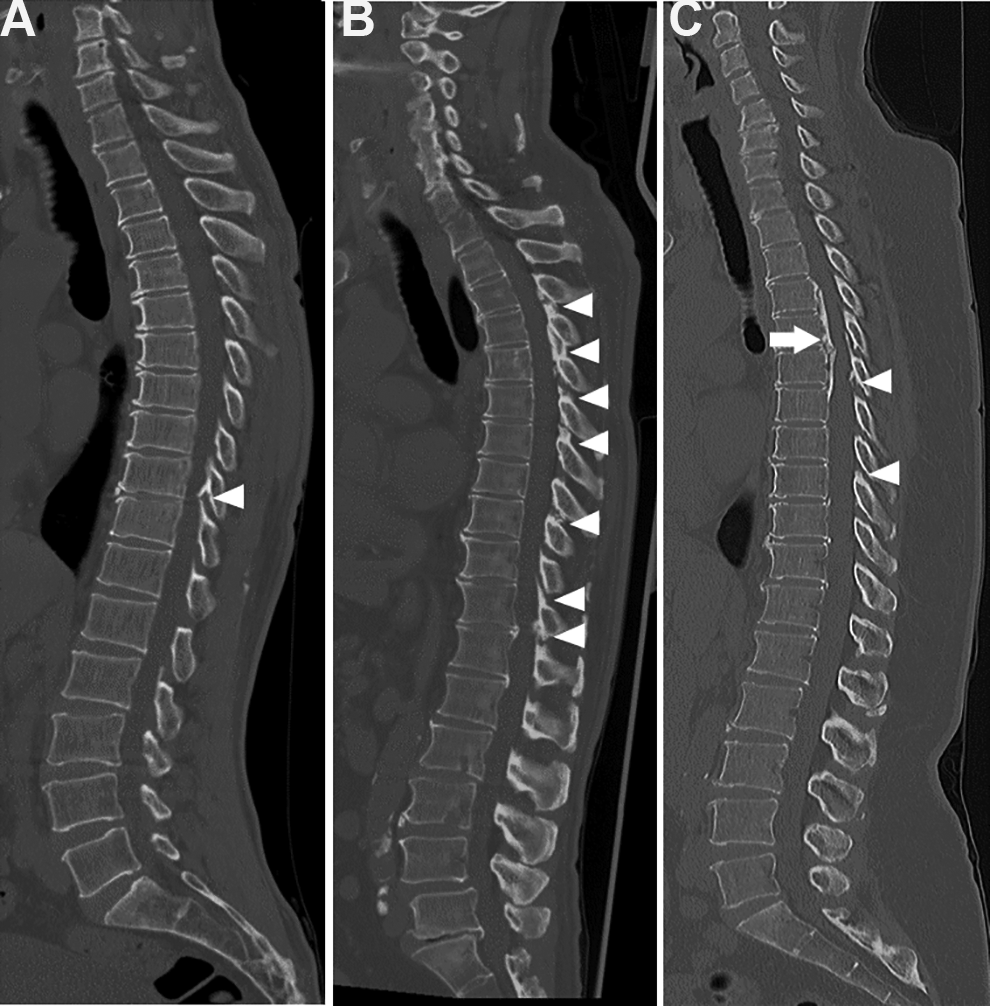
Sagittal reconstruction CT images of the entire spine in patients with thoracic OLF. A, A representative case from the localized OLF group. A 42-year-old man with a BMI of 24.1 kg/m2 has a localized OLF (arrowhead) in the thoracic spine at the T10/11. B, A representative case from the multilevel OLF group. A 58-year-old man with a BMI of 28.8 kg/m2 has an OLF (arrowheads) in the multi-segmental thoracic spine. C, A representative case from the OLF + OPLL group. A 52-year-old woman with a BMI of 40.1 kg/m2 has thoracic OPLL (arrow) and OLF (arrowheads).OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index; CT, computed tomography.
Influence of Obesity on Thoracic OLF
Data on BMI is shown in Figure 2 and Table 2. The proportion of severely obese patients (BMI ≥ 30 kg/m 2 according to obesity classification for Asian population defined by World Health Organization [WHO] 19 ) in the total population with thoracic OLF was 24.0%. The mean BMI was significantly higher both in the multilevel OLF group (28.6 ± 4.8 kg/m2) and the OLF + OPLL group (30.4 ± 6.3 kg/m2) than in the localized OLF group (23.1 ± 2.8 kg/m2, P < 0.01) and the control group (23.3 ± 3.5 kg/m2, P < 0.01) (Figure 2). The proportion of severely obese patients both in the multilevel OLF and the OLF + OPLL group was significantly higher than in the localized OLF and the control group (P < 0.001). The proportion of severely obese patients in the OLF + OPLL group was the highest among the 4 groups (Table 2).
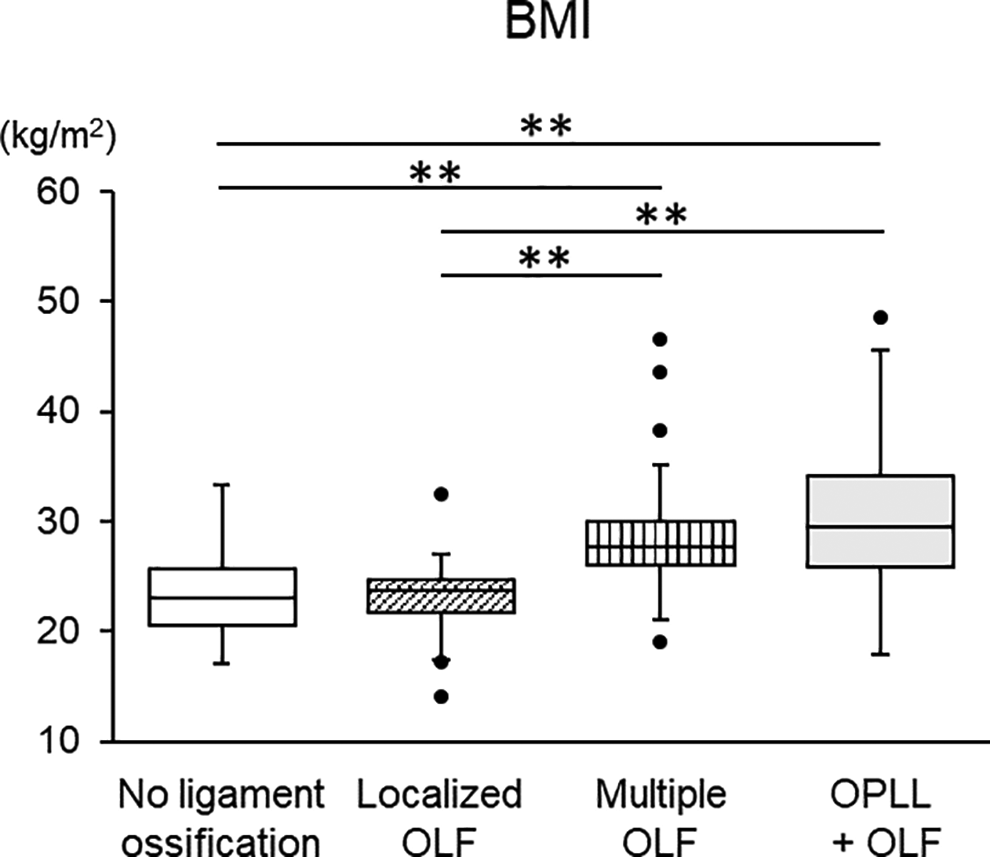
Comparison of body mass index in the thoracic OLF groups and the control group. **: P < 0.001. OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index.
Comparison of the Degree of Obesity and the Rate of Co-Existing Spinal Ligament Ossification in the OLF Groups.
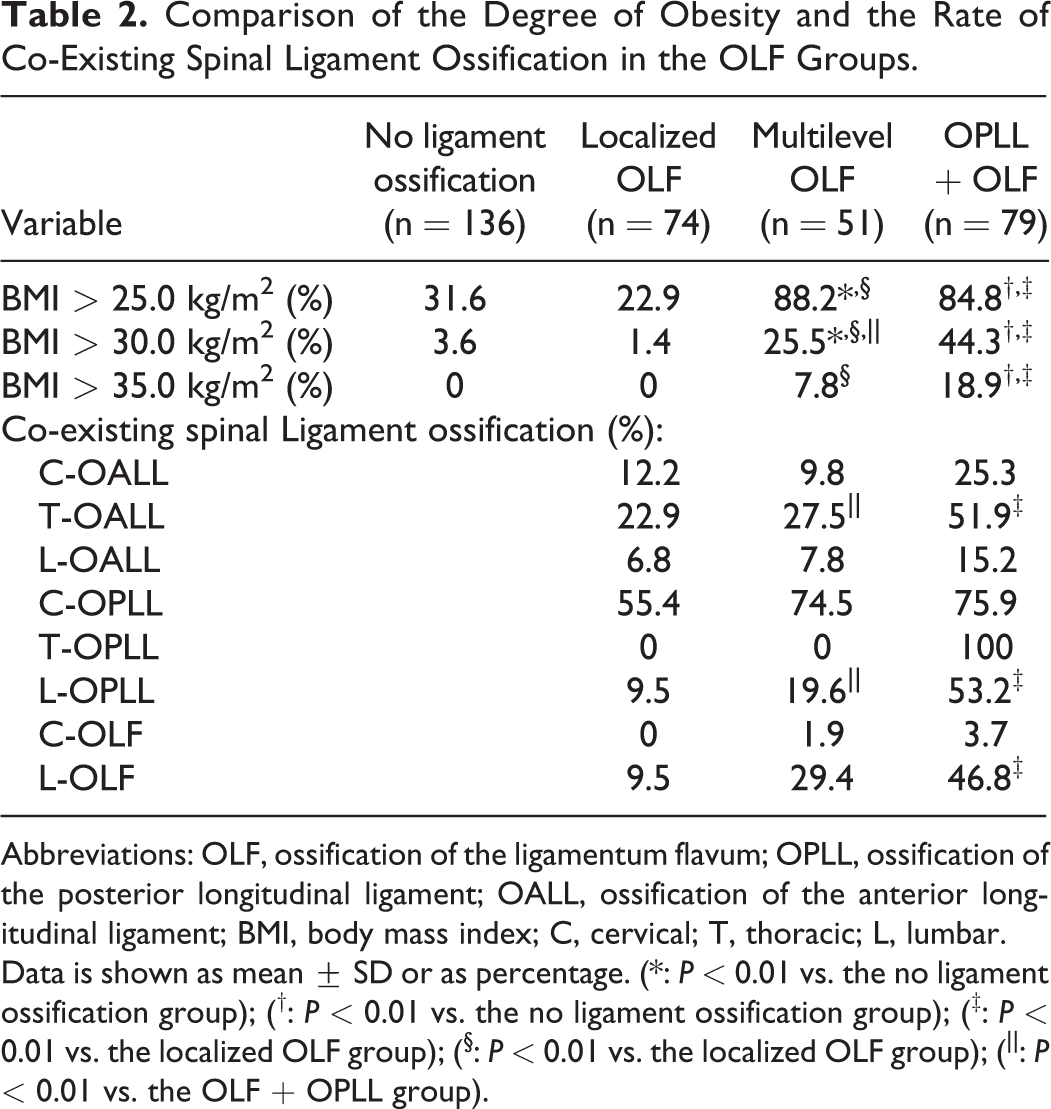
Abbreviations: OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; OALL, ossification of the anterior longitudinal ligament; BMI, body mass index; C, cervical; T, thoracic; L, lumbar.
Data is shown as mean ± SD or as percentage. (*: P < 0.01 vs. the no ligament ossification group); (†: P < 0.01 vs. the no ligament ossification group); (‡: P < 0.01 vs. the localized OLF group); (§: P < 0.01 vs. the localized OLF group); (||: P < 0.01 vs. the OLF + OPLL group).
Prevalence of Co-Existing Heterotopic Spinal Ligament Ossification Among Patients With Thoracic OLF
We evaluated the proportion of patients with co-existing spinal ligament ossification to verify whether the tendency of ossification of the entire spine affects the severity of thoracic OLF. The OLF + OPLL group had the highest proportion of co-existing ligament ossification of the entire spine (i.e., C-OALL, T-OALL, L-OPLL, and L-OLF) among all groups (Table 2). The coexistence of L-OPLL and L-OLF in the multilevel OLF group was higher than in the localized OLF group, but the difference was not significant. The coexistence of T-OALL and L-OPLL in the OLF + OPLL group was significantly higher than in the multilevel OLF group.
The OLF index was used to compare the severity of OLF among the 3 groups (Figure 3). The OLF index in the thoracic spine (the T-OLF index), the OLF index in the lumbar spine (the L-OLF index), and the sum of all OLF indices (the total OLF index) were obtained. The T-OLF index in the multilevel OLF group was significantly higher than both in the localized OLF and the OLF + OPLL groups. The L-OLF index and the total OLF index both in the multilevel OLF and the OLF + OPLL groups were significantly higher than in the localized OLF group, respectively (P < 0.01) (Figure 3A-C).
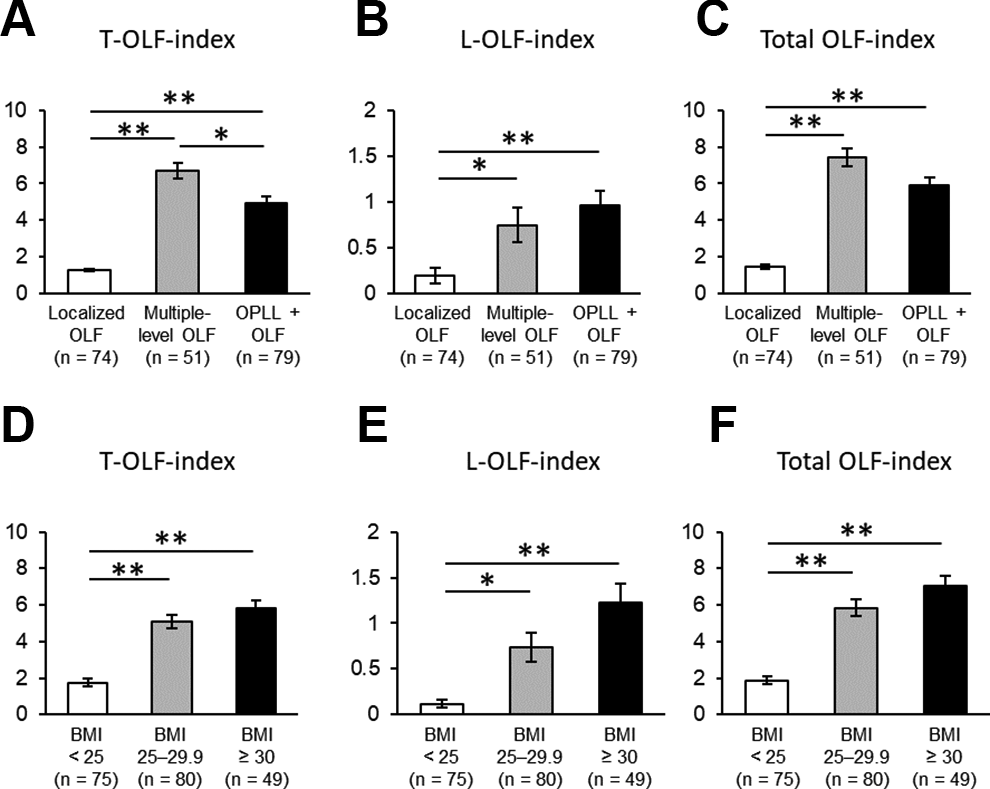
Comparison of the OLF indices by ossification type of the thoracic OLF and the BMI stage. *: P < 0.01, **: P < 0.001. OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index; T, thoracic; L, lumbar. A-C. T-OLF, L-OLF, and total OLF indices by ossification type of the thoracic OLF. D-F. T-OLF, L-OLF, and total OLF indices by BMI stage.
We then divided the thoracic OLF patients into 3 groups according to the BMI stage and evaluated the relationship between the OLF index and BMI. The T-OLF index, L-OLF index, and total OLF index were significantly higher both in the obese group (BMI: 25-29.9 kg/m2) and the severely obese group (BMI ≥ 30 kg/m2) than in the normal weight group (BMI < 25 kg/m2), respectively (P < 0.01) (Figure 3D-F). InOLF patients without OPLL (i.e., the localized OLF and the multilevel OLF groups), there was a positive correlation between BMI and the T-OLF index (R = 0.565) (Figure 4).
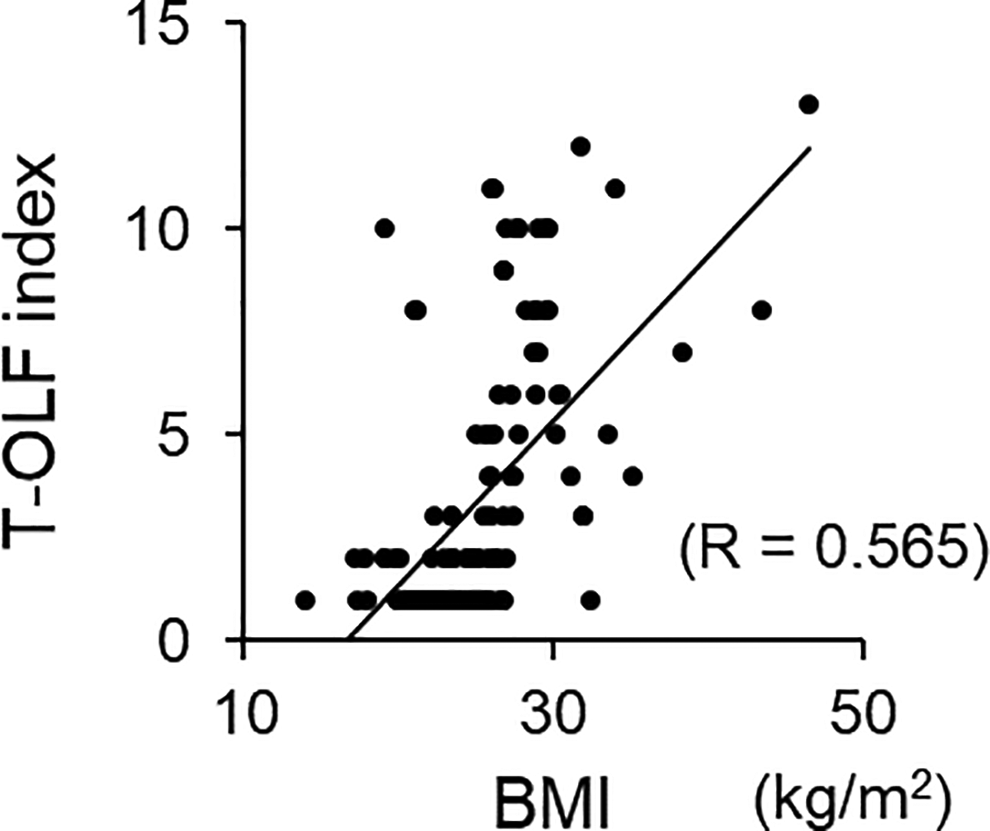
Correlation between the thoracic OLF index and body mass index in OLF patients without OPLL. OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index; T, thoracic.
Risk Factors Associated With the Severity of Thoracic OLF
We performed multiple regression analysis in all subjects on the associations of risk factors with the severity of thoracic OLF. Age, BMI, and co-existing C-OPLL and L-OLF were revealed as factors associated with the T-OLF index (Table 3). The BMI value was the factor most strongly associated with the T-OLF index compared to other independent variables (standardized β, 0.43; 95% CI, 0.16 to 0.34; P < 0.001).
Multiple Regression Analysis for Factors Associated With the T-OLF Index.
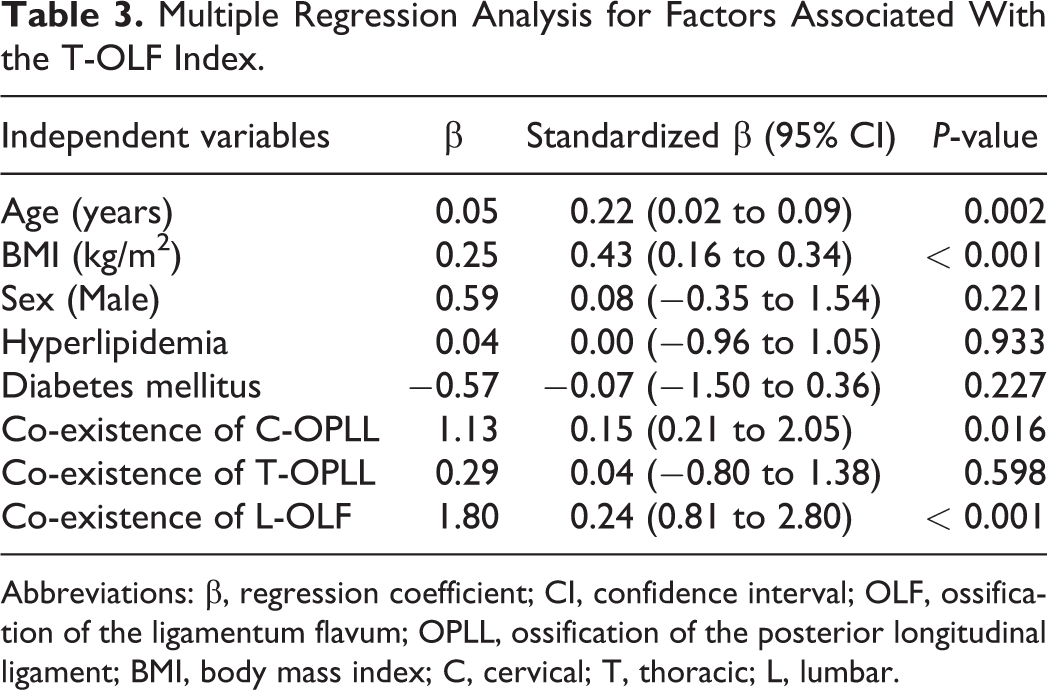
Abbreviations: β, regression coefficient; CI, confidence interval; OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; BMI, body mass index; C, cervical; T, thoracic; L, lumbar.
Discussion
The realization of the link between obesity and heterotopic spinal ligament ossification, 15,16,20-22 which has become apparent in recent years, could provide opportunities for the development of treatments for these diseases where no effective treatment has been identified. However, it remains unclear which background characteristics of the patients are involved in both obesity and ossification. The current study revealed that the prevalence of severe obesity (BMI ≥ 30 kg/m2) in symptomatic patients with thoracic OLF (i.e., the localized OLF, the multilevel OLF, and the OLF + OPLL) was surprisingly high at approximately 24.0%, which was 6 times higher than that in the general Japanese population (3.8%). 18 In comparison with thoracic OLF combined with OPLL, the proportion of severe obesity in multilevel thoracic OLF was significantly lower; however, we succeeded in characterizing that OLF with a high severity of ossification also contains a high proportion of obesity. An association between obesity and OPLL has been established,15,16,21,22 but the association between obesity and OLF has not been reported. Such a high prevalence of severe obesity in patients with thoracic OLF has not been recognized may be because most patients with thoracic OLF have co-existing cervical or thoracic OPLL and these patients have not been classified as either OPLL or OLF.
Our results suggest that obesity is associated with the severity of spinal ligament ossification in thoracic OLF. This was supported by a positive correlation between BMI values and the thoracic OLF index and the results of multiple regression analysis. A more interesting finding was that the severity of ossification of the ligamentum flavum in multilevel thoracic OLF was more severely affected than in thoracic OLF combined with OPLL (Figure 3A). Similar to earlier studies of thoracic OPLL,15,16 patients with a high BMI had multiple levels of thoracic OLF. Considering the fact of the high prevalence of OLF in OPLL,10-14 our results showed that thoracic OLF shared many clinical features with thoracic OPLL. Given that the average BMI of the general Japanese population is 21 kg/m2 (men, 21.83 kg/m2; women, 21.20 kg/m2) and that of the control group in this study was 23.2 kg/m2 (men, 22.4 kg/m2; women, 24.3 kg/m2), 19 it is possible that patients with thoracic OLF and BMI > 30 kg/m2 have a genetic predisposition to obesity.
Multiple regression analysis also revealed age and coexistence of cervical OPLL and lumbar OLF as other independent risk factors for the severity of thoracic OLF. It has been reported that ossified lesions of OLF increase with aging,3,4 which is consistent with our results. The presence or absence of lumbar OLF has not been reported to affect the severity of thoracic OLF. The distribution of OLF is 0.3% in the lumbar spine and negligible in the cervical spine.13,23,24 In this study, 29.4% of patients with multilevel thoracic OLF had lumbar OLF (Table 2), and the severity of lumbar OLF was elevated as mean BMI increased (Figure 3E). The ossification tendency of the entire spine contributes to the development of OLF. Our results also supported that of a previous report, suggesting that the degree of obesity might contribute to the severity of OLF of the entire spine.
It should be emphasized that single-level or double-level localized thoracic OLF was less associated with obesity and did not reflect the ossification tendency of the entire spine. In a situation where the clinical background of OLF was not clearly distinguished, the finding that the characteristics of localized thoracic OLF and multilevel thoracic OLF were markedly different was very important. The fact that large numbers of OLF exist in the lower thoracic spine suggest that spinal rotation and local instability may be involved in the development of OLF and the increase in ossification lesions.13,23-25 In the present study, the highest incidence of OLF, 65.0%, in patients with localized thoracic OLF was at T10-11-12 (data not shown), which was consistent with previous reports.4,5 OLF may originate from different mechanisms: local mechanical stimulation and the effects of humoral factors on systemic bone metabolism.
There were some limitations to this study. First, because the study was a cross-sectional study and we were unable to collect age and BMI data at the onset of symptoms, we could not conclude whether severe obesity was the cause or consequence of thoracic OLF. Long-term or experimental animal model studies are needed to reach conclusions. Second, because OLF patients are rare, the sample size was small, and the statistical power was low. In the future, our findings should be validated in multicenter and nationwide studies.
In summary, this study showed that patients with multiple levels of thoracic OLF were characterized by a higher prevalence of severe obesity than those with local levels of thoracic OLF. The degree of obesity was also associated with the severity of OLF, which warrants further investigations to elucidate this causal relationship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.