
Abstract
Purpose
The objective of this study was to clarify the characteristics of immediate neurological deterioration (ND) after ambulation and its potential preventative measures using multi-rod reinforcement during posterior decompression and fusion (PDF) with instrumentation for thoracic ossification of the posterior longitudinal ligament (T-OPLL).
Methods
Study 1: Fifteen patients with T-OPLL who underwent PDF before 2020 were included. Demographic, radiographic, intraoperative, and postoperative data were compared between the 6 patients with ND and 9 patients without ND after ambulation. Study 2: The primary (incidence of ND after ambulation) and the secondary (postoperative hospital stay) outcomes were compared between 15 patients with a multi-rod construct since 2020 (multi-rod group) and 15 patients with a dual-rod construct before 2020 (dual-rod group; patients who were indicated in study 1).
Results
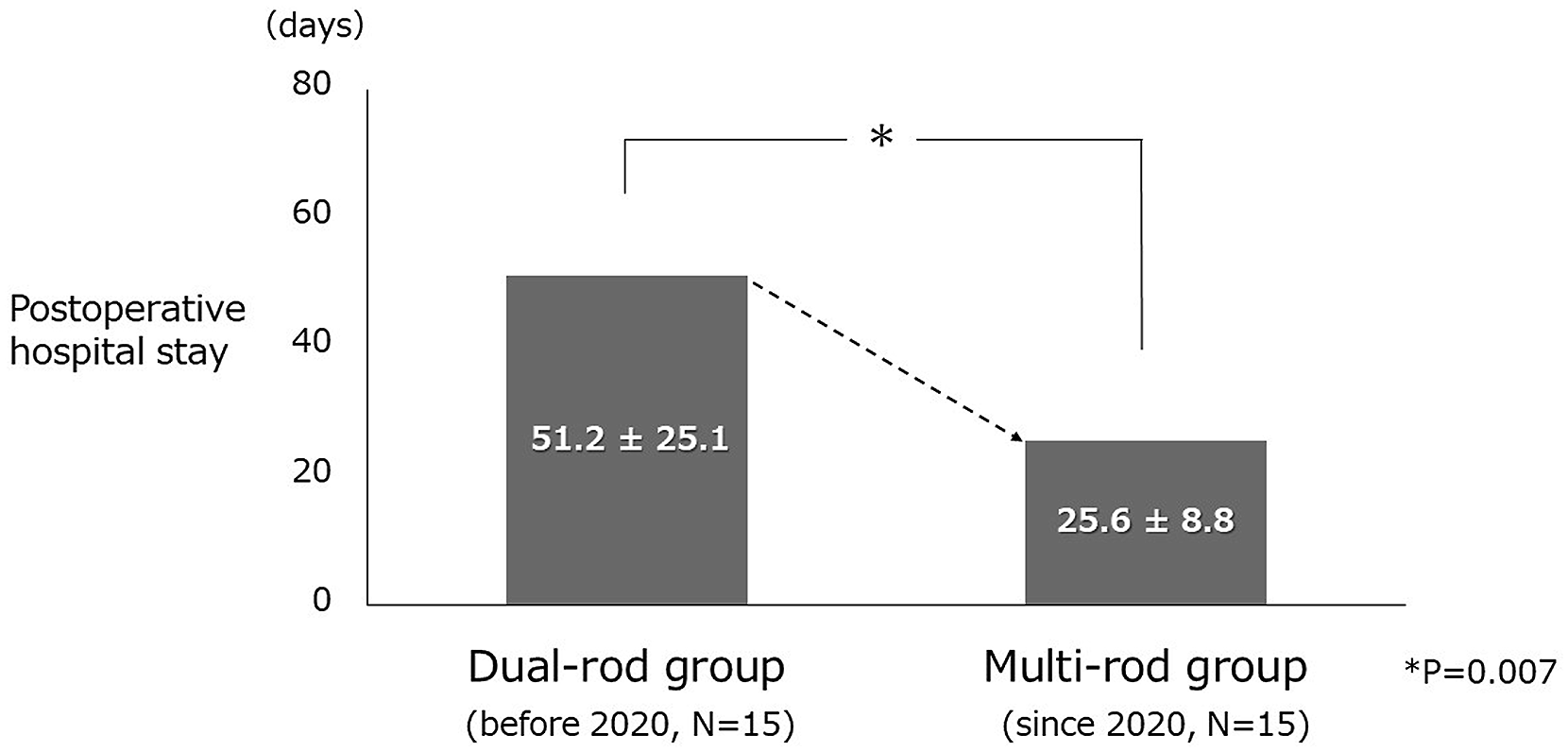
Study 1: ND after ambulation tends to occur only in the upper or middle thoracic spine. The mean maximum OPLL occupation ratio was significantly different between the groups (ND vs non-ND, 67.7% vs 53.4%; p = .021). Study 2: The incidence of ND after ambulation (dual-rod vs multi-rod, 40% vs 6.7%; p = .040) and the mean duration of the postoperative hospital stay (dual-rod vs multi-rod, 51.2 days vs 25.6 days; p = .007) were significantly different between the groups.
Conclusions
Immediate ND after ambulation occurs in the upper or middle thoracic spine, and a higher maximum OPLL occupation ratio is a significant risk factor. Multi-rod reinforcement can reduce its incidence, regardless of maximum OPLL occupation ratio, and duration of postoperative hospital stay, which could be a potential preventative measure.
Keywords
Introduction
Posterior decompression and fusion (PDF) with instrumentation for thoracic ossification of the posterior longitudinal ligament (T-OPLL) was first reported in 2006 1 as a surgical technique to prevent postoperative paralysis after laminectomy alone. Since then, PDF with instrumentation has become widely popular as a surgical method that provides stable postoperative outcomes in the short- to medium term 2 and medium- to long term. 3 In a recent nationwide survey, 4 PDF with instrumentation was performed in 73.9% of cases of T-OPLL and is currently adopted as the standard surgical procedure 5 at many institutions.
Postoperative motor paralysis of the lower limbs is the most common and major complication of T-OPLL. 4 Among these, immediate neurological deterioration (ND) after ambulation is a rare and unique postoperative complication.6–8 It occurs immediately upon sitting or standing 2 or 3 days post-surgery but shows immediate recovery after bed rest. The preoperative characteristics of the cases in which this complication occurs remain unknown. In contrast, insufficient fixation force has been reported to be a possible contributing factor of this complication.6,8 Since 2020, we have attempted to strengthen instrumentation by using multi-rod constructs bridging the decompressed spinal levels in all surgical cases of T-OPLL to prevent this complication. However, its effectiveness has not yet been investigated.
This single-center, retrospective study aimed to identify the preoperative characteristics of cases in which ND occurred immediately after ambulation in patients undergoing PDF with instrumentation for T-OPLL. We conducted this study to clarify these characteristics and to evaluate the effectiveness of multi-rod reinforcement as a preventive measure, with the goal of enhancing surgical safety for T-OPLL.
Materials and methods
Between January 2013 and December 2023, 33 consecutive patients with T-OPLL underwent PDF with instrumentation (Figure 1), following our uniform surgical procedures. The surgical procedure was as follows. Pedicle screws were inserted into each of the minimum three vertebral bodies, cranially and caudally, across the spinal levels responsible for thoracic myelopathy for fixation. The fixed range was expanded based on the OPLL range. Wide laminectomy, including resection of the medial bilateral pedicle and ossification of the ligamentum flavum (OLF) was carefully performed to a sufficient extent at the spinal level responsible for the thoracic myelopathy1,2 with skipped pedicle screw insertion under temporary rod fixation and transcranial motor-evoked potential monitoring. In principle, the spinal fixation was performed in situ1,2,9 with the alignment obtained in the prone position using dual-rod construct with a diameter of ≧6.0 mm in the T-OPLL segments. No additional procedures, such as kyphosis correction10–12 or anterior spinal cord decompression using the posterior approach13–16 was performed. Images of a representative case are shown in Figure 2. In all cases, the surgical procedure was decided by the chief of the spine surgery unit during the preoperative conference. All surgeons approved the decision. Flow diagram for the study sample selection. Images of a representative case with a dual-rod construct in study 1. Plain CT showing thoracic OPLL at T1-T3 and T6-T8 (a). The MRI reveals that the spinal level responsible for the thoracic myelopathy is T7/8 (b). PDF with instrumentation with a dual-rod construct at C7-T11, including wide laminectomy at T6-T8 is performed (c and d). No additional rods were used prior to 2020. CT: computed tomography; OPLL: ossification of the posterior longitudinal ligament; MRI: magnetic resonance imaging; PDF: posterior decompression and fusion.

We retrospectively collected patient demographic factors, including age, sex, height, body weight, body mass index, presence or absence of diabetes mellitus as a frequent comorbidity, hemoglobin A1c level, walking ability, and Japanese Orthopaedic Association (JOA) scores. We evaluated the JOA scores for cervical myelopathy, excluding scores for the upper extremities (maximum score: 11 points). 17 We also collected radiographic factors, including the spinal levels responsible for thoracic myelopathy (“upper” for T1–T4, “middle” for T5–T8, and “lower” for T9–T12), 4 which were considered based on physical examination and magnetic resonance imaging (MRI) findings; presence or absence of beak-type OPLL; maximum OPLL occupation ratio of the responsible spinal level of thoracic myelopathy, which was defined as the greatest thickness of OPLL divided by the antero-posterior diameter of the bony spinal canal on a preoperative axial computed tomography (CT) image; 18 local ossification angle, which was defined as the medial angle at the intersection between a line from the superior posterior margin at the cranial vertebral body of maximum OPLL to the top of OPLL with beak type and a line from the lower posterior margin at the caudal vertebral body of the maximum OPLL to the top of OPLL with beak type. 19 Moreover, we collected intraoperative factors including operative time, estimated blood loss, presence or absence of OLF at laminectomy levels, visible or invisible of preincisional waveform of motor-evoked potential monitoring in the lower limb, presence or absence of incidental dural tear, numbers of instrumented intervertebral levels, numbers of vertebrae with skipped pedicle screws, rod material, and postoperative factor including the duration of postoperative hospital stay.
A comprehensive agreement for academic use of patient information, such as type of treatments, treatment progress or any other data acquired during their treatments was obtained from the patients by the hospital at the time of their hospitalization, and no identifiable information of the participants is included in the manuscript.
Study 1. Characteristics of immediate neurological deterioration after ambulation
Before 2020, 18 consecutive patients with T-OPLL underwent PDF with instrumentation. Among these, three patients who underwent additional emergency surgery before starting ambulation due to postoperative massive epidural hematoma were excluded. Fifteen patients were included in this study (Figure 1). Six board-certified spine surgeons were involved in study 1.
Immediate ND after ambulation occurred in 6 of 15 cases (40.0%). All patients showed manual muscle testing of the lower limbs aggravated by >1 grade while sitting or standing, and motor weakness rapidly improved when lying down. According to previous methodology,6,7 all six patients were instructed to continue bed rest for 3 weeks. To elucidate the factors that significantly influenced immediate ND after ambulation, univariable analyses were conducted between the six patients who experienced it (ND group) and the other nine patients who did not experience it (non-ND group). We compared all the factors described above. Furthermore, in the ND group, the presence or absence of massive epidural hematoma on T2-weighted MRI at the time of the incidence and the outcomes of 3-week bed rest after the incidence were investigated. Finally, the JOA score at 2-year follow up and the recovery rate were evaluated. The recovery rate was calculated using Hirabayashi’s method,
20
which was modified for thoracic myelopathy (
Study 2. Effectiveness of multi-rod reinforcement
Since 2020, multi-rod reinforcement was used in all 15 consecutive surgical cases of T-OPLL. Among these, two patients were previously operated on for T-OPLL in different thoracic spinal segments. In both cases, the spinal level responsible for thoracic myelopathy was separated from two or more spinal levels of the uppermost or lowest instrumented vertebrae.
We performed multi-rod reinforcement using at least one additional rod between the bilateral main rods to bridge the decompressed spinal levels, which are responsible for thoracic myelopathy due to T-OPLL, and fixed them to the main rods using lateral connectors in all cases. No other surgical procedures or decision process were changed. Images of a representative case are shown in Figure 3. Seven board certified spine surgeons were involved in study 2. Images of a representative case with a multi-rod construct in study 2. Plain CT showing the thoracic OPLL at T5-T10 (a). The MRI reveals that the spinal level responsible for the thoracic myelopathy is T7/8 (b). PDF with instrumentation at T4-T12, including wide laminectomy at T6-T8 was performed (c and d). Since 2020, at least one additional rod (arrow heads) has been fixed between the bilateral main rods in all cases to bridge the decompressed spinal levels using lateral connectors (arrows) to create a multi-rod construct.
To evaluate the preliminary results of the multi-rod reinforcement, univariable analyses were conducted between the 15 cases since 2020, which used a multi-rod construct (multi-rod group), and the 15 cases included in study 1 with a dual-rod construct before 2020 (dual-rod group) as the historical control (Figure 1). We compared the incidence of immediate ND after ambulation as the primary outcome and the duration of postoperative hospital stay as the secondary outcome. We also compared the same data, including the patient demographic, radiographic, and intraoperative factors described in study 1. Furthermore, the diameter, material, and numbers of additional rods in the multi-rod group were investigated. Finally, postoperative complications except for immediate ND after ambulation were investigated in both groups.
Statistical analyses
Student’s t test and Mann–Whitney U test were used to compare parametric and non-parametric data, respectively. The chi-square and Fisher’s exact tests were used for categorical data. All statistical analyses were performed using EZR software (version 1.3.0; Saitama Medical Center, Jichi Medical University). 21 p values < .05 were considered statistically significant.
Results
Study 1
Demographic and radiographic factors in study 1.

Note. Data are presented as the mean and the standard deviation or as the number of patients. ND: neurological deterioration; BMI: body mass index; DM: diabetes mellitus; Hb: hemoglobin; JOA: Japanese Orthopaedic Association; OPLL: ossification of the posterior longitudinal ligament. p Values were determined using the student’s t test, Mann–Whitney U test, and Fisher’s exact test. The level of significance (*) was set at p < .05.
Intraoperative and postoperative factors of study 1.

Note. Data are presented as the mean and the standard deviation or as the number of patients. ND: neurological deterioration; OLF: ossification of the ligamentum flavum; MEP: motor-evoked potential; PS: pedicle screws; JOA: Japanese Orthopaedic Association. p Values were determined using the Mann–Whitney U test and Fisher’s exact test. The level of significance (*) was set at p < .05.
Study 2
Regarding the primary outcome, the incidence of immediate ND after ambulation was significantly different between the groups (dual-rod vs multi-rod, 6 [40.0%] vs 1 [6.7%] out of 15 cases respectively, p = .040, Figure 4). Regarding the secondary outcome, the mean duration of postoperative hospital stay was significantly different between the groups (dual-rod vs multi-rod groups, 51.2 ± 25.1 vs and 25.6 ± 8.8 days, p = .007, Figure 5). Incidence of immediate neurological deterioration after ambulation. This is the primary outcome of study 2. In the dual-rod (before 2020, N = 15) and the muti-rod (since 2020, N = 15) groups, there are 6 cases (40.0%) and one case (6.7%) of the incidence, respectively. According to the Fisher’s exact test, there is a significant difference between the 2 groups (p = .040). Postoperative hospital stay. This is the secondary outcome of study 2. The mean duration of postoperative hospital stay in the dual-rod (before 2020, N = 15) and the multi-rod (since 2020, N = 15) groups were 51.2 ± 25.1 days and 25.6 ± 8.8 days, respectively. According to the Mann–Whitney U test, there is a significant difference between the two groups (p = .007).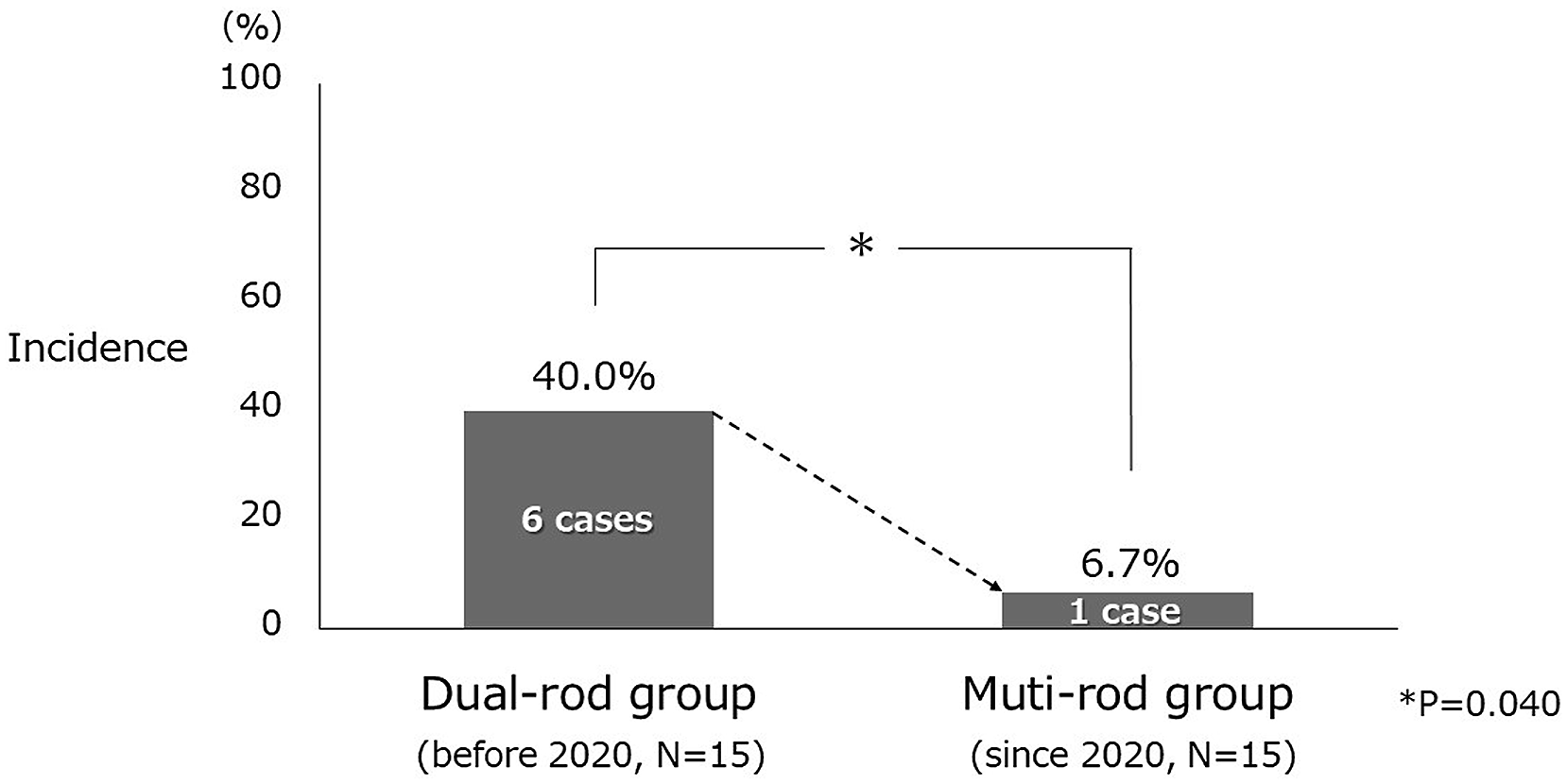
Demographic and radiographic factors in study 2.

Note. Data are presented as the mean and the standard deviation or as the number of patients. BMI: body mass index; DM: diabetes mellitus; Hb: hemoglobin; JOA: Japanese Orthopaedic Association; OPLL: ossification of the posterior longitudinal ligament. p Values were determined using the student’s t test, Mann-Whitney U test, chi-square test, and Fisher’s exact test. The level of significance (*) was set at p < .05.
Intraoperative factors and postoperative complications except for the immediate neurological deterioration after ambulation in study 2

Note. Data are presented as the mean and the standard deviation or as the number of patients. OLF: ossification of the ligamentum flavum; MEP: motor-evoked potential; CSF: cerebrospinal fluid. p Values were determined using the Mann–Whitney U test, chi-square test, and Fisher’s exact test. The level of significance (*) was set at p < .05.
Discussion
The largest multicenter study to date reported an incidence of motor paralysis after surgery for T-OPLL of 32.2%. 4 The incidence of immediate ND after ambulation in the current study 1 with a dual-rod construct before 2020 was 40.0% (6 of 15 cases), which was relatively high compared with the previous report. In this study, ND was defined as motor paralysis occurring immediately upon sitting or standing 2 or 3 days after surgery, with immediate recovery after bed rest. Following highly invasive surgery, such as posterior decompression and fusion with long-level spinal instrumentation for T-OPLL, for some cases, early ambulation may be delayed owing to patients’ postoperative general condition. Such cases may not have been identified as ND in the previous study, which may explain the relatively high incidence observed in the present study.
The findings of study 1 revealed the characteristics of immediate ND after ambulation in patients undergoing PDF with instrumentation for T-OPLL. This event tends to occur in the upper or middle thoracic spine, and a higher maximum OPLL occupation ratio is a significant risk factor. Once this event occurred, a 3-week bed rest with limited ambulation resulted in a significantly prolonged postoperative hospital stay. These findings are novel, as no similar studies have been previously reported. As insufficient fixation force has been reported to be a possible contributing factor to this complication,6,8 it was considered that when the patient begins to assume a sitting or standing position, the weight of the upper body is applied, which causes the rod to deflect slightly and increases kyphosis, which aggravates the compression on the spinal cord due to the ossified lesion with higher maximum OPLL ratio and causes neurological deterioration.
The findings of study 2 revealed a potential preventative measure for immediate ND after ambulation in patients undergoing PDF with instrumentation for T-OPLL. The comparative study of the two groups, for which no differences were observed in demographic and radiographic factors, including maximum OPLL occupation rate, which is a risk factor obtained from study 1, multi-rod reinforcement using one or two additional rods significantly reduced the incidence of this complication and also significantly reduced the duration of postoperative hospital stay without increasing other complications. These are also novel findings, as no similar studies have been reported before.
Postoperative paralysis after posterior surgery for T-OPLL occurs more frequently in the upper and middle thoracic spine, and less frequently in the lower thoracic spine. 22 This is because the ossified lesion of T-OPLL is anterior to the spinal cord, and it is difficult to directly decompress the spinal cord using the posterior approach in the upper and middle thoracic spines with kyphotic alignment. Similarly, in the present study, immediate ND after ambulation occurred only in patients with upper and middle thoracic OPLL. Although beak-type T-OPLL 23 and higher local ossification angle 19 are both risk factors for postoperative paralysis, the present findings indicated that it occurred in cases with a higher maximum OPLL occupation ratio, rather than beak-type OPLL and local ossification angle. However, the beak-type OPLL was present in three of the six cases in the ND group. In contrast, in the non-ND group, the beak-type OPLL was present in only one of nine patients. Moreover, the local ossification angle tended to be higher in the ND than in the non-ND group. Therefore, although the difference was not significant, we believe that caution should be taken to prevent this event from occurring in cases of beak-type OPLL and higher local ossification angle. Furthermore, additional surgical procedures, such as anterior decompression and fusion, anterior spinal cord decompression using the posterior approach,13–16 and kyphosis correction,10–12 may be considered for patients at high-risk for T-OPLL.
Of the six patients in the ND group, three had massive epidural hematomas at the time of neurological deterioration. It has been reported that postoperative epidural hematoma associated with neurological deficit occurs most frequently in the thoracic spine; 24 therefore, epidural hematoma is thought to be one of the indirect causes of this event, but the details are unknown because postoperative MRI was not taken in the non-ND group. In addition, five of the six patients in the ND group experienced no recurrence after 3 weeks of bed rest. The instrumentation construct should remain mechanically unchanged, even after 3 weeks of bed rest. It is assumed that the spinal cord gradually recovered from its critical state and epidural hematoma was gradually absorbed after 3 weeks of bed rest. Moreover, biomechanical changes including spinal cord condition were also unknown, because follow-up MRI was not taken after 3 weeks of bed rest in the ND group. In any case, instructing patients to rest in bed for a limited duration is considered appropriate when immediately ND after ambulation occurs. However, it is desirable to prevent this complication, as it delays the resumption of rehabilitation and directly leads to prolonged hospital stay.
In long-range spinal fixation, multi-rod constructs reinforced with additional rods generally provide mechanically stronger fixation than dual-rod constructs. 25 It is thought that the reinforcement of the construct with additional rods stabilized the range of decompressed spinal levels, which are responsible for thoracic myelopathy due to T-OPLL, leading to more stabilization of the compressed spinal cord and a decrease in the incidence of this event. Regarding rod materials, cobalt-chrome is generally considered to have better strength than titanium alloy;26,27 however, in the present study, titanium alloy was used in more cases for the main rod in the multi-rod group. Nevertheless, the incidence of immediate ND after ambulation was reduced in the multi-rod group with additional rod reinforcement alone. Therefore, as suggested in previous reports,6,8 the primary cause of this event was thought to be insufficient fixation strength of the instrumentation at the spinal levels responsible for thoracic myelopathy due to massive T-OPLL.
Before starting this study, we had not performed PDF with instrumentation for T-OPLL. No changes were made to the technique or method other than additional rods in study 2. Therefore, the significantly shorter operative time in the multi-rod group in study 2 was thought to be due to our learning curve for PDF with instrumentation for T-OPLL. It was also thought that a trend toward reduced estimated blood loss was observed along with the reduction in operative time. As kyphosis correction or anterior decompression from the posterior approach was not performed in this study, bias due to the surgical methods was excluded. Therefore, the findings from the present studies, that is, multi-rod reinforcement using one or two additional rods can reduce the incidence of immediate ND after ambulation regardless of maximum OPLL occupation ratio, are clinically significant.
There are several methodological limitations in both studies. First, the numbers of patients included in both studies were limited. Multivariable analysis would normally be required to determine the risk factors for postoperative complications; however, due to the small number of cases in study 1, only univariable analyses were performed. Because this study strictly required unified surgical methods and procedures, it was difficult to conduct at multiple institutions. Furthermore, T-OPLL is much less common than cervical OPLL; 28 therefore, the number of cases was also limited in study 2. Second, radiographic angle measurements were not performed in either study. In T-OPLL surgery, the instrumentation often extends to the upper thoracic spine. However, the upper thoracic spine overlaps with the shoulder joint, making imaging difficult to read because X-rays cannot pass through it. Therefore, accurate radiographic angle measurements are difficult in the upper thoracic spine. In addition, preoperative radiographs are not taken in sitting or standing positions in patients who are unable to walk; body position during radiography is not standardized. Therefore, it is difficult to determine rod deflection or kyphotic changes using radiographic angle measurements. Third, biomechanical data on dual-rod constructs and multi-rod reinforcement in posterior T-OPLL surgery are lacking in study 2. Fourth, the postoperative follow-up period for patients with multi-rod reinforcement was short in study 2. Although caution should be taken when applying multi-rods and abuse should be avoided due to the preliminary results of study 2, we believe that multi-rod reinforcement could be a simple and useful preventative measure against this complication. In the future, a biomechanical study of multi-rod reinforcement with unified rod conditions for T-OPLL is necessary, and long-term follow-up of multi-rod reinforcement cases is mandatory.
Conclusions
Immediate neurological deterioration after ambulation tends to occur in the upper or middle thoracic spine in patients undergoing PDF with instrumentation for T-OPLL, and a higher maximum OPLL occupation ratio is a significant risk factor. Multi-rod reinforcement using one or two additional rods can reduce the incidence of this complication, regardless of maximum OPLL occupation ratio, and can also reduce the duration of postoperative hospital stay, which could be a potential preventative measure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Health Labour Sciences Research Grand (20FC1038).