
Abstract
Study Design
Retrospective observational study.
Objectives
To evaluate the long-term recurrence rates and functional status of patients with thoracic ossification of the posterior longitudinal ligament (OPLL) after decompression and posterior fusion surgery.
Methods
Thirty-seven consecutive patients who underwent posterior thoracic spine surgery at a single institution were retrospectively reviewed. The long-term neurological and functional outcomes of 25 patients who were followed up for ≥10 years after surgery were assessed. Factors associated with the recurrence of myelopathy were also analyzed.
Results
The mean preoperative Japanese Orthopaedic Association score was 3.7, which improved to 6.5 at postoperative year 2 and declined to 6.0 at a mean follow-up of 18 years. No patient experienced a relapse of myelopathy due to OPLL within the instrumented spinal segments. However, 15 (60%) patients experienced late neurological deterioration, 10 of whom had a relapse of myelopathy due to OPLL or ossification of the ligamentum flavum (OLF) in the region outside the primary operative lesion, while 4 developed myelopathy due to traumatic vertebral fracture of the ankylosed spine. Young age, a high body mass index, and lumbar OPLL are likely associated with late neurological deterioration.
Conclusions
Decompression and posterior instrumented fusion surgery is a reliable surgical procedure with stable long-term clinical outcomes for thoracic OPLL. However, as OPLL may progress through the spine, attention should be paid to the recurrence of paralysis due to OPLL or OLF in regions other than the primary operative lesion and vertebral fractures of the ankylosed spine after surgery for thoracic OPLL.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is a well-known cause of cervical myelopathy, especially in Asian populations, 1 and it also occurs less commonly in the thoracic spine.2,3 Since thoracic myelopathy secondary to OPLL is mostly progressive and does not respond to conservative treatment, surgical intervention is indicated once paralysis develops. However, removal of the entire ossified ligament is mostly impossible and should not be performed due to its technical difficulty and the associated high risk for spinal cord damage.4,5 Furthermore, an epidemiological study showed that patients with symptomatic thoracic OPLL are likely to have multiple ossified lesions over their entire spine.2,6 Hence, there is a possibility that any residual ossified tissue or newly developed OPLL can grow and cause spinal cord compression over a long period after surgery. 7 However, data on the long-term clinical outcomes and recurrence rates of neurological symptoms after surgery are scarce in the literature.8-10
We investigated the long-term clinical course of thoracic OPLL after decompression and posterior instrumented fusion surgery to elucidate whether residual OPLL or new OPLL lesions develop and lead to symptomatic spinal cord compression. This study highlights the need for continued follow-up in patients with T-OPLL, which may lead to the development of early treatment opportunities for relapse of myelopathy after thoracic spine surgery.
Materials and Methods
Study Design
This retrospective observational study included patients who underwent decompression and posterior instrumented fusion surgery for thoracic OPLL between 1992 and 2011 at a single institution. This study was approved by our institutional review board (# 022-0004) and conducted in accordance with the guidelines of the Declaration of Helsinki. The study was based on data obtained from medical records and imaging findings of 37 patients who underwent decompression and posterior instrumented fusion surgery for myelopathy caused by thoracic OPLL. The need for patient informed consent was waived due to the retrospective nature of the study and the deidentified data used.
Patients
Data of 37 patients with thoracic myelopathy secondary to thoracic OPLL who underwent decompression and posterior instrumented fusion surgery were extracted from the database of our hospital. The patients included 13 men and 24 women with a mean age at time of surgery of 54.9 (range 34-78) years. All patients presented with thoracic myelopathy secondary to thoracic OPLL with or without ossification of the ligamentum flavum (OLF) when thoracic decompression and posterior instrumented fusion surgery was performed.
Eight patients who were lost to follow-up within 10 years postoperatively were excluded from analyses. Four patients who were confirmed to have died within the 10-year follow-up period were also excluded from all analyses except the mortality analysis. Outcomes were therefore assessed in 25 patients who could be followed up for more than 10 years, including 20 surviving patients and 5 deceased patients at the time of investigation. Thus, the follow-up rate was 67.6%. The mean follow-up period was 16.3 (range 10-28) years for the 25 patients.
Operative Procedures
Laminectomy and instrumented posterior spine fusion was performed in all patients. The levels of spinal decompression were determined based on preoperative neurological status and imaging findings, including computed tomography (CT), magnetic resonance imaging (MRI), and myelography. For the management of OPLL, 29 of the 37 patients underwent an additional anterior decompression maneuver using a posterior approach, according to Otsuka et al.4,11 The requirement for anterior decompression was determined according to the type (beak-type) and size of the OPLL. Spinal instrumentation was used in all patients. Patients who underwent laminectomy and instrumented posterior spine fusion were classified into the posterior decompression and fusion (PDF) group and those who underwent PDF and anterior decompression through a posterior approach into posterior circumferential decompression and fusion (PCDF) groups. During the spinal instrumentation, 2 vertebrae, each above and below the decompressed vertebrae, were basically anchored with pedicle screws or hooks and connected by a 5.5 mm diameter titanium rod. In the case of long-segment fixation, we often additionally placed anchors in the middle of the fixation range. In case the pedicles were anatomically too narrow to safely insert a pedicle screw, it was omitted or anchored with hooks. Especially in cases operated on before the 2000s, the use of thoracic pedicle screws tended to be minimized, and hooks were used in combination.
Clinical Evaluation
Hospital and attendance records of all patients were reviewed to determine their demographic data, neurological examination, imaging findings, surgical reports, and follow-up data. The Japanese Orthopaedic Association (JOA) score was used to assess physical and neurological dysfunction. The JOA score for cervical myelopathy (maximum of 17 points) was modified to exclude the assessment of upper extremity function (reduced to a maximum of 11 points) and used to evaluate neurologic deficits in each patient. The neurologic recovery rate was calculated using the preoperative JOA score and the JOA score at the follow-up, according to the following formula; Recovery rate = (JOA score at follow-up − preoperative JOA score)/(11 − preoperative JOA score) × 100 (%). The Nurick grading system was used to assess ambulatory function.
Late neurological deterioration experienced by any patient was evaluated for its cause during the postoperative follow-up period and defined as a decrease in the JOA score by 1 or more points during the postoperative period from week 4 to the final follow-up. Additional spine surgeries for late neurological deterioration and neurological recovery after surgery were investigated from medical records.
Each patient underwent CT scanning and MRI both before surgery and when paralysis recurred. Some patients underwent repeat whole-spine CT examinations at 3- to 5-year intervals to assess the progression of ossification of lesions and the appearance of new lesions over the entire spine.
Late complications associated with surgery, additional spine surgery during the postoperative follow-up period, mortality, and causes of death were reviewed from medical records.
Statistical Analysis
JMP Pro version 15 (SAS Institute Inc, Cary, NC, USA) was used for statistical analyses. The differences in the measured variables between the late neurological deterioration vs non-deterioration groups, the long-term preservation of neurological function vs non-preservation groups, and PDF vs PCDF groups were analyzed using Student’s t-test or Fisher’s exact test, as appropriate. The selection of priori variables was based on previous literature and their clinical importance. Univariate analysis using the Kaplan-Meier method combined with log-rank statistical analysis was performed to test for group differences in survival. A P value <.05 was considered significant.
Results
Baseline Characteristics of the Study Participants
The 25 patients who were finally observed for more than 10 years after decompression and posterior instrumented fusion surgery included 9 men and 16 women, with an average age of 52.5 ± 10.4 years at the time of surgery. The mean follow-up period was 17.8 years, ranging from 10 to 29 years. The main preoperative symptoms were vague back pain, myelopathy presenting with paresis of the lower limbs, and urinary disturbances. The mean preoperative Nurick score was 4.1. Of the 25 patients, 5 (20%) were unable to walk when they were admitted (Nurick score 5), and 17 (68%) were unable to walk without help or the aid of a frame (Nurick score 4). Twelve patients had cervical OPLL, and 4 of them had undergone cervical laminoplasty before the thoracic operation. Nine patients had lumbar OPLL and/or OLF, and 3 of them had undergone lumbar decompression surgery before the thoracic operation.
Long-Term Neurologic Outcomes
The mean preoperative JOA score of the 25 patients was 3.7 ± 1.5, and it improved to 5.3 ± 1.5 at postoperative week 4, then to 6.5 ± 2.5 at postoperative year 2, before declining to 6.0 ± 2.6 at the final follow-up (Figure 1). The average neurologic recovery rate was 23% at postoperative week 4, 38% at postoperative year 2, and 31% at the last follow-up. Most patients had residual paralysis; however, their neurological condition at 2 years after surgery appeared to be unchanged at the last follow-up (an average of 16.3 years postoperatively). However, 15 (60%) patients experienced late neurological deterioration during the postoperative follow-up period, from 4 weeks after surgery to the last follow-up. In 8 of the 15 patients, neurological function recovered to the pre-deterioration level after additional posterior decompression with or without spinal fusion surgery, whereas the remaining 7 patients showed partial recovery after additional surgery (their neurological function did not improve to the pre-deterioration level). Long-term neurologic outcome before and after posterior decompression and fusion surgery for myelopathy caused by thoracic OPLL. A) JOA scores for thoracic myelopathy. B) Lower extremity motor function score of the JOA score. C) Sphincter function of the JOA score. D) Nurick grade as an ambulatory function. OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association.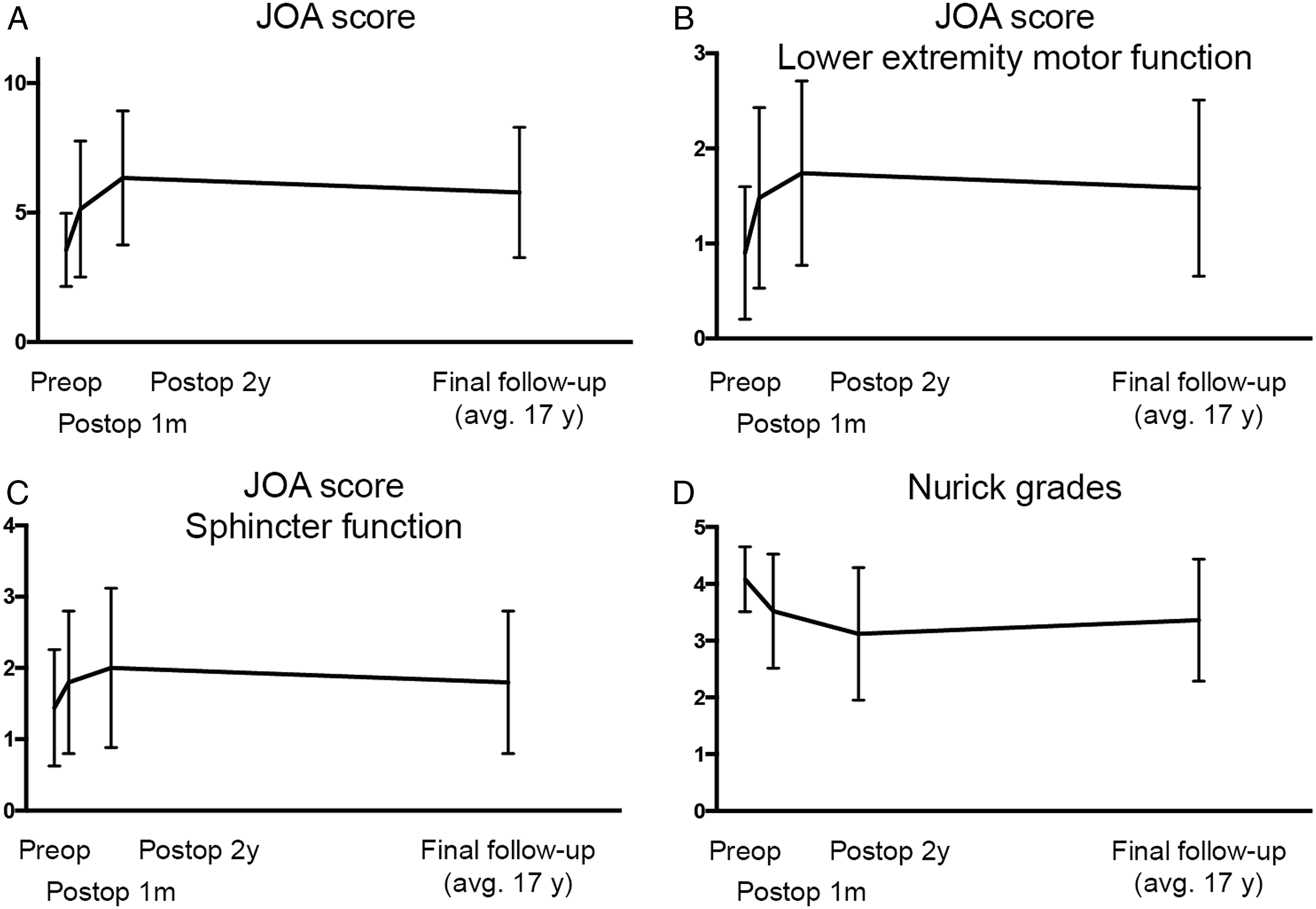
In this case series, 7 patients (28%) showed some neurological deterioration immediately after the primary thoracic surgery. Three of them recovered to preoperative levels or better within the first postoperative month, and their neurological condition was maintained until the last follow-up, except for 1 case who experienced late neurological deterioration due to cervical myelopathy caused by cervical OPLL during the postoperative course. In 1 of 7 patients, paralysis did not improve to the preoperative level at 1 month postoperatively but then gradually improved to more than the preoperative level during the second postoperative year and was maintained until the final follow-up. The remaining 3 never recovered to the preoperative level until the final follow up.
Causes of Late Neurological Deterioration
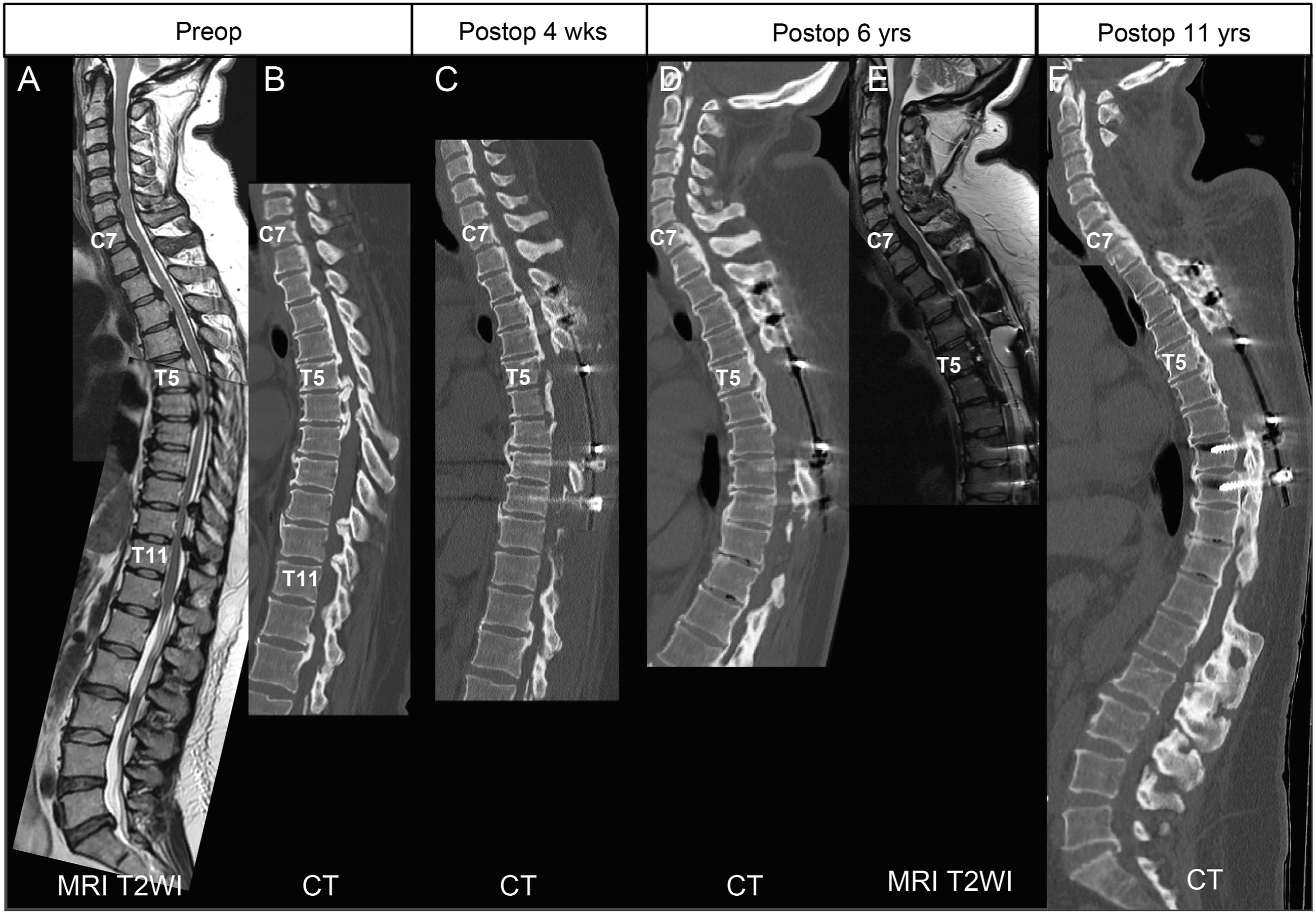
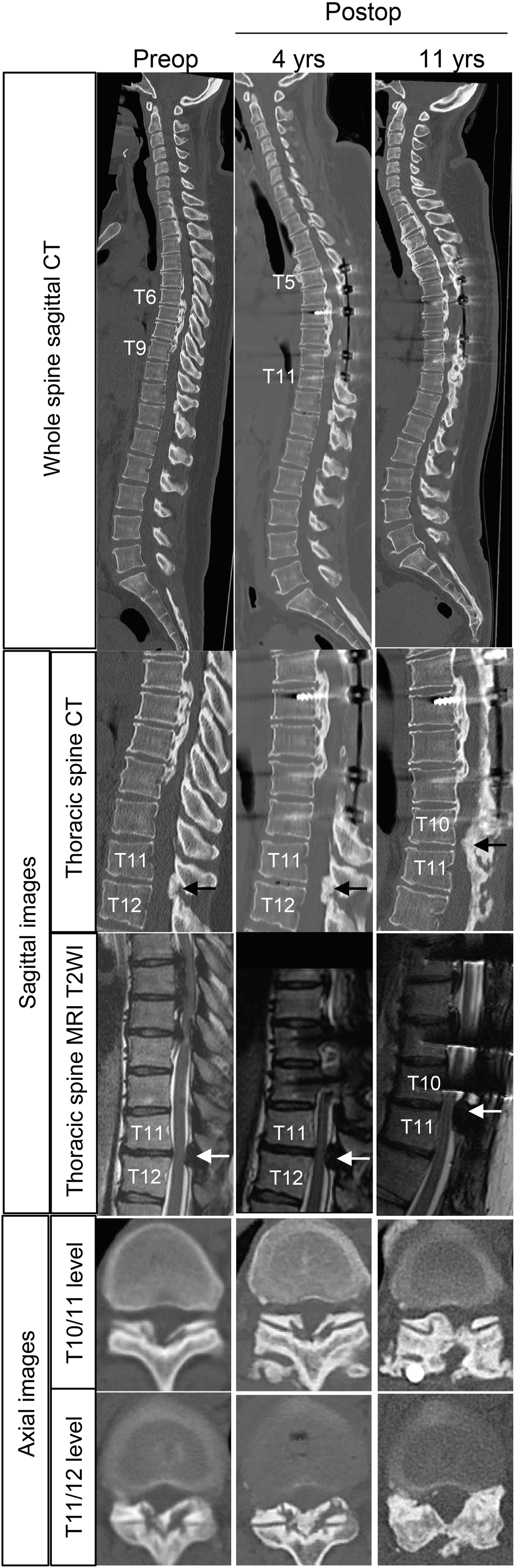
The causes of late neurological deterioration and the times of onset are shown in Figure 2. Although no patient experienced a relapse of myelopathy due to recurrence of OPLL within the instrumented spinal fusion segments, some patients developed myelopathy or cauda equina syndrome in regions outside of the operative segments. Among the 15 patients who developed late neurological deterioration after PDF surgery for thoracic OPLL, 11 developed myelopathy and/or cauda equina syndrome due to OPLL or OLF in regions other than the instrumented spinal fusion segments (Figure 3). In 2 of the 11 patients, neurological deterioration was caused by thoracic OLF at the adjacent segment caudal to the instrumented fusion level (Figure 4). Surgical treatment was performed for 13 spinal lesions in the 11 patients, and neurological function successfully recovered to pre-deterioration levels in 8 of the 11 patients. Three additional surgeries were performed within the first postoperative year, whereas the remaining 10 additional surgeries were performed at a median of 6 (range 4-10) years postoperatively. The causes of late neurological deterioration and the timing of their onset during the postoperative course after PDF surgery in 25 cases with thoracic OPLL who were finally followed-up for at least 10 years. OPLL, ossification of the posterior longitudinal ligament; PDF, posterior decompression and fusion. A representative case of a 55-year-old woman with relapsed myelopathy caused by cervical OPLL, 6 years after thoracic surgery. (A, B) Preoperative images show thoracic OPLL (T5-8) and OLF (T10-12) compressing the spinal cord. C) She underwent posterior decompression and fusion (PDF) surgery for thoracic OPLL and OLF with floating of the OPLL (T5-7). (D, E) At postoperative year 6, she developed cervical myelopathy due to enlarged OPLL in the cervical and upper thoracic spine and underwent C4-T1 laminoplasty. F) Postoperative 11 years images showing no progression of OPLL but showing progression of thoracic kyphosis. OPLL, ossification of the posterior longitudinal ligament; OLF, ossification of the ligamentum flavum; PDF, posterior decompression and fusion. A representative case of a 38-year-old woman with relapsed myelopathy caused by OLF at the level adjacent to the posterior instrumented spinal fusion for thoracic OPLL. Preoperative images show T6-9 OPLL compressing the spinal cord. She underwent PDF surgery with T5-T10 pedicle screw instrumentation. She presented with a relapse of myelopathy at postoperative year 4 due to progression of OLF at T11-12 and underwent posterior decompression surgery. Images at postoperative year 11 show progression of OLF at T10-11. OPLL, ossification of the posterior longitudinal ligament; OLF, ossification of the ligamentum flavum.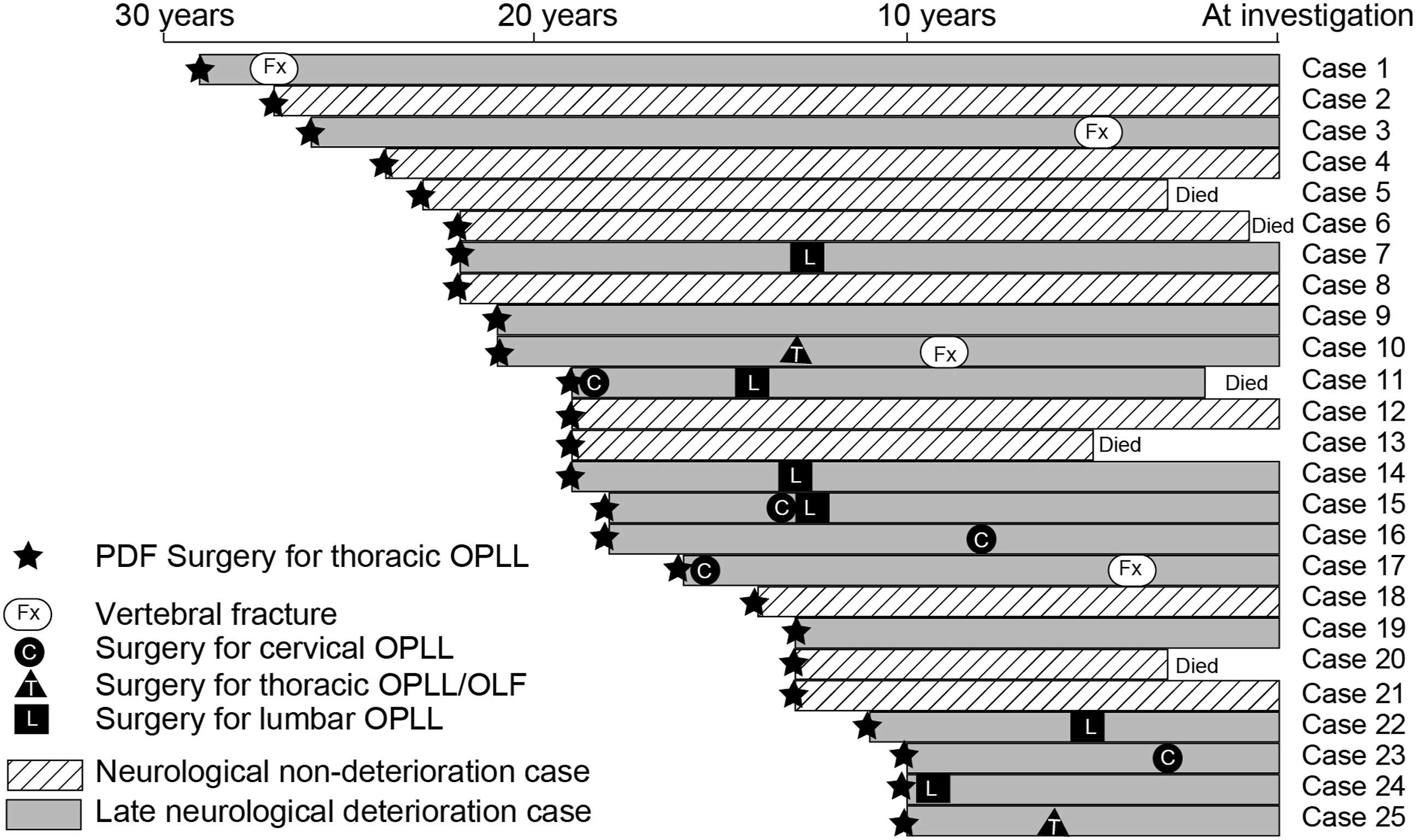
Four of the 15 patients who developed late neurological deterioration had worsened neurological function following traumatic vertebral fractures; 1 of them had a cervical spine fracture at postoperative year 12, while the other 3 had a thoracic spine fracture at postoperative week 5, postoperative year 12, and postoperative year 21, respectively. All 4 vertebral fractures occurred within the ankylosed segments of the spine (Figure 5). Three of the 4 patients underwent posterior decompression and fusion, while 1 patient received brace treatment. Bone union was achieved in all 4 patients; however, neurological function only showed partial recovery and did not improve to the pre-worsening level. A representative case of a 41-year-old man that developed late neurological deterioration caused by a thoracic vertebral fracture of the ankylosed spine due to falling at 12 years after the thoracic PDF surgery. He underwent posterior decompression and instrumented fusion surgery for thoracic myelopathy caused by OPLL, followed by cervical laminoplasty for cervical OPLL. He also underwent posterior decompression surgery for lumbar canal stenosis caused by OPLL. His middle and lower thoracic spine was spontaneously fused at 10 years after the thoracic PDF surgery (A). At 12 years after the thoracic PDF surgery, a reverse Chance fracture at the T11 vertebra occurs after falling (B, C, D). Fracture heals spontaneously after 6 months of brace treatment (E). OPLL, ossification of the posterior longitudinal ligament; PDF, posterior decompression and fusion.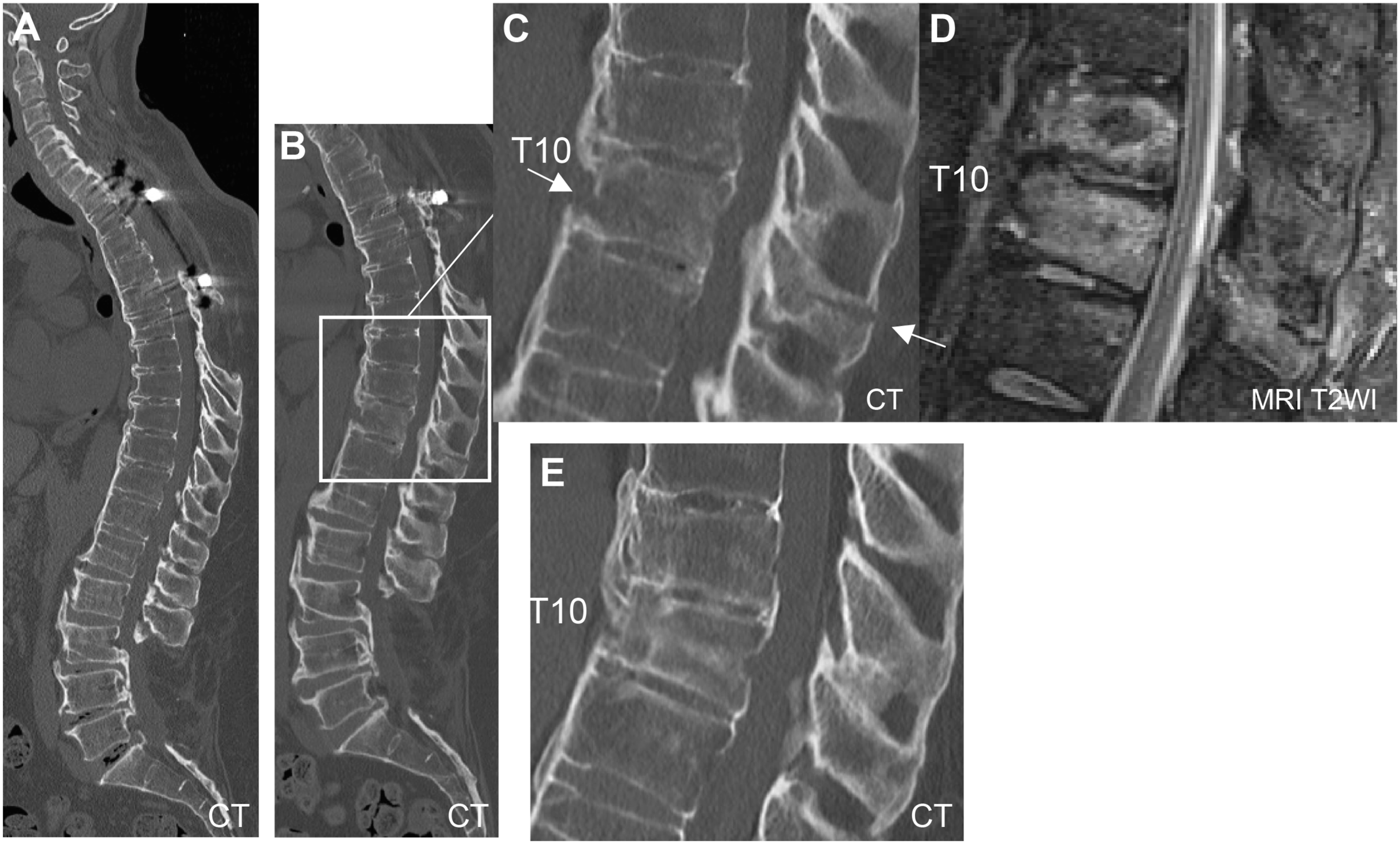
Ambulatory function gradually worsened in 2 of the 15 patients with late neurological deterioration during the follow-up period without evidence of OPLL progression or newly developed ossified lesions over the entire spine.
Other Late Complications of PDF Surgery
Two patients who opted to have spinal instrumentation removed due to deep wound infection showed progression of thoracic kyphosis. One developed chronic osteomyelitis due to Pseudomonas aeruginosa, which produced a purulent discharge from a fistula at the surgical site of the thoracic spine 21 years after the primary thoracic spine surgery. After debridement and irrigation surgery, a fracture of the ankylosed thoracic spine occurred from minimal trauma, resulting in neurological deterioration. This patient underwent posterior decompression and instrumented spine fusion; however, neurological function showed partial recovery and did not improve to the pre-worsening level (Figure 6). A case compelled to remove spinal instrumentation due to deep surgical site infection resulted in chronic osteomyelitis. At 21 years after the initial surgery, thoracic spinal infection flared up (A-C). Because of resistance to antibiotics therapy, surgical debridement for active infectious lesion, which was identified by PET-CT (C), was performed. At 2 weeks after surgical debridement, a T9 vertebral column fracture occurred (D). Because her paraplegia worsened, she underwent instrumented posterior fusion surgery (E). Bone union of T9 vertebra was achieved (D), but neurological function showed partial recovery. PET-CT, positron emission tomography/computed tomography.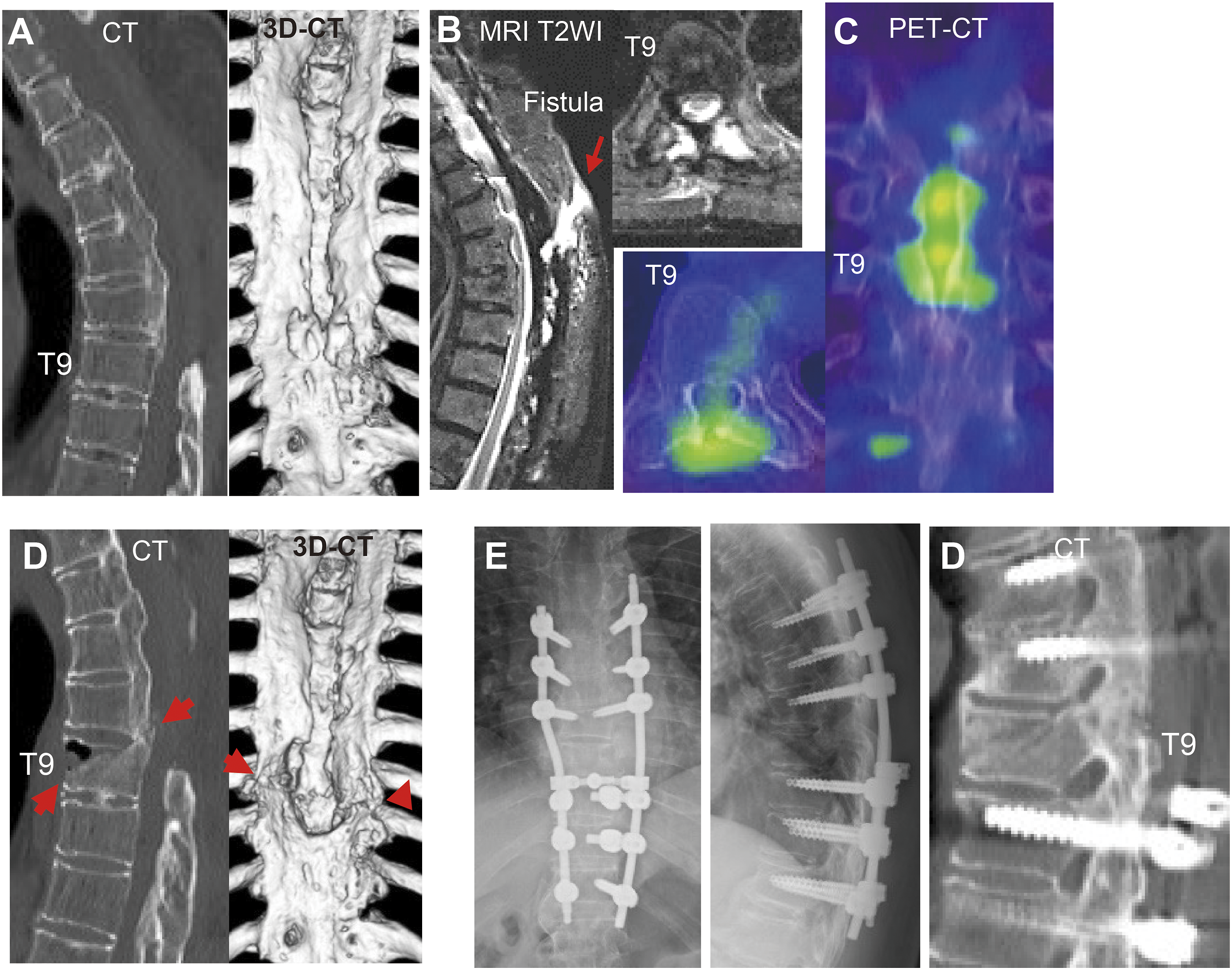
There were no implant-related complications until the last follow-up, except for the 2 cases of deep surgical site infection noted above. The number of spinal segments fused with spinal instrumentation varied from 4 to 10 (average and SD: 6.8± 2.1), and there was diversity in the types (pedicle screw or hooks), location, and number of spinal anchors; however, there were no cases of pseudoarthrosis or rod breakage.
Comparison of Characteristics Between the Late Neurological Deterioration and Non-deterioration Groups
Comparison of characteristic features of patients between the late neurological deterioration group and non-deterioration group.
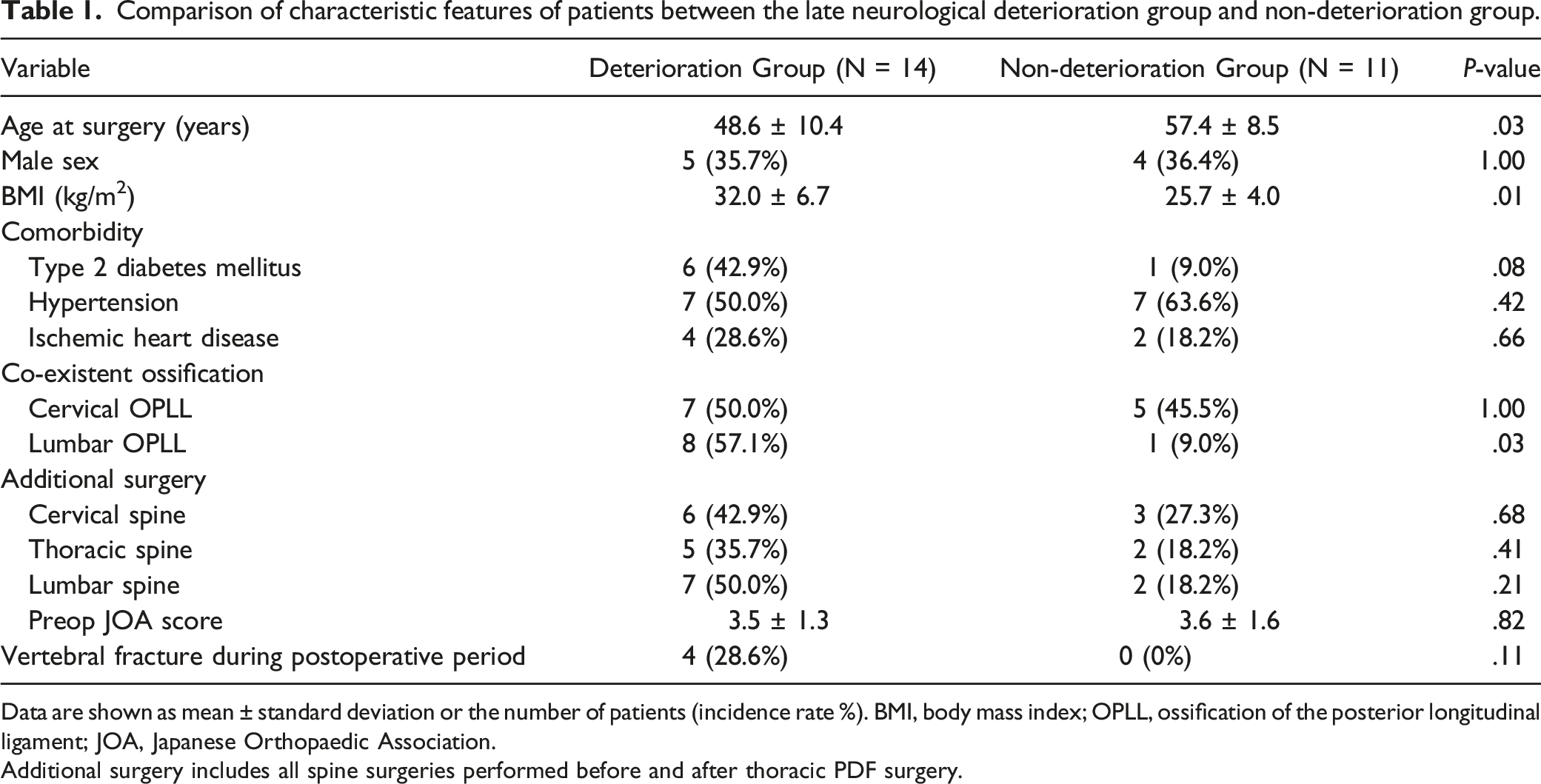
Data are shown as mean ± standard deviation or the number of patients (incidence rate %). BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association.
Additional surgery includes all spine surgeries performed before and after thoracic PDF surgery.
Comparison of Characteristics Between the Long-Term Preservation of Neurological Function Group and Non-preservation Group
Comparison of characteristic features of patients between the long-term preservation of neurological function group and non-preservation group.
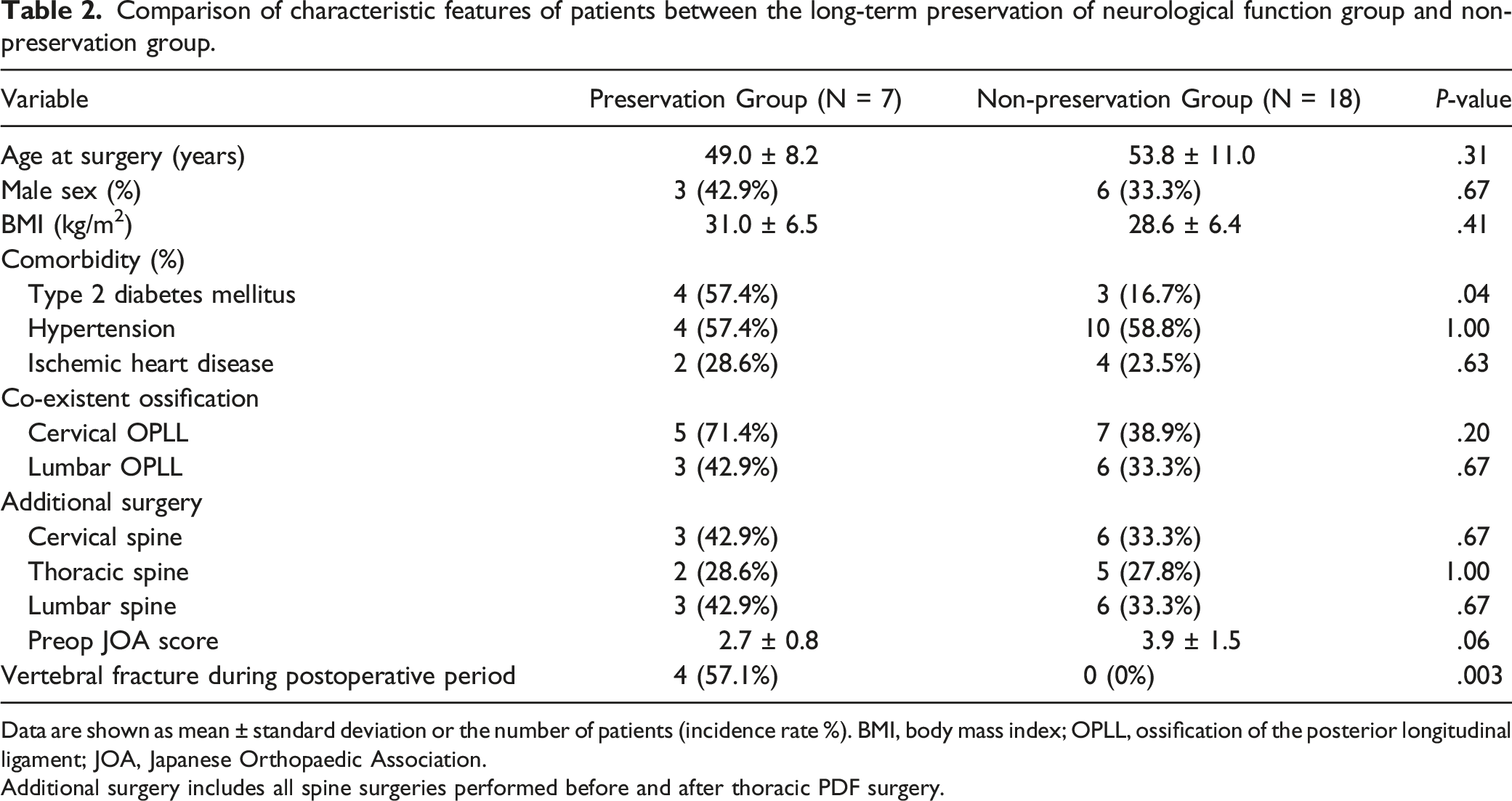
Data are shown as mean ± standard deviation or the number of patients (incidence rate %). BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association.
Additional surgery includes all spine surgeries performed before and after thoracic PDF surgery.
Long-Term Morphological Changes of Thoracic OPLL
There were no cases in which the size of the OPLL within the range of instrumented spine fusion segments increased by more than 3 mm in sagittal thickness and/or the longitudinal distance of the ossified mass on CT images. In many cases, the thoracic OPLL had been remodeled into trabecular bone or incorporated into the vertebral body long-term after surgery.
Comparison of Surgical Outcomes Between PDF and PCDF Group
Comparison of surgical outcomes between posterior decompression and fusion (PDF) and posterior circumferential decompression and fusion (PCDF) group.
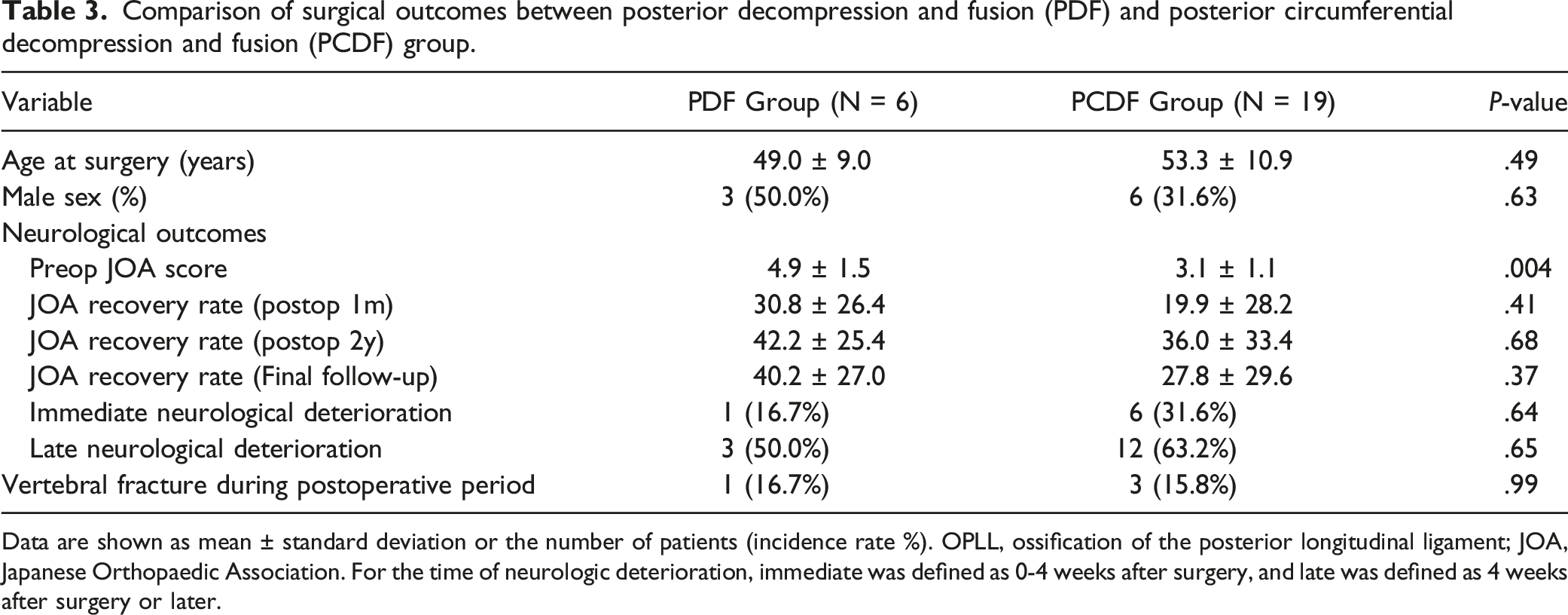
Data are shown as mean ± standard deviation or the number of patients (incidence rate %). OPLL, ossification of the posterior longitudinal ligament; JOA, Japanese Orthopaedic Association. For the time of neurologic deterioration, immediate was defined as 0-4 weeks after surgery, and late was defined as 4 weeks after surgery or later.
Factors Affecting Survival
Among 29 patients who were finally followed up for more than 10 years or until death, 9 (31%) died of causes unrelated to surgery: heart failure (n=3), aspiration pneumonia (n=2), sepsis (n=1), leukemia (n=1), pancreatic cancer (n=1), and unknown (n=1). The survival time from PDF surgery to death in the 9 deceased patients ranged from 1 to 22 years, with a median of 9 years. Their median age at death was 72 (range 61-92) years.
Univariate analysis using the Kaplan-Meier method combined with the log-rank test demonstrated that hypertension and ischemic heart disease were associated with shorter survival. Conversely, T2D, obesity, co-existence of cervical OPLL, and DISH fractures did not significantly influence survival rates (Figure 7). Kaplan–Meier survival curves stratified according to diabetes mellitus (A), hypertension (B), ischemic heart disease (C), obesity (D), co-existence of cervical OPLL (E), and vertebral fractures (F). OPLL, ossification of the posterior longitudinal ligament.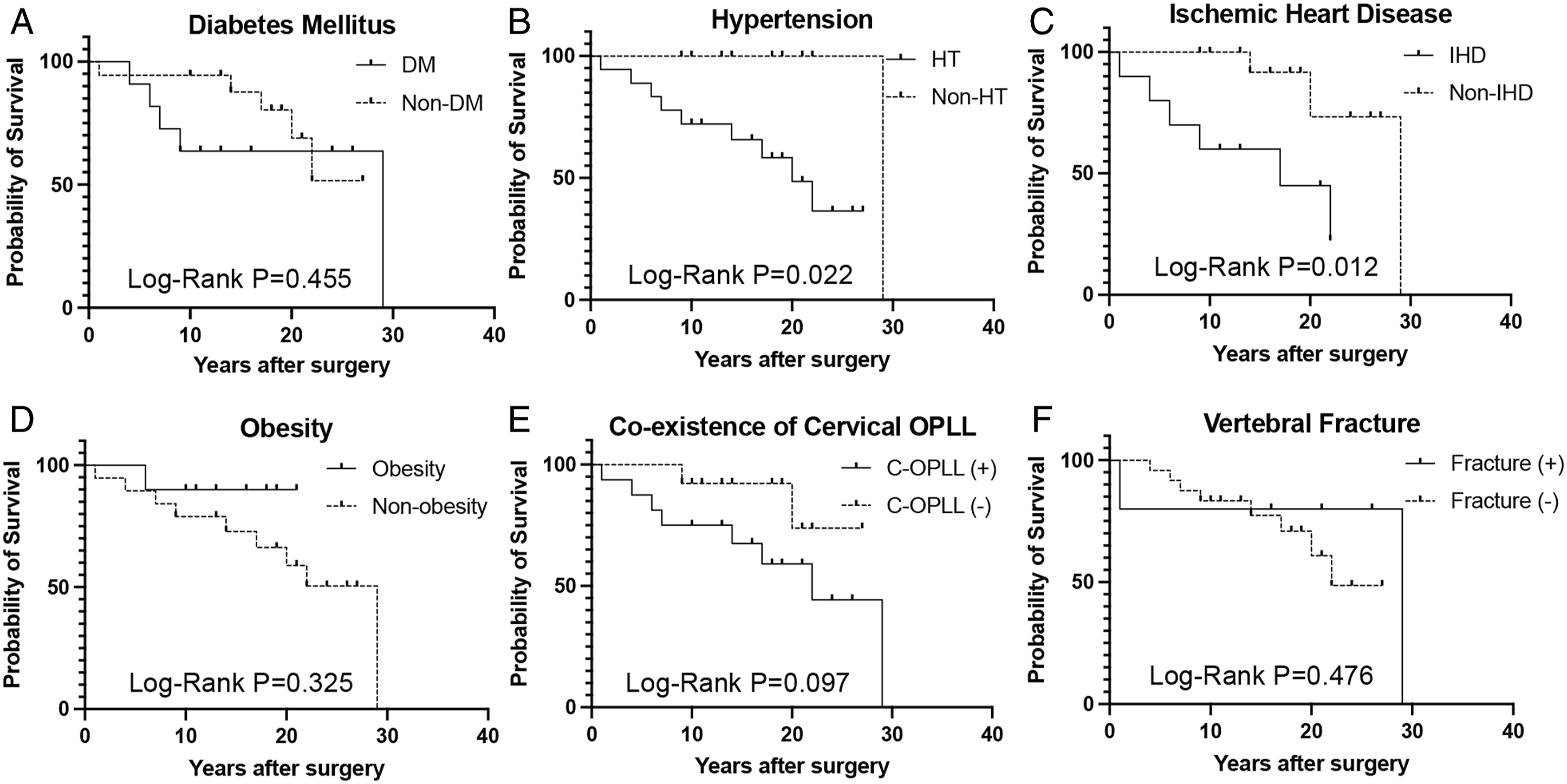
Discussion
This study shows that decompression and posterior instrumented fusion surgery for thoracic OPLL is a reliable procedure with stable long-term results, consistent with the results of earlier studies.8-10 However, we found that patients with thoracic OPLL were more likely to have a relapse of myelopathy or to present with cauda equina syndrome due to OPLL in the cervical and/or lumbar spine or OLF in the segment adjacent to the instrumented spine. This is probably because OPLL has the tendency to progress over the entire spine in patients with symptomatic thoracic OPLL.2,6,7,12 As a result, more than half the patients in this study underwent multiple spine surgeries for OPLL or OLF after thoracic spine surgery. Therefore, the involvement of cervical or lumbar lesions should always be considered if patients with thoracic OPLL develop new or worsening neurological symptoms in the postoperative course.
Another important finding was that patients with thoracic OPLL were at high risk of experiencing DISH-related vertebral column fractures, which occurred more than 10 years after PDF surgery. Patients with DISH frequently exhibit stress-shielding osteoporosis 13 ; this is to be expected in patients with thoracic OPLL because of the condition’s strong tendency to cause diffuse ligamentous ossification. Furthermore, the susceptibility of patients to fragility fractures is probably due to the high fall risk resulting from residual gait and balance dysfunction. Vertebral fracture may even occur within the fused area after instrumented PDF. 14 Unlike that caused by OPLL or OLF, paralysis caused by vertebral fracture showed poor recovery even after additional surgery. Therefore, attention should be paid to the risk of DISH-related osteoporotic fracture, which is underestimated through dual-energy X-ray absorptiometry scans, 13 especially in patients with ankylosing spine and residual paraplegic symptoms.
Our study shows that spinal instrumentation is important for maintaining positive long-term outcomes and immediate functional recovery in patients with OPLL. It provides stability to the spinal segments, protecting the spinal cord from dynamic compression.14-16 Although it is still inconclusive whether instrumented spinal fusion can suppress the progression of OPLL in size and shape,7,10,17-21 our data showing that no patient experienced a relapse of myelopathy within the instrumented spinal segments after more than 10 years of surgery suggest that OPLL will not progress enough to cause a relapse of myelopathy after posterior instrumented fusion surgery. OPLL within the fusion segments is often remodeled into trabecular bone or incorporated into the vertebral body, suggesting that spinal instrumented fusion exerts a stress-shielding effect on OPLL. 22 Additionally, spinal instrumentation may help prevent the progression of kyphosis: the 2 cases where spinal instrumentation had to be removed due to deep wound infection resulted in the progression of kyphosis.
A mortality analysis of patients with thoracic OPLL who underwent PDF surgery showed that hypertension and cardiac disease were associated with mortality. This is consistent with the findings of a national cohort study on 1 025 340 Koreans, which identified that hypertension, cardiovascular and cerebrovascular disease, diabetes, and renal disease were significantly associated with mortality in patients with cervical OPLL. 23 Some patients with cervical OPLL die at an early stage due to pneumonia 24 ; this may also be true in some patients with thoracic OPLL based on the fact that 2 of the 9 deceased patients in our study died due to aspiration pneumonia and many patients with thoracic OPLL also had cervical OPLL.
Our study has several limitations. First, the sample size was small due to the rarity of the disease and the difficulty of conducting long-term follow-up for more than 10 years, preventing multivariate or Cox proportional hazards analysis and making it difficult to draw conclusions on risk factor analysis for re-worsening of paralysis or death. Second, we were unable to quantitatively assess the change in OPLL size with CT. The reason for this is that CT images of cases treated more than 20 years ago had low resolution, and therefore progression could not be determined without a change of at least 3 mm. In addition, change in the size of the lesion for which extirpation or anterior floating was performed was hard to measure. Third, regarding mortality analysis, we could not conclude whether the life expectancy of patients with thoracic OPLL was shorter than that of the general population because of the lack of controls. Lastly, the lack of necessary images made it impossible to measure long-term postoperative spinal alignment changes. However, as the images of the representative cases in the figures show, most cases presented a noticeable alignment change. This observation and the effects on pain and quality of life should be further studied.
In conclusion, although instrumented PDF for patients with thoracic OPLL is a reliable surgical procedure with excellent outcomes, the predisposition of the OPLL for diffuse progression over the entire spine elicits a focus on the relapse of paralysis due to OPLL or OLF in regions outside the operative lesion and on vertebral fractures of the ankylosed spine during the postoperative course.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.