
Abstract
Study Design
Retrospective observational study.
Objectives
To identify radiographic and clinical predictors of fracture-type proximal junctional kyphosis (PJFx) and associated myelopathy (PJFx-M), with the goal of facilitating timely surgical intervention.
Methods
We retrospectively reviewed 438 patients with adult spinal deformity who underwent long-segment fusion surgery at our institution between 2013 and 2023. Risk factors for PJFx and PJFx-M were analyzed, focusing on demographic and radiographic parameters. In PJFx-M cases, we specifically assessed sliding length, screw protrusion, and superior articular facet fractures.
Results
PJFx occurred in 102 patients (23.3%). Significant risk factors for PJFx included a lower Hounsfield unit (HU) value at the upper instrumented vertebra (UIV) and reduced preoperative lumbar lordosis. PJFx-M was identified in 10 patients (2.3%). Radiographic predictors of PJFx-M included increased sliding length, screw protrusion into the upper vertebra, and bilateral superior articular facet fractures (all P < 0.001). Additionally, a fall within 1 month of symptom onset was frequently observed in PJFx-M cases. PJFx-M was not associated with demographic factors or body mass index.
Conclusions
Lower HU at the UIV and reduced preoperative lumbar lordosis were key predictors of PJFx. PJFx-M should be suspected in the presence of increased sliding length, screw protrusion into the upper vertebra, superior articular facet fractures, and a recent fall. These findings highlight the importance of vigilant postoperative radiographic and clinical monitoring to enable early detection and intervention, potentially preventing neurological deterioration.
Keywords
Background
Adult spinal deformity (ASD) is characterized by abnormal spinal alignment that develops in adulthood. 1 Patients with ASD experience significant back pain, radiculopathy, and gait disturbances as a result of coronal and sagittal misalignment.2,3 These symptoms substantially impact quality of life and are important when determining the need for corrective surgery. Surgical interventions has been shown to improve health-related quality of life more effectively than non-surgical treatments, particularly in patients with severe deformity. 4 Nevertheless, these procedures come with high complication rates, with revision rates reaching up to 47%.5-7 These rates may be even higher with extended postoperative follow-up.
Proximal junctional kyphosis (PJK) is one of the most frequent complications following ASD surgery8-10 and typically results from fractures at the upper instrumented vertebra (UIV) or the adjacent vertebrae or from disruption of the posterior ligament. The main cause of PJK is proximal junctional fracture (PJFx), which usually occurs within the first 3 months after surgery.11,12 Identified risk factors include osteoporosis, 13 overcorrection of alignment, 14 and severe preoperative deformity,15,16 although findings have been inconsistent and not fully understood.
In most cases, symptoms of PJFx are mild and repeat surgery is not required. However, in some cases, PJFx leads to myelopathy and paralysis, necessitating immediate surgical intervention. Despite prompt treatment, paralysis may persist and significantly impact quality of life.
This study aimed to clarify the risk factors for PJFx by analyzing a large dataset from a single spine center. It also sought to identify risk factors for myelopathy resulting from PJFx (PJFx-M) and potential risk factors, which has not been well characterized in previous studies.
Methods
We retrospectively reviewed all patients who underwent surgery for ASD at our hospital between January 1, 2013 and December 31, 2023. Institutional review board approval was secured, permitting patient enrollment and data collection. The inclusion criteria were age 21 years or older at the time of surgery, a minimum postoperative follow-up of 1 year, surgery that involved posterior instrumentation spanning 5 or more levels, and complete radiographic data available. At the UIV, bilateral pedicle screws were placed in all cases, resulting in a uniform screw density of two per vertebra. Screw trajectory, angulation, and insertion depth were determined intraoperatively by each surgeon based on anatomical landmarks and bone quality. The underlying causes identified included degenerative kyphosis/kyphoscoliosis, complications following lumbar surgery, and vertebral fractures. Any deformity caused by tumor or infectious disease was excluded.
Three-column osteotomy entailed use of pedicle subtraction osteotomy or vertebral column resection. PJK was defined as kyphosis exceeding 10° between the UIV and the 2 vertebrae above it (UIV+2), while PJFx was defined as PJK resulting from a vertebral fracture, with the specific angle termed the proximal junctional angle. Myelopathy resulting from PJFx was categorized as PJFx-M. The decision to pursue surgical vs conservative treatment for PJFx was made based on patient condition and shared decision-making between surgeon and patient. All patients who developed PJFx-M had initially received conservative management without immediate revision surgery.
To evaluate the influence of screw placement on PJFx and PJFx-M, we conducted a detailed radiographic analysis of pedicle screws at the upper instrumented vertebra (UIV). The following parameters were assessed on postoperative sagittal CT images: Screw trajectory angle in the sagittal plane, measured relative to the superior endplate. Positive values indicate cranial direction, negative values indicate caudal angulation. Screw tip–superior endplate distance (%): the vertical distance from the screw tip to the superior endplate, normalized to the total vertebral body height. Screw tip–anterior cortex distance (%): the distance from the screw tip to the anterior cortical margin of the vertebral body, normalized to its anteroposterior diameter. All parameters were measured on both right and left screws. For analysis, the mean values of bilateral screws were used to represent each patient.
We collected data for age, sex, body mass index (BMI), medical comorbidities, bone mineral density at the femoral neck (T-score), and details on use of medication for osteoporosis before and after surgery. Medical comorbidities included diabetes, renal dysfunction, and cerebrovascular, cardiovascular, and respiratory diseases. Radiographic measurements included the sagittal vertical axis (SVA), thoracic kyphosis (TK) from T4 to T10, thoracolumbar kyphosis from T10 to L2, lumbar lordosis from L1 to S1, sacral slope, pelvic incidence, and pelvic tilt (PT). Global tilt (GT) was defined as the sum of the PT and the C7 vertical tilt, the angle created by the intersection of 2 lines; the first line is drawn from the center of the C7 vertebra to the center of the sacral endplate, and the second line is drawn from the center of the femoral heads to the center of the sacral endplate. The positioning of the lower instrumented vertebra, whether fixed to the sacrum or not, was also examined. These parameters were assessed in a standing position before and 2 weeks after surgery and at the latest radiographic follow-up. Ideal spinal alignment was defined as a pelvic incidence–lumbar lordosis mismatch (PI–LL) angle within –10° to +10° according to the SRS-Schwab ASD classification. 17 Referring to a previous report, 18 we also measured the relative pelvic version (RPV; equal to the measured minus the ideal SS), the relative LL (RLL; equal to the measured minus the ideal LL), the lordosis distribution index (LDI; equal to the L4-S1 lordosis divided by the L1-S1 lordosis multiplied by 100), and the relative spinopelvic alignment (RSA; equal to the measured minus the ideal GT). The ideal values of SS, LL, and GT were defined according to previous reports that analyzed their relationship with PI using asymptomatic population records. Age was stratified into 2 subgroups: <60 years and 60 years or older. The GAP score was calculated by adding the scores for RPV, RLL, LDI, RSA, and the age factor, according to a previous report. The Hounsfield Unit (HU) value at the UIV was assessed in the midsagittal view using preoperative CT imaging.
In patients with PJFx, we analyzed the proximal junctional angle at the time of the last follow-up or immediately before repeat surgery. Additional assessments included examination of screw back-out into the caudal side disc or upper vertebra, the slip distance between the posterocranial point of the UIV and posterocaudal point of the UIV+1, and fractures of the superior articular process (none, unilateral, or bilateral, Figure 1). Mechanism and Radiographic Findings of Myelopathy Following Proximal Junctional Failure. Abbreviations: UIV, Upper Instrumented Vertebra; UIV+1, the Vertebra One Level Above the UIV; UIV+2, the Vertebra Two Levels Above the UIV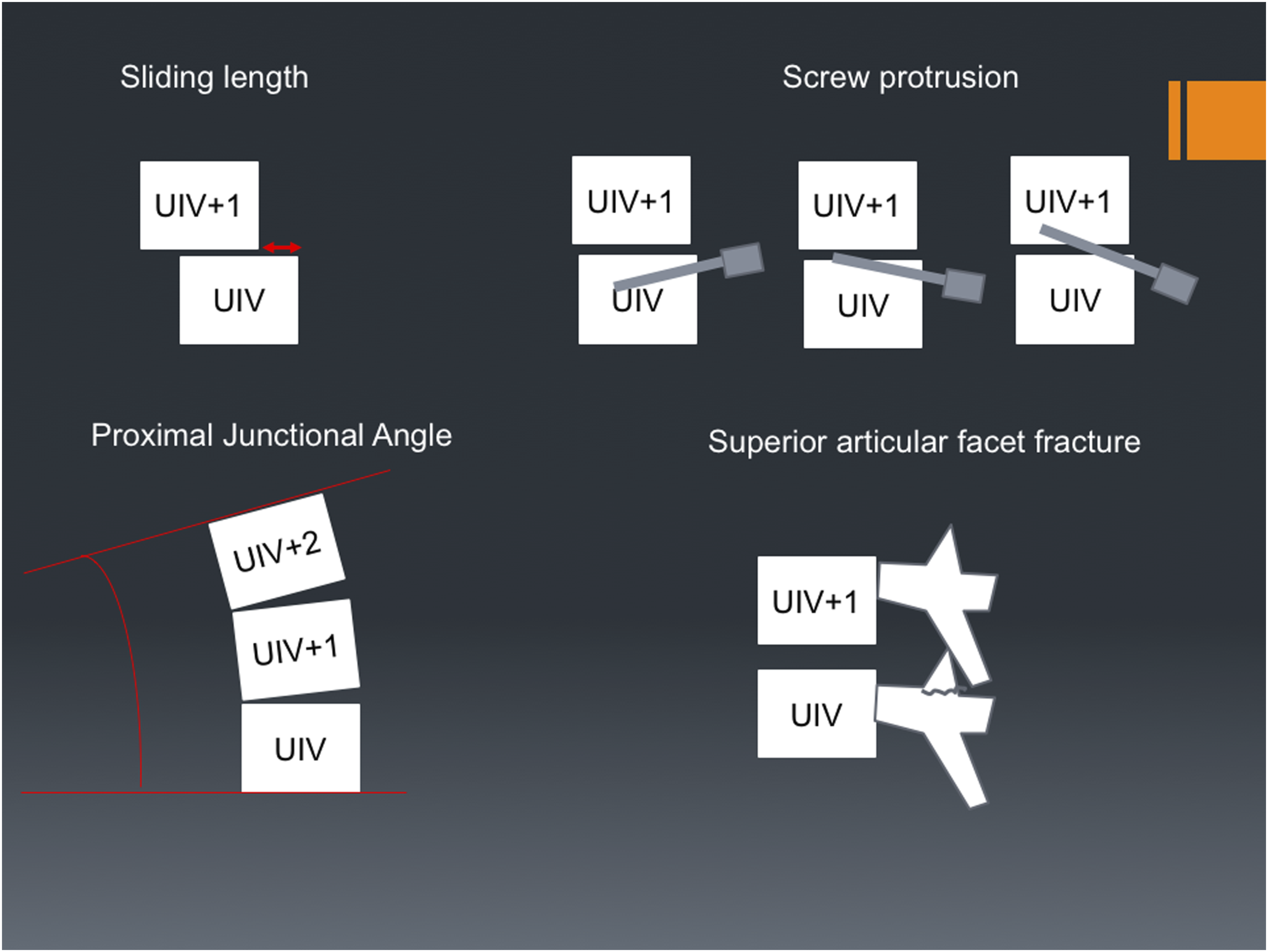
Patients were categorized into 2 groups, namely, those with PJFx [PJFx(+)] and those without (PJFx (−)), with further division of the PJFx(+) group into those with myelopathy (PJFx-M (+)) and those without myelopathy (PJFx-M (−)). To address our 2 main objectives—first, to identify risk factors for PJFx, and second, to explore which cases of PJFx progressed to PJFx-M—we performed 2 separate sets of analyses. Specifically, we compared PJFx(+) and PJFx(−) groups to identify PJFx risk factors, and then compared PJFx-M(+) and PJFx-M(−) within the PJFx group to assess predictors of myelopathy. Continuous variables were compared between groups using t-tests and categorical variables using chi-squared tests. Risk factor analysis for PJFx was performed using multivariate logistic regression with a stepwise forward procedure (P < 0.1 for entry).Missing values were handled using the last observation carried forward method. All statistical analyses were performed using IBM SPSS Statistics for Macintosh, version 25.0 (IBM Corp., Armonk, NY). A P-value of <0.05 was deemed statistically significant.
Results
Demographic and Clinical Data for Patients Who Underwent Surgery for Adult Spinal Deformity
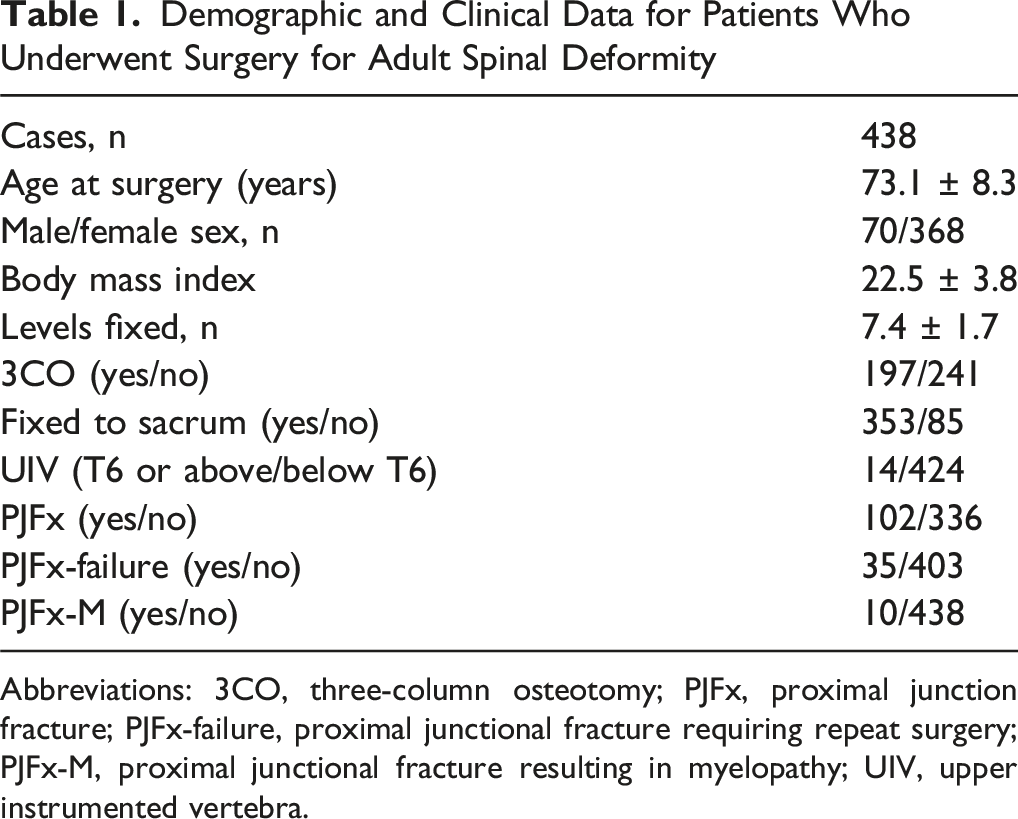
Abbreviations: 3CO, three-column osteotomy; PJFx, proximal junction fracture; PJFx-failure, proximal junctional fracture requiring repeat surgery; PJFx-M, proximal junctional fracture resulting in myelopathy; UIV, upper instrumented vertebra.
Demographic and Radiographic Data for Patients With and Without Proximal Junction Fracture
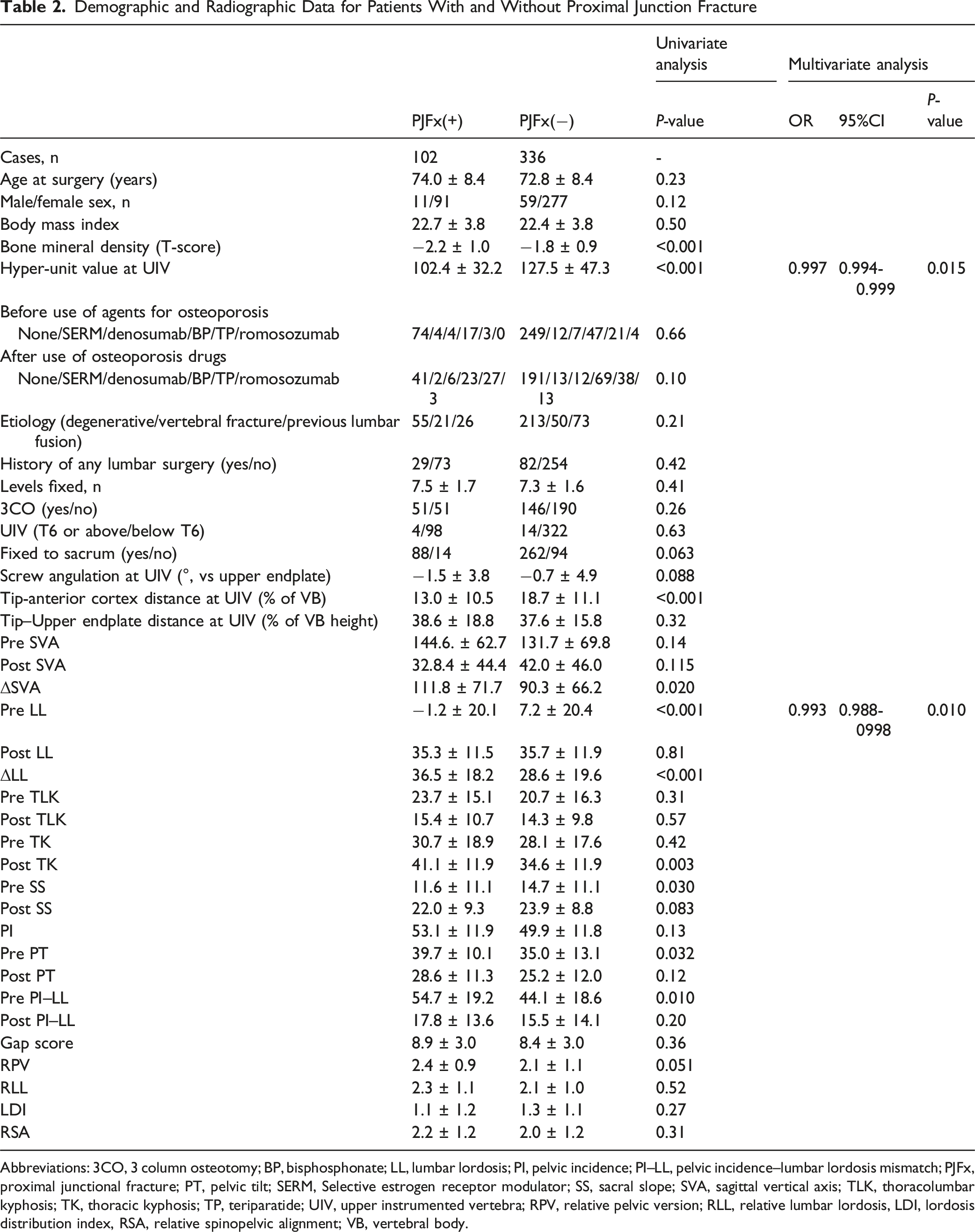
Abbreviations: 3CO, 3 column osteotomy; BP, bisphosphonate; LL, lumbar lordosis; PI, pelvic incidence; PI–LL, pelvic incidence–lumbar lordosis mismatch; PJFx, proximal junctional fracture; PT, pelvic tilt; SERM, Selective estrogen receptor modulator; SS, sacral slope; SVA, sagittal vertical axis; TLK, thoracolumbar kyphosis; TK, thoracic kyphosis; TP, teriparatide; UIV, upper instrumented vertebra; RPV, relative pelvic version; RLL, relative lumbar lordosis, LDI, lordosis distribution index, RSA, relative spinopelvic alignment; VB, vertebral body.
Demographic and Radiographic Data for the Group With PJFx-M and the Group Without PJFx-M
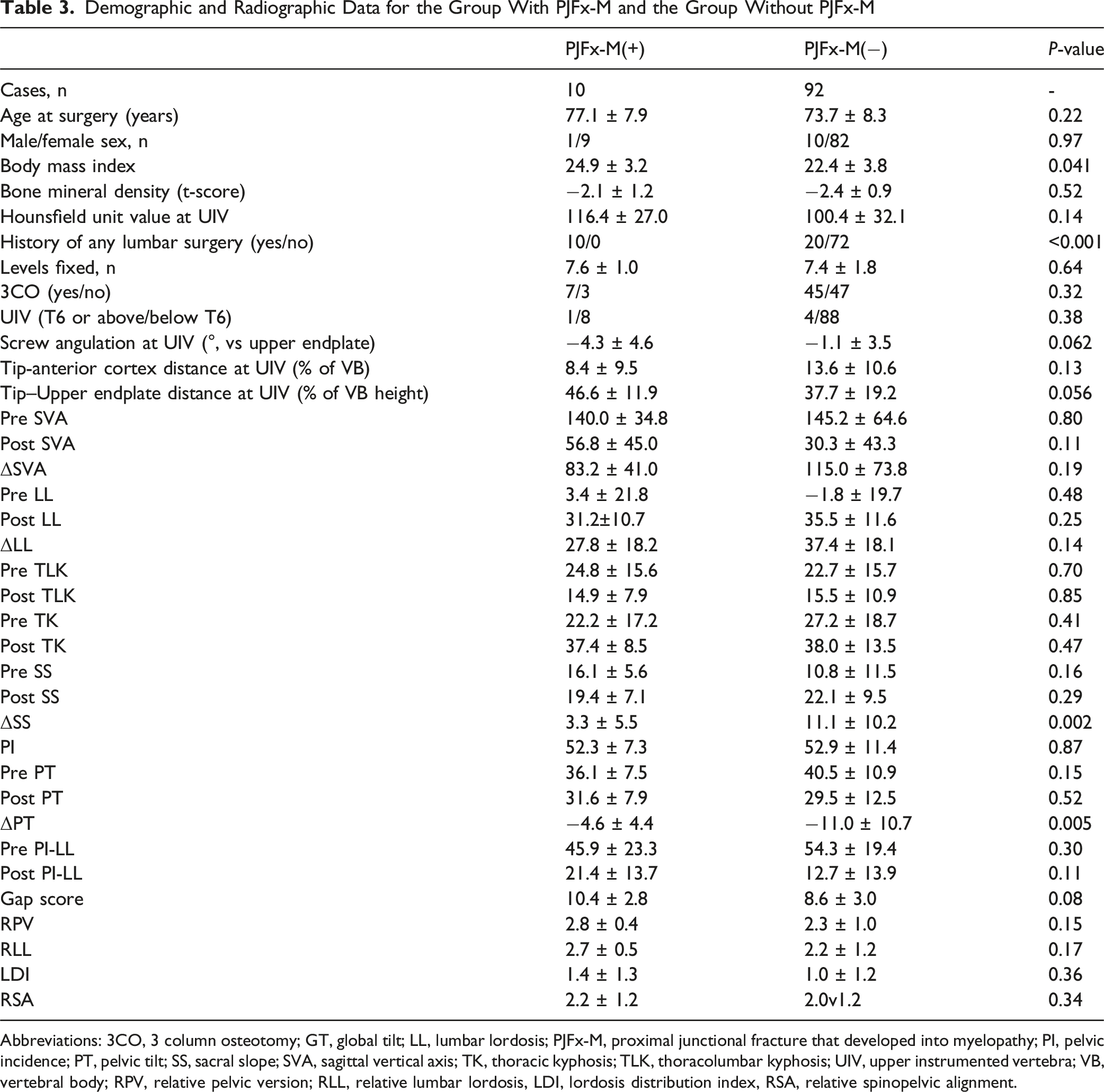
Abbreviations: 3CO, 3 column osteotomy; GT, global tilt; LL, lumbar lordosis; PJFx-M, proximal junctional fracture that developed into myelopathy; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; SVA, sagittal vertical axis; TK, thoracic kyphosis; TLK, thoracolumbar kyphosis; UIV, upper instrumented vertebra; VB, vertebral body; RPV, relative pelvic version; RLL, relative lumbar lordosis, LDI, lordosis distribution index, RSA, relative spinopelvic alignment.
Radiographic Indicators of PJFx-M
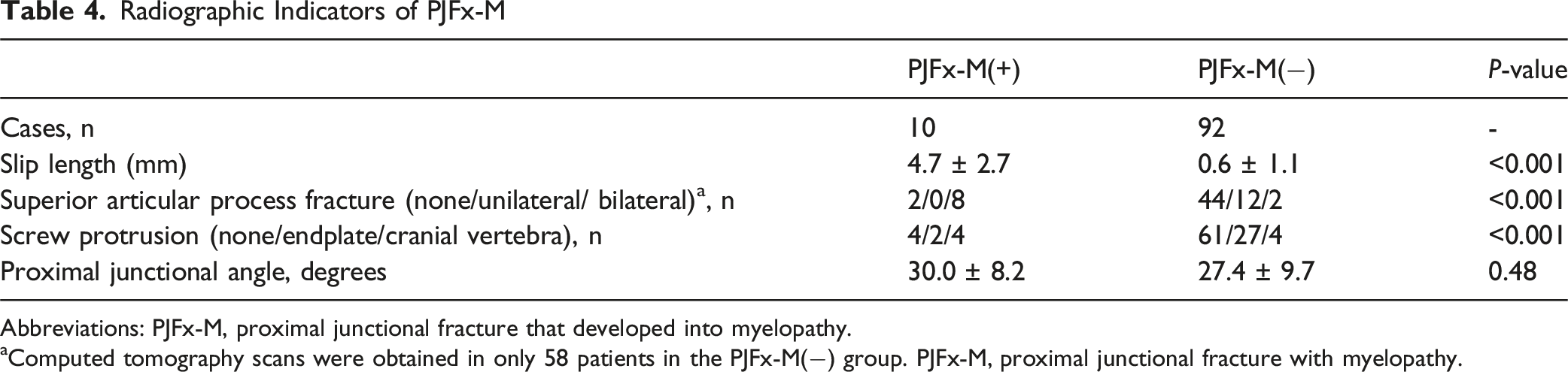
Abbreviations: PJFx-M, proximal junctional fracture that developed into myelopathy.
aComputed tomography scans were obtained in only 58 patients in the PJFx-M(−) group. PJFx-M, proximal junctional fracture with myelopathy.
Discussion
There have been few studies on the classification of PJK. Yagi et al. 12 classified PJK based on type and grade, including spondylolisthesis, providing a simple and effective way for clinicians to discuss the types of PJK. In this study, we focused specifically on fracture-type PJK (PJFx), also known as type 2 PJK, given that most cases of PJK are caused by fractures at the UIV or the vertebra immediately above (UIV+1). Severe PJK is typically caused by these fractures, which usually occur within the first 3 months post-surgery. 19 We reviewed all our cases of PJFx and noted inconsistency in the criteria used for revision, which we attributed to decisions being influenced by patient resilience or surgeon preference. Therefore, we further analyzed cases of myelopathy that required immediate revision surgery, where the timing of intervention was critical.
First, we analyzed risk factors for PJFx. A lower preoperative LL and HU value at UIV was identified as a significant risk factor for PJK, whereas age, sex, and BMI did not show any correlation with the incidence of PJK. Previous studies have identified older age,20-22 osteoporosis, 13 a high BMI, 21 and sarcopenia 23 to be risk factors for PJK following surgery for correction of ASD. Although age ≥50 years is often cited as a risk factor, the average age of our patients was ≥70 years, which may explain why age did not significantly affect the PJK rate. Another study found that patients with low bone mineral density, including those with osteoporosis or osteopenia, had a 30.9% increase in risk of developing PJK, 19 which aligns with our present findings. Yagi et al reported that the incidence of type 2 PJK in patients with osteopenia was significantly lower in those treated with teriparatide than in controls (4.6% vs 15.2%, P = 0.02). 24 In our study, only a limited number of patients received teriparatide preoperatively and postoperatively, so we could not examine its potential protective effect. Sacral fixation was assessed as a potential risk factor for PJFx. Although the incidence of PJFx was slightly higher in patients with sacral fixation, this difference was not statistically significant. Therefore, sacral fixation was not treated as a stratified variable in our multivariate analysis. Nonetheless, rigid distal fixation may biomechanically contribute to increased stress at the proximal junction, and this possibility should be considered in future studies.
In terms of radiographic parameters, forward stepwise logistic regression indicated that the preoperative LL was a significant risk factor for PJFx. Maruo et al found that a preoperative TK of ≥30° was a predictor of PJK, and a meta-analysis identified a pre TK >40° as a risk factor for PJK. 25 Other studies have also found that a preoperative proximal junctional angle of ≥10° and pelvic incidence >55° are associated with an increased risk of PJK. 14 Helgeson et al noted that postoperative changes in SVA of ≥50 mm increased the incidence of PJK, 15 while other studies found that a postoperative SVA of <50 mm significantly increased the risk of proximal junctional failure. 26 A change in lumbar lordosis of ≥30° has also been identified as a risk factor for PJK. 14 However, analysis of the risk factor of fracture type PJFx is limited.
Characteristics of Individual Patients With PJFx-M
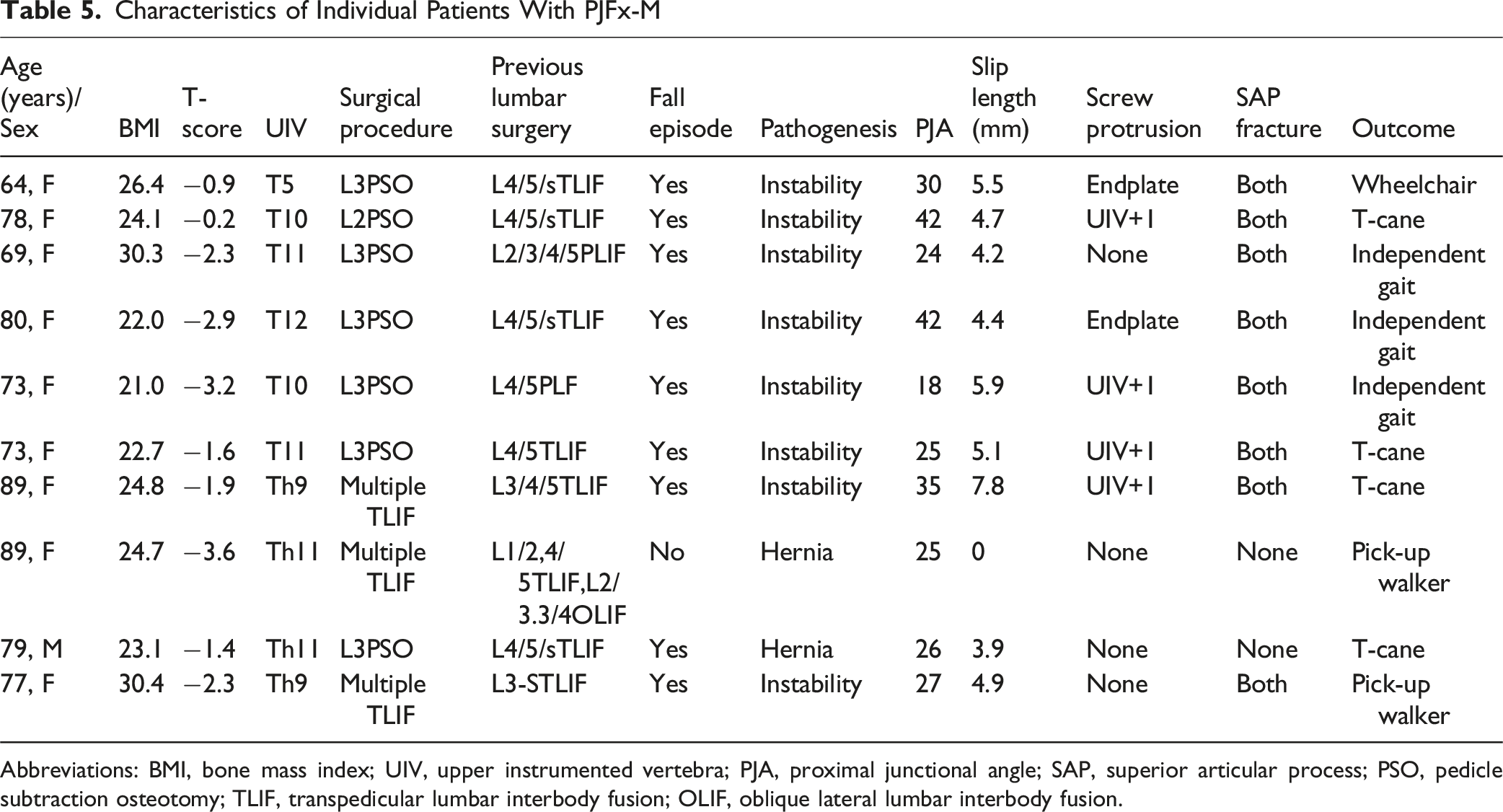
Abbreviations: BMI, bone mass index; UIV, upper instrumented vertebra; PJA, proximal junctional angle; SAP, superior articular process; PSO, pedicle subtraction osteotomy; TLIF, transpedicular lumbar interbody fusion; OLIF, oblique lateral lumbar interbody fusion.
Several studies have explored the use of cement augmentation to prevent PJK and proximal junctional failure in patients with osteoporosis.27-30 1 study found that prophylactic vertebroplasty at UIV and UIV+1 reduced the incidence of PJK by 8% and that of proximal junctional failure by 5% at 6 months. 27 Spinal hooks have also been used to prevent PJK, with 1 study showing a 0% incidence of PJK in a hook group compared with 29.6% in a pedicle screw group. 15 Another technique involves reconstructing the posterior ligamentous complex using Mersilene tape to reduce loading stress, with a systematic review showing a lower incidence of PJK and a reduction in disc pressure in comparison with use of pedicle screws.31,32 These methods reduce violations of the superior articular facet at the UIV, potentially lowering the risk of myelopathy.
To date, no studies have clearly identified risk factors for myelopathy or the optimal timing of intervention in patients with PJFx. In our study, all patients with PJFx-M had a history of prior lumbar fusion surgery, and changes in sacral slope (SS) and pelvic tilt (PT) were significantly smaller in these patients. These findings suggest that prior lumbar fusion may restrict compensatory pelvic alignment, thereby contributing to the onset of myelopathy. As for the timing of intervention, increased sliding length of UIV+1, screw protrusion into UIV+1, and bilateral fractures of the UIV’s superior articular process were key radiographic predictors of impending myelopathy. Additionally, a fall episode was observed within 1 month prior to symptom onset in many patients. These findings underscore the importance of vigilant postoperative radiographic and clinical surveillance to allow early detection and timely intervention, potentially preventing neurological deterioration.
This study has several limitations. First, its retrospective design inherently limits causal inference. Second, all data were obtained from a single institution, which may affect the generalizability of the findings. Finally, the number of patients with PJFx-M was relatively small, which may limit the statistical power for detecting significant differences.
Conclusion
In this study, lower preoperative LL and lower HU value at UIV were identified as key risk factors for PJFx. Age and BMI did not show a significant correlation in our cohort. If a fall occurs in a patient with PJFx, immediate intervention is recommended when increased sliding length, screw protrusion into the UIV+1, or superior articular facet fractures is present, given that these factors can lead to myelopathy.
Footnotes
Ethical Approval
The study was approved by the ethics committee of all institutions involved. Informed consent was waived by the above ethics committee as the present retrospective cohort study involved already existing data and records at the time of investigation and did not retain personal identifiers of the gathered information. The ethical committee, Kudanzaka Hospital; 2019-5.
Author Contributions
Atsuyuki Kawabata analysed the data and wrote the original draft. Yu Matsukura, Takuya Oyaizu, Hiroaki Onuma, and Toshitaka Yoshii conceived of, reviewed, and edited the paper. Keisuke Hide, Takayuki Motoyoshi, Jun Hashimoto, Kazuo Kusano, Kazuyuki Otani, Satoru Egawa, Kentaro Yamada and Shigeo Shindo acquired the data. Shingo Morishita performed the investigation. Toshitaka Yoshii validated the paper. Kazuyuki Otani, Shigeo Shindo, and Toshitaka Yoshii supervised the research. All authors contributed to the writing of the final manuscript. All authors approved the manuscript to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.