
Abstract
Study design
Retrospective study.
Objectives
To investigate the effects of transverse process hook (TPH) at the uppermost instrumented vertebra (UIV) + 1 on the prevention of proximal junctional kyphosis/failure (PJK/F) following adult spinal deformity (ASD) surgery.
Methods
We included patients who underwent fusion of the lower thoracic spine (T8–T11) to the sacrum for ASD. The patients were divided into the non-TPH and TPH groups. PJK and PJF were defined as proximal junctional angle >20° and any cases requiring revision surgery. Multiple regression analysis was performed, including surgical techniques (non-use of TPH vs TPH) and confounding variables.
Results
Altogether, 153 patients were included in the study (women, 91.5%; mean age, 69.2 years; total levels fused, 8.5). The non-TPH and TPH groups comprised 88 and 65 patients. Unadjusted bivariate analysis showed that the TPH did not significantly affect the risk of PJK and PJF. However, multiple regression analysis revealed that the non-use of TPH was associated with an increased risk of developing PJK and PJF (odds ratio [OR] = 3.079, P = 0.029 for PJK; OR = 6.363, P = 0.049 for PJF). In patients who underwent TPH fixation, confounder-adjusted regression analysis showed that two-level TPH fixation did not further decrease the risk of PJK/F.
Conclusions
The preventive effect of TPH against PJK/F development was not significant in the unadjusted bivariate analysis. However, multiple regression analysis adjusted for the confounding factors demonstrated that TPH fixation at the UIV +1 significantly decreased the risk of PJK and PJF.
Keywords
Introduction
The demand for surgical treatment of adult spinal deformity (ASD) has increased enormously owing to an aging society. In the surgical treatment of ASD, long-segment spinal fusion is frequently required to achieve adequate sagittal alignment. Proximal junctional kyphosis (PJK) is a broad radiographic term to describe kyphosis development at the proximal junction of the long construct.1,2 Proximal junctional failure (PJF) refers to a structural failure that can result in significant clinical consequences such as increased kyphotic deformity, aggravated pain, myelopathy, and subsequent revision surgery.3-7 Considering their adverse effects on the clinical outcomes, preventing PJK/F is crucial for the success of ASD surgery.
Although the etiology of PJK/F is multifactorial, the generally accepted pathomechanism is the increased stress incurred at the most proximal junction.2,4,5,8,9 To address this phenomenon, transverse process hook (TPH) fixation has been introduced as a “soft-landing technique”. 10 The theoretical background of TPH fixation is that compared with pedicle screws, hooks anchored at the most proximal level provide a more gradual transition of construct stiffness to the non-instrumented vertebrae and less mechanical stress. This theory has been supported by several biomechanical studies that have demonstrated a better range of motion and less construct stiffness with the use of TPH.11-14
However, these results have not been consistently reported in the clinical settings. Some studies advocated the preventive roles of TPH,15,16 whereas others questioned the effects of TPH in preventing PJK.17,18 Moreover, recent systematic reviews have concluded that evidences regarding the efficacy of TPH remains inconsistent and conflicting.19,20 These controversial results of TPH could be caused by the lack of homogeneity in the comparison groups, which acts as a significant confounder. The potential confounding factors between the comparison groups must to be adequately controlled to assess the efficacy of any local preventive technique. Therefore, this study aimed to investigate the effects of TPH fixation on the prevention of PJK/F by comparing it with a pedicle screw-only construct, using multiple regression analysis to adjust for confounding factors.
Materials and Methods
This study was approved by the institutional review board of our center. The requirement for informed consent was waived owing to the retrospective nature of the study.
Study Population
Patient records retrieved from a prospective ASD database at our tertiary hospital were analyzed retrospectively. The study cohort comprised consecutive patients who received corrective surgery for degenerative ASD between 2014 and 2022. The patient inclusion criteria were as follows: ASD radiographically defined as pelvic incidence (PI)−lumbar lordosis (LL) mismatch ≥10°, pelvic tilt (PT) ≥ 25°, C7–sagittal vertical axis (C7–SVA) ≥ 5 cm, or coronal Cobb angle ≥30°; and fusion from the lower thoracic spine (T8–T11) to the sacrum. Pelvic fixation was routinely performed using conventional iliac screws, except in cases of lumbosacral fusion because of the prior fusion surgery. The minimum follow-up duration was 2 years. Patients were excluded if they had non-degenerative deformity such as infectious or tumorous conditions; received revision surgery for pseudoarthrosis due to bilateral rod fractures; had prophylactic cement augmentation at the uppermost instrumented vertebra (UIV) or UIV+1; and lacked appropriate radiographic data.
All the surgeries were performed by two attending spine surgeons with clinical experience ≥10 years. The decision regarding TPH use and the number of TPH fixations (one- or two-level TPH) was at the discretion of the surgeons (Figure 1). Bilateral hooks were placed over the transverse process at the UIV +1 level. None of patients were treated with a combined hook and pedicle screw at the same level. Plain or offset hooks were used considering the proximal rod contour. No laminar hooks were used. Although the level with the TPH placed can be considered the UIV, we defined the UIV as the uppermost level fixed by pedicle screws in this study to match the pedicle screw-fixed fusion length between the non-TPH and TPH groups. Therefore, the level with the TP hook was expressed as the UIV+1. Patients were divided into two groups based on TPH implementation: non-TPH and TPH groups. (A) No transverse process hook (TPH). (B) One-level TPH fixation. (C) Two-level TPH fixation.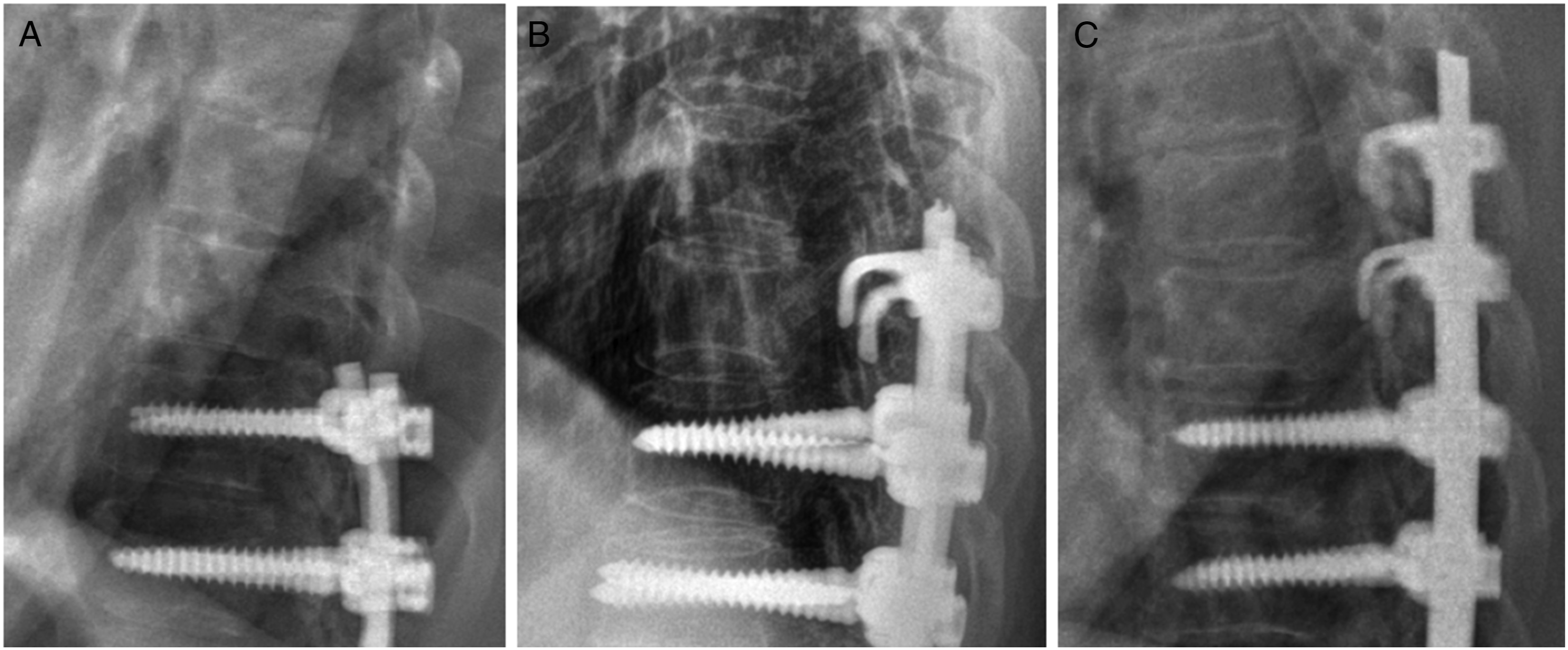
Data Collection
Baseline data on sex, age, American Society of Anesthesiology physical status grade, T-score (lowest score on spine or hip dual-energy X-ray absorptiometry), body mass index (BMI), revision cases, lateral lumbar interbody fusion (LLIF), pedicle subtraction osteotomy (PSO), pelvic fixation, total fused levels, and follow-up duration were obtained.
Regarding the radiographic results, the following conventional radiographic parameters were measured preoperatively and at 6 weeks postoperatively: PI, PI−LL, LL, sacral slope (SS), PT, thoracic kyphosis (TK), and C7–SVA. In addition to 6-week PI−LL, the postoperative PI−LL correction status was evaluated using the alignment assessment metrics including the Global Alignment Proportion (GAP) score and sagittal age-adjusted alignment score (SAAS). The GAP score was evaluated using an original GAP scoring system as follows: proportional (≤ 2 points); moderately disproportioned (3-6 points); and severely disproportioned (≥ 7 points). 21 The SAAS is a recently introduced radiographic alignment scheme which comprised three sagittal components: age-adjusted PI–LL, PT, and TPA. 22 Scores are provided to each sagittal component according to the difference between the current and target values. Based on the total sum of SAAS, sagittal correction was categorized into “undercorrection” if it was < −1, “matched” if it was between −1 and +1, and “overcorrection” if it was > + 1.
Definition of PJK/F
PJK was defined as proximal junctional angle (PJA) > 20°.23,24 PJF was defined as any case requiring revision surgery because of proximal junctional complications. In patients who developed PJK, failure modes were investigated in terms of vertebral fractures at the UIV, vertebral fractures at the UIV+1, and ligamentous failure. Ligamentous failure represents kyphosis development with a PJA exceeding 20° without accompanying vertebral fractures.
Statistical Analysis
Categorical variables were compared using the chi-square or Fisher’s exact tests, and continuous variables were assessed for normality and compared between the two groups using the independent t-test or Mann–Whitney U-test, as appropriate. Two regression models were created to report the odds ratio (OR) of TPH fixation in preventing PJK/F. First, unadjusted bivariate analyses were performed to calculate the crude OR for the surgical techniques (non-TPH vs TPH fixation). Second, multiple regression analyses were performed using the surgical techniques (non-TPH vs TPH fixation) and confounders. The confounding factors subjected to multiple regression analyses were those that showed significant differences in baseline and perioperative radiographic data between the non-TPH and TPH groups. For patients who underwent TPH fixation, subgroup analysis was performed according to TPH level (one- or two-level) to investigate whether two-level TPH fixation further decreased the risk of PJK/F compared with one-level TPH fixation. Similar to previous regression methods, bivariate and multiple regression analyses were performed using the surgical technique variable (two-level TPH vs one-level TPH fixation) and the variables showing significant differences in the intergroup comparisons of baseline and radiographic data between one- and two-level TPH groups. All statistical analyses were performed using SPSS (version 27.0.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at P < 0.05.
Results
Baseline and Perioperative Radiographic data Among the Groups.
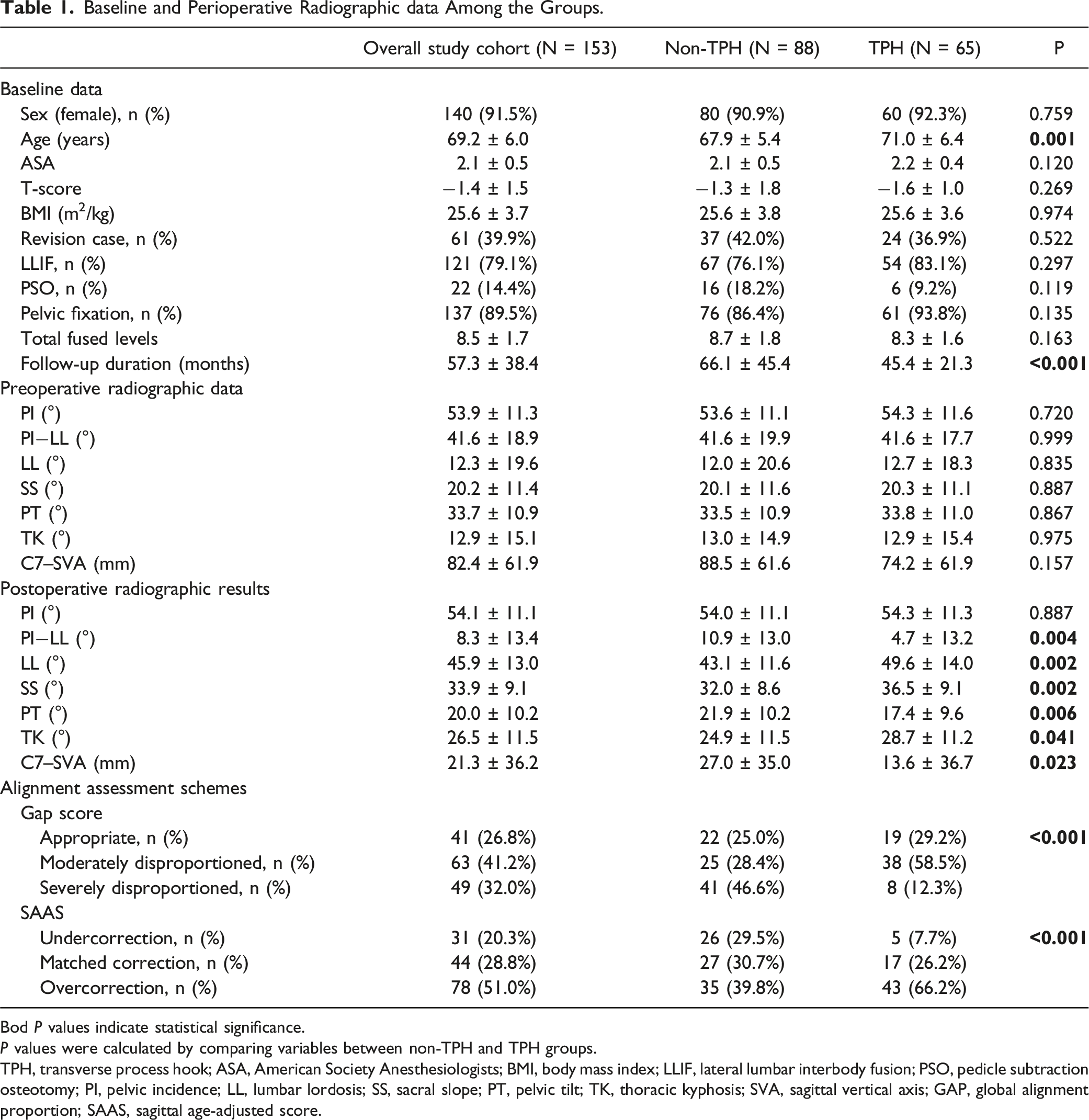
Bod P values indicate statistical significance.
P values were calculated by comparing variables between non-TPH and TPH groups.
TPH, transverse process hook; ASA, American Society Anesthesiologists; BMI, body mass index; LLIF, lateral lumbar interbody fusion; PSO, pedicle subtraction osteotomy; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; GAP, global alignment proportion; SAAS, sagittal age-adjusted score.
The non-TPH and TPH groups comprised 88 (57.5%) and 65 (42.5%) patients, respectively (Table 1). The patients in the TPH group were significantly older (P = 0.001) and had a significantly shorter follow-up duration (P < 0.001) than those in the non-TPH group. No significant differences in the preoperative radiographic parameters were noted between the two groups. Postoperatively, the TPH group showed a trend toward greater magnitude of sagittal correction compared with the non-TPH group with significant differences in PI−LL (P = 0.004), LL (P = 0.002), SS (P = 0.002), PT (P = 0.006), TK (P = 0.041), and C7–SVA (P = 0.023) between the two groups. Regarding the global alignment assessment schemes, significant differences in the proportion of patients with subcategories of GAP score (P < 0.001) and SAAS (P < 0.001) were observed between the two groups. The non-TPH group comprised more patients with “severely disproportioned” of the GAP score than in the TPH group (46.6% vs 12.3%), whereas more patients showed overcorrection of SAAS in the TPH group than in the non-TPH group (66.2% vs 39.8%). Of the overall study cohort, 41 and 12 patients developed PJK and PJF, respectively with the PJK and PJF rates being significantly different between the non-TPH and TPH groups (29.5% vs 23.1%, P = 0.461 for PJK; 10.2% vs 4.6%, P = 0.239 for PJF) (Figure 2). (A) Number of patients with proximal junctional kyphosis (PJK) in the non-transverse process hook (TPH) and TPH groups. (B) Number of patients with proximal junctional failure (PJF) in the non-TPH and TPH groups.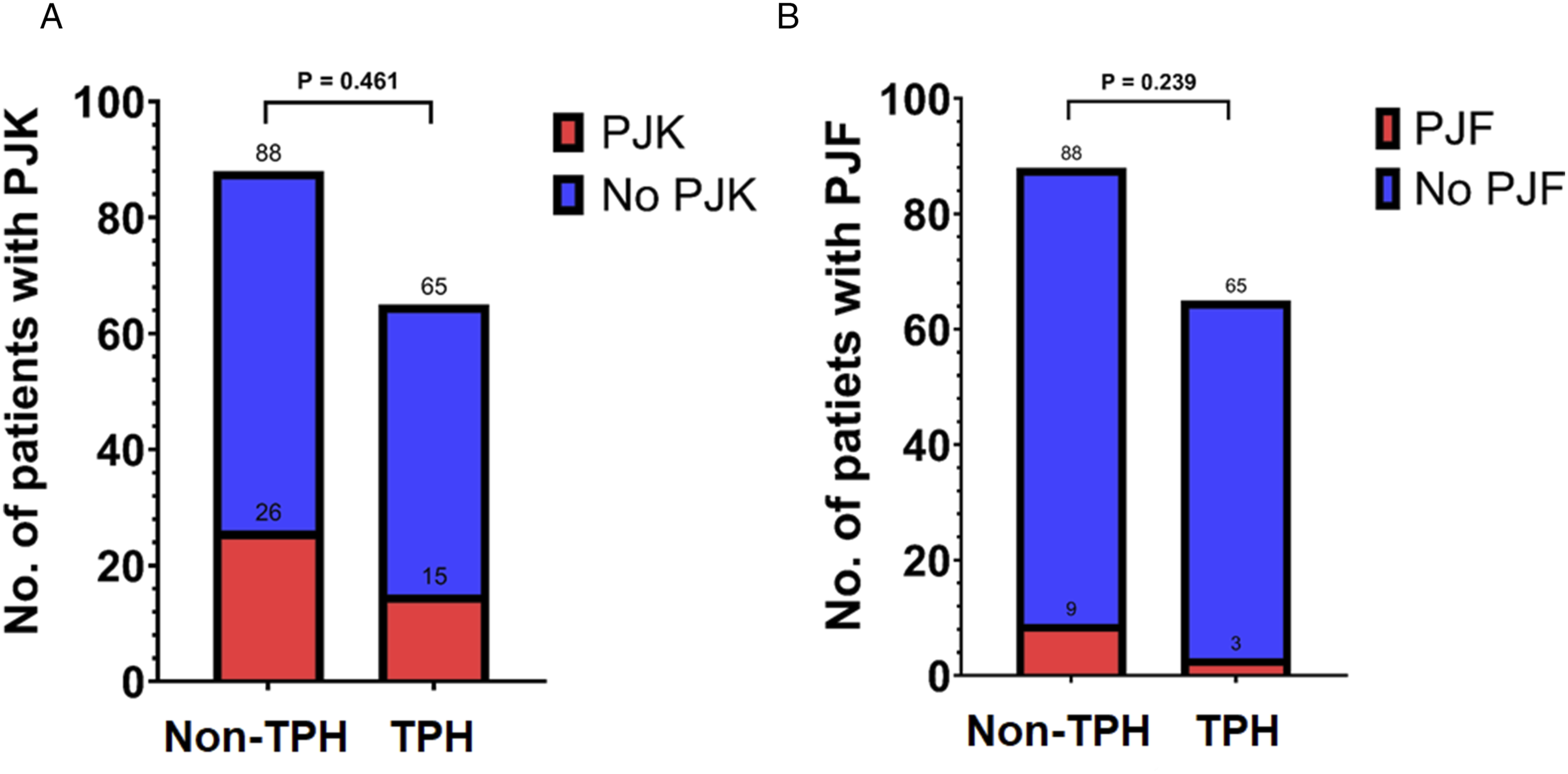
Bivariate and Multivariate Regression Models for TPH Fixation to Prevent PJK and PJF.
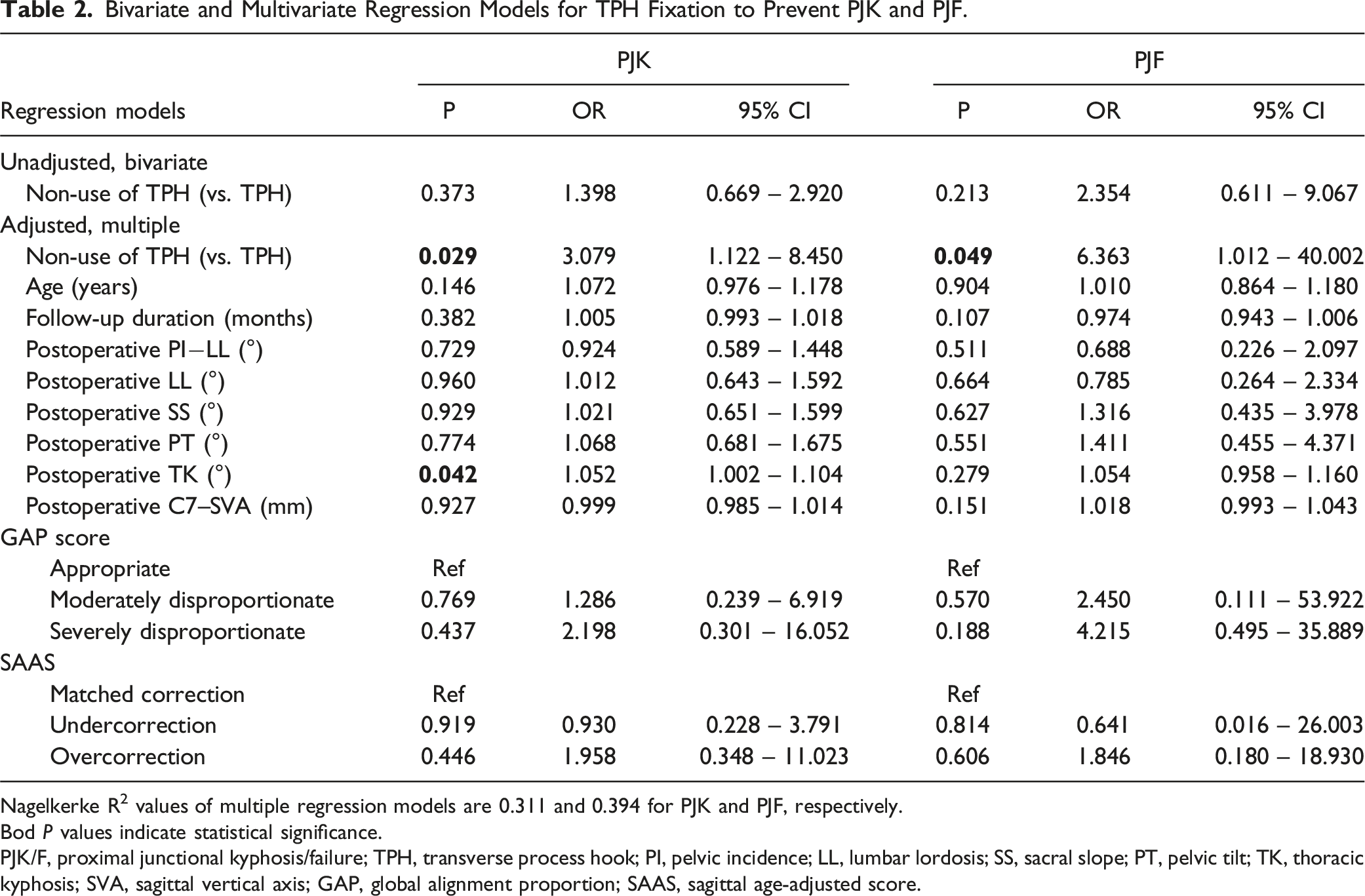
Nagelkerke R2 values of multiple regression models are 0.311 and 0.394 for PJK and PJF, respectively.
Bod P values indicate statistical significance.
PJK/F, proximal junctional kyphosis/failure; TPH, transverse process hook; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; GAP, global alignment proportion; SAAS, sagittal age-adjusted score.
Comparison of Failure Modes and Revision Rates Between Non-TPH and TPH Groups for patients who Developed PJK.
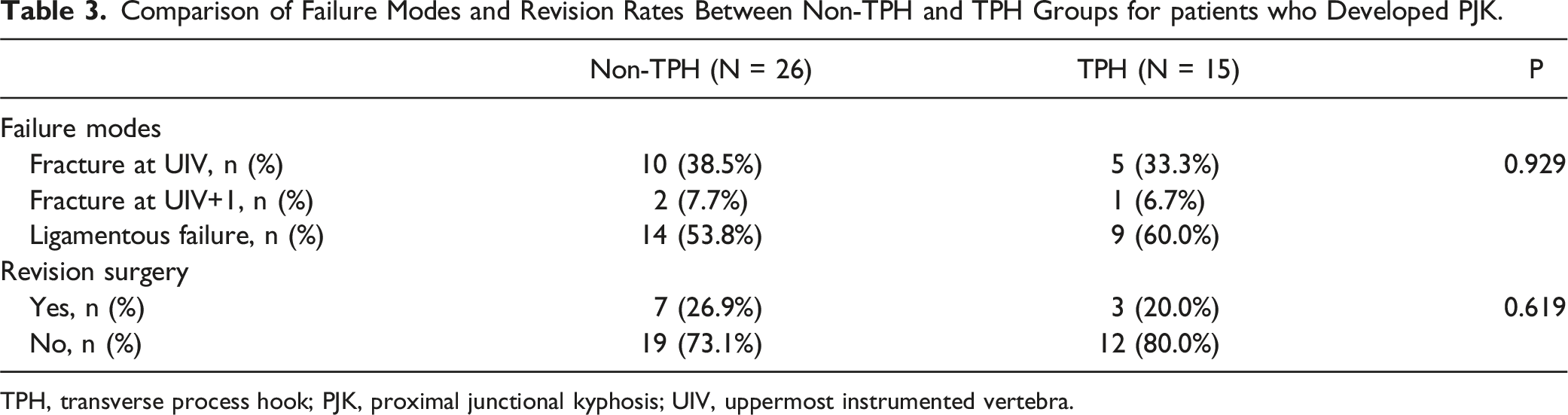
TPH, transverse process hook; PJK, proximal junctional kyphosis; UIV, uppermost instrumented vertebra.
Comparison of Variables Between one- and Two-level TPH Fixation.
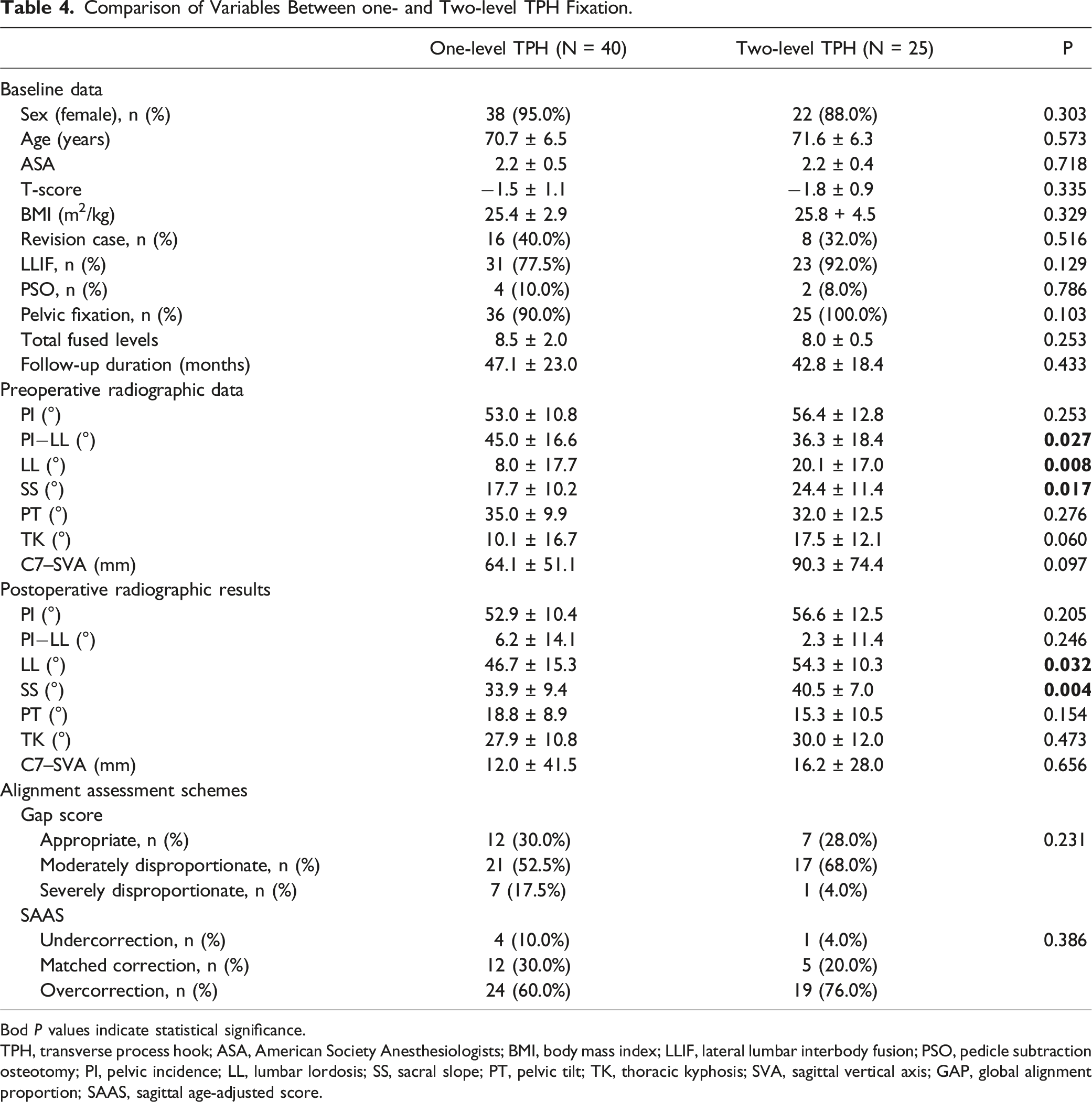
Bod P values indicate statistical significance.
TPH, transverse process hook; ASA, American Society Anesthesiologists; BMI, body mass index; LLIF, lateral lumbar interbody fusion; PSO, pedicle subtraction osteotomy; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; GAP, global alignment proportion; SAAS, sagittal age-adjusted score.
Bivariate and Multivariate Regression Models for Two-level TPH Fixation to Prevent PJK/F.
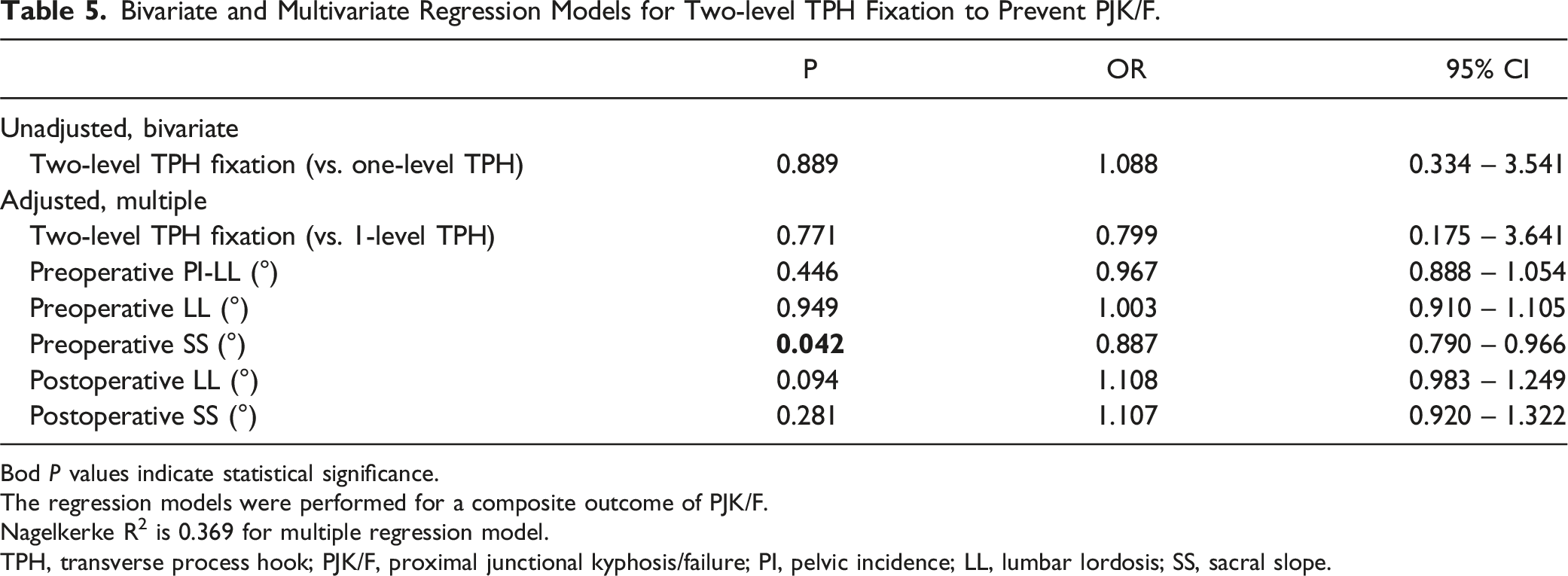
Bod P values indicate statistical significance.
The regression models were performed for a composite outcome of PJK/F.
Nagelkerke R2 is 0.369 for multiple regression model.
TPH, transverse process hook; PJK/F, proximal junctional kyphosis/failure; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope.
Discussion
PJK/F is primarily caused by the increased stiffness of long-segment instrumented fusion and the resultant abrupt changes in segmental motion at the proximal junction. This concept has been supported by several biomechanical studies that have demonstrated more gradual changes in range of motion and less construct stiffness decreased the development of PJK/F.11-14 This mechanism of PJK/F has been also proved by the clinical studies.25-28 Among the diverse surgical techniques for the correction of ASD, multirod construct
25
(vs. dual rods), pelvic fixation
26
(vs. no pelvic fixation), and anterior reconstruction
28
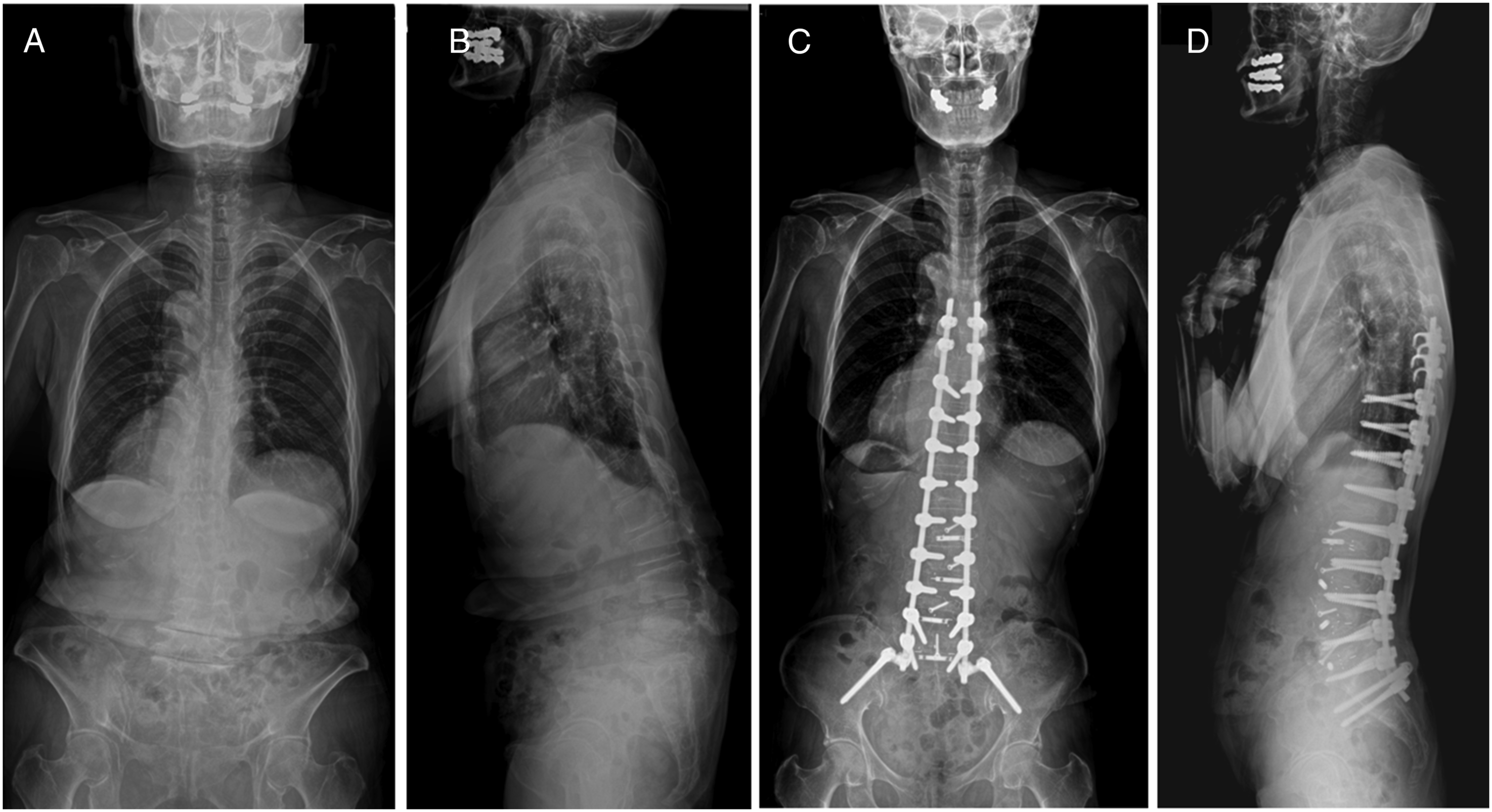
(vs. PSO) increase the risk of PJK/F, all of which are related with increased stiffness of construct. During the past decased, efforts have been made to reduce the abrupt changes in stiffness at the proximal junction. The TPH is a representative surgical tool used to achieve this goal (Figures 3 and 4). Of several local preventive techniques, TPH fixation is easier to perform than other methods, such as posterior tethering, use of additional flexible rods, and use of sublaminar tape, and has no risk of extravasation related to prophylactic vertebroplasty.29-32 Case example 1-level transverse process hook (TPH) fixation. A 74-year-old patient presented with severe back pain due to kyphoscoliosis (Figure A and B). She underwent corrective surgery from T10 to pelvis using TPH fixation at T9. Her sagittal alignment was well maintained until three years postoperatively without proximal junctional complications (Figure C and D). Case example of 2-level transverse process hook (TPH) fixation. A 71-year-old patients presented with stooping due to severe flatback deformity (Figure A and B). She underwent corrective surgery from T10 to pelvis using TPH fixation at T8 and T9. Her sagittal alignment was well maintained until two years postoperatively without proximal junctional complications (Figure C and D).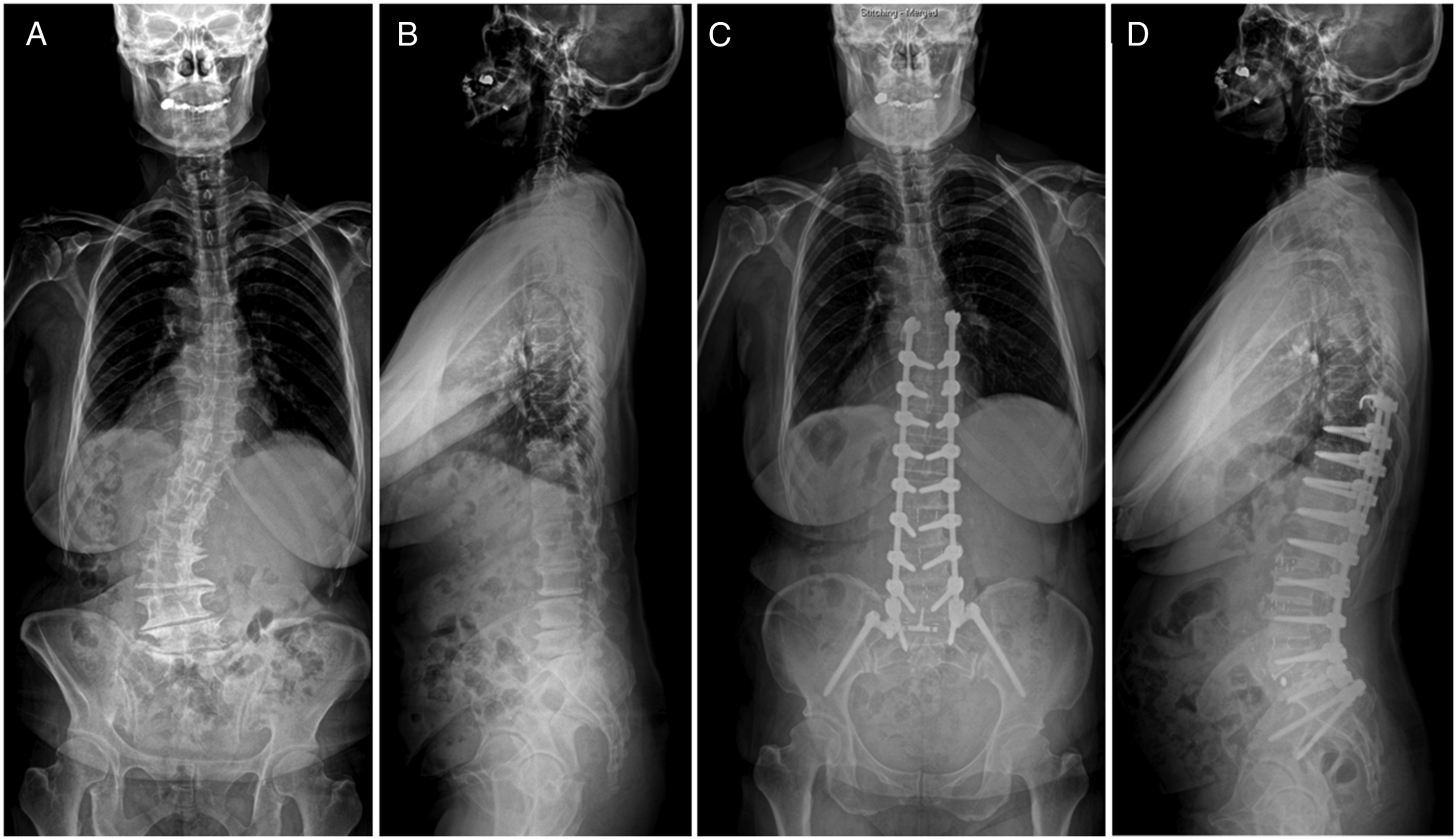
The efficacy of TPH fixation in preventing PJK/F has been well supported by previous biomechanical studies showing a smooth transition of segmental motion from fused to unfused spines.11-14 However, in contrast to the results of biomechanical studies, the clinical results are conflicting. Hassanzadeh et al. evaluated 47 patients, of whom 20 received TPH fixation and 27 received pedicle screws alone as the control group. During a follow-up duration of 2 years, none of the patients in the TPH group developed PJK (defined as PJA > 10°), whereas eight (29.6%) patients in the pedicle screw group developed PJK. 15 However, in Matsumura’s study including 39 patients, the incidence of PJK (defined as PJA > 20°) was comparable between the hook and pedicle screw groups (17.6% vs 27.3%, P = 0.47). 17 More recently, Tsutsui et al. studied 53 patients with 28 patients in the TPH group and 25 in the pedicle screw group. They identified a significantly higher incidence of PJK (defined as PJA > 10°) even in the TPH group than in the pedicle screw group (25.7% vs 8.0%) at a minimum 1-year follow-up. 18
These inconsistent results regarding the efficacy of TPH fixation in preventing PJK/F may be attributable to the relatively small number of patients and, more importantly, the heterogeneity between the groups compared. As decisions regarding whether to perform TPH may not be uniformly made, but largely at the surgeon’s discretion, considering the bone quality, fusion levels, baseline deformity status, and correction magnitude, the groups compared are bound to have inhomogeneous characteristics. These differences in the baseline status between the groups can bias the final results regarding the efficacy of TPH fixation by acting as confounding variables. In the present study, a high grade of heterogeneity in terms of age, follow-up duration, and postoperative correction status was observed between the groups. In particular, the proportions of patients according to the GAP score and SAAS, which are global alignment assessment metric used to predict mechanical failures, significantly differed between the non-TPH and TPH groups. In the unadjusted bivariate analyses (before adjusting for confounders), TPH fixation did not affect the development of PJK and PJF (Table 2). However, multiple regression analyses, including potential confounders, showed that TPH fixation significantly reduced the risk of PJK and PJF by 3.079 and 6.363 times, respectively. These two opposite results of bivariate and multiple regression analyses underscore the importance of confounder control in evaluating the efficacy of local preventive methods.
In patients who developed PJK, no significant differences in failure modes and revision rates were observed between the non-TPH and TPH groups. This finding indicates that once PJK developed even in the use of TPH fixation, the failure mechanisms are similar to those of non-TPH group. In terms of failure modes, ligamentous failure (60.0%) was the most common type in the TPH group, whereas fractures at the UIV or UIV +1 comprised 40% of PJK. This finding suggests that TPH fixation is more effective in preventing fracture-type PJK than soft tissue-type PJK. This result is partly consistent with the lower PJF rates in the TPH group than in the non-TPH group. Considering that the fracture-type PJK has a higher risk of requiring subsequent revision surgery than ligamentous PJK, TPH fixation can be effective in lowering the risk of PJF. Finally, we compared the efficacy of one- and two-level TPH fixation in the prevention of PJK/F. For patients undergoing TPH fixation, confounder-adjusted multiple regression analysis showed that two-level TPH fixation did not further decrease the risk of PJK/F compared with one-level TPH. Therefore, one-level TPH fixation is sufficient to achieve its goal to prevent PJK/F.
This study has several limitations. First, this retrospective study included only patients from a single institution. The patients were not randomly divided; thus, the selection bias in deciding TPH fixation inevitably exists. Second, the study population comprised patients whose UIV was located in the lower thoracic spines (T8–T11) because fusion to the lower thoracic spines is an overwhelmingly more common procedure than fusion extending to the upper thoracic spine in our society. This fusion length-related issue may limit the generalizability of our results to patients who underwent fusion to the upper thoracic spines. Nevertheless, the strict criteria regrading fusion levels in the current study may be advantageous by minimizing fusion length-related bias, considering the lower and upper thoracic spines had the different distinct biomechanical properties.6,33,34 Lastly, the number of patients might be insufficient to perform regression analyses, particularly for PJF prevention and one- and two-level comparisons, potentially leading to overfitting. Therefore, future studies using larger cohorts will be necessary.
Conclusions
The preventive effect of TPH fixation at the UIV +1 against PJK/F development was not significant in the unadjusted bivariate analysis. However, multiple regression analysis adjusted for confounding factors demonstrated that TPH fixation significantly decreased the risk of PJK and PJF. Two-level TPH fixation did not confer additional benefit over one-level TPH fixation in terms of reducing the PJK/F.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
SMC 2024-07-144.