
Abstract
Study design
Retrospective review of a prospectively-collected multicenter database.
Objectives
The objective of this study was to determine optimal strategies in terms of focal angular correction and length of proximal extension during revision for PJF.
Methods
134 patients requiring proximal extension for PJF were analyzed in this study. The correlation between amount of proximal junctional angle (PJA) reduction and recurrence of proximal junctional kyphosis (PJK) and/or PJF was investigated. Following stratification by the degree of PJK correction and the numbers of levels extended proximally, rates of radiographic PJK (PJA >28° & ΔPJA >22°), and recurrent surgery for PJF were reported.
Results
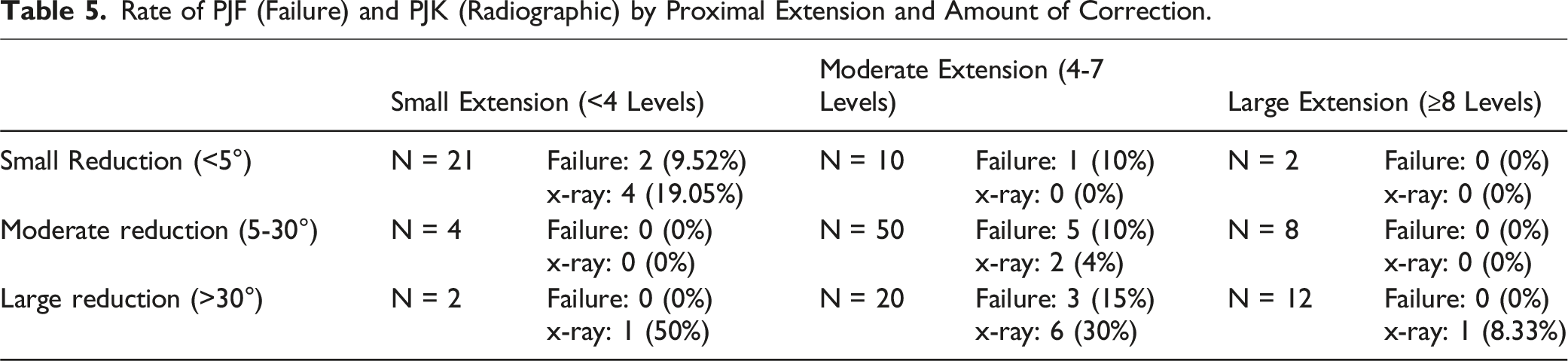
Before revision, mean PJA was 27.6° ± 14.6°. Mean number of levels extended was 6.0 ± 3.3. Average PJA reduction was 18.8° ± 18.9°. A correlation between the degree of PJA reduction and rate of recurrent PJK was observed (r = −.222). Recurrent radiographic PJK (0%) and clinical PJF (4.5%) were rare in patients undergoing extension ≥8 levels, regardless of angular correction. Patients with small reductions (<5°) and small extensions (<4 levels) experienced moderate rates of recurrent PJK (19.1%) and PJF (9.5%). Patients with large reductions (>30°) and extensions <8 levels had the highest rate of recurrent PJK (31.8%) and PJF (16.0%).
Conclusion
While the degree of focal PJK correction must be determined by the treating surgeon based upon clinical goals, recurrent PJK may be minimized by limiting reduction to <30°. If larger PJA correction is required, more extensive proximal fusion constructs may mitigate recurrent PJK/PJF rates.
Keywords
Introduction
Surgery for adult spinal deformity (ASD) results in substantial clinical benefits for selected patients,1-5 however is also associated with high complication rates.6-12 While minor complications are thought to have a relatively limited impact on long-term clinical outcomes in most cases, 13 major complications often result in adverse long-term clinical deficits.13,14 Proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) are major complications associated with long-construct fusions for ASD.15-17 PJK is a radiological finding demonstrating accelerated angular deformity of the spine proximal to the upper instrumented vertebra (UIV),15-17 and may be subclinical in nature. Most used definition for PJK is a kyphotic angle of 10 degrees measure between the UIV and UIV+2 combined with a kyphotic change greater than 10 degrees. 18
Proximal junctional failure (PJF), however, is a more severe variant and is more commonly associated with suboptimal clinical outcomes, including pain, instability and often neurologic injury and need for revision surgery. 19 Furthermore, in those patients requiring cranial extension of their fusion for treatment of PJF, the risk of recurrent PJK and PJF remains unacceptably high, with an estimated incidence of 44.3%. 20
Patient-related, radiographic, and surgical risk factors for primary PJK and PJF development are well-described in the literature.15,21-27 However, evidence-based strategies for prevention of recurrent PJF in revision cases requiring proximal extension of fusion constructs are poorly reported to date. In this study, we evaluated a population of patients with PJF undergoing cranial extension of prior spinal fusions with the goal of defining successful surgical strategies in terms of angular correction and levels of proximal extension for the prevention of recurrent PJF.
Materials and Methods
Patient Population
Retrospective review of a prospectively-collected multicenter database of ASD patients was performed. This study was conducted according to strict institutional review board standards at each institution and abided by ethical guidelines for human subject research (Clinicaltrials.gov identifier: Nct00738439). All included patients provided their informed consent to take part in the study.
All care was provided by specialists with expertise in treating ASD, and all participating centers obtained institutional review board approval for data collection. Inclusion criteria for database enrollment are age ≥18 years and at minimum one of the following: scoliosis >20°, sagittal vertical axis >5 cm (SVA), pelvic tilt >25° (PT) and/or thoracic kyphosis >60° (TK). Exclusion criteria include spinal deformities associated with acute trauma or with autoimmune, neoplastic, neuromuscular, syndromic and/or infectious disorders. For this project, only patients undergoing revision surgery for diagnosis of PJF following posterior correction and stabilization were included. PJF included all types of failures: fracture, kyphosis, hardware loosening, spondylolisthesis… All selected cases were reviewed and validated by an orthopaedic spine surgeon specializing in ASD.
Data Collection
Baseline demographic data including age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) score, and history of prior spinal fusion were collected. Radiographic parameters collected included level of diagnosed PJK, Pelvic Incidence (PI), Pelvic tilt (PT), spino-pelvic mismatch (pelvic incidence minus lumbar lordosis, PI-LL), T10-T12 angle, T1-T12 angle, and T1 Pelvic Angle (TPA). Surgical factors including cranial extent of fusion (number of levels), PJK angular reduction, operative time, estimated blood loss (EBL), surgical approach, neurologic decompression, any osteotomy, 3-column osteotomy, and interbody fusion were collected. PJK angles including upper instrumented vertebra (UIV) to UIV+2, UIV-1 to UIV+1, and UIV-1 to UIV+2 were collected at all timepoints.
Clinical outcomes were collected including revision surgery for any reason, revision surgery for diagnosis of recurrent PJF, and recurrent PJK as defined radiographically according to angle severity (proximal junction (PJ) angle ≥28° and a change in PJ angle ≥22°). 28
Statistical Analysis
For direct comparisons of continuous variables, either unpaired t-test or Man-Whitney U test (depending on appropriateness) were utilized. Appropriateness of testing was determined using the Kolmogorov-Smirnov test for normal distribution. For categorical variables, Chi-squared or Fisher exact test were used. Paired t-test or Wilcoxon signed-rank test were utilized for comparison of variables between pre- and post-operative timepoints. Pearson correlation coefficient was utilized to evaluate correlation.
Results
Baseline Data
A total of 151 surgical cases meeting inclusion criteria were identified in the database. One-hundred-twenty-eight unique patients undergoing 134 unique surgical cases had complete surgical data, pre-revision images, and post-revision images and were included in the analysis. Specifically, this included 122 patients who only underwent 1 revision surgery during the follow-up period and 6 patients who underwent 2 surgeries during this time (Figure 1). The mean age among all patients was 66 (min 33-max 87). Female patients comprised 72.2% of the study cohort. The mean BMI was 28.9 (min 16.8-max 50.2). The mean ASA score was 2.7 (min 2 – max 4). The majority of patients (65.7%) requiring revision for PJK had an original upper instrumented vertebrae (UIV) in the lower thoracic spine (T8-T12). In contrast, 15.7% of patients had a UIV in the upper thoracic spine (T2-T7) and 17.9% of patients had a UIV in the lumbar spine (L1-L3). One patient with a UIV in the cervical region was excluded from the analysis. The large majority (90.3%) of patients had at least one pedicle screw at the UIV, with 8% having some cement at the UIV level. Most (88.8%) of fusions extended caudally to the sacrum and/or pelvis. 56-year-old female underwent initial treatment to correct severe coronal and sagittal lumbar deformity with staged anterior-posterior surgery in 12/2010 (A to B). Patient was reoperated in 11/2011 due to progressive sagittal deterioration combined with coronal decompensation (C). Patient underwent posterior instrumentation from T10 to pelvis with pedicle substraction osteotomy at L3 (D). Patient rapidly presented signs of proximal failure, requiring reoperation in 12/2012 (E). PJF treatment included proximal extension to T3 with reduction of focal kyphosis from 51° to 19° with T10 vertebral column resection (VCR). Patient required second extension for progressive cervico-thoracic focal kyphosis (38°), anterior cervical malalignment (C2-T3 SVA: 14 cm) and neck pain in 11/2013 with posterior instrumentation up to C2 (F).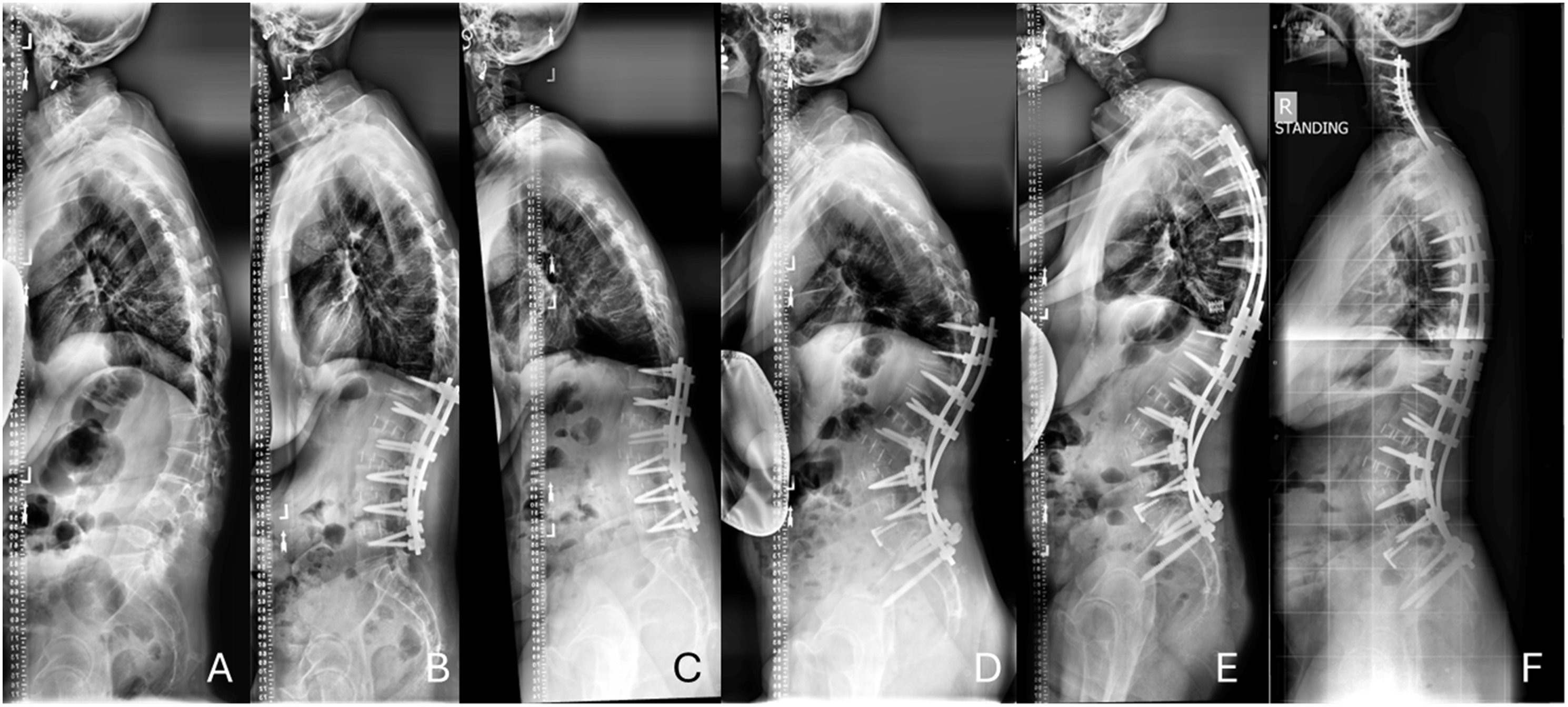
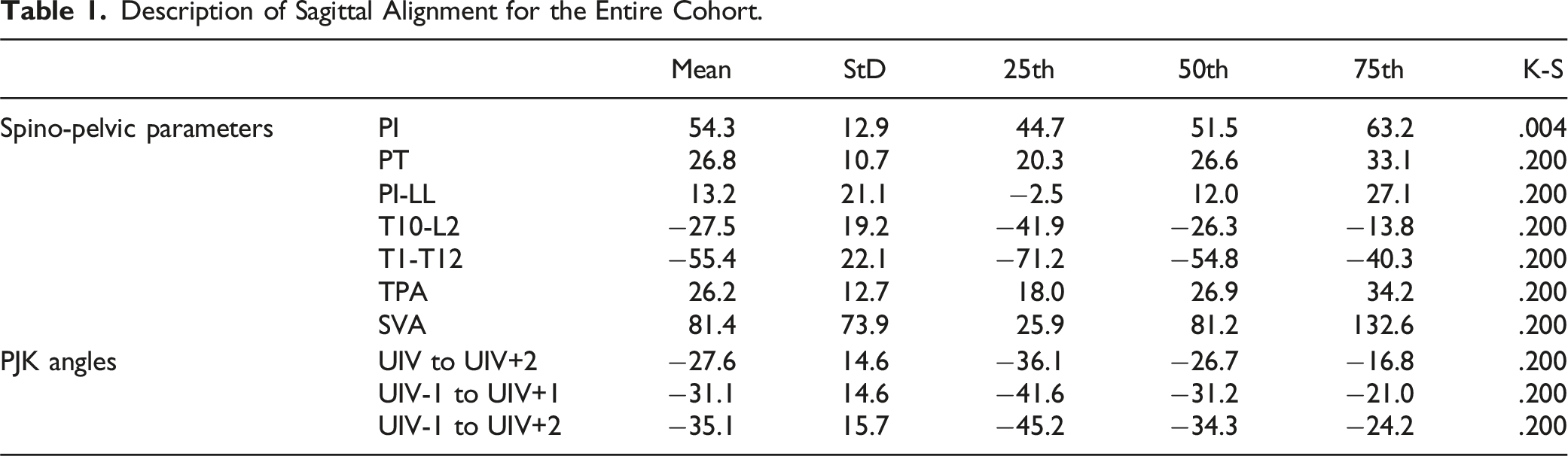
Description of Sagittal Alignment for the Entire Cohort.
Comparison of Sagittal Alignment Parameters Prior to Revision Based upon PJK Location
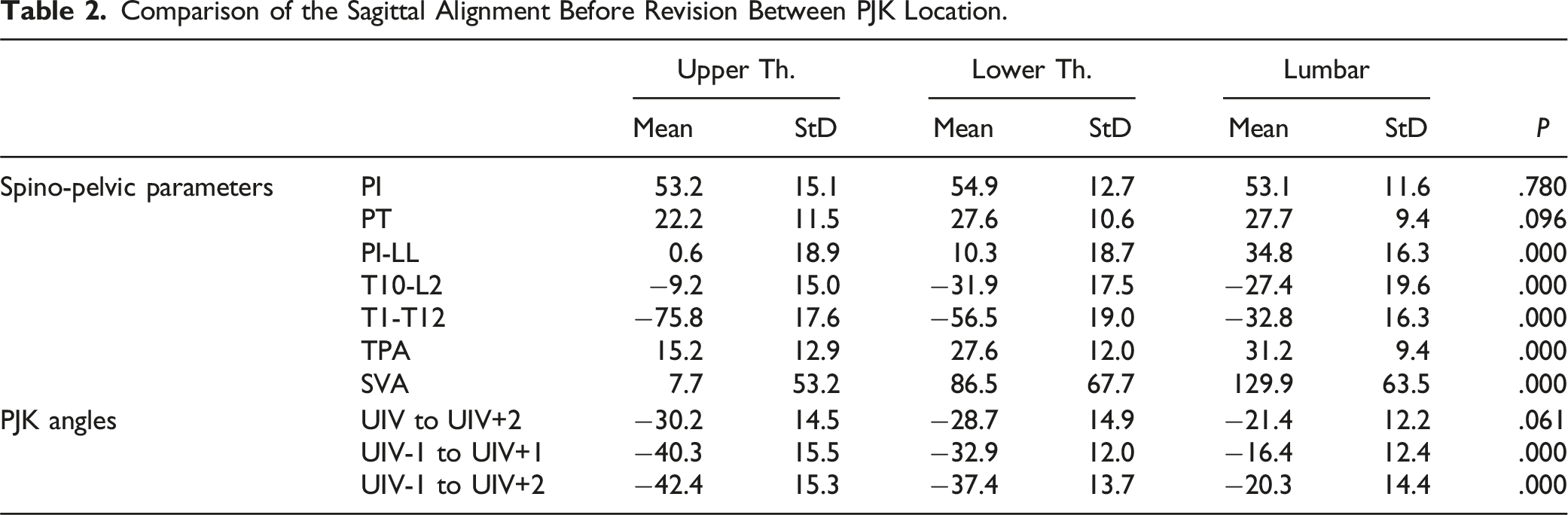
When pre-revision alignment parameters were compared after stratification by UIV level, substantially more global sagittal malalignment was noted in those experiencing PJK at more caudal levels (Figure 2). Specifically, both T1 pelvic angle (TPA) [UT 15.2° ± 12.9° vs LT 27.6° ± 12.0° vs Lumbar 31.1° ± 9.4°, P < .001] and Sagittal vertical axis (SVA) [UT 7.7 mm ± 53.2 mm vs LT 86.5 mm ± 67.7 mm vs Lumbar 129.9 mm ± 63.5 mm, P < .001] were worse in those with lower UIVs and PJK. Likewise, a significant association between lower PJK levels and worse spino-pelvic mismatch (PI-LL) was noted [UT 0.6° ± 18.9° vs LT 10.3° ± 18.7° vs Lumbar 34.8° ± 16.3°, P < .001]. Mean thoracic kyphosis (TK) was larger in those with higher PJK levels [UT 75.8° ± 17.6° vs LT 56.5° ± 19.0° vs Lumbar 32.8° ± 16.3°, P < .001]. More cranial PJK regions were also associated with higher magnitude of 3-segment (UIV-1 to UIV+2) PJK magnitude [UT 42.4° ± 15.3° vs LT 37.4° ± 13.7° vs Lumbar 20.3° ± 14.4°, P < .001] (Table 2). 66-year-old female presents with severe back pain for the past 15 years. History of spine fusion from T11 to pelvis presenting with severe proximal kyphosis (60 deg) (A). Patient treated in 9/2017 with posterior proximal extension from T11 to T3 and Smith-Petersen osteotomy to reduce focal kyphosis to 20 deg (B). Patient underwent revision surgery for painful right iliac screw in 11/2018 (C) and pseudoarthrosis and rod breakage at L5-S1 in 08/2020 (D). New proximal angle went from 7° of lordosis before PJK surgery (A) between T1 and T3 to 24°- kyphotic 4 years post-operative (D). Comparison of the Sagittal Alignment Before Revision Between PJK Location.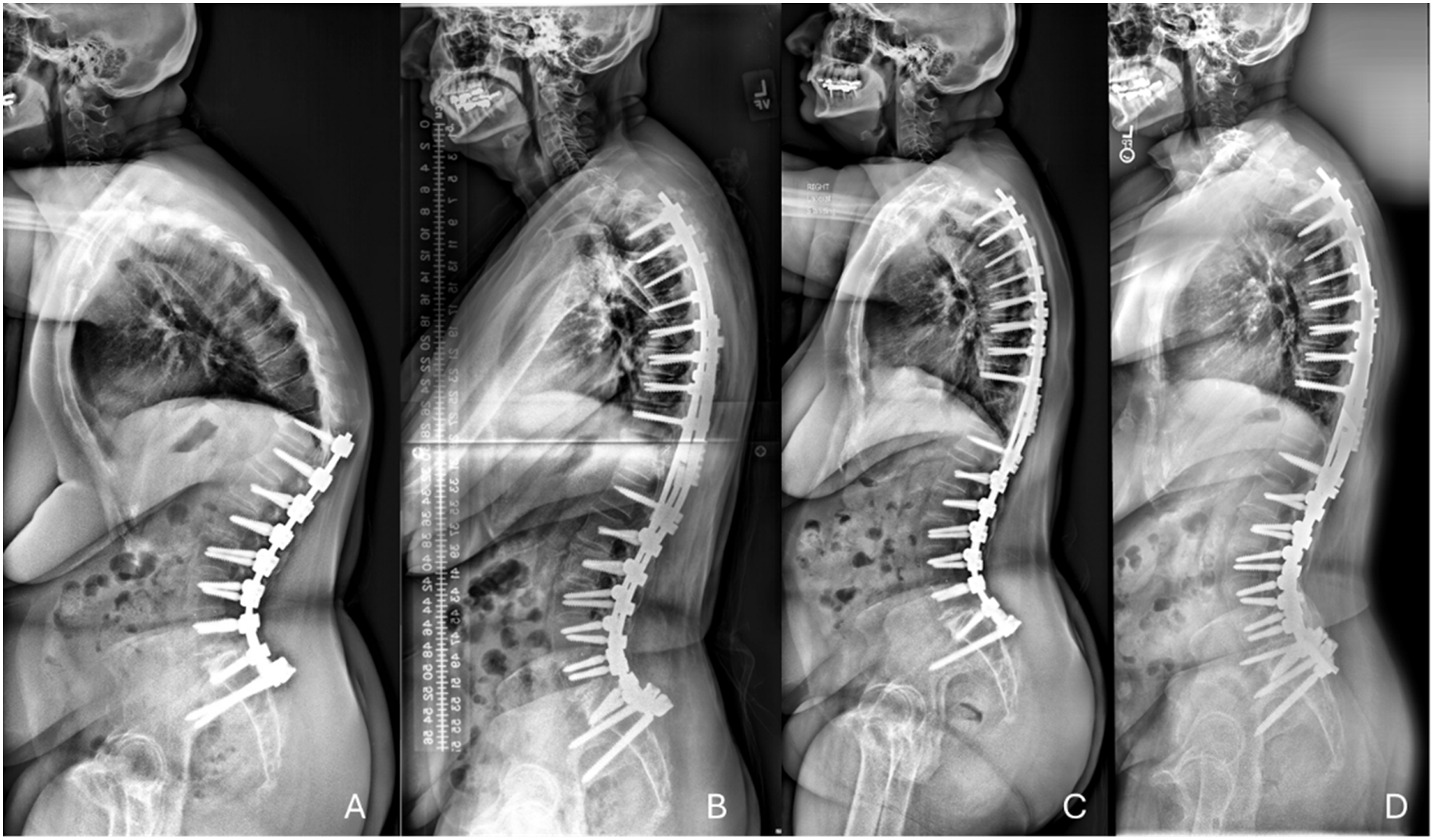
Surgical Metrics
Comparison Surgical Data Between PJK Location.
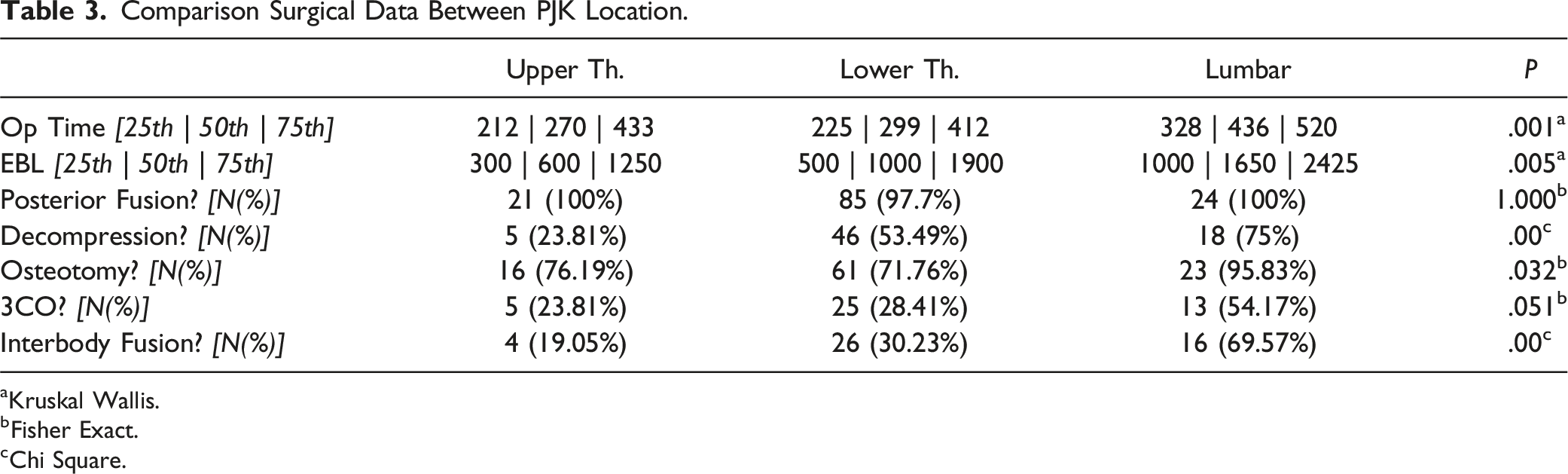
aKruskal Wallis.
bFisher Exact.
cChi Square.
Postoperative Alignment Parameters
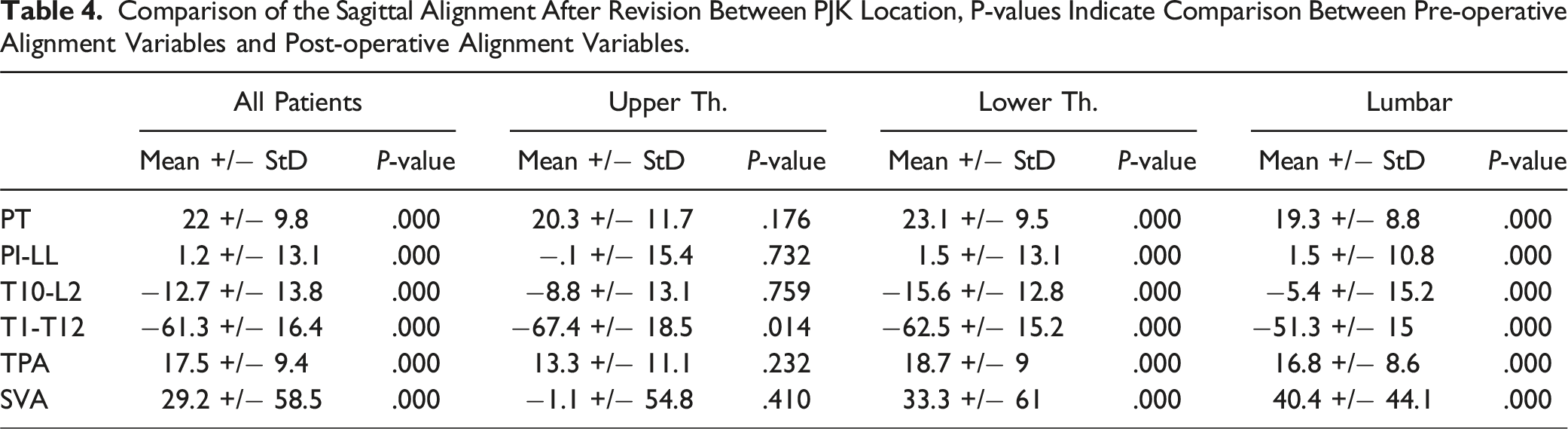
Comparison of the Sagittal Alignment After Revision Between PJK Location, P-values Indicate Comparison Between Pre-operative Alignment Variables and Post-operative Alignment Variables.
Correction Strategies: Proximal Extension and Focal Deformity Reduction
The mean number of levels extended proximally was 6.0 ± 3.3 (23.3% ≤ 3 levels; 16.5% ≥ 9 levels). No significant difference in number of levels extended was noted between PJK level cohorts (UT 4.7 levels vs LT 6.2 levels vs LL 6.3 levels, P = .173). Average PJA reduction (UIV-1 to UIV+2) was 18.8.°±18.9 [<5° (small) for 24.8% of patients, 5 to 30° (moderate) for 49.6% of patients, and >30° (large) for 25.6% of patients]. Larger focal angular corrections were generally required for those with lower PJK levels (all P < .005).
Relationship Between Focal Deformity Correction, Proximal Extension, and Recurrent PJF Rates
No significant association between amount of focal angular reduction and new PJK angle was noted (all P > .05). While the degree of PJA reduction was correlated with the recurrent radiographic PJK (r = −.222), there was no statistically significant difference between amount of angular reduction and recurrent PJF (as measured by need for another revision). Small (<5°) and large (>30°) angular reductions were both associated with increased radiographic recurrent PJK rates (small 18.2% vs moderate 9.1% vs large 29.4%, P < .037). While no significant differences between amount of proximal extension and either PJK (small [<4 levels] 16.1% vs moderate [4-7 levels] 10.0% vs large [≥8 levels] 4.5%, P = .478) or PJF (small [<4 levels] 6.5% vs moderate [4-7 levels] 11.3% vs large [≥8 levels] .0%, P = .291) was noted, there was a trend toward lower rates of both in those undergoing longer extension of their fusions.
Rate of PJF (Failure) and PJK (Radiographic) by Proximal Extension and Amount of Correction.
Discussion
Despite widespread awareness among spine surgeons as well as numerous technical advancements in the field, PJK and PJF continue to result in substantial morbidity for ASD patients. Patient-related, surgical, and biomechanical risk factors for PJK and PJF have been studied extensively, as have a number of strategies for prevention.17,23,25,29-39 Nevertheless, the optimal revision strategy for patients who have already experienced PJF, in order to prevent recurrent failure, remains unknown. Patients who have already experienced proximal junctional failure are at an inherently higher risk of experiencing the same phenomenon again following revision surgery, with recurrence rates estimated at 44%.
20
This at-risk population requires special consideration in order to prevent a cascading pattern of multiple surgeries resulting in more and more proximal fusion levels and associated increases in morbidity and mortality. This study sought to determine the optimal biomechanical revision strategy for such patients in terms of both focal angular correction and levels of proximal extension. Because there is an inherent biomechanical relationship between focal deformity correction and the length of the lever arm created by proximal extension of the fusion, it is logical that these factors should be considered in tandem. This study determined that those with large focal reductions and minimal extension proximally were at the highest risk of recurrent failure. Yang et al, in an evaluation of 763 operative ASD patients, similarly concluded that overcorrection was associated with significantly increased risk or PJF.
27
Some authors, with the hopes of minimizing the risk or PJK and PJF, have advocated for concepts including intentionally less aggressive correction targets and age-adjusted alignment goals.40,41 Nevertheless, it appears that under-correction, even when using age-adjusted alignment targets, is common, with one recent paper citing under-correction rates of 30.3% for SVA, 41.0% for PT, and 43.6% for PI-LL when measured with postoperative full-body radiographs .
42
Such under-corrections are noted to necessitate substantial compensatory mechanisms, including increased posterior pelvic shift, knee flexion, thoracic hypokyphosis, and cervicothoracic compensation.40,41 Our finding that small angular reductions were also associated with increased radiographic PJK rates suggests that under-correction of focal malalignment with small proximal extension of fusion is not a viable strategy for prevention of recurrent PJK. Large focal reductions are often required in these cases in order to restore global sagittal alignment and achieve the primary goals of surgery. Rather, in patients who require a large angular reduction for correction of existing PJK, this data suggests that surgeons might consider more extensive fusions proximally, as this may mitigate the risk of recurrence. Daniels et al, comparing patients undergoing fusions from the pelvis to either lower or upper thoracic upper instrumented vertebrae (UIVs), found that upper thoracic UIVs were associated with both greater sagittal vertical axis (SVA) improvement and lower PJK rates.
43
Additionally, the authors noted that greater coronal cobb angle, greater thoracic cobb angle, and performance of a 3-column osteotomy were all associated with surgeon decision to fuse to the upper thoracic spine. This indicates that the bias of most surgeons treating ASD is already to increase the levels of proximal fusion in cases where large angular corrections are required. The current study complements the prior literature by introducing objective criteria for a reasonable amount of proximal extension needed based upon the focal correction required. Surgeons should consider more cephalad UIV choices when performing large angular corrections (Figure 3). Standing sagittal films of 68-year-old female with low back pain and neurogenic claudication attributable to adult spinal deformity (A). Following initial treatment with 2-stage T10-Pelvis fusion construct, the patient re-presented with increasing low back pain and decompensated sagittal balance (PJA 34°) (B). The patient underwent a large (31°) PJK correction and moderate (6 level) proximal extension of fusion (D). Unfortunately, she experienced recurrent PJF with new PJA of 45° (E). She then underwent a moderate (22°) angular correction and moderate (5 level) proximal extension to C6, with maintenance of correction at 6-month follow-up examination (F).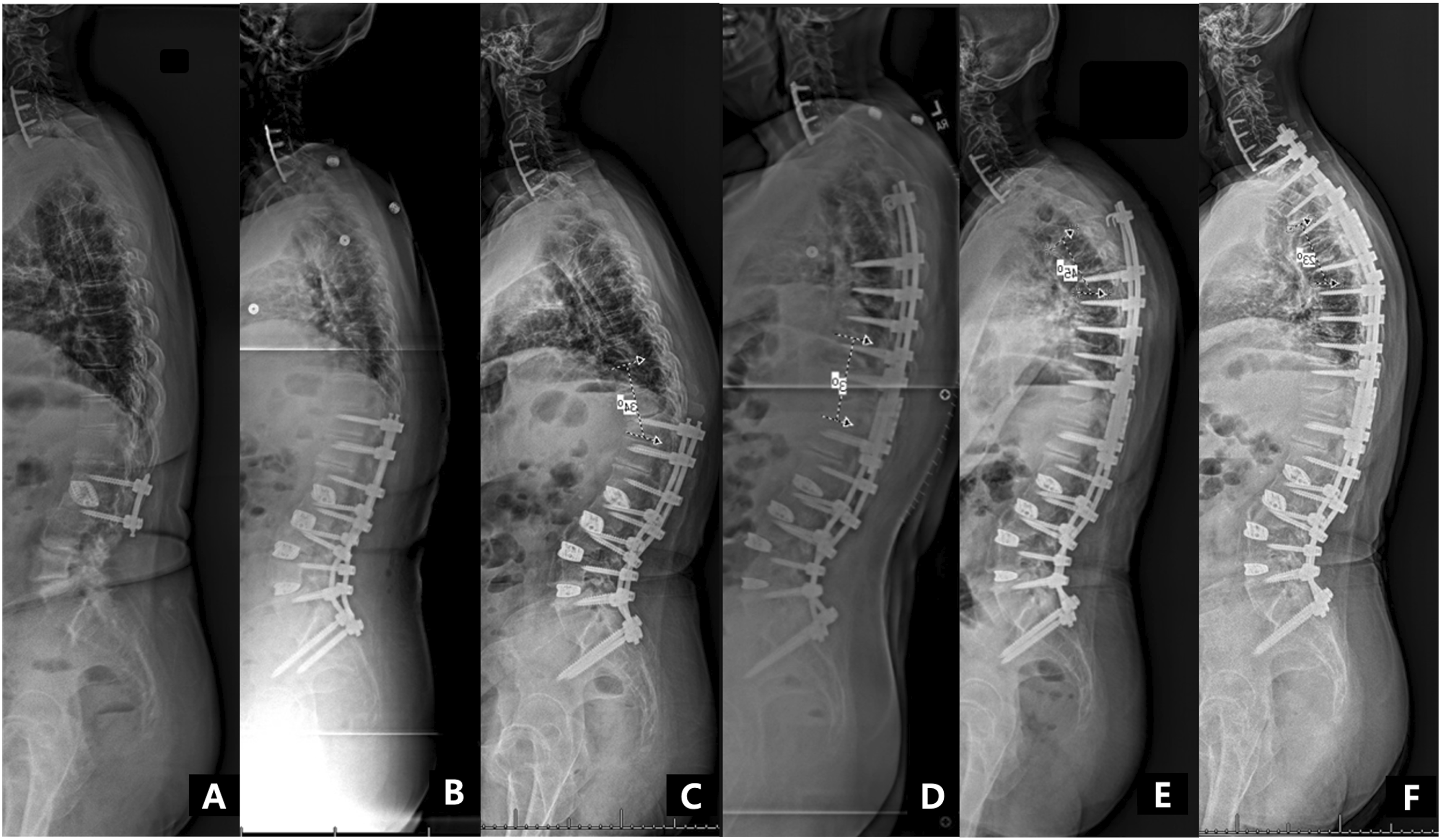
A number of important study limitations merit discussion. First, this study was a retrospective review of a prospectively-collected database. No randomization was performed, and the decision regarding angular correction and extent of proximal extension was ultimately determined according to the best judgement of the treating surgeon. For example, in the large majority of cases resulting in small angular corrections, the surgeon elected to perform small proximal extensions of fusion. Disassociating this interaction was impossible in this study. Secondly, this study was only able to adequately analyze surgical strategy for revision of PJK in terms of angular correction and proximal extension. A number of other factors likely important for the prevention of recurrent PJK were not included in this limited analysis. Suboptimal alignment of fusion caudal to the PJK, for example, may predispose patients to recurrent junctional issues. Given the low number of cases in which distal alignment was changed in our series, such variables are unable to be studied with adequate power. Additionally, given the rolling prospective nature of data collection in this database, there is significant variability in final follow-up time between patients, which introduces the potential for bias. Important parameters that most likely significantly impact decision strategy and maintenance of the results were also missing due to the retrospective nature of this analysis, with bone health (BMD) and posterior muscle quality being the two main ones. Finally, it should be noted that while the majority of patients in this study presented with PJF at the low thoracic level, patients with PJF at the high thoracic and lumbar levels were also included. This was necessary in order to increase the power and generalizability of the study, however also introduces substantial variability. The biomechanical forces acting on the upper thoracic, lower thoracic, and lumbar spine are inherently different, and the optimal numbers in terms of angular correction and proximal extent of fusion may be different depending upon which part of the spine is being treated. Despite this fact, the core concept introduced by this study, that larger angular corrections require more proximal extensions of fusion in order to optimize stability, is likely universal. Further studies with increased power for sub-stratification between regions are necessary to establish more accurate surgical goals.
Conclusion
Our understanding of the radiographic and biomechanical predictors of proximal junctional failure following surgery for adult spinal deformity has grown exponentially in recent years. Nonetheless, surgical strategies for focal correction and proximal fusion levels continue to vary widely, especially amongst those undergoing revision surgery. In order to provide optimal surgical care for this high-risk patient population, a higher level of reproducibility and predictability must be achieved. This study establishes principals for focal correction goals and proximal fusion levels. Specifically, for large PJK angle corrections, surgeons should consider large proximal extensions. Such guidelines may help with surgical planning and reduce preventable complications in this high-risk patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the International Spine Study Group Foundation (ISSGF). The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2M (current), Innovasis (past), Biomet (past), and individual donations. Funding sources did not play a role in investigation.