
Abstract
Study Design
Retrospective cohort study.
Objectives
This study aimed to examine the incidence and risk factors for recurrent proximal junctional failure (R-PJF) in adult spinal deformity (ASD) surgery.
Methods
Among 482 patients receiving ≥ five-level fusion to the pelvis for ASD, 60 patients who underwent fusion extension surgery for PJF were included in the study cohort. R-PJF was defined as the performance of re-revision surgery after revision surgery for PJF. Various clinical and radiographic variables were compared between no R-PJF and R-PJF groups. Stepwise multivariate logistic analysis was performed to identify the risk factors for R-PJF.
Results
Of the 60 patients, there were 51 women (85.0%) and 9 men (15.0%) with a mean age of 72.4 ± 6.7 years. The mean fusion length at the index surgery was 7.3 ± 1.6 levels and an average of 4.1 ± 1.3 levels was extended during the revision surgery. Among them, R-PJF developed in 17 patients (28.3%). Multivariate analysis revealed that overcorrection relative to age-adjusted pelvic incidence (PI) – lumbar lordosis (LL) at the index surgery and high total sum of proximal junctional kyphosis severity scale (PJKSS) at the revision surgery were significant risk factors for R-PJF development. The cutoff value for the PJKSS sum was calculated as 8.5 points.
Conclusions
R-PJF was developed in 17 patients (28.3%). PI–LL overcorrection should be avoided during the index surgery to mitigate the R-PJF. In addition, timely surgical intervention is required in patients with PJF, considering that the PJF severity tends to increase over time.
Keywords
Introduction
Proximal junctional failure (PJF) is one of the most common mechanical complications after adult spinal deformity (ASD) surgery. Unlike proximal junctional kyphosis (PJK), PJF is a structural failure that can result in significant clinical consequences such as increased deformity, aggravated pain, late-onset neurologic deficit, and subsequent revision surgery.1-7 The revision rate for PJF is reportedly 10%-20% among patients undergoing ASD surgery.8-10
Despite the extensive studies to prevent PJF development, PJF and subsequent revision surgery cannot be completely avoided likely due to its multifactorial etiologies. When the revision surgery for PJF is performed, it generally involves extending the fusion proximally to correct the kyphotic segment and stabilize the spine. Additional laminectomy at the PJF level is sometimes necessary in the case of thoracic myelopathy due to spinal cord compression. Although there has not been much research, some patients experience recurrent PJF (R-PJF) despite a revision surgery for PJF, necessitating re-revision surgery. 11 When revision surgery is planned, it is even more important to prevent the re-revision surgery because the re-revision procedure will impose a significant economic and physical burden on the patients. 12 Therefore, proper surgical strategies are necessary during revision surgery, particularly in patients with a high risk for developing R-PJF.
In the literature, various risk factors for PJF occurrence have been identified including older age, low bone quality, greater preoperative sagittal imbalance, excessive surgical correction of sagittal imbalance, and ending the fusion at the thoracolumbar junction.1,6,7,13-16 However, the risk factors of R-PJF after revision surgery for PJF have been poorly documented in the literature. Thus, the purpose of this study was to examine the incidence and risk factors of R-PJF in patients who underwent revision surgery for PJF in ASD surgery.
Materials and Methods
This study was approved by the institutional review board of our institution (IRB no. 2024-07-144). The requirement for informed consent was waived due to the retrospective nature of this study.
Study Population
This study was a retrospective case series, and all patient records were retrieved from a prospective ASD database at our tertiary hospital. The study cohort consisted of consecutive patients who underwent surgery for degenerative ASD from 2012 to 2023. The inclusion criteria for the overall database at the index procedure were as follows: 1) adult patients with radiographic signs of spinal deformity in the sagittal and/or coronal plane, defined by one or more of the following: C7 sagittal vertical axis (SVA) ≥ 50 mm, pelvic incidence (PI) - lumbar lordosis (LL) mismatch ≥10°, pelvic tilt (PT) ≥ 25°, or coronal Cobb angle ≥30°; 2) fusion of ≥5 vertebral levels, including the sacrum or pelvis. Pelvic fixation was routinely performed using conventional iliac screws, except in cases of L5-S1 fusion due to previous surgery. Patients were excluded if they had neuromuscular, inflammatory, or other pathological conditions rather than degenerative ones; underwent revision surgery for reasons other than PJF such as rod fractures; or lacked appropriate radiographic data. For the current study, we only retained patients who underwent revision surgery for PJF following their index deformity procedures. All of the surgeries were performed by 2 surgeons at our institution (S-J P and C-S L).
R-PJF was defined as a case necessitating re-revision surgery due to recurrent proximal junctional complications developing after revision surgery. Among patients who were revised for PJF, patients who experienced R-PJF at any time, or had a ≥ 1-year follow-up duration in cases without R-PJF development were included in the final study cohort. Therefore, patients who did not develop R-PJF but followed up for less than 1 year were excluded.
Following revision for PJF, these patients were divided into 2 groups according to the development of R-PJF: no R-PJF and R-PJF groups. The decision to perform re-revision surgery was made based on clinical factors such as pain severity, neurological status, progression of the deformity observed on radiological examination, and the general condition of the patients to tolerate the surgery. Two patients were scheduled to undergo re-revision surgery, but their condition deteriorated, and surgery was finally canceled. We included these patients in the R-PJF group because both the surgeons and the patients agreed to the necessity of the surgery.
Data Collection
Basically, data were collected at the time of revision surgery; however, some radiographic variables were also obtained from the index surgery. Patient factors included age, sex, T-score (on hip bone densitometry), osteoporosis (defined as a hip bone T-score ≤ -2.5), body mass index (BMI), and American Society of Anesthesiology (ASA) grade. Surgical factors included total level fused after index procedure, time from index surgery to revision surgery, performance of laminectomy at the PJF level, number of fusion levels extended, final uppermost instrumented vertebra (UIV) level (T1-4 vs T5-8 vs T9-11), and transverse process (TP) hook fixation at UIV+1 level.
Radiographic evaluations were performed at two-time points: immediately after the index procedure and at the time of revision surgery. In this study, we included the radiographic data at the index surgery because we thought that immediate correction status after index surgery may affect the post-revision outcomes, and it is difficult to assess the correction status properly at the time of revision surgery due to correction loss within the instrumented segments and compensatory changes in response to PJF development. Regarding the conventional radiographic parameters, pelvic incidence (PI), lumbar lordosis (LL), PI–LL, sacral slope (SS), pelvic tilt (PT), thoracic kyphosis (TK), T1 pelvic angle (TPA), and C7-sagittal vertical axis (C7–SVA) were measured at 6 weeks after index procedure, before revision surgery, and after revision surgery. The global correction status after the index surgery was assessed using previously established metrics of the age-adjusted PI–LL scheme, the Global Alignment and Proportion (GAP) score. The age-adjusted PI–LL target was calculated using the previously reported formula: PI–LL= (age – 55) / 2 + 3.17,18 Matched correction relative to the age-adjusted PI–LL target indicates current values within a ±10-year range from the calculated ideal target; overcorrection was defined when PI–LL was less than the suggested target range (eg, <10 years). 19 There were no patients with undercorrection relative to this target after the index surgery. Therefore, correction status relative to the age-adjusted PI–LL was evaluated on 2 categories of matched correction and overcorrection. The GAP score was evaluated using an original GAP scoring system as follows: proportional (≤2 points); moderately disproportional (3-6 points); and severely disproportional (≥7 points). 20
Last, the severity of PJF at the revision surgery was assessed using the proximal junctional kyphosis severity scale (PJKSS) introduced by the Hart–International Spine Study Group (ISSG).21,22 This scoring system consists of 6 categorical components; neurological deficit, focal pain, instrumentation problem, change in kyphosis/posterior ligamentous complex, UIV/UIV+1 fracture, and level of UIV. Each component was further categorized and assigned a specific point value to each category, with a maximum PJKSS total score of 15 points.
Statistical Analysis
The data are presented as frequencies with percentages for categorical variables and as means with standard deviations for continuous variables. Bivariate analyses comparing the variables between the 2 groups were performed using the Chi-square test or Fisher’s exact test for categorical variables and the independent t test or Wilcoxon rank-sum test for continuous variables. Stepwise multivariate logistic regression analyses were performed using all variables that had significance <0.20 upon bivariate analyses to identify the independent risk factors for R-PJF. Receiver operating characteristic (ROC) curve analysis was performed to calculate the cutoff value of the designated risk factor. Statistical analyses were performed by professional statisticians using SPSS (version 27.0.0; IBM Corp., Armonk, NY, USA). A P-value <0.05 was considered statistically significant.
Results
Baseline Data
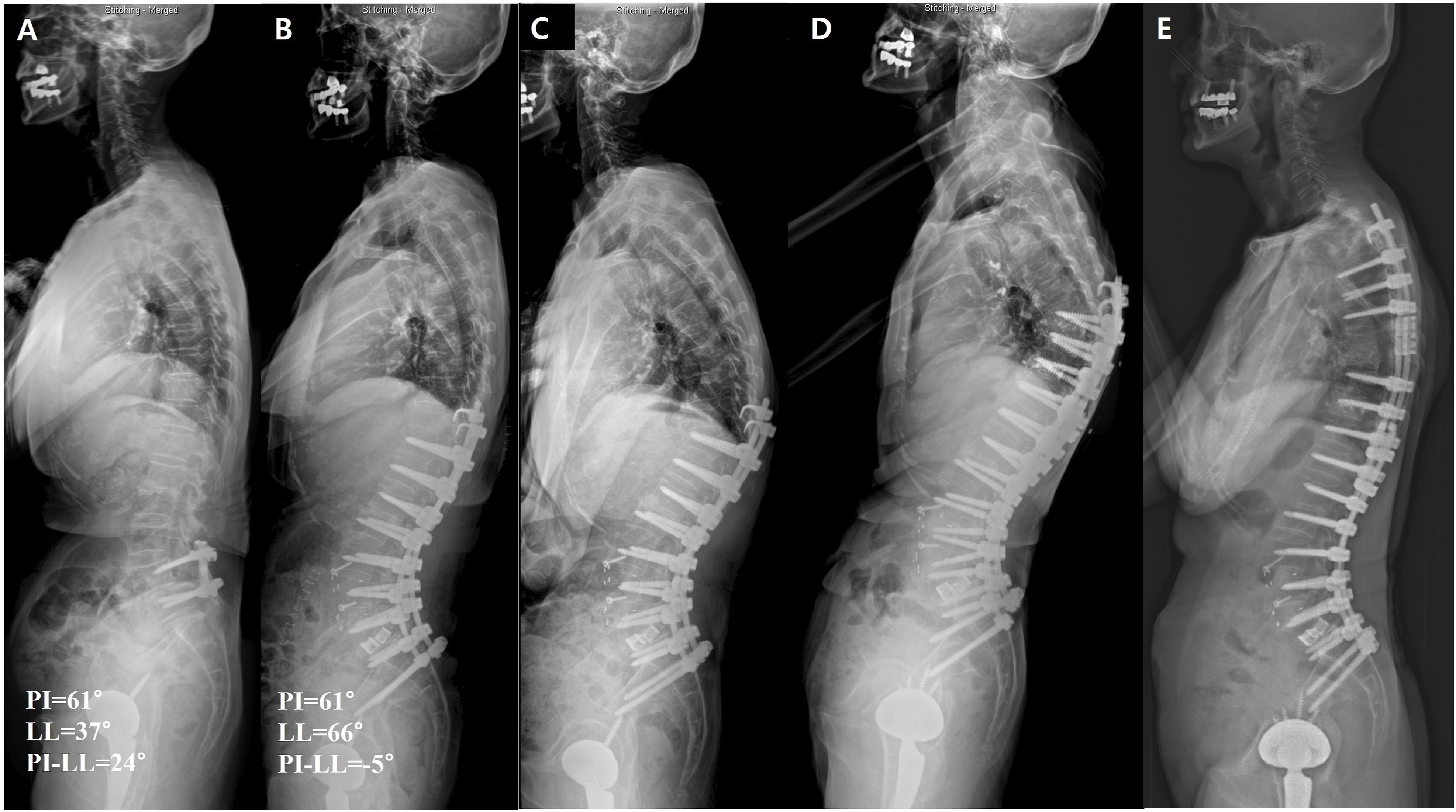
Of 482 patients with ≥ 5-level fusion to the pelvis, 67 patients underwent revision surgery for PJF. After excluding 7 patients due to early (<1 year) loss of follow-up without re-revision surgery, a total of 60 patients comprised the final study cohort (Figure 1). The mean fusion length at the index procedure was 7.3 ± 1.6 levels. There were 51 women (85.0%) and 9 men (15.0%) with a mean age of 72.4 ± 6.7 years at revision surgery. During the mean follow-up duration of 24.3 ± 20.6 months (range: 1.7 - 94.1 months) after revision surgery, 17 patients (28.3%) underwent re-revision surgery and were assigned to the R-PJF group (Figure 2). Flowchart showing the patient selection process. A case of a 75-year-old woman with R-PJF. (A) Preoperatively, her PI, LL, and PI–LL were 61°, 37°, and 24°, respectively. (B) After corrective surgery, LL improved to 66° with a PI–LL of −5°. This PI–LL was overcorrected relative to the age-adjusted PI–LL target. (C) The patient developed PJF with a PJKSS score of 10 points. Following the overcorrection, recurrent anterior dislocation of the existing hip prosthesis occurred due to posterior impingement caused by pelvis retroversion. This necessitated a cup revision between time points (C, D). (D) Fusion extension surgery was performed, but R-PJF developed. (E) Finally, re-revision surgery was done by extending fusion to T4.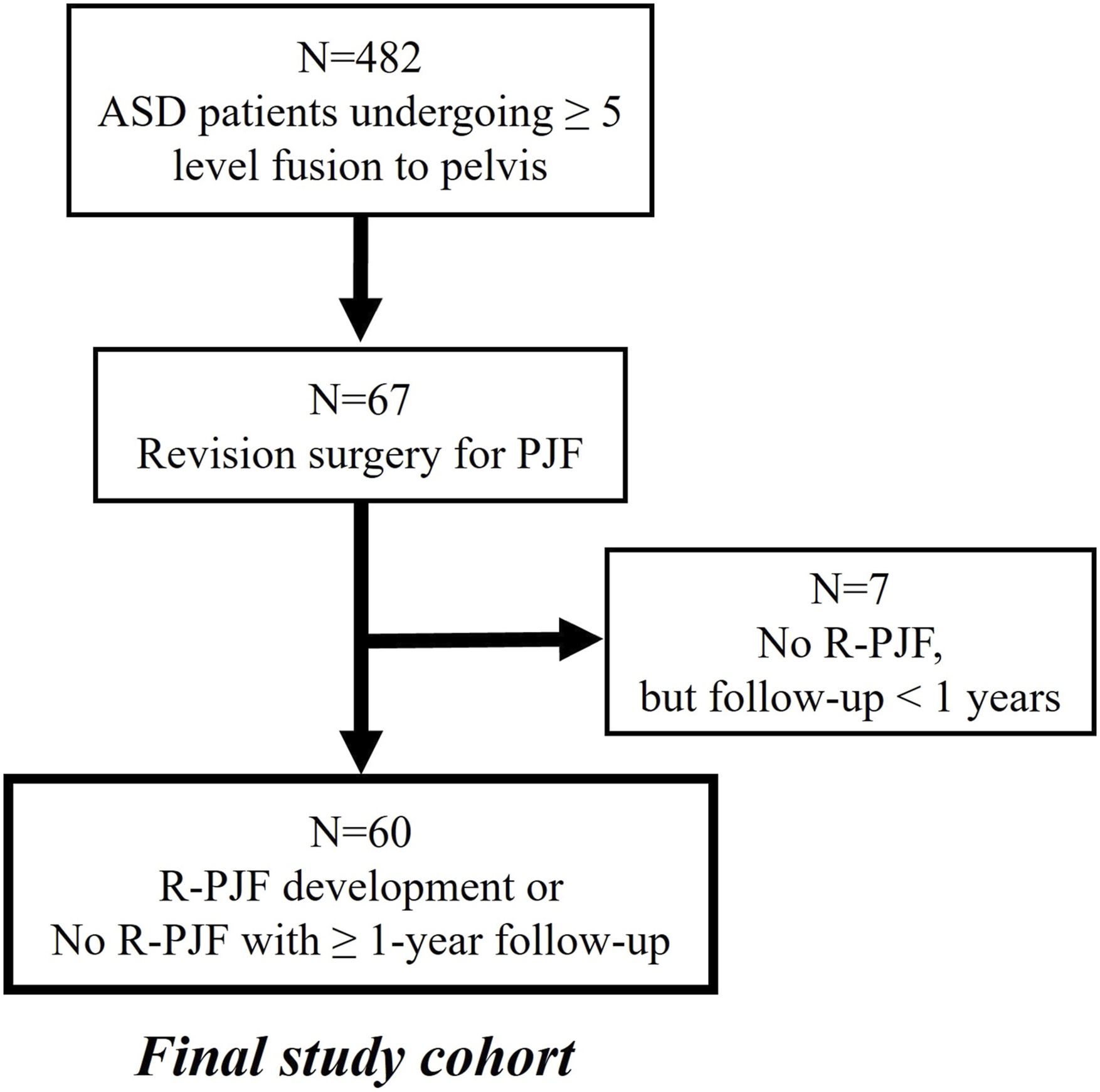
Bivariate Analyses
Comparison of patient and Surgical Factors.
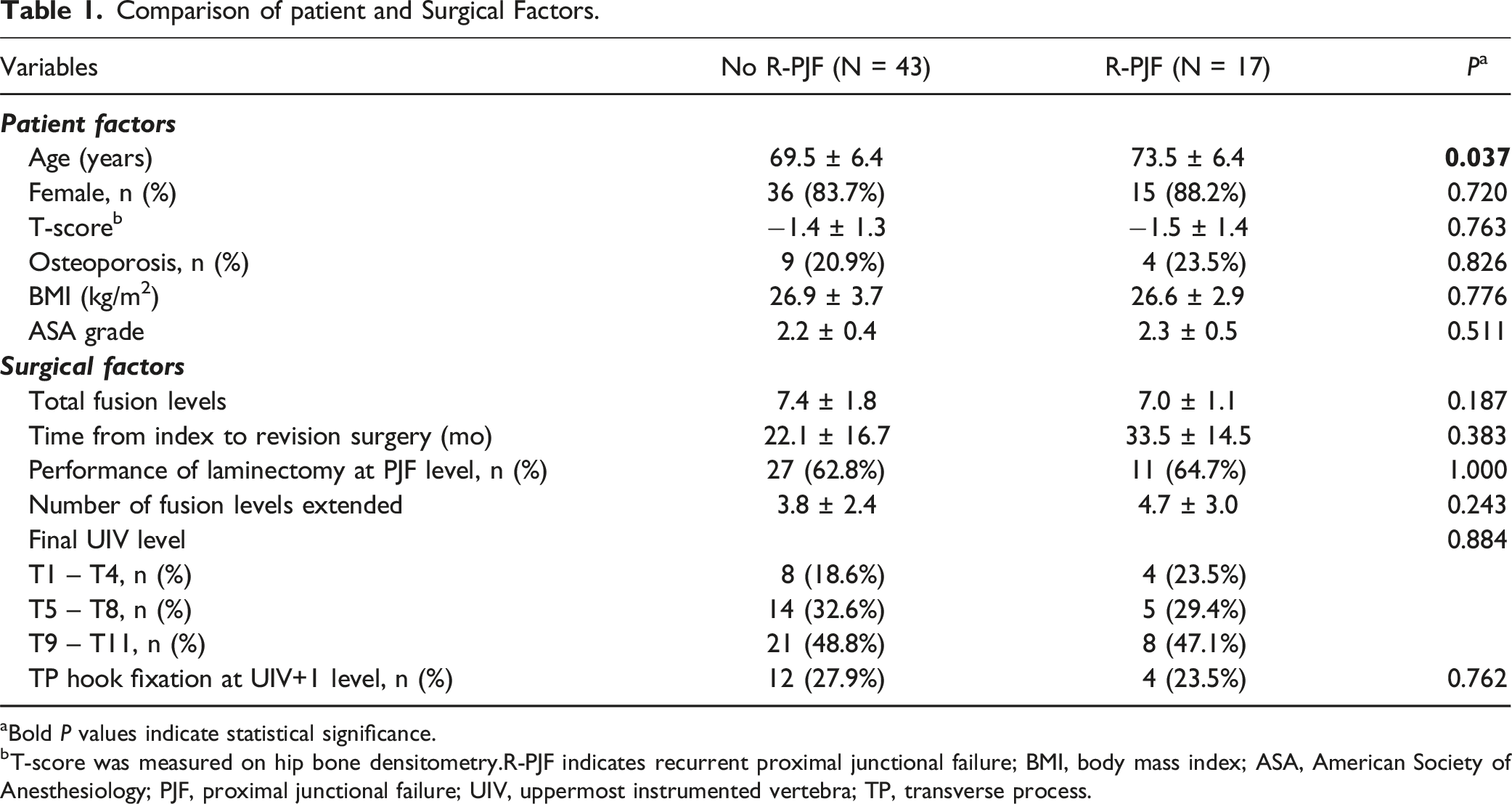
aBold P values indicate statistical significance.
bT-score was measured on hip bone densitometry.R-PJF indicates recurrent proximal junctional failure; BMI, body mass index; ASA, American Society of Anesthesiology; PJF, proximal junctional failure; UIV, uppermost instrumented vertebra; TP, transverse process.
Comparison of Postoperative Radiographic Parameters and Correction Status After the Index Surgery.
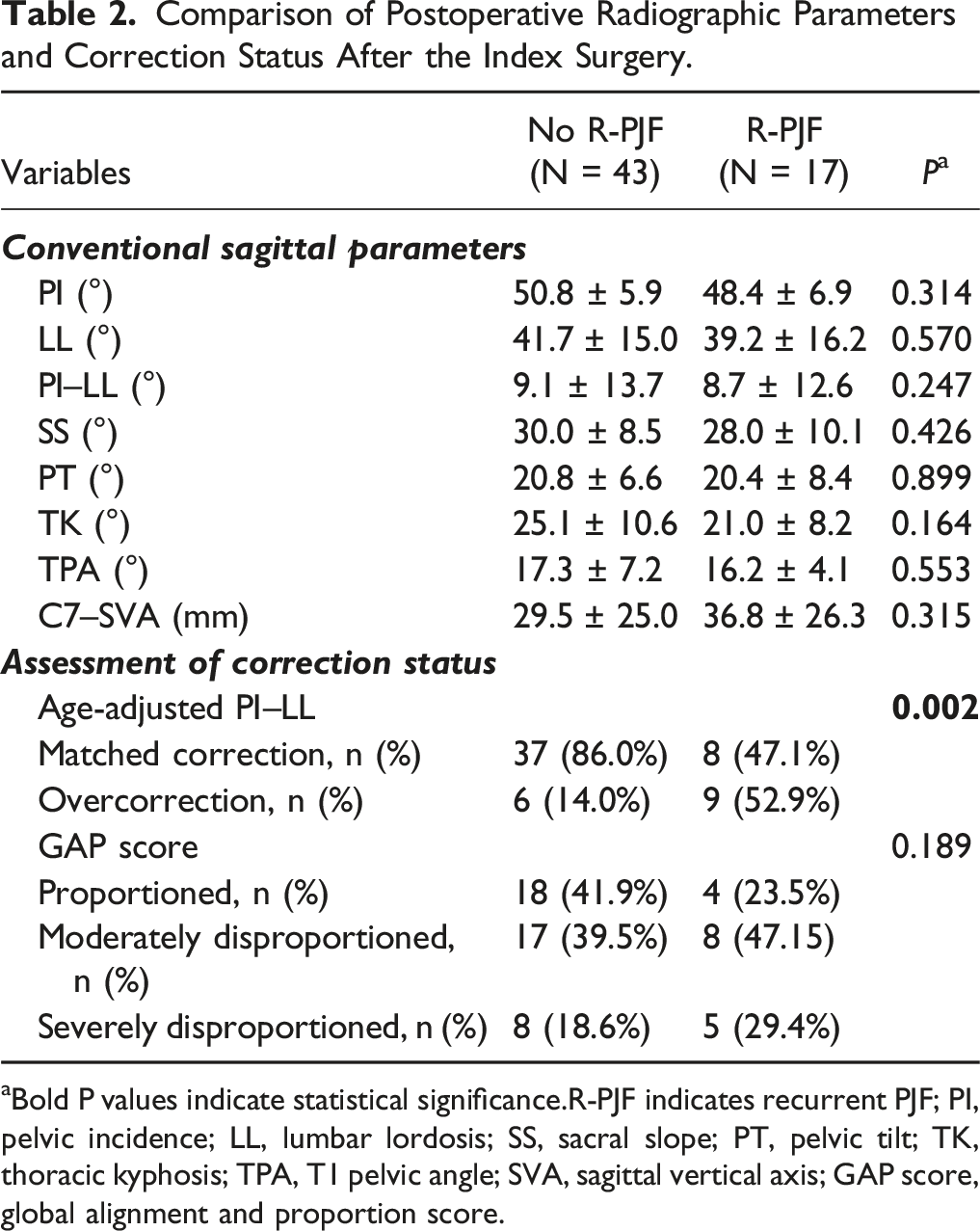
aBold P values indicate statistical significance.R-PJF indicates recurrent PJF; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis; GAP score, global alignment and proportion score.
Comparison of Sagittal Parameters at the Revision Surgery.
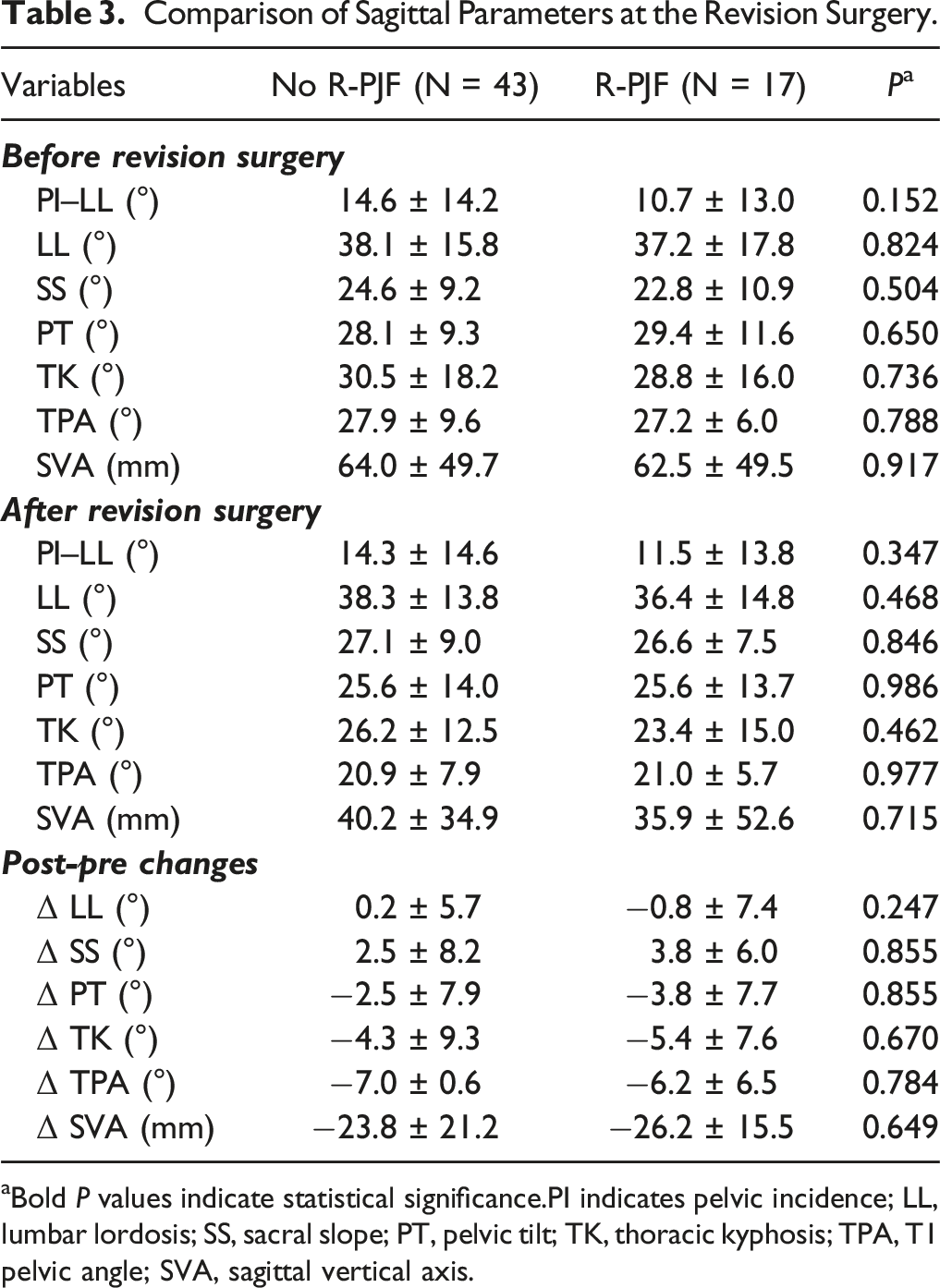
aBold P values indicate statistical significance.PI indicates pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; TPA, T1 pelvic angle; SVA, sagittal vertical axis.
Comparison of Proximal Junctional Kyphosis Severity at the Revision Surgery.
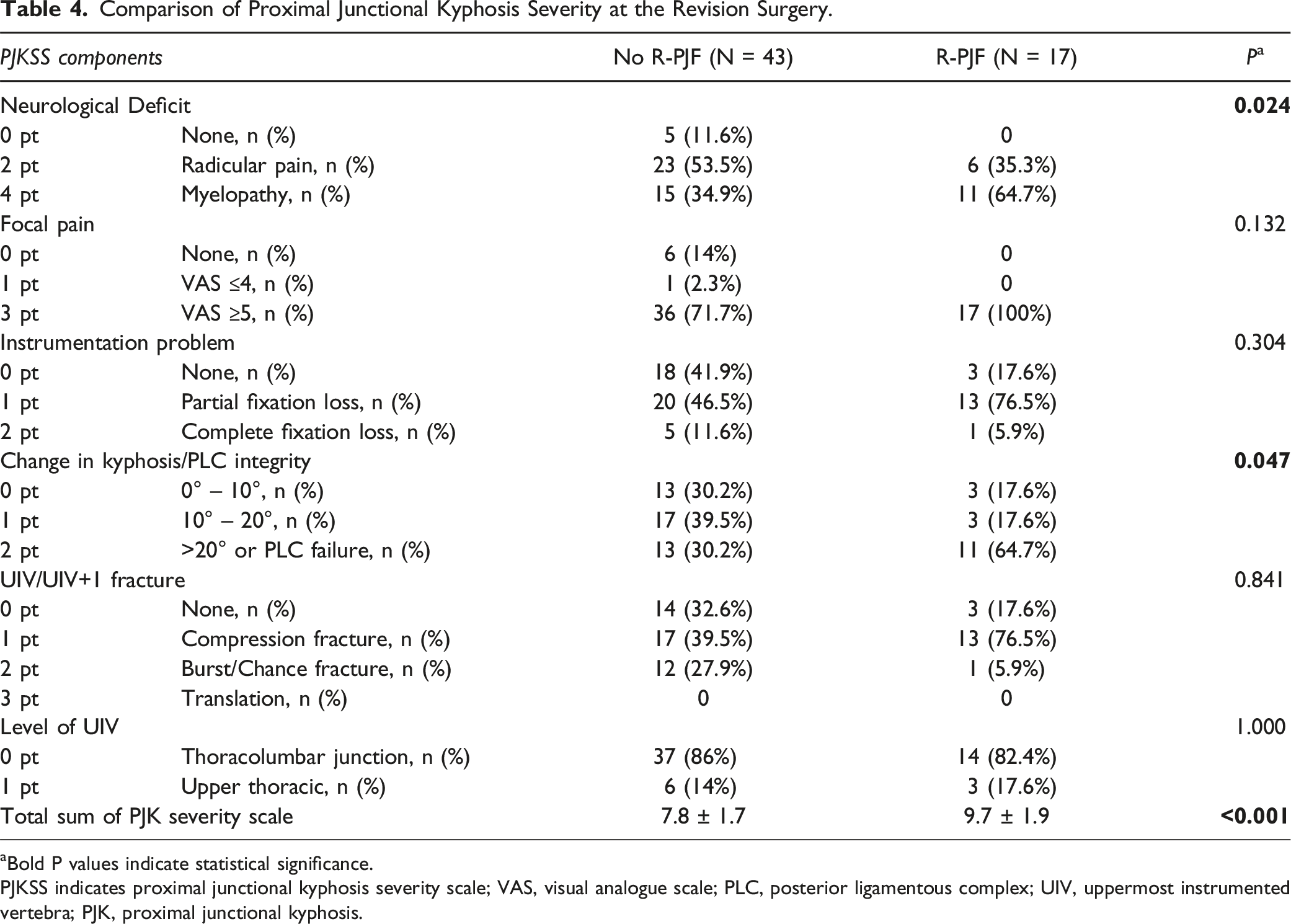
aBold P values indicate statistical significance.
PJKSS indicates proximal junctional kyphosis severity scale; VAS, visual analogue scale; PLC, posterior ligamentous complex; UIV, uppermost instrumented vertebra; PJK, proximal junctional kyphosis.
Multivariate Analysis
Stepwise Multivariate Logistic Analysis of the Risk Factors for R-PJF.

aBold P-values indicate statistical significance.
R-PJF indicates recurrent proximal junctional failure; PI, pelvic incidence; LL, lumbar lordosis; PJKSS, proximal junctional kyphosis severity scale.
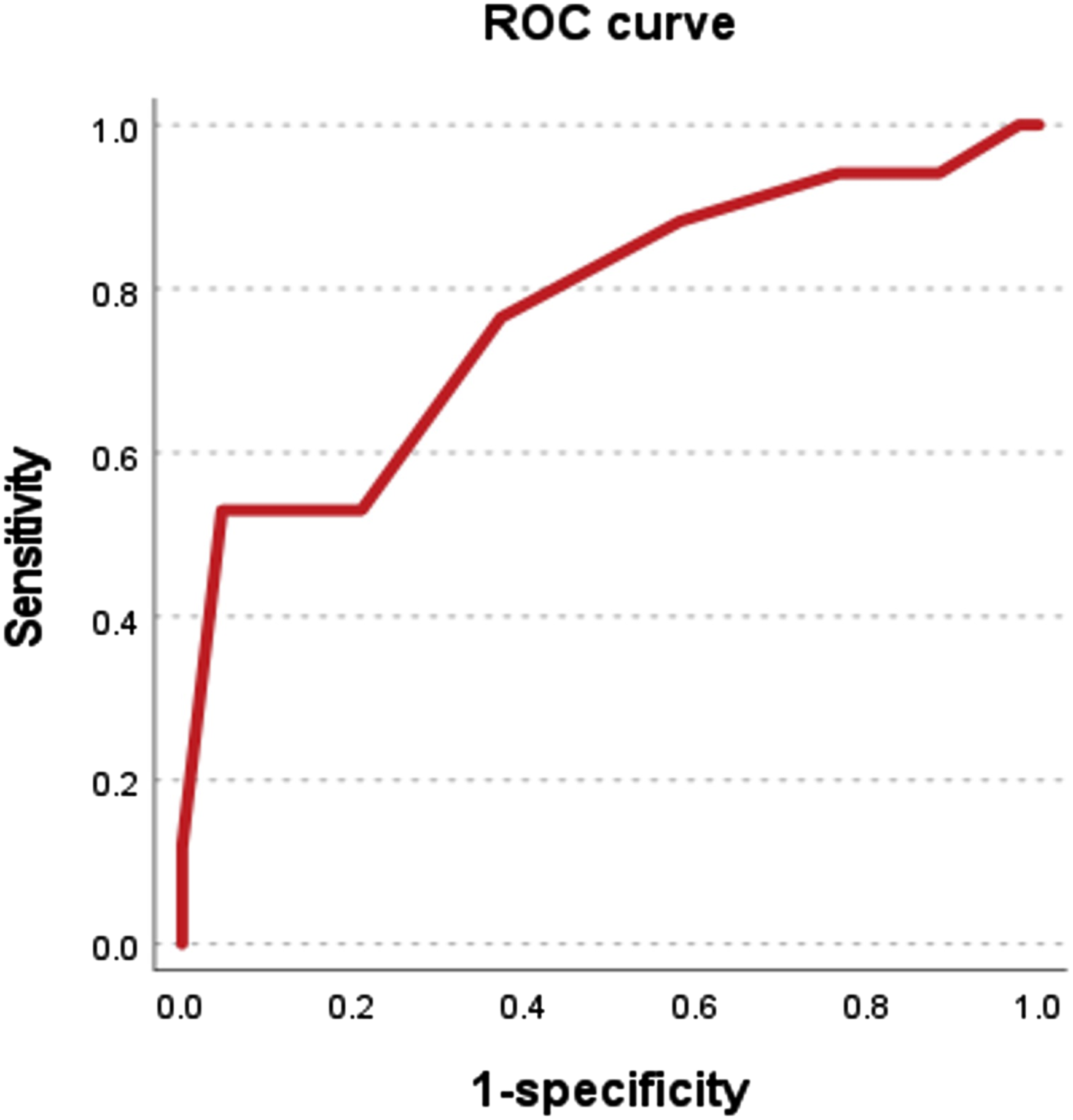
ROC curve for calculating the cutoff value of PJKSS for R-PJF development (AUC = 0.772, 95% CI = 0.630 – 0.914, P < 0.001).
R-PJF Rates according to the Risk Factors
R-PJF Rates According to the Presence of Risk Factors.
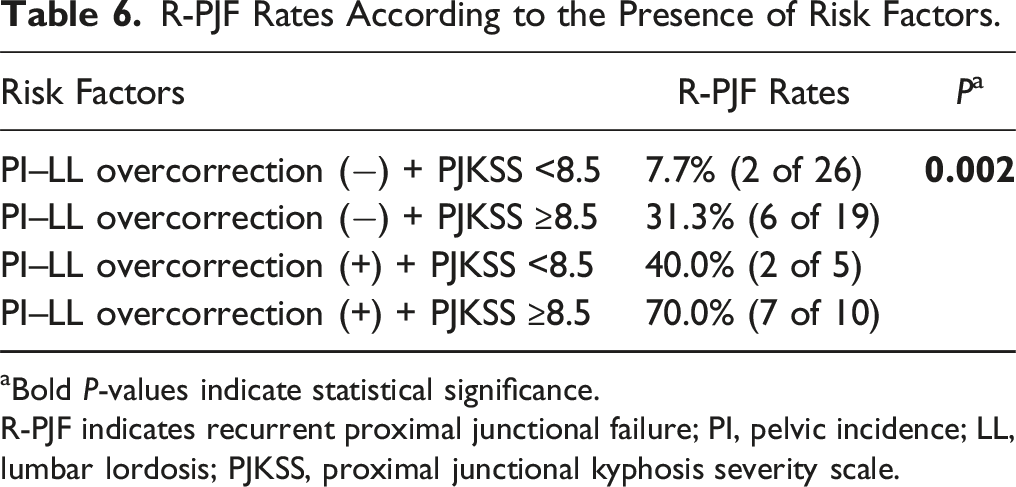
aBold P-values indicate statistical significance.
R-PJF indicates recurrent proximal junctional failure; PI, pelvic incidence; LL, lumbar lordosis; PJKSS, proximal junctional kyphosis severity scale.
Discussions
The exact pathogeneses of PJF and R-PJF are unclear, but the cause is considered to be multifactorial. A complex interplay of biomechanical, surgical, patient-related, and radiographic factors are the likely etiologies. 23 Considering the re-revision surgery (defined as R-PJF in the current study) is definitely more burdensome for both surgeons and patients than the first revision surgery, it is necessary to identify the risk factors for R-PJF and thereby establish proper strategies to avoid R-PJF. The present study revealed that overcorrection relative to the age-adjusted PI–LL at the index procedure, and a high total sum of the PJKSS at the revision surgery were significant risk factors for R-PJF.
We found that overcorrection relative to the age-adjusted PI–LL at the index procedure was the strongest risk factor for R-PJF development (OR = 5.275). The concept of age-adjusted PI–LL target, first introduced by Lafage et al, in 2016, 17 has been well validated in several studies demonstrating that overcorrection relative to the age-adjusted PI–LL is associated with PJF development.5,24,25 In addition to PJF provocation of overcorrection, it is also reported that overcorrection relative to this age-adjusted target is associated with greater severity of PJF. Park et al. found that patients with overcorrection relative to the age-adjusted PI–LL was associated with higher initial proximal junctional angle (PJA) on the identification of PJF, greater PJA progression during follow-up, and subsequently increased risk of revision surgery compared to those with matched correction. 26 In the present study, we found that overcorrection relative to the age-adjusted PI–LL at the index procedure affected the development of R-PJF after revision surgery. That implies that the effect of overcorrection created during the index surgery lasts even after revision surgery for PJF. It can be assumed that the over-corrected portion at the lumbar spine acts as a lever arm to dorsally shift the UIV, thereby re-routing the reciprocal kyphogenic force at the proximal junction. This reciprocal kyphogenic force caused by the overcorrection may be sustained unless the revision surgery includes the entire thoracic spine. 27 Passias et al reported that any residual deformities should be addressed and corrected in planning revision surgery for PJF to prevent recurrent PJF. 28 This suggestion appears to be valid only in cases with initial undercorrection of PI–LL because more lordosis can be surgically achieved using three-column osteotomy or anterior column realignment surgery. However, if a patient was initially over-corrected relative to the age-adjusted PI–LL during the index surgery, converting overcorrection to the matched correction (ie, decreasing lordosis within a fused spine) is surgically impossible. Therefore, avoidance of overcorrection during the index surgery is of utmost importance to mitigate the risk of R-PJF. When performing revision surgery for PJF in patients with PI–LL overcorrection, extending fusion to the upper thoracic spines could be a feasible surgical strategy to avoid R-PJF.
Hart-ISSG developed the PJKSS system that includes 6 categorical characteristics with a total score of 15. 29 The PJKSS represents the severity of PJK and has been well validated in terms of strong correlations with health-related quality of life outcomes and the likelihood of revision surgery for PJF.22,29 In the current study, we found that a higher score of PJKSS was a significant risk factor for R-PJF. It means that the more severe the PJF at the time of revision surgery, the higher the risk of developing R-PJF. This association of PJKSS with R-PJF gives us an insight into the appropriate timing for revision surgery at the first identification of PJF. Among the 6 components of the PJKSS system, the categories of instrumentation problem, UIV/UIV+1 fracture, and level of UIV are unchangeable with time. However, the other categories such as neurologic deficit, focal pain, and kyphosis change can be worsened during the follow-up. If patients have progressive neurologic deficits, urgent revision surgery is required regardless of PJF severity. However, in patients without acute neurologic deficits, revision surgery for PJF is sometimes waived under close supervision. In this case, excessive delay in revision surgery may aggravate the PJF severity increasing the total sum of PJKSS and the risk of R-PJF. Therefore, it is recommended that timely revision surgeries at the first identification of PJF should be performed to prevent the R-PJF following revision surgery. Park et al reported that fracture-type PJF with proximal junctional angle ≥22° increased the likelihood of revision surgery in neurologically intact patients with PJF. 30 Raj et al calculated the threshold of PJKSS to perform revision surgery in patients developing PJF. 22 They suggested that early revision surgery should be considered in patients with PJKSS greater than 4.5 points.
This study has several limitations. First, our results may be underpowered due to the small sample size of the study cohort. However, the patients included in the current study were retrieved after screening a large volume of ASD database (n = 482). In addition, our multivariate analysis revealed only 2 risk factors which are acceptable, given that the number of events (R-PJF) was 17 cases. Second, this study included patients in whom the UIV was predominantly located at the lower thoracic spine, which may limit the generalizability of our findings to those undergoing fusion to the upper thoracic spine. Lastly, although patients in no R-PJF group did not undergo re-revision surgery at least 1 year after PJF development, re-revision surgery might be necessary later during longer follow-up. However, most of the re-revision surgeries (13 / 17 re-revisions, 76.5%) were performed within 1 year after revision surgery.
Conclusions
This study revealed that overcorrection relative to the age-adjusted PI–LL at the index surgery, and high total sum of proximal junctional kyphosis severity scale (PJKSS) at the revision surgery were significant risk factors for R-PJF. Therefore, it is recommended that overcorrection should be avoided during the index surgery. Additionally, considering that the severity of PJF tends to increase over time, timely revision surgery should be considered in patients with symptomatic PJF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.