
Abstract
Study Design
Prospective Cohort Study.
Objective
Untreated pre-surgical depression may prolong post-surgical pain and hinder recovery. However, research on the impact of untreated pre-surgical depression on post-spinal surgery pain is lacking. Therefore, this study aimed to assess pre-surgical depression in patients and analyze its relationship with post-surgical pain and overall post-surgical outcomes.
Methods
We recruited 100 patients scheduled for lumbar spine surgery due to spondylolisthesis, degenerative lumbar disc diseases, and herniated lumbar disc diseases. Psychiatrists evaluated them for the final selection. We assessed the Beck Depression Inventory (BDI), Japanese Orthopaedic Association (JOA), Oswestry Disability Index (ODI), and EuroQoL 5 Dimensions (EQ-5D) scores, numerical back and leg pain scales, and medication dosage data collected before and at 6 weeks, 3 months, and 6 months after surgery.
Results
Ninety-one patients were included in this study; 40 and 51 were allocated to the control and depression groups, respectively. The pre- and post-surgical leg pain, back pain, and functional scores were not different. However, the depression group showed higher ODI and EQ-5D and lower JOA scores than the control group 3 months post-surgery. Partial correlation analysis revealed an inverse correlation between the JOA and BDI scores and a positive correlation between the EQ-5D and BDI scores at 3 months postoperatively.
Conclusion
Untreated depression can prolong postoperative pain and hinder recovery. Detecting and treating depression in patients before spine surgery may improve their overall quality of life and functional recovery.
Introduction
In the Republic of Korea, about 150 000 out of 15 million patients with spinal disease underwent spinal surgery in 2022. Indeed, spine surgery is one of the most frequently performed surgeries, and its number is gradually rising with the aging population. Despite the increasing number of patients seeking spinal surgery, there remains a prevailing sense of uncertainty among these individuals regarding the expected outcomes.1-3 Even in cases with positive, objective assessments after successful surgery of spinal lesions, pain and reduced quality of life persist. This challenge is further compounded by the fact that a substantial portion, ranging from 10%-40%, of post-surgical patients continue to experience pain for a variety of reasons.4-6
A consensus of several studies underscores the complexity of post-surgical pain, acknowledging that it can stem from multiple contributing factors. Pre-surgical considerations can be broadly classified into 2 domains: the psychosocial predisposition to pain and the intrinsic features of the spine that surgeons identify during the evaluation process. Intriguingly, recent research has illuminated a paradigm shift in the understanding of factors that predict surgical outcomes. Contrary to earlier assumptions, structural abnormalities detected via pre-operative magnetic resonance imaging (MRI), while undoubtedly significant, are no longer the sole indicators of positive surgical outcomes. Psychosocial factors emerge as potent determinants, exerting a more profound influence on the surgical trajectory. Conditions such as depression, hypochondria, anxiety, and somatization disorders are gaining increasing recognition for their substantial impact on the prognosis of spinal surgery.7-9
In particular, depression is known to be more related to pain than other psychological factors. Increased depression has been reported to result in the aggravation and extension of pain.10,11 In addition, excessive depression impedes the treatment process after surgery and impairs patient remission, which results in severe and prolonged pain. Previous studies have focused on depression after spinal surgery and on psychological changes in patients with pre-existing psychiatric diseases after surgery. 12 However, research on untreated pre-surgical depression and its impact on pain after spinal surgery is lacking, and the associations between untreated pre-surgical depression and post-spinal surgical pain and outcomes remain unclear. Thus, this study aimed to quantify pre-surgical depression in patients and analyze its correlation with post-surgical pain and overall outcomes after spinal surgeries.
Methods
Study Population and Data Analysis
This single-center prospective study was conducted at the secondary general hospital from September 2021 to August 2022. A total of 100 patients with spondylolisthesis and degenerative lumbar and herniated lumbar disc diseases who underwent scheduled lumbar spine surgery were recruited. Patients who underwent spinal surgery for fractures, infections, or tumors were excluded. Patients who had a history of psychiatric treatment were also excluded. We included surgeries performed by 3 spine surgeons at a single hospital, and all types of lumbar spinal surgeries, including spinal fusion, laminectomy only, and discectomy only, were included in the study.
Data were collected before surgery for all participants, including age, sex, psychiatric history, numerical back and leg pain scale, Japanese Orthopaedic Association (JOA) score, 13 Oswestry Disability Index (ODI), 14 EuroQoL 5 dimensions (EQ-5D) 15 survey, and Beck Depression Inventory (BDI).16,17 The pre-operative and postoperative assessment encompassed several scales: the JOA scale, used to evaluate neurological status and self-assessed low back pain on a scale of 0 to 17; the ODI scale, which gauged functional recovery and the subjective percentage of disability in daily activities on a scale from 0 to 50; the EQ-5D scale, offering a standardized self-assessment of health-related quality of life on a scale from 0 to 15; and the BDI scale, a widely-recognized tool for measuring the severity of depression symptoms, known for its high reliability with a Cronbach’s alpha value of .85 in Koreans, and chosen for its practicality in large patient population studies, all with the aim of categorizing depression severity before and after discharge.
After surgery, the study recorded the total amount of pain medication administered during hospitalization (including tramadol, pethidine, non-steroidal anti-inflammatory drugs [NSAIDs], pregabalin, limaprost, and duloxetine), the level of spine surgery, and the actual operation type (fusion, laminectomy, discectomy). Follow-up assessments were conducted at 6 weeks and 3 and 6 months after surgery at the outpatient clinic, including measurements and recordings of the numerical back and leg pain scale, JOA, ODI, EQ-5D scores, and pain medication dosage (NSAIDS, gabapentinoid, and limaprost).
Categorization
During the study period, 100 research-enrolled patients who underwent lumbar spine surgery were screened by psychiatrists using the BDI scale. Based on the results, the patients were categorized into a control group and a depression group. BDI value of 10-18 was considered mild depression, 19-29 moderate depression, and 30-63 severe depression (Figure 1).16,17 Patient categorization.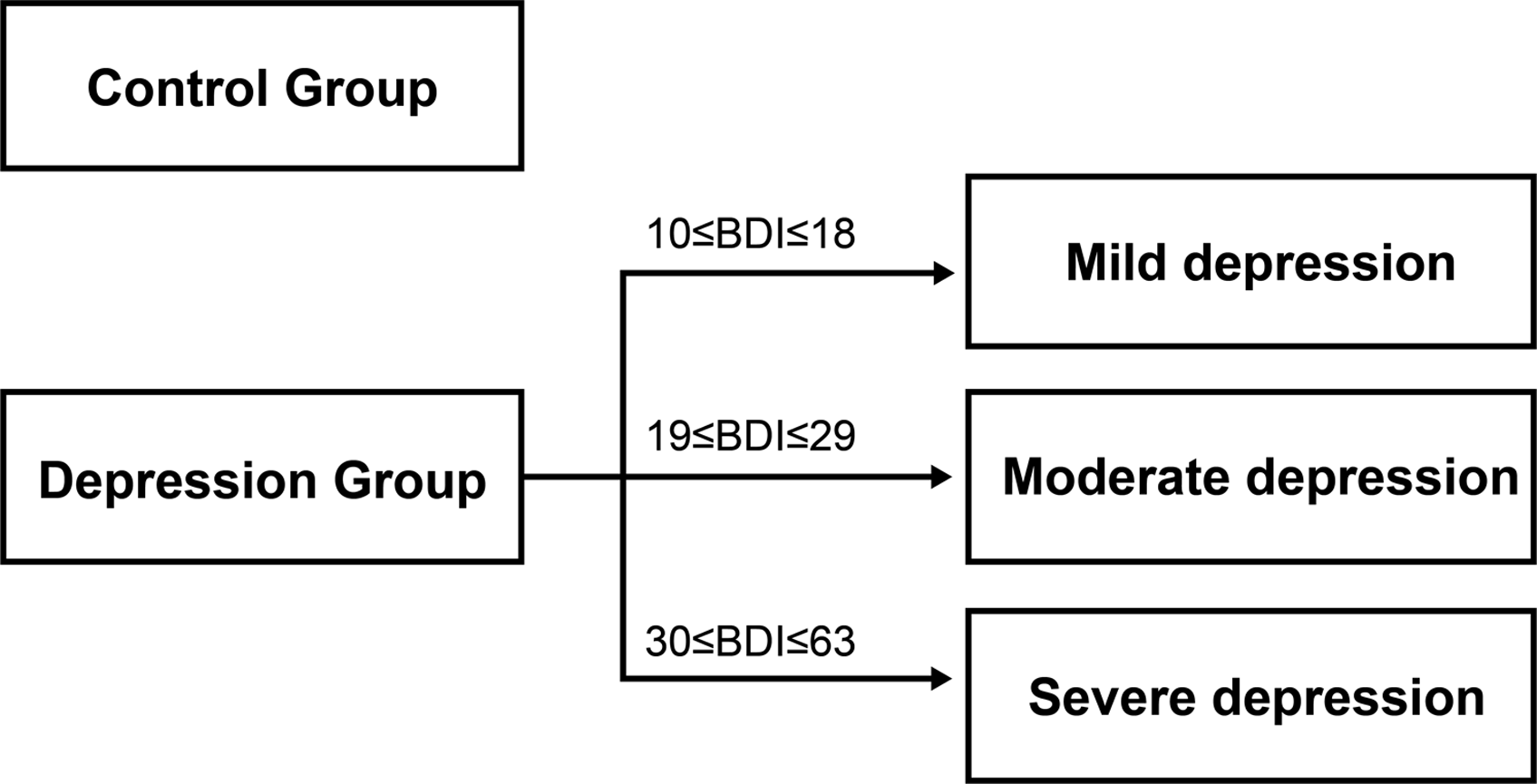
Statistical Analysis
Pre- and post-surgical (6 weeks and 3 and 6 months) JOA, ODI, EQ-5D scores, numerical back and leg pain scales, and usage of each pain medication were compared between the depression and control groups using a paired t-test. Partial correlation analysis was performed between the BDI and functional scores (JOA, ODI, EQ-5D) at each follow-up, with sex, age, operation type, and surgeon as covariates. A P value of <.05 was considered statistically significant.
Ethics Declaration
This study was approved by the Institutional Review Board of the XXX Hospital, and written informed consent was obtained from all subjects before each procedure.
Results
Demographic and Clinical Characteristics of Participants.
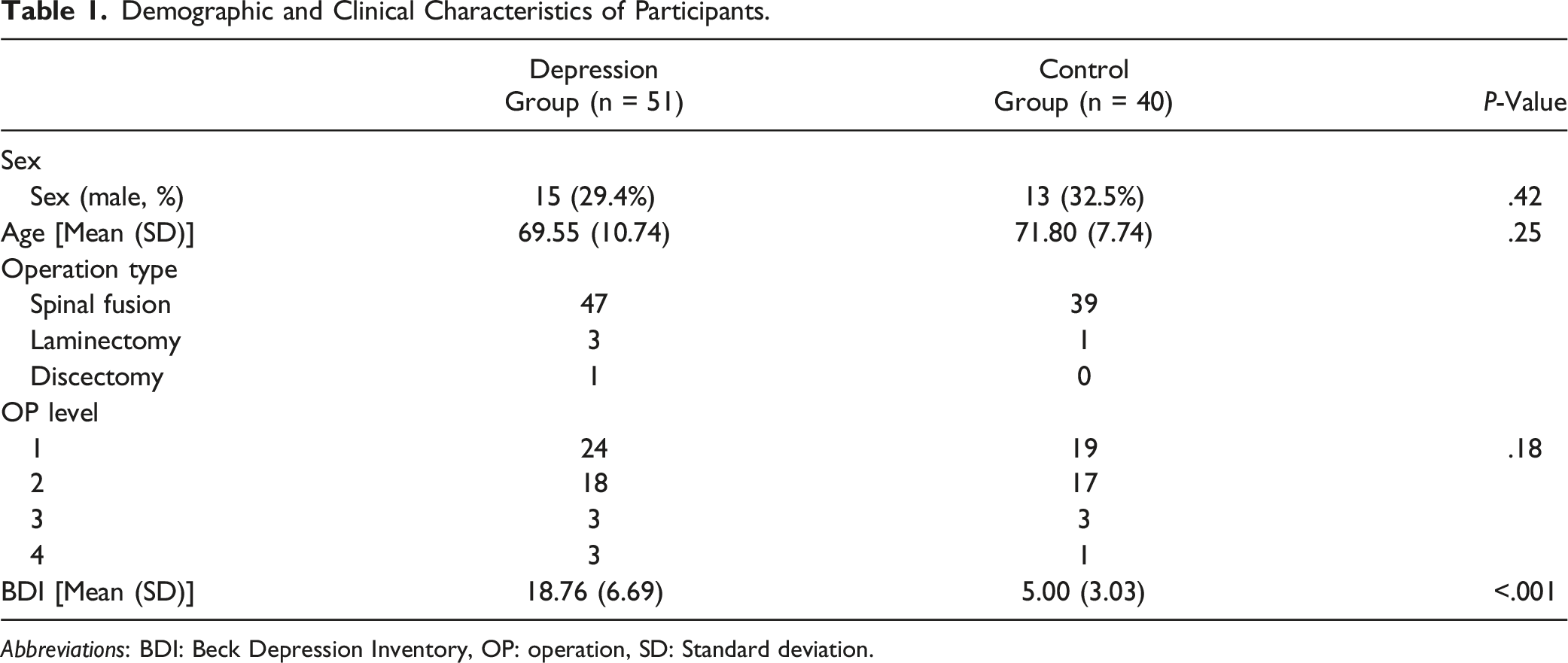
Abbreviations: BDI: Beck Depression Inventory, OP: operation, SD: Standard deviation.
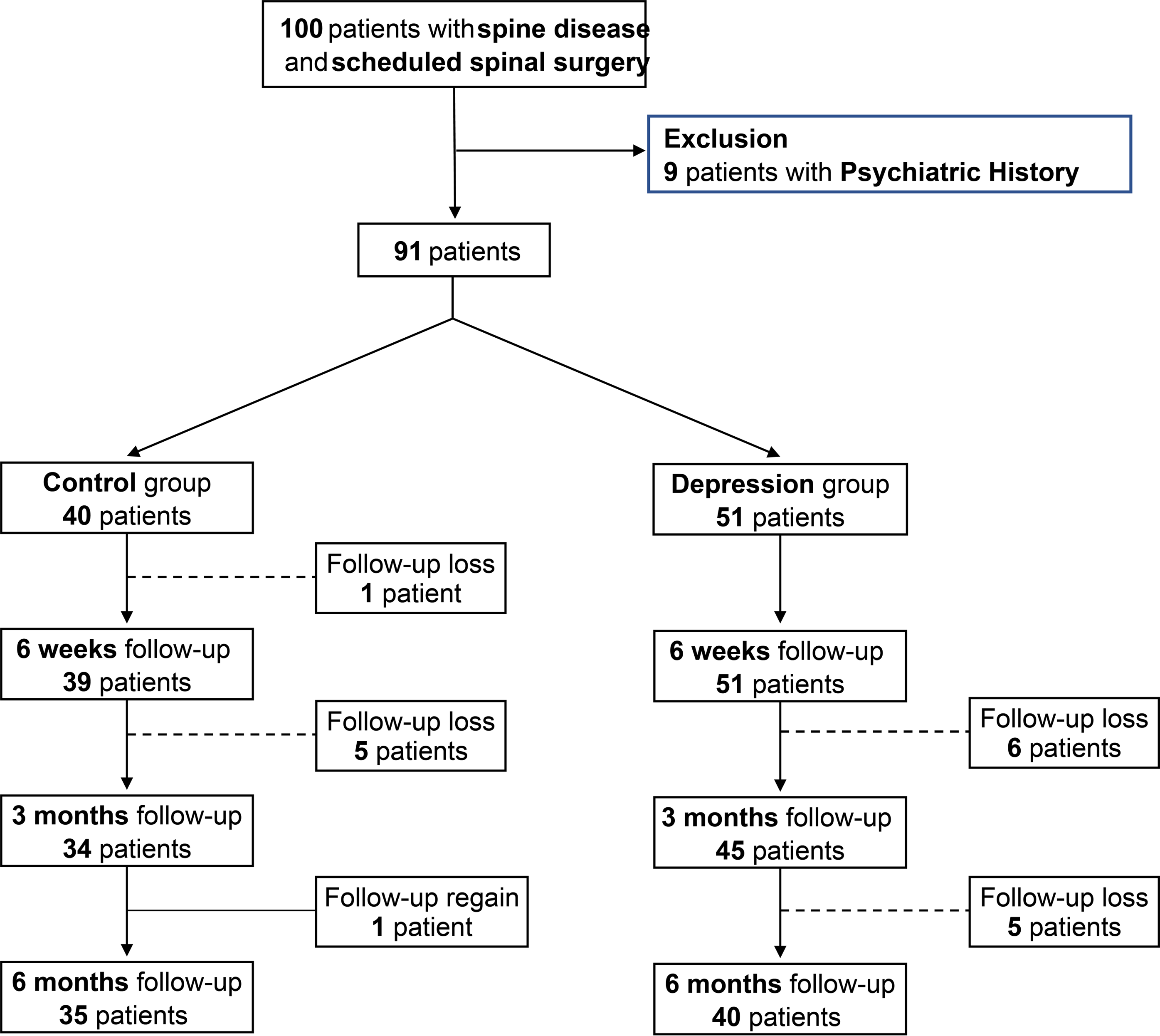
Overall flow chart of this study.
The Pain Scale and Functional Scores Before and 6 Weeks, 3 Months, and 6 Months After Surgery.
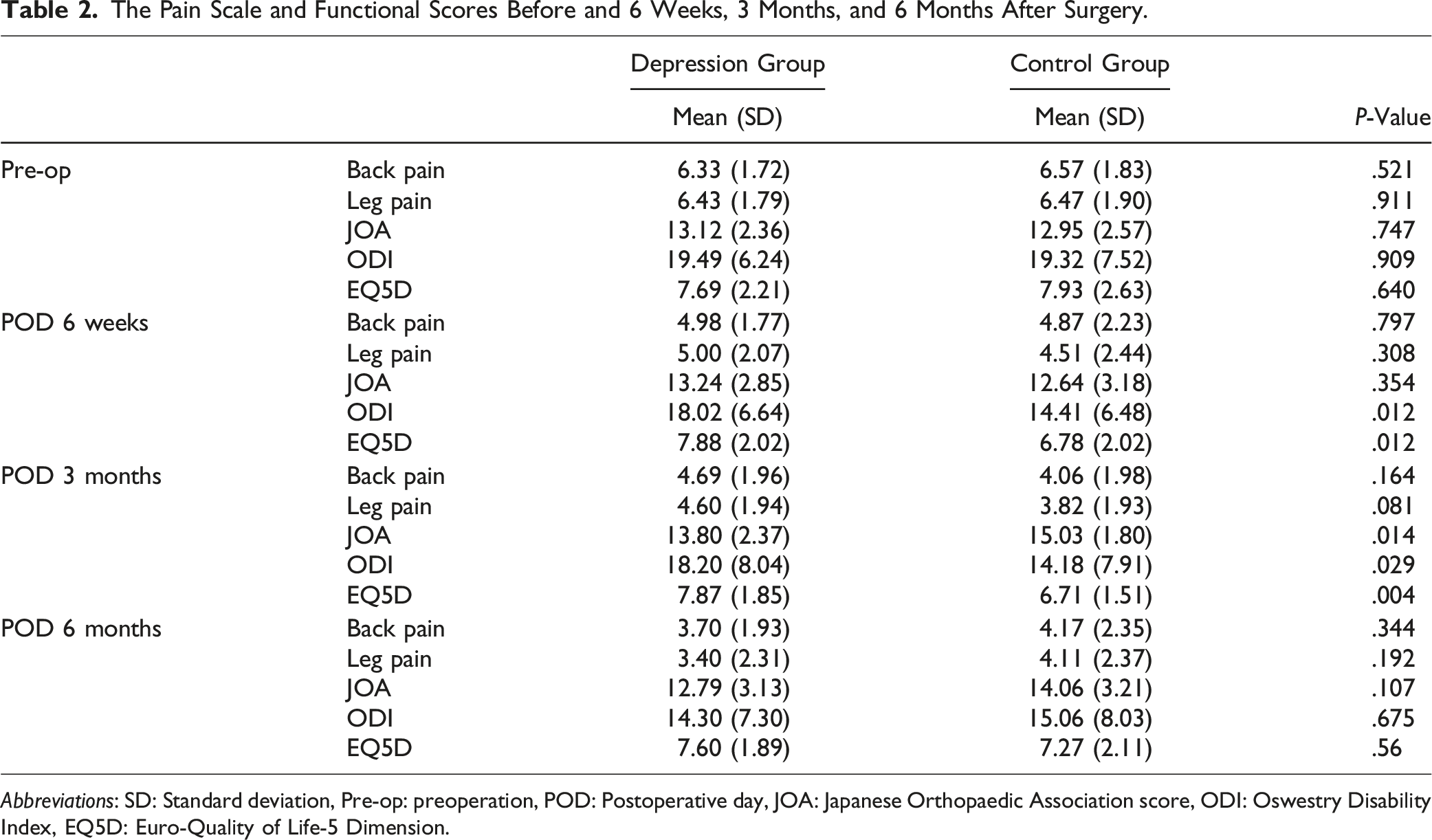
Abbreviations: SD: Standard deviation, Pre-op: preoperation, POD: Postoperative day, JOA: Japanese Orthopaedic Association score, ODI: Oswestry Disability Index, EQ5D: Euro-Quality of Life-5 Dimension.
Medication Dosage Data Collected Consecutively Before and 6 Weeks, 3 Months, and 6 Months After Surgery.
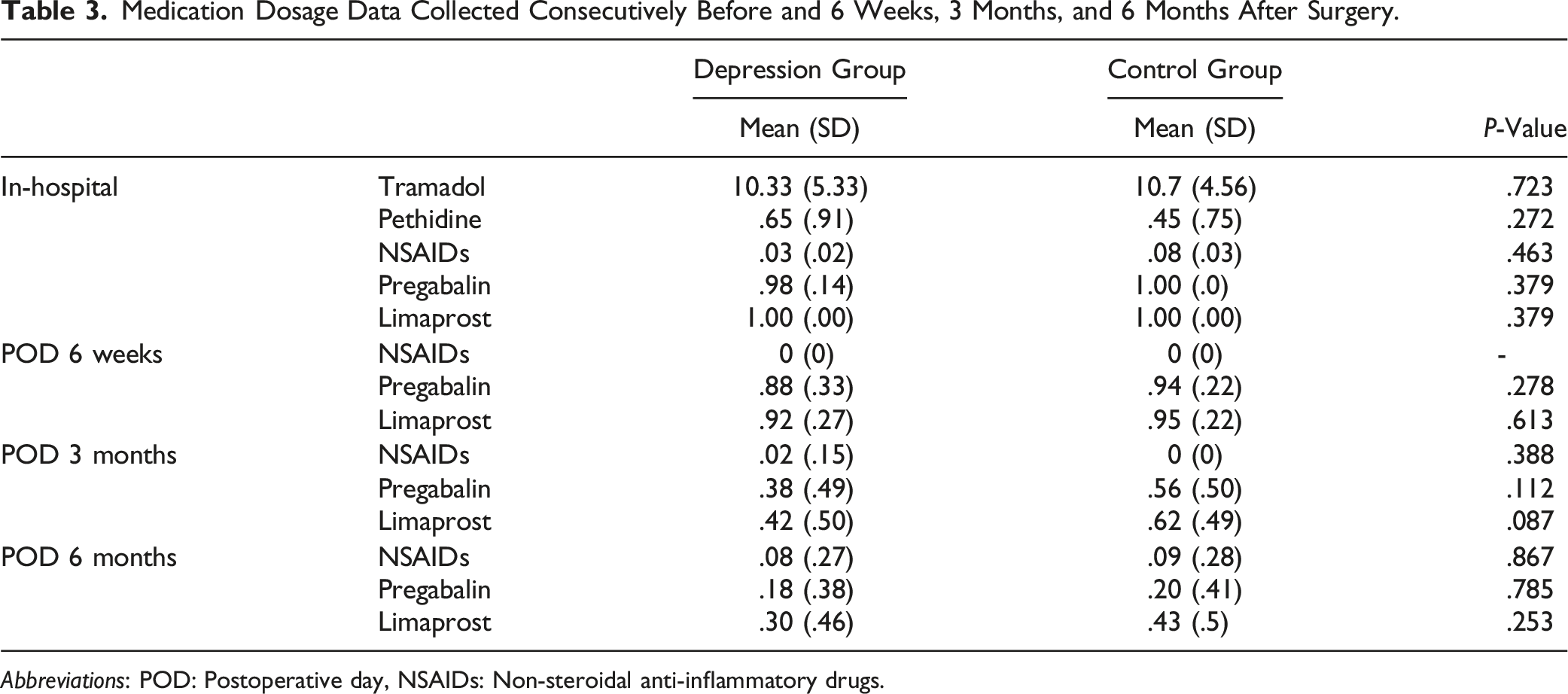
Abbreviations: POD: Postoperative day, NSAIDs: Non-steroidal anti-inflammatory drugs.
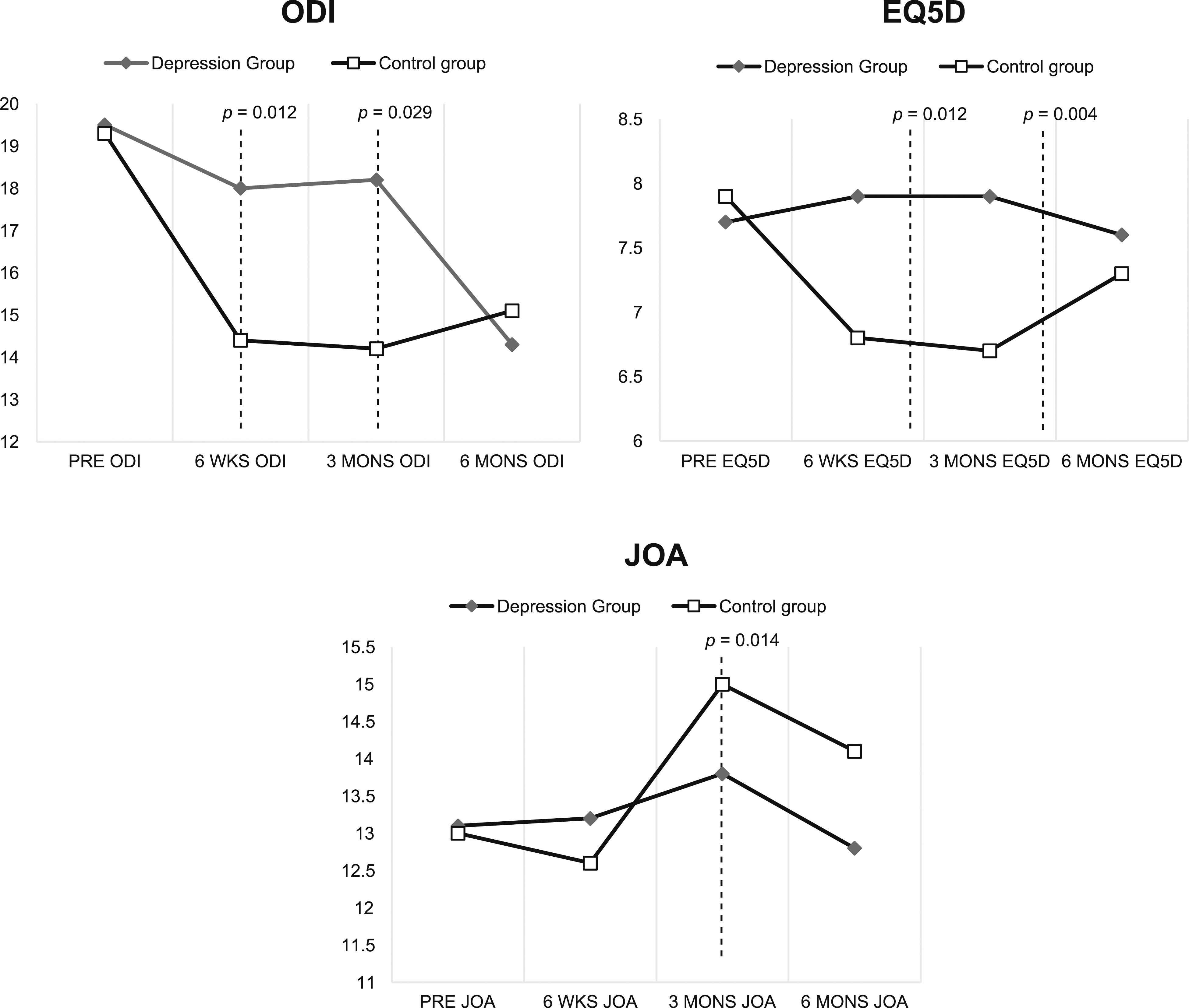
Patients’ functional score pre-operatively at 6 weeks and 3 and 6 months after surgery.
Partial correlation analysis revealed that the 3-month JOA score was inversely proportional to the BDI, and the 3-month EQ-5D score was directly proportional to the BDI. The respective R values were −.312 and .356, and the corresponding P values were .007 and .002. Sex, age, type of operation, and surgeon were set as covariates (Figure 4). Partial correlation analysis revealed that the 3-month JOA score is inversely proportional to the BDI, and the 3-month EQ-5D score is directly proportional to the BDI. Abbreviations: BDI, Beck Depression Inventory; EQ-5D, EuroQoL 5 Dimensions; JOA, Japanese Orthopaedic Association.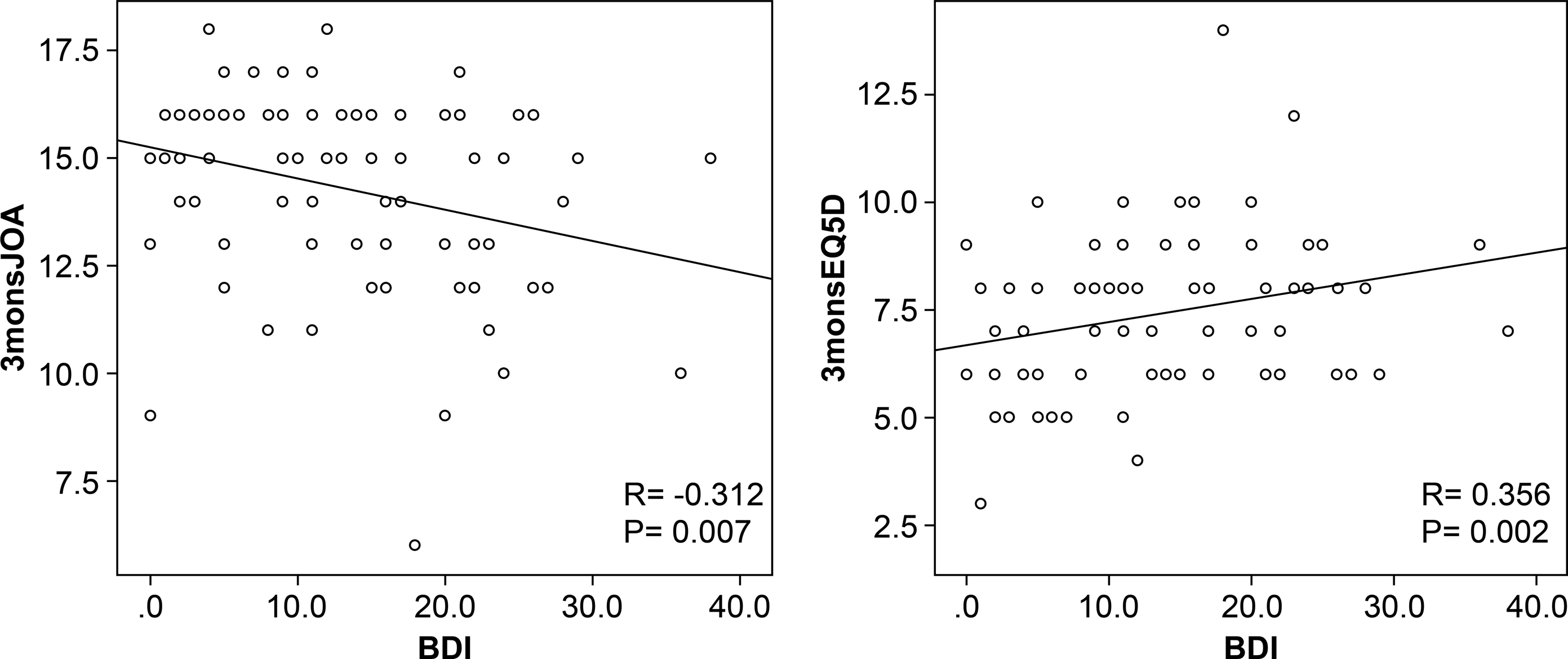
In both groups, there were no intraoperative complications. However, postoperative complications included early screw loosening in one patient each from the depression and control groups who underwent spine fusion. No other major postoperative complications occurred. Objective measurements of neurologic function were conducted before and after the surgery for both cohorts. No major neurologic problems were observed after surgical treatment.
Discussion
Patients who often undergo spinal surgery hold high expectations for postoperative pain relief. However, it is not uncommon for patients to experience persistent pain and reduced function even after a technically successful surgery. 18 A substantial body of research has indicated that psychological factors may underlie this phenomenon, with pre-operative psychological factors emerging as significant contributors to postoperative pain and overall outcomes.19-23
Numerous studies have explored the relationship between post-surgical depression and its impact on pain and functional recovery. Post-surgical depression has been reported to occur at different frequencies, according to various studies. In one study, approximately 10% of patients who underwent knee osteoarthritis surgery reported a depression phenotype following surgery. In contrast, a different study reported higher rates of post-surgical depression after hip and knee arthroplasty surgery.24,25 In addition, a review of the prevalence of depression in the intensive care unit found the rate of depression among patients who underwent surgery to be 28%. This post-surgery depression was associated with severe pain and reduced physical activity, further intensifying the depression phenotype.26-28 Furthermore, patients with untreated pre-surgical depression could experience a more severe form of depression after surgery. 21 Therefore, pre-surgery depression is a relevant aspect that needs to be assessed. This study evaluated the variation in the patterns of postoperative pain and functional outcomes depending on the severity of depression.
The study’s findings indicate that untreated pre-surgical depression has a definite impact on post-spine surgery quality of life. This impact is noteworthy, as it persists despite the absence of statistically significant differences in prescribed pain medication and post-surgery back and leg pain levels between the depression and control groups. However, a differentiation in functional outcomes is observed. Three aspects of functional outcomes were evaluated: neurological status (measured by the JOA score), disability level (measured by the ODI score), and health-related quality of life (measured by EQ-5D). The depression group exhibited worse neurological status at 3 months after surgery, exhibited higher disability levels at 3 weeks and 3 months post-surgery, and reported better quality of life at 6 weeks and 3 months after surgery when compared to the control group. These functional outcome disparities were significant at 6 weeks and 3 months but not at 6 months after surgery. In summary, pre-surgical depression significantly influences short-term functional outcomes following surgery, while long-term functional outcomes remain largely unaffected. One noteworthy point is that when a subgroup analysis was conducted within the depression group, comparing the mild depression group to the moderate and severe depression group, there were no differences in pain, functional outcomes, or medication dosage between the 2 groups. This suggests that the presence of depression, rather than its severity before surgery, may have a greater impact on functional outcomes. However, due to the small number of patients, further research is needed.
There can be prolonged immobilization and uncontrolled postoperative pain after the surgery because of the nature of spine surgery, it can lead to emotional fluctuations such as depression and negatively impact postoperative pain and various functions. However, as time passes, beyond 6 months post-surgery, mobilization becomes smoother, and function gradually improves and stabilizes. Consequently, the influence of emotional fluctuations is expected to diminish. This phenomenon is observed in other surgeries with long periods of immobilization and extended postoperative pain, which also shows reduced immediate outcomes. 29
In previous studies, the BDI or Hamilton Depression Scale was also reported to be a negative predictor of post-surgical outcomes after spinal fusion surgery. Considering the fact that pre-surgical psychological factors affect postoperative outcomes, the importance of psychological screening is emphasized, and interventions before surgery were shown to be necessary to improve post-surgical outcomes.12,30,31 In this study, only patients with untreated pre-surgical depression were included. Through partial correlation analysis, we revealed that the 3-month JOA score was inversely proportional to the BDI, and the 3-month EQ-5D score was directly proportional to the BDI.
Considering these results, patients with pre-surgical depression have worse quality of life and more serious functional deficits than psychologically stable patients, even though there was no difference in pain perception. While this study showed an association between pre-surgical depression and post-surgical outcomes, it is important to note that these findings do not allow us to conclude the effectiveness of pre-surgical psychiatric intervention in improving the psychological status, functional recovery, and quality of life after spinal surgery.32,33 Further research is needed to explore the potential benefits of pre-surgical psychiatric intervention in this context.
There is substantial evidence supporting the benefits of pre-operative psychological interventions on surgical outcomes, including those related to spine surgery. These interventions, such as cognitive-behavioral therapy and relaxation techniques, can significantly improve perioperative outcomes by reducing anxiety and pain, which in turn may positively impact the overall recovery and short and mid-term outcomes for patients. Given these benefits, spine surgeons should consider integrating pre-operative psychological assessments and interventions into their practice. This approach can enhance the recovery after surgery and improve patients’ quality of life by addressing both the psychological and physiological aspects of surgical care. 34
The limitations of this study are as follows: the sample size was small, although the data are statistically significant. As the follow-up period was rather short (6 months), no long-term clinical outcomes could be observed. The surgical results were not reflected in the clinical outcomes. In the future, we plan to analyze the effects of other pre-surgical psychosocial factors other than depression on post-surgical outcomes.
In summary, although there was no difference in leg and back pain in addition to the prescribed pain medication dosage after spine surgery, it was found that the early functional outcome of the patients differed according to the degree of pre-surgical depression.
Conclusion
Undiagnosed and untreated depression can extend the duration of postoperative pain and impede recovery. Identifying and addressing depression in patients before spine surgery can enhance their quality of life and functional rehabilitation.
Supplemental Material
Supplemental Material - Association of Untreated Pre-surgical Depression With Pain and Outcomes After Spinal Surgery
Supplemental Material for Association of Untreated Pre-surgical Depression With Pain and Outcomes After Spinal Surgery by Jae-Won Shin, Yung Park, Sung-Hoon Park, Joong Won Ha, Woo-Seok Jung, Hak-Sun Kim, Kyung-Soo Suk, Si-Young Park, Seong-Hwan Moon, Byung Ho Lee, Ji-Won Kwon, and Jaeun Ahn in Global Spine Journal
Footnotes
Acknowledgments
Author Contributions
Conceptualization: JWS, JA, YP. Data curation: JWS, SHP. Formal analysis: JWS, JA. Funding acquisition: JWS. Investigation: JWS, WSJ. Methodology: JWS, JA. Resources: JWS. Software: JWS. Supervision: JWS, YP, JWH, HSK, KSS, JWK, SHM, SYP, BHL, JA. Validation: JWS, JA. Visualization: JWS. Writing-original draft: JWS. Writing-review & editing: JWS, JA, YP. Approval of final manuscript: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Institutional Review Board of the National Health Insurance Service Ilsan Hospital (IRB No. 2021-03-051-003) and written informed consent was obtained from all subjects before each procedure.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.