
Abstract
Study Design
Systematic Review.
Objectives
To describe existing craniocervical junction and upper cervical spine classification systems and their integration into a unified rational hierarchical system of the AO Spine Upper Cervical Injury Classification System (UCIC).
Methods
A systematic review of MEDLINE, EMBASE and Cochrane Databases was performed in keeping with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
Results
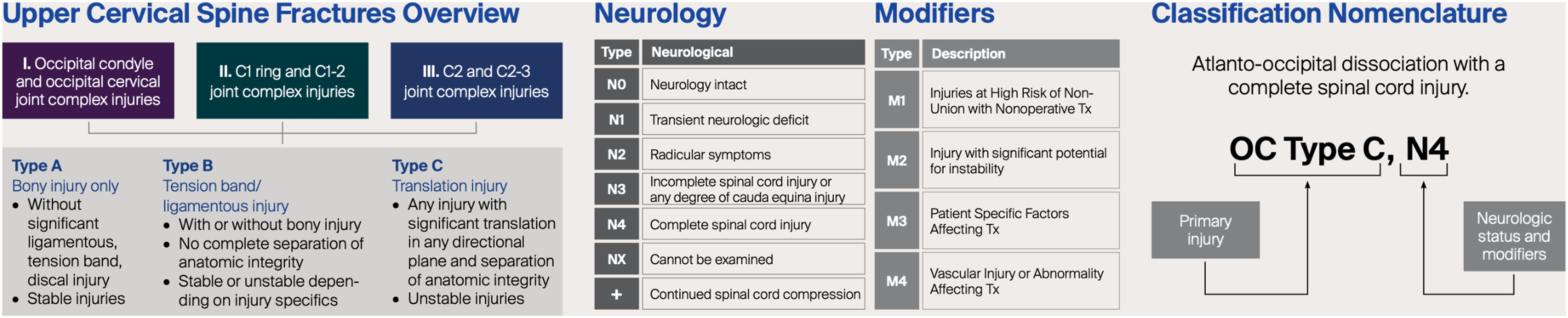
859 articles were identified which yielded 10 established classification systems for injuries of the occipital condyles, craniocervical junction as well as atlas and axis. All systems were either non-hierarchical, conferred minimal clinical significance or failed to consider neurological status of patients. For example, the Traynelis classification simply relies upon describing the direction of displacement which has dubious clinical significance. Similarly, the Jefferson description of atlas fractures simply grades injuries by fracture line pattern. The AO Spine UCIC system synthesizes each published historical scheme into a rational graded method by which clinicians can assess the severity of injuries to this region. The three grades of injury range from type A being generally stable bony injuries, type B constituting potentially unstable (osseoligamentous) injuries and type C representing grossly unstable translational injuries.
Conclusion
The AO Spine UCIC System is a validated methodology of integrating historical landmark grading systems and evolving this into a structured means of grading severity of injuries to guide timely clinical management. The implementation of this universal system will enable clinicians to consistently assess craniocervical junction injuries and implement appropriate management strategies. Future studies will examine outcomes after operative or non-operative management with progression to a standardized quantified algorithm.
Introduction
The cervical spine is traditionally biomechanically divided by White et al into the upper cervical spine consisting of the occipital-atlanto-axial complex bound together by ligamentous structures, the middle cervical spine (C2-C5) and lower cervical spine including the cervico-thoracic junction (C5-T1). 1 These functional units of the cervical spine were chosen because the kinematics and kinetics of the upper cervical spine are unique, and contrast greatly to the lower subaxial cervical spine which behaves more similarly to the upper thoracic spine. 2 The flexibility afforded to the cervical spine is an advantage but also increases its susceptibility to traumatic injury.3–6 Indeed, cervical spine injuries have an incidence estimated to be between 11.8 and 15.0 in 100 000 and are associated with potentially devastating neurological outcomes with a mortality of 5.9% in the general population and 14% in elderly patents 65 years and older.7–12
Timely surgical intervention improves neurological and functional outcomes, but recent studies in global variations in the treatment of subaxial cervical spine fractures have shown there still exists a high degree of controversy and discrepancy in management. 13 Investigation into the global variations in the treatment of subaxial cervical spine fractures demonstrates there are still some areas of classification and management, especially regarding between different burst fracture morphology subtypes, which require further investigation.14–16 Reassuringly, contemporary biomechanical understanding has evolved from White and Panjabi’s 1978 concept of the ‘major injuring vector’ to now a more sophisticated understanding of the spine’s response under varying loads and deformation with the aid of fresh cadaveric, animal and finite element models.17–20 Despite this, a multitude of historical classification systems exist. For example, in the assessment of occipital condyle fractures currently it is necessary for clinicians to combine the bony pattern of injury as stratified by Anderson and Montesano and the grading system for transverse ligament injury by Dickman et al in order to infer stability.21,22
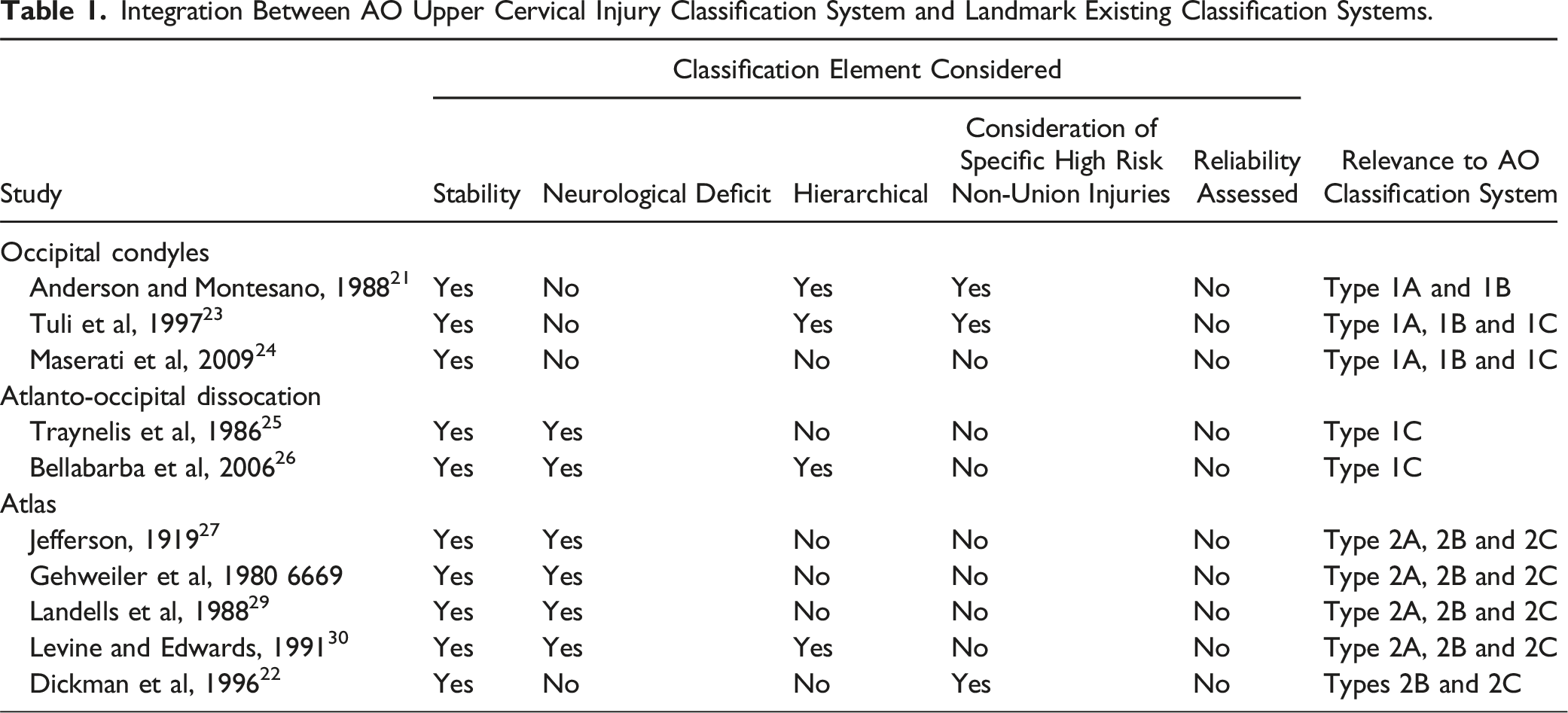
Integration Between AO Upper Cervical Injury Classification System and Landmark Existing Classification Systems.
Methods
Search and Eligibility Criteria
The authors conducted a systematic electronic search of the Medline, EMBASE and Cochrane Database of Systematic Reviews from their date of inception to August 2024 in keeping with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases were queried with the proceeding terms combined with various Boolean operators: ‘craniocervical junction’, ‘atlanto-occipital joint’, ‘atlas’, ‘C1’, ‘grad*’, ‘classification’, ‘system’ and ‘fracture’. Only studies examining human subjects in the language English or with available English translations were included. No registered review protocol exists for this study.
Inclusion and Exclusion Criteria
Two authors (B.T.S.K and J.W.T) screened articles for those appropriate to undergo full-text examination. Bibliographies of included studies were also scrutinized for further eligible articles. Discrepancies were discussed until consensus attained. Inclusion criteria were defined as: 1. Any form of article, whether randomised or non-randomised controlled trials, cohort study, case series, case report or review article which proposed a new classification system defined as a method of grading fractures upon a rational basis with two or more categories 2. Any article which added a new category to an established classification system 3. Human Subjects.
Study Selection and Data Extraction
Extraction of data into a preformatted spreadsheet was performed independently by one author (B.T.S.K) and cross-checked by another (J.W.T) in accordance with the Cochrane Handbook for Systematic Reviews. 32 No authors were contacted for further unpublished data.
Appraisal and Synthesis of Results
The Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool and Murad et al instrument was applied for included non-randomized studies and case studies or case reports respectively.33,34 Study quality was independently assessed by two authors (B.T.S.K and J.W.T) with consensus attained following discussion. The ‘Robvis’ tool was utilised to generate the traffic light plot in accordance with Cochrane recommendation. 35
Results
Study Selection
The primary search retrieved 869 articles which was filtered to 751 after duplicates were removed (Figure 1). 58 studies demanded full-text assessment for eligibility after screening was concluded. Ultimately, 10 studies were included in the systematic review with the majority of screened articles being excluded either for failing to propose a new classification system or simply being a review article. PRISMA flowchart demonstrated the funnel of search timepoints from identification, to screening, eligibility and finally included studies.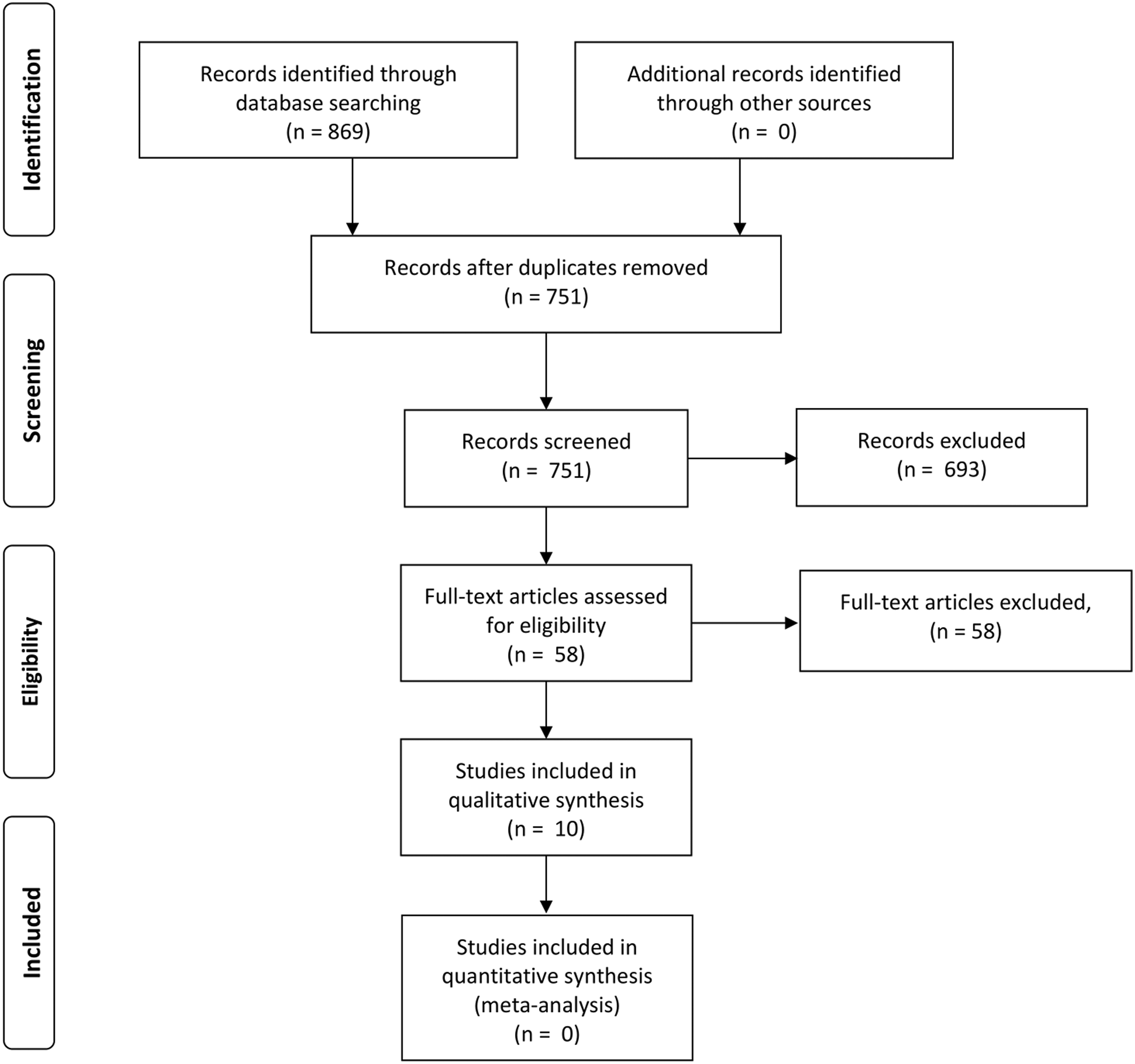
Study Quality
Risk of Bias Assessment of Included Case Series and Case Report Studies Assessed by the Tool Developed by Murad et al 1 .
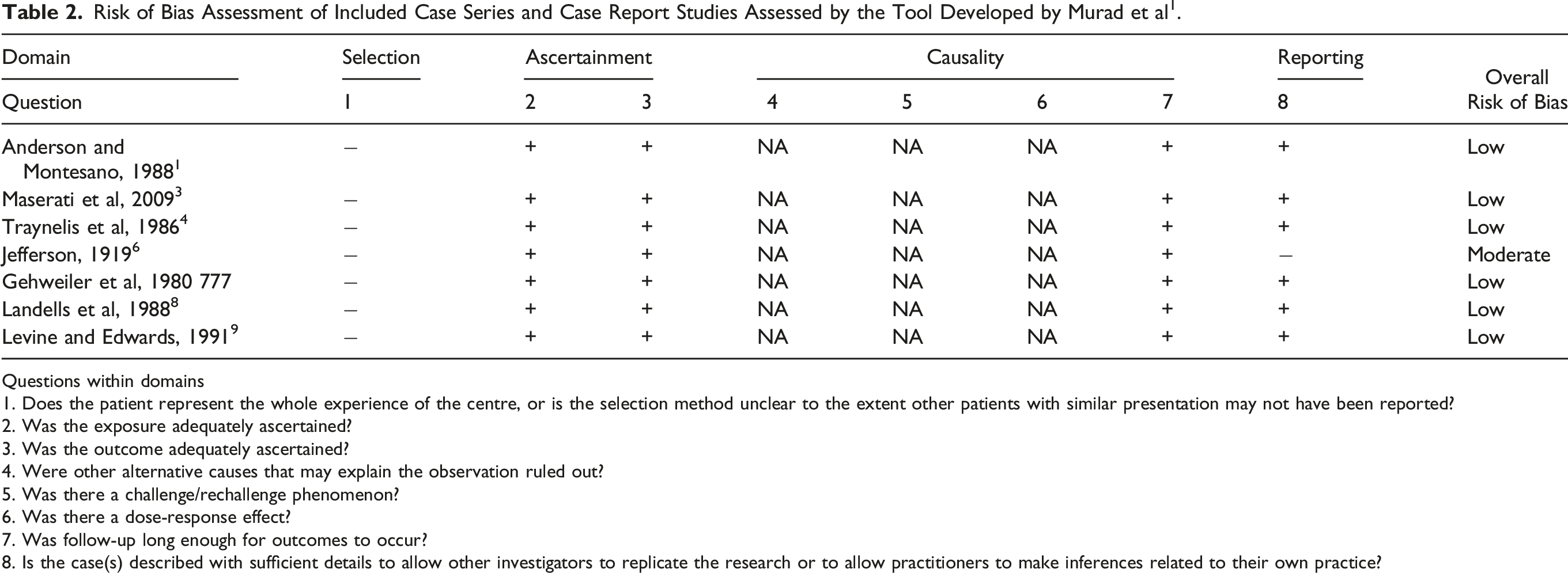
Questions within domains
1. Does the patient represent the whole experience of the centre, or is the selection method unclear to the extent other patients with similar presentation may not have been reported?
2. Was the exposure adequately ascertained?
3. Was the outcome adequately ascertained?
4. Were other alternative causes that may explain the observation ruled out?
5. Was there a challenge/rechallenge phenomenon?
6. Was there a dose-response effect?
7. Was follow-up long enough for outcomes to occur?
8. Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners to make inferences related to their own practice?
Classification Systems
There were 10 individual classification systems identified which was split into three identified occipital condyle fracture systems, two specialized atlanto-occipital dissociation classifications and five atlas fracture grading schemes (Table 1).
Discussion
Occipital Condyle Fractures
The occipital-atlanto-axial complex relies upon both its geometric shape of its joints, in the form of deep concave atlas facet sockets housing the convex occipital condyles, as well as its ligamentous structures and musculature for stability. 1 The basic movements of flexion and extension are mainly performed at the C0/C1 articulation, whilst axial rotation of up to 47° occurs at the C1/2 joint limited only by the loose atlanto-axial membranes.36,37 However, Van Mameren et al 30 challenged these traditional generalisations by using cineradiographs to image the spine and found that there was no directional or temporal consistency in these ranges of movement. 38 More than this, there is also significant variation between individuals. 37 In fact, up to 3-8 degrees of axial rotation may occur at the atlanto-occipital joint and up to 10 degrees of flexion-extension at the atlanto-axial joint. 39 Yoganadan et al realised the clinical significance of this after examining 6 cadaver head-neck complexes and finding that a reduced atlanto-axial range of motion increases the likelihood of traumatic injury. 40 It is evident that the craniocervical junction is a complex region and this has led to the proposition of a multitude of injury classifications in an attempt to both categorise and guide surgical management.21,27,30,41–43 The AO Spine Upper Cervical Injury Classification System (UCIC) system unites all of these disjointed and at times too detailed systems into a hierarchical validated scheme.44,45
Occipital condyle fractures are traditionally classified by the 1988 Anderson and Montesano system into three types. 21 A type 1 injury is impaction of the occipital condyle occurring as the result of axial loading similar to the force which results in a Jefferson fracture of C1. 21 The ipsilateral alar ligament may be disrupted but the contralateral alar ligament and intact tectorial membrane usually confer mechanical stability. 21 Type 2 fractures represent extension of a basilar skull fracture into the occipital condyle usually as a consequence of a direct force to the head. 21 Given the alar ligaments and tectorial membrane are intact, these injuries are also generally stable. 46 Finally, type 3 fractures are rotational or lateral bending injuries associated with alar ligament avulsion. 21 Werne et al performed cadaveric dissection and found the tectorial membrane limits flexion and extension whilst the strong alar ligaments check lateral flexion and rotation. 47 As such, type 3 injuries are usually deemed to be the most severe in nature and potentially unstable.48,49 Criticisms of the Anderson and Montesano grading scheme include their reliance of the diagnosis of ligamentous integrity using computed tomography before the era of magnetic resonance imaging, and the fact that their case series of six patients included only a single patient with a type 3 injury.21,50
Craniocervical Junction Fractures
Subsequent to this, Tuli et al proposed a new classification system to categorise occipital condyle fractures that was based upon an escalating degree of instability. 23 This retrospective review of 93 cases actually only included three index cases. 23 The authors identified that the stability of the occipital-C1-C2 joint is due to both the fibrous capsule that blends into the anterior and posterior atlanto-occipital membranes as well as superficial and deep ligamentous structures. 23 Tuli et al specifically identified three superficial ligaments of importance as the apical ligament, Barkow's ligament and alar ligament, despite often being overlooked for the more renowned deeper tectorial membrane and cruciate ligament.23,51,52 Type 1 injuries are non-displaced stable injuries which do not require immobilization, type 2A injuries are stable displaced fractures without ligamentous disruption which can be treated with a hard collar and type 2B injuries are unstable displaced with ligamentous disruption requiring a halo or surgical fixation. 23 More specifically, the criteria for instability were proposed to be > 8° of axial rotation of the occiput-C1 to one side, > 1 mm of occiput-C1 translation, > 7 mm of overhang of C1 on C2, > 45° of axial rotation of C1-C2 to one side, > 4 mm of C1-2 translation, < 13-mm distance between the posterior body of C2 to the posterior ring of C1 and an avulsed transverse ligament with ligamentous disruption on MRI. 23
West et al examined both proposed classification systems by performing a retrospective review of 13 363 patients presenting to a single level 1 trauma centre. 53 Of the 46 patients who were found to have an occipital condyle fracture, it was striking that 59% had an associated cervical spine injury but no patient required surgery for the occipital condyle injury. 53 Interestingly, using the Anderson and Montesano system resulted in 28 patients being classified with a type 1 injury, 6 with a type 2 injury and 17 with a type 3 injury.21,53 Conversely, the Tuli classification determined 33 of the injuries were type 1 and 17 were type 2A with strikingly none of the injuries being type 2b.23,53 As such, clinicians are faced with the Tuli classification system that in theory guides management but in practice describes such a rare severe injury that none were observed even in a large cohort of injuries at a trauma centre.23,47–49,53,54 Furthermore, neither of these existing classification schemes take into consideration other important patient factors such as underlying long segment bone disease or presence of a neurological deficit including a lower cranial nerve palsy.23,53,54
In response, Maserati et al attempted to simplify these two landmark occipital condyle fracture classifications by closely examining a series of 24 745 consecutive trauma patients at a level 1 trauma centre.
24
After identifying 100 patients with 106 occipital condyle fractures, it was argued that craniocervical misalignment defined as a condyle-C1 interval > 2.0 mm was the only factor of importance to guide whether the injury was amenable to treatment with an external cervical collar vs immobilization with occipitocervical fusion or halo fixation. However, only two patients in their entire series demonstrated this degree of misalignment and both underwent surgical fixation.
24
Simplifying these existing classifications, the novel AO Spine UCIC system classifies occipital condyle and craniocervical junction injuries into type IA as isolated bony injuries to the condyles, type IB as a non-displaced ligamentous injury and type IC as an injury with displacement on spinal imaging (Figure 2).
54
This rational introduction of injuries is particularly useful for clinician communication. Type 1A injuries are limited to the bony occipital condyle, whereas type 1B are comprised of type 1B non-displaced ligamentous injuries (craniocervical junction). Finally, type 1C are any injury with displacement.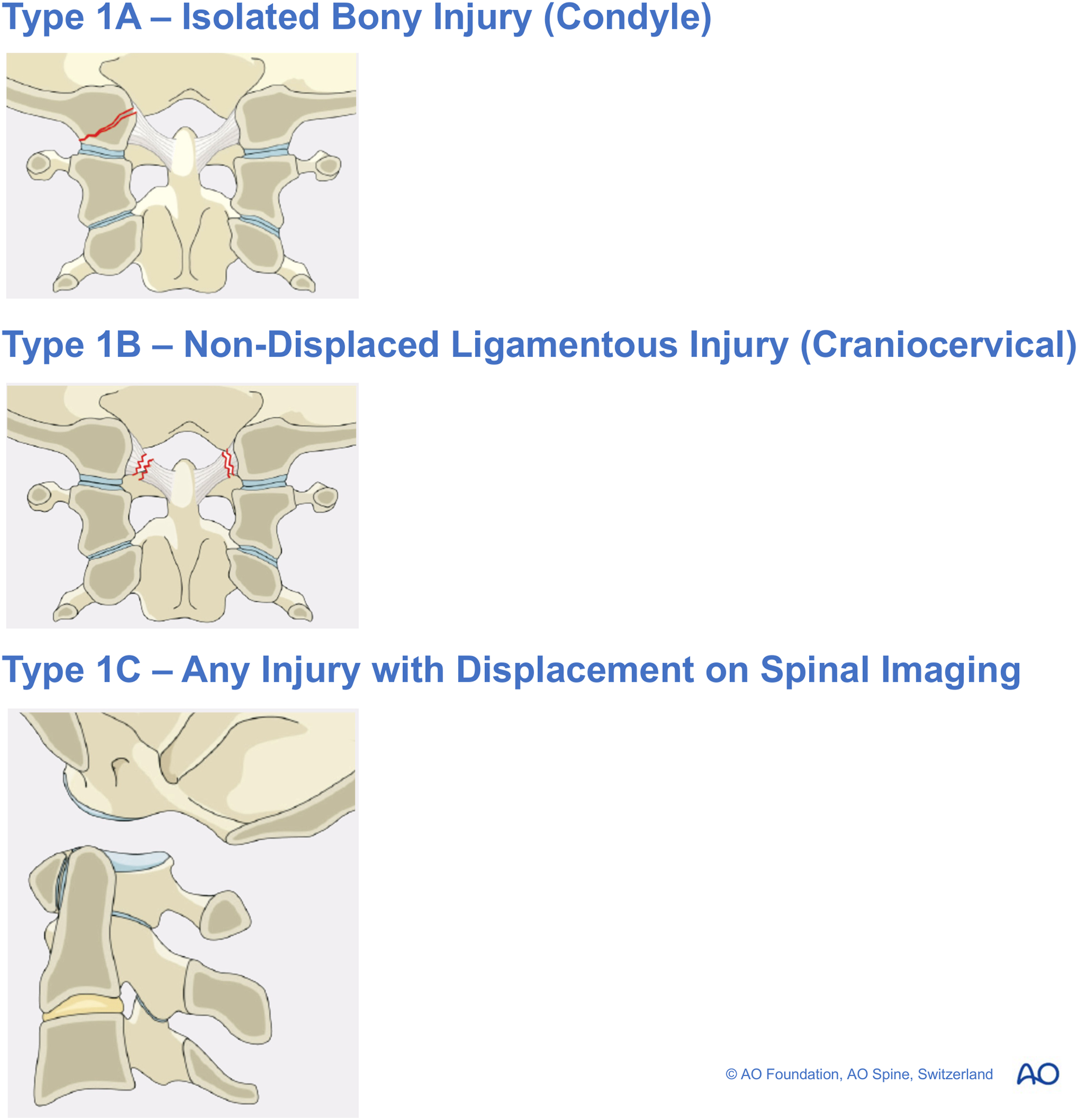
An AO Spine IC injury is consistent with occipital cervical dissociation. 54 This is a severe injury given there is usually almost complete disruption of the ligamentous structures before craniocervical dissociation.55,56 Capuano et al actually believed these injuries were not as rare as believed and had been merely overlooked. 56 . The importance of its recognition as a separate category was underlined by Bohlman et al who, in their series of 300 patients who sustained acute fractures and dislocations of the cervical spine, found a delay in diagnosis in up to one-third of cases. 55 Importantly, the presentation of asymmetrical upper extremity weakness associated with lower cranial nerve palsies raises the suspicion of a cervicomedullary syndrome and should not be overlooked. Despite this, 13 of the 17 patients in one case series were diagnosed in a delayed fashion with an average delay period of 2 days. 26 In a retrospective interrogation of radiographs, the cardinal intervals of the basion-dens interval (BDI) and basion-axion interval (BAI) were abnormal. 26 This was associated with profound neurological deterioration and poorer clinical outcomes. A universal standardized means of detecting this injury is therefore imperative.25,26
The Traynelis classification of atlanto-occipital dissociation is familiar and classifies injuries simply according to the direction of displacement: type 1 is anterior dislocation of the occiput, type 2 longitudinal dislocation and type 3 is posterior dislocation. 25 There is no grading of severity of the injuries and no suggestions as to management with this classification that is simply based on the final resting relationship between the two dissociated structures. 25 Indeed, a major criticism of this classification is that severe instability and disruption of the ligamentous structures based on a methodology reliant on the final displacement of the atlanto-occipital joint at the time of radiograph is almost arbitrary. 26 The entire system is also based upon a single case report. 25
To expand upon this, the Harborview classification proposed by Bellabarba et al attempted to categorise injuries according to degree of spinal stability. 26 Stage 1 injuries include minimal or non-displaced craniocervical dissociation which are generally stable and amenable to conservative management. 26 These injuries may include unilateral alar ligament avulsion or a partial ligamentous injury with ≤ 2 mm of distraction on provocative radiography. 26 Stage 2 injuries are minimally displaced (defined as ≤ 2 mm) dissociative injuries which have spontaneously entirely or at least partly self-reduced. 26 A positive traction test confirms complete loss of ligamentous integrity and these injuries therefore require surgical stabilization. 26 Finally, Stage 3 dissociation is typified by gross craniocervical misalignment with the basion-atlanto interval or basion-dental interval being > 2 mm and these are grossly unstable requiring surgical stabilization. 26
The AO Spine UCIC integrates this injury along a continuum of occipital condyle fractures and a IC injury. 54 It is therefore evident that the AO Spine UCIC system manages to distil all of these disjointed historical classification systems into three simple injury types. The Anderson and Montesano, Tuli and Maserati et al occipital condyle fracture systems are condensed into subtypes IA and IB which guides clinicians with a mechanism of injury as well as stability, whilst the Traynelis and Harbourview classifications are summarized as IC injuries.21,23–26,54
Atlas Fractures
The atlanto-axial junction permits rotation and is composed of the median and lateral atlanto-axial joints. 37 The median atlanto-axial joint lies between the anterior arch of the atlas and the odontoid process, whilst the lateral atlanto-axial joint is formed by any articulation between the lateral masses of C1 and C2.57,58 Steel reported the concept of the rule of thirds which stated that at the level of the atlas the space is equally occupied in thirds by the spinal cord, odontoid process and space. 59 Biomechanically, the atlas ring is merely a passive washer between the head and remainder of the cervical spine. 37
Atlas fractures demonstrate a bimodal distribution and are usually due to high energy trauma in the young population, with a peak at 24 years of age, or low energy trauma in the osteoporotic elderly accounring for a second peak at 80-84 years of age.10,12,60–63 Common mechanisms include diving into shallow water or motor vehicle crashes. 64 Matthiessen et al determined from 1537 Swedish cases of atlas injuries that the majority were in males (56.5%) and C1 injuries constituted 10.6% of cervical spine injuries. 60 There was also an additional cervical spine injury in 19% of cases. Remarkably, Fowler et al and Landells et al both identified an additional C2 fracture in 46% of cases.29,65 Perhaps the greatest strength and weakness of the upper cervical spine is the mobility afforded to it by its complex ligamentous support. 46
Jefferson in 1919 reported four cases of atlas fractures before conducting a thorough review or the literature available at that time. 27 A method classifying fracture subtype purely according to anatomical location was employed with Jefferson listing injuries in which the posterior arch alone was fractured, the anterior arch alone damaged, both arches injured, lateral masses alone disrupted or concurrently the lateral masses and posterior arch bearing the consequences of the force vector. 27 The rationale behind this was the fact that Jefferson astutely noted that the first two cervical nerves are intimately related to the posterior arch of atlas. 66 The greater occipital nerve has a more closely confined canal passing beneath the posterior arch, whereas the suboccipital nerve possesses a wider groove which is co-habited by the vertebral artery. 67 Importantly, although the suboccipital nerve provides motor supply to the muscles of the suboccipital triangle the presence of strong posterior cervical muscles means its division is often not clinically noticeable. 27 Of note, Jefferson observed that cord injury in the presence of burst atlas fractures was absent in 50% of cases. 27
Similar to the Traynelis classification of craniocervical dissociation, the Jefferson system of assigning a category to atlas fractures purely based upon the location of the fracture line is easily reproducible but does not provide any suggestion as to appropriate management. 27 In 1985, Levine and Edwards attempted to address this by analysing 34 patients with C1 fractures. 30 Three main groups of injuries were identified with the first group sustaining bilateral posterior arch fractures, the second group sustaining fractures in the lateral mass region and the final group sustaining the classical Jefferson burst fracture. 30 Levine and Edwards suggested that patients who had fractures with lateral mass overhang between 2 and 7 mm be managed with halo immobilization for 10-12 weeks, whilst those with greater displacement than 7 mm were treated with reduction and delayed stabilization. 30 In other words, Levine and Edwards were relying upon the findings of Spence et al from 1970 which argued that diagnosis of an atlas burst fracture could be identified on an anteroposterior radiograph.30,68 More than this, the degree of the atlas’ lateral mass overhang on the axis was used as a surrogate for whether the transverse atlantal ligament was preserved or disrupted with a high probability of it being intact should the overhang be less than 5.7 mm, and equally for a high probability of its failure the spread should be greater than 6.9 mm. 68 Importantly, clinicians must recognise that if only one arch is fractured there can be no lateral displacement or for that matter atlanto-axial instability. 68
Landells et al expanded upon the 1985 classification proposed by Levine and Edwards by examining their own series of 35 patients with atlas fractures in 1987. 29 There was a stricter definition applied to 3 types of atlas fractures but again it was primarily by anatomical location of the fracture line. 29 Type 1 injuries of a single arch which did not cross the equator of the atlas were believed to be a consequence of a hyperextension force, and these were associated with the highest rate of neurological deficit (20%). Despite being most commonly associated with other cervical spine fractures (81%), these fractures were in general managed conservatively. 29 Due to vertical compression forces and usually occurring in isolation with only 15% demonstrating another cervical spine injury. Type 2 fractures involve both the anterior and posterior arches crossing the equator of the axis representing the archetypal Jefferson fracture. 29 These injuries resulted in a neurological deficit only 8% of the time. 29 Finally, type 3 injuries were the rarest and involve primarily the lateral mass extending into a single arch injury. 29 Landells et al documented six injuries of this nature and only one patient suffered a neurological deficit. 29 Whilst Levine and Edwards recommended 10-12 weeks of immobilization for stable injuries, Landells et al found a period of just six weeks was sometimes adequate.29,30
A more detailed classification was proposed by Gehweiler et al who divided injuries into five subgroups and has been the preferred system in Europe until now.28,69 A type 1 injury is a fracture of the anterior arch, type 2 a predominantly bilateral fracture of the posterior ring and the type 3 being the typical Jefferson burst fracture of the anterior and posterior arches. 69 Type 3 injuries are further divided into stable injuries (3a) if the transverse atlantal ligament is intact vs unstable (3b) if the ligament is lesioned. 69 Type 4 injuries are those of the lateral masses and type 5 are isolated C1 transverse process fractures which require careful interrogation of the vertebral arteries to exclude a traumatic dissection. 69 Gehweiler et al argued that the subtypes 1, 2 and 5 were stable injuries and could be conservatively managed with six weeks of immobilization. 69
The subdivision of Gehweiler type 3 injuries was addressed by Dickman et al with their system in which an isolated ligamentous injury is a type 1 injury and this is further divided into a mid-portion injury (1a) or an avulsion injury (1b) from its insertion. 22 Based upon their case series of 39 patients, all 16 of the patients with a type 1 disruption of the transverse atlantal ligament failed to heal without surgical fixation. 22 Given the stiff and elastic nature of the ligament a mid-substance ligamentous injury is unlikely to heal. In contrast, type 2 injuries are bony injuries in which there is either tubercle avulsion (2a) or a comminuted lateral mass fracture (2b). 22 Whereas all type 1 injuries should be managed operatively, Dickman et al found that although the transverse ligament was physiologically incompetent, given the substance of the ligament itself was not torn, type 2 injuries could be successfully treated 74% of the time non-operatively with a halo brace . 22 Indeed, type 2 injuries should be treated initially conservatively and only fused if there is proven instability after 3-4 months. 22 However, this specialised system focussing entirely upon the transverse atlantal ligament fails to take into consideration the C0-1-2 complex as a whole and the neurological status of the patient. 22
For this reason, Gehweiler et al integrated the excellent work of Dickman et al into the type 3 classification of atlas fractures.22,69 In stable C1 fractures such as 3a injuries, a hard collar is reasonable whilst unstable 3b injuries should be managed operatively.22,69 More specifically, cases of a severely displaced bony avulsion fragments which may not necessarily unite with the lateral mass or a mid-substance transverse atlantal ligamentous injury are likely to require a C1/2 fusion. 28 Finally, there is a broad range of type 4 fractures ranging from minimally displaced to grossly misaligned which require an individual tailored approach. 28 The Gehweiler classification has been independently evaluated by Laubach et al and found to have moderate reliability for assessment of fracture stability (κ = 0.50) and whether operative or non-operative management is indicated (κ = 0.53). 70 However, there still exists discrepancy particularly with respect to the management of type 3b fractures. 70 The ideal management strategy must also take into consideration the fact that 80%-90% of rotation is lost with occipital-cervical fusion and 50% is lost with C1/2 fusion. 71
The AO Spine UCIC simplifies and advances these classification systems based upon degree of stability.44,54 This has been validated and utilized in a practical sense by O’Neill et al and Lambrechts et al.72,73 Type 2A fractures amalgamate all isolated bony arch injuries alone and the majority of these, being an axial loading force with burst mechanism expanding the canal, remain stable and are suitable for conservative management (Figure 3)44,54 This is proceeded by type 2B injuries in which there is transverse atlantal ligamentous injury which Dickman et al further divided, before the more unstable type 2C atlanto-axial instability is introduced (Figure 3).22,44,54 A final strength of this integrating classification is the ability to take into consideration the presence of neurological deficit or whether vascular injury has occurred (Figure 4). Type 2A injuries represent bony only C1 arch fractures, whereas type 2B fractures involve ligamentous injury. The most severe subtype of Type 2C occurs in the setting of atlantoaxial instability/translation. AO Spine classification classifies craniocervical junction injuries into occipital condyle or complex disruptions, C1 or C1/2 injuries and finally C2 as well as C2/3 joint complex fractures.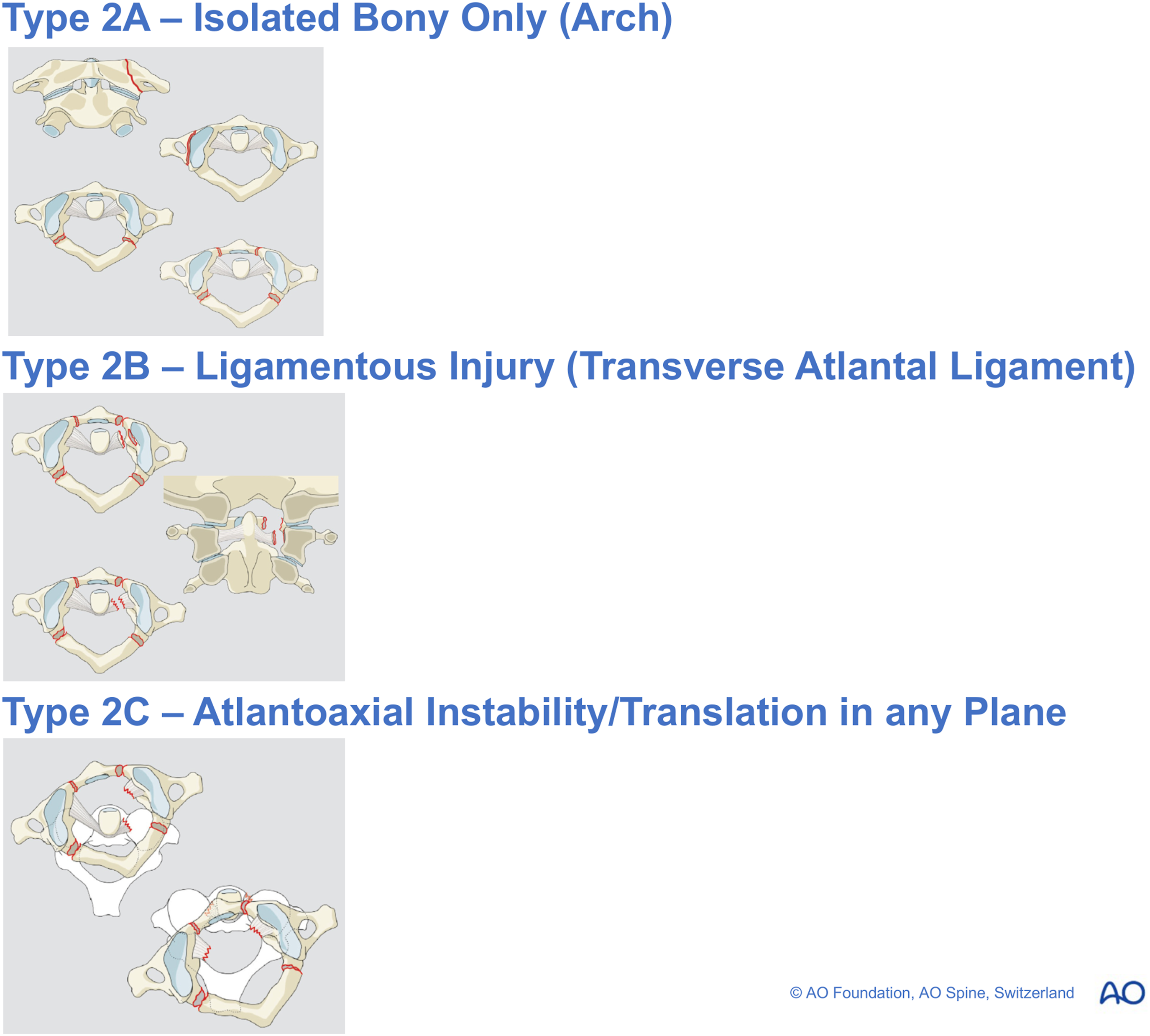
Conclusion
The AO Spine UCIC efficiently summarizes historical classification systems into three categories for injuries of the occipital condyle. Subtypes IA and IB encapsule the traditional Anderson and Montesano, Tuli and Maserati et al injuries, before the more severe IC injuries pay tribute to the Traynelis and Harbourview classifications.21,23–26,54 With respect to atlas injuries, the AO Spine UCIC simplifies injuries into stable Type A injuries being isolated bony injuries through one arch, both anterior and posterior arches or even the lateral mass. 54 This is proceeded by ligamentous injuries in Type B injuries followed by grossly unstable translational injuries in Type C. 54 What is unique is that the AO Spine integrates all the stable Gehwiler subtypes 1, 2 and 5 or Jefferson 1 and 2 subtypes into a single stable category of Type A injuries, followed by Dickman Type 1 or Gehwiler subtype 3 into Type B injuries, and finally the grossly unstable Type C, whilst simultaneously taking into consideration neurological status. 54 This pioneering system therefore represents progression and evolution of existing systems and informs clinicians of the severity of injuries in relation to other fracture morphologies in order to guide surgical decision making.
Supplemental Material
Supplemental Material - Craniocervical Junction and Upper Cervical Spine Fractures: Historical Systems and Advancements with the AO Spine Classification
Supplemental Material for Craniocervical Junction and Upper Cervical Spine Fractures: Historical Systems and Advancements with the AO Spine Classification by Barry Ting Sheen Kweh, MBBS (Honours), Alexander R. Vaccaro, MD, PhD, MBA, Gregory Schroeder, MD, Jose A. Canseco, MD, PhD, Maximilian Reinhold, MD, Mohamed Aly, MD, PhD, MRCS, Sebastian Bigdon, Mohammad El-Skarkawi, MD, PhD, Richard J. Bransford, MD, Andrei Fernandes Joaquim, MD, PhD, Harvinder Singh Chhabra, MBBS, MS (ORTHO), Emiliano Vialle, MD, Rishi M. Kanna, MS, MRCS, FNB, Charlotte Dandurand, MD, MSc, FRCSC, Cumhur Öner, and Jin Wee Tee, BMedSci, MBBS, MD, FRACS in Global Spine Journal
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine, AO Network Clinical Research through the AO Spine Knowledge Forum Trauma.
Ethical Statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.