
Abstract
Study Design:
Retrospective observational study.
Objective:
To establish occipital condyle dimensions (length, width, height), as well as the medialization angle necessary for safe occipital condyle screw placement in occipitocervical fixation.
Methods:
Between 1/2014-6/2014, patients who presented to a single level 1 academic trauma center emergency room and received computed tomography (CT) imaging of the cervical spine as part of routine clinical care were identified. After excluding patients with cervical fractures, neoplastic disease, or infection, 500 condyles representing 250 patients were analyzed. Condyle length, height, and width (all reported in millimeters [mm]) were evaluated on the sagittal, coronal, and axial series, respectively. Medialization angle (reported in degrees) was evaluated on the axial series of CT imaging. Measurements were compared by sex and age.
Results:
The average condyle length, width, and height were 18.6 millimeters (mm) (range, 14.5-23.0 mm), 10.5 mm (range, 7.4-13.8 mm), and 11.3 mm (7.1-15.3 mm), respectively. Additionally, the average occipital condyle medialization angle was 23° (range, 14-32°). Occipital condyles of men were significantly longer, wider, and taller (all comparisons, p < 0.05). The medialization angle was significantly steeper for women than men (p < 0.05). No measurement differences were appreciated by age.
Conclusion:
Our findings are similar to previous studies in the field; however, length appears slightly shorter. Further, measurement differences were appreciated by sex but not age. Thus, our measurement findings emphasize the importance of preoperative planning utilizing individual patient anatomy to ensure safe placement of occipital condyle screws for optimal outcomes.
Introduction
The primary indication for occipitocervical fixation is instability. In general, acute instability occurs secondary to trauma,1-3 while chronic instability occurs typically secondary to neoplasms,4,5 inflammatory processes (e.g., rheumatologic disease), 4 or congenital malformations.5-7 Despite careful preoperative planning, complications are relatively common from surgery and can often lead to debilitating or fatal consequences.8-11 In many instances, the undesirable outcomes may be secondary to the unique anatomy of the occipitocervical junction posing substantial surgical challenges. In many instances, the occiput precludes easy access for instrumentation and provides limited space for the multiple fixation points required as part of appropriate surgical treatment.
Given the surgical challenges in this anatomic area, a variety of different techniques have been employed in search for the one that provides the best clinical outcomes. The literature suggests that modern occipital plate and screw systems are biomechanically superior to older rod and wire constructs12,13; the best occipital bone purchase with midline plates achieved with 12-14 mm screws in the thick occipital midline keel. 12 However, variations in occipital bone thickness or previous/concurrent suboccipital craniectomy can preclude the use of occipital plates in certain cases.12,14 These concerns have led to additional operative strategies being developed, including the inside-outside technique 15 and transarticular technique. 16 However, given the operative challenges that remain, innovative techniques have continued to be sought after to further improve occipitocervical fixation.
First described by Uribe et al in 2008, 17 occipital condyle screws have become an attractive salvage technique or initial approach for occipitocervical instability when other fixation options are not appropriate. In the setting of inadequate surgical fixation or when acceptable occipital plate fixation cannot be achieved, the use of occipital condyles screws has shown promise.14,18,19 The approach has been shown to have a number of key benefits, including being biomechanically equivalent to occipital plating techniques, increasing the occipital surface for arthrodesis, and helping to avoid wound issues associated with prominent occipital plates. 14 However, potential injury to surrounding neurovascular structures remains an area of concern. As a result, detailed knowledge of the dimensions of the occipital condyle and the surrounding anatomy of the occipitocervical junction is critical when placing occipital condyle screws.
Overall, there has been relatively limited literature aiming to define the morphological features of occipital condyles to ensure safe screw placement.20-22 Thus, using the largest patient sample size to date, we aimed to externally validate the morphological features of occipital condyles reported by others. Therefore, the objective of this study was to establish occipital condyle dimensions (length, width, height), as well as the medialization angle necessary for safe occipital condyle screw placement to achieve occipitocervical stabilization.
Methods
This retrospective observational study was approved by the appropriate Institutional Review Board (IRB) under protocol: STUDY00001014.
In this retrospective study, patient charts were reviewed for those presenting between January 2014 and June 2014 to a single Level 1 academic trauma center. Consecutive patients were evaluated. In order to be included in the present study, patients needed to receive computed tomography (CT) imaging of the cervical spine as part of their clinical care. A complete set of CT images were required (axial, sagittal, and coronal). All CT images were taken with the Philips Brilliance 64 CT system. Patients found to have cervical fractures, neoplastic disease, or infection were excluded. Ultimately, A total of 500 condyles, representing 250 patients, were identified and included.
Patient sex (women or men), age (years), body mass index [BMI] (kilograms/meters2), height (meters), and weight (kilograms) were recorded.
Using the acquired CT imaging, condyle length, height, and width (all reported in millimeters [mm]) were evaluated on the sagittal, coronal, and axial series, respectively. The medialization angle (reported in degrees) was evaluated on the axial series. The two-dimensional (2D) images were utilized.
Measurements were conducted by the study team, which included a neurosurgery spine fellow, orthopedic surgery resident, and medical student. Each member was directly instructed by the senior author (AM), a fellowship-trained orthopedic spine surgeon, on the appropriate way to make each measurement. The senior author monitored practice measurements by each team member prior to allowing independent measurements. The picture archiving and communication system (PACS) system was used to access all images, and the bone window was used while determining all measurements.
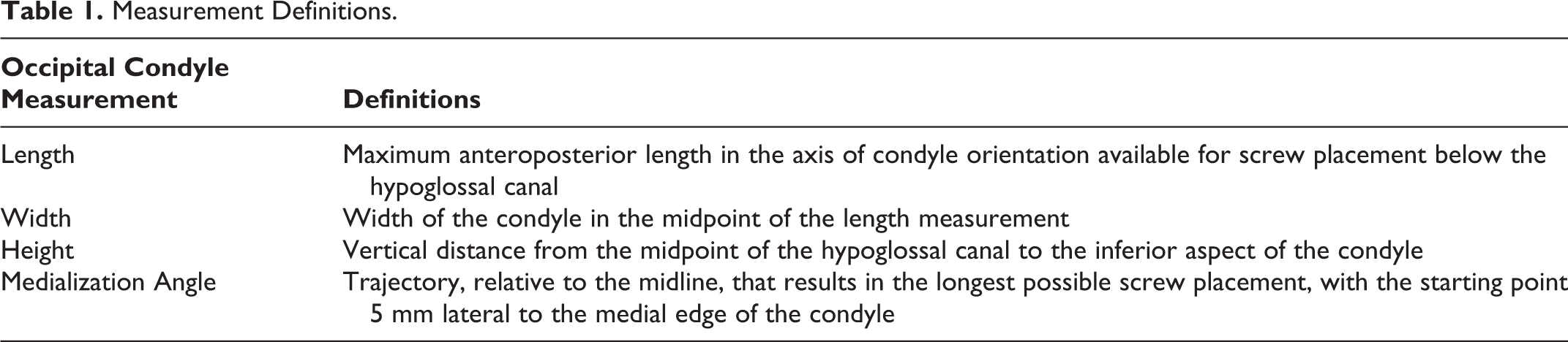
The specific definitions used for each measurement can be seen in Table 1, and an example of representative measurements can be seen in Figure 1.
Measurement Definitions.
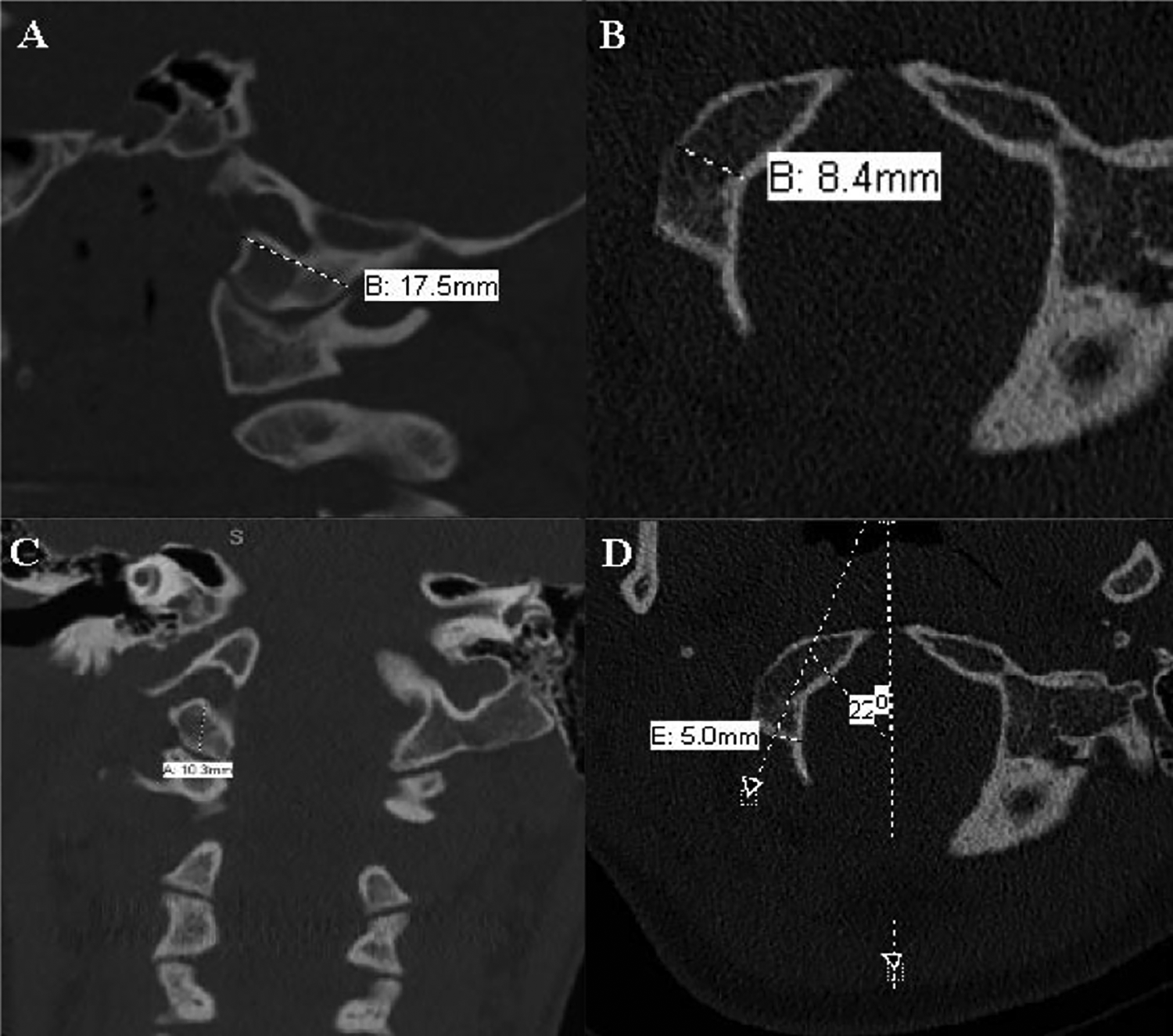
An illustration of the representative measurements used in the present study. A) Occipital condyle length; B) Occipital condyle widtht; C) Occipital condyle height; D) Occipital condyle medialization angle.
All right and left occipital condyle measurements were compared by sex (men versus women) and age (non-elderly [<65 years old] versus elderly [≥ 65 years old]). These comparisons were performed using the Mann-Whitney U test, as the data were not normally distributed.
All statistical analyses conducted using Stata/SE 14.2 for Mac (College Station, TX, USA). A priori, significance was set at p < 0.05.
Results
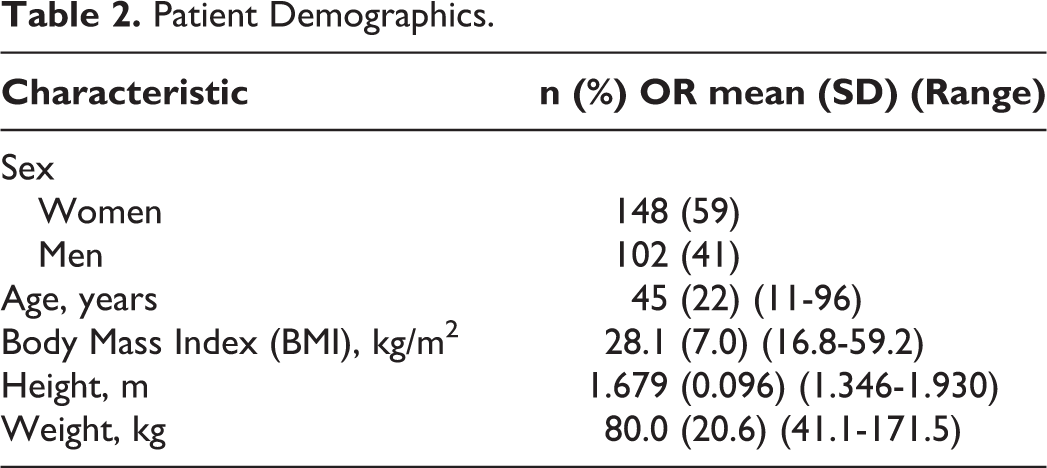
Of the 250 patients (representing 500 occipital condyles) included in the current study, a majority of the patients were women (148 patients [59%], Table 2). The average age and body mass index (BMI) were 45 years (range, 11-96 years) and 28.1 kilogram (kg)/meter (m)2 (range, 16.8-59.2 kg/m2), respectively (Table 2). The average height and weight were 1.679 m (range, 1.346-1.930 m) and 80.0 kg (range 41.1-171.5 kg), respectively (Table 2).
Patient Demographics.
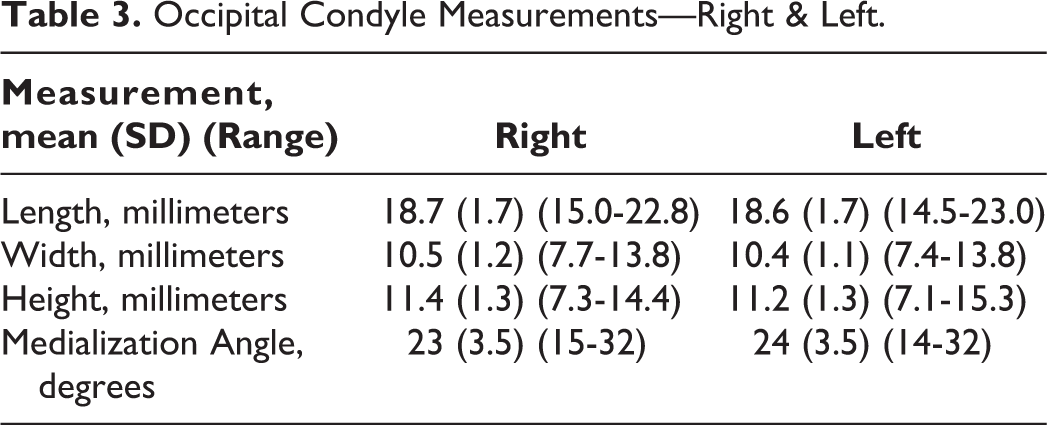
The average measurements with standard deviations and ranges for occipital condyle length, width, and height for both right and left condyles are presented in Table 3. Additionally, the average occipital condyle medialization angles with standard deviation and range for both right and left condyles are presented in Table 3.
Occipital Condyle Measurements—Right & Left.
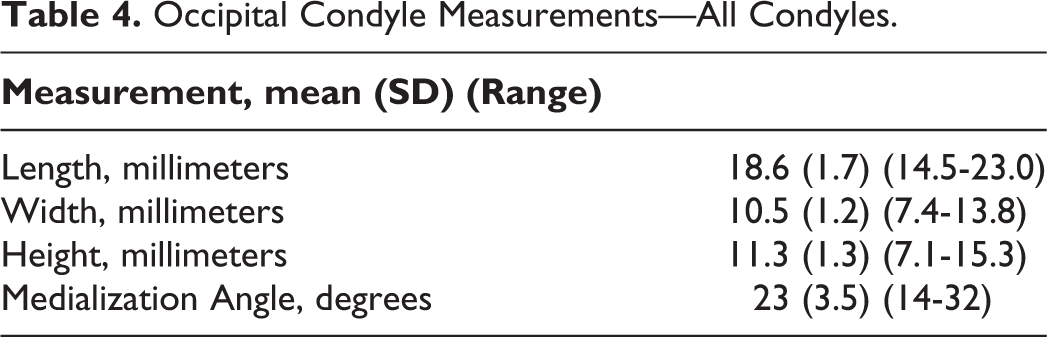
Across all 500 occipital condyles analyzed via CT imaging, the average condyle length, width, and height were 18.6 millimeters (mm) (range, 14.5-23.0 mm), 10.5 mm (range, 7.4-13.8 mm), and 11.3 mm (7.1-15.3 mm), respectively (Table 4). Additionally, the average occipital condyle medialization angle was 23° (range, 14-32°) (Table 4).
Occipital Condyle Measurements—All Condyles.
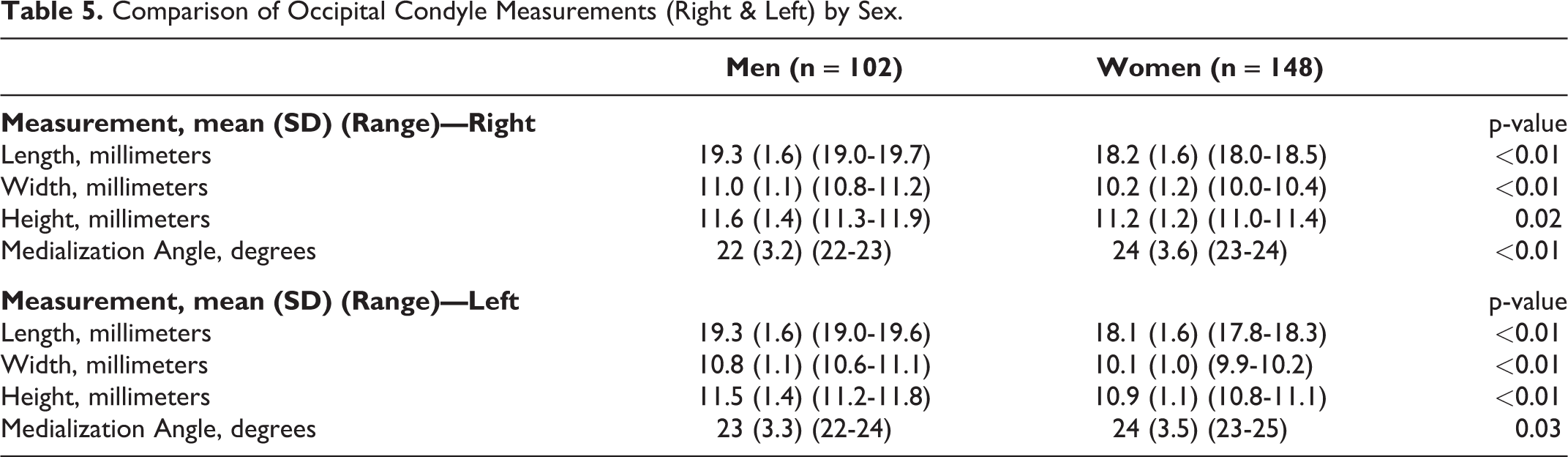
When comparing right and left occipital condyle measurements by sex, the occipital condyles of men were significantly longer (Right: 19.3 mm (19.0-19.7 mm) vs. 18.2 mm (18.0-18.5 mm), p < 0.01; Left: 19.3 mm (19.0-19.6 mm) vs. 18.1 mm (17.8-18.3 mm), p < 0.01), wider (Right: 11.0 mm (10.8-11.2 mm) vs. 10.2 mm (10.0-10.4 mm), p < 0.01; Left: 10.8 mm (10.6-11.1 mm) vs. 10.1 mm (9.9-10.2 mm), p < 0.01), and taller (Right: 11.6 mm (11.3-11.9 mm) vs. 11.2 mm (11.0-11.4 mm), p = 0.02; Left: 11.5 mm (11.2-11.8 mm) vs. 10.9 mm (10.8-11.1 mm), p < 0.01) than those of women (Table 5). Additionally, the medialization angle was slightly, but significantly, steeper for women (Right: 24° (range, 23-24°) vs. 22° (range, 22-23°), p < 0.01; Left: 24° (range, 23-25°) vs. 23° (range, 22-24°), p = 0.03) (Table 5).
Comparison of Occipital Condyle Measurements (Right & Left) by Sex.
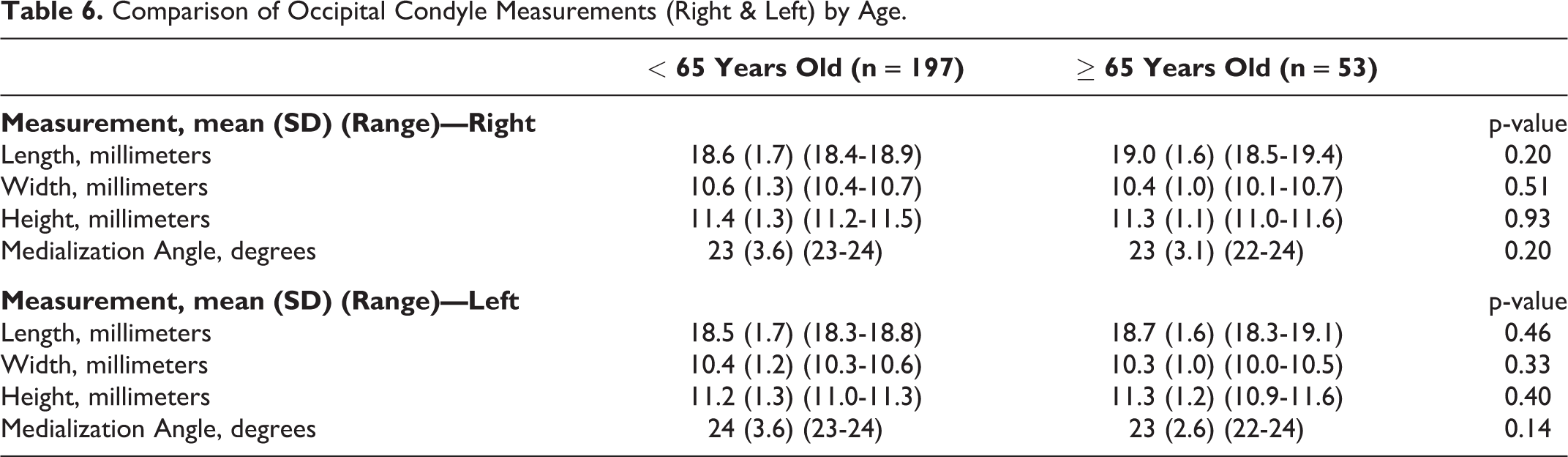
When comparing right and left occipital condyle measurements and medialization angle by age (non-elderly vs. elderly), no significant difference was found (p > 0.05 for all comparisons) (Table 6).
Comparison of Occipital Condyle Measurements (Right & Left) by Age.
Discussion
Occipitocervical instability is a devastating condition with significant morbidity and mortality if left untreated. Surgical management for stabilization is the mainstay of treatment. However, because of technical challenges posed by the unique anatomy of this region spine surgeons have sought innovative techniques. First described in 2008 by Uribe et al, 17 occipital condyle screws have shown promise as an alternative surgical method to traditional techniques.14,18,19 However, in order to ensure outcomes using this technique are as optimal as possible, a robust understanding of the occipital condyle morphology is warranted. To our knowledge, the present study builds upon the previous literature in this area using the largest patient sample size to date. We found that the average condyle length, width, and height were 18.6 mm (range, 14.5-23.0 mm), 10.5 mm (range, 7.4-13.8 mm), and 11.3 mm (7.1-15.3 mm), respectively, and the average occipital condyle medialization angle was 23° (range, 14-32°). These findings suggest that most occipital condyles should be able to easily accept a commonly used 3.5 mm diameter screw, and, on average across all patients, the maximum bicortical length available for screw placement is 18.6 mm. However, when taking sex into account, men have significantly longer, wider, and taller occipital condyles than women, which may alter what constitutes acceptable screws. Therefore, our findings emphasize the role of preoperative planning with individual patient anatomy, as the ranges can be quite large and sex- and possibly other patient factors- may play in occipital condyle morphology.
The present study must be evaluated with its limitations considered. First, while our patient sample is the largest analyzed to date from our knowledge, all CT scans were still gathered from patients presenting to an emergency department at a single institution; thus, it is possible that our findings may not be generalizable to other populations. Second, it is possible that slight variations between co-authors in measurement technique could alter our reported findings. Indeed, we did not perform inter- and intra-rater reliability tests on measurements. However, the appropriate technique for making accurate measurements of occipital condyles on 2D CT scans was provided by the senior author (AM), a fellowship-trained orthopedic spine surgeon, to all participating co-authors, providing an important level of measurement consistency. Third, 3-dimensional (3D) CT reconstruction images were not used for any measurements. Future research can consider the use of 3D CT reconstruction images to help further confirm occipital condyle morphology. Fourth, the patient sample in the current study includes only patients without known injury or pathology in the occiput and/or cervical spine region; thus, our findings should be used with caution in patients needing operative management with overlying injury or pathology. Fifth, our patient sample includes 14 patients (5.6% of 250 patients) less than 18 years of age (average: 45 years [range, 11-96 years]). Because there may be slight developmental differences in this population, we feel it is important to make this transparent to readers. However, we believe it is appropriate to include such patients given our goal of providing an overarching set of occipital condyle measurement estimates. Further this portion of patients make up a small percentage of the total patient sample in the setting of a clear understanding that our findings should be used as a guideline only by spine surgeons. Despite our limitations, we feel the present study provides important insight on occipital condyle morphology that can be used as the starting point for future studies and individualized clinical care.
One of the more notable findings in the present study is our measured occipital condyle length at 18.6 mm (14.5-23.0 mm) across all patients. Compared to previous CT imaging-based and cadaveric studies,21-23 our calculated mean length is notably smaller. For example, Zhou et al, 21 Le et al, 22 and Naderi et al 23 reported mean occipital condyle lengths of 19.3 ± 1.9 mm, 22.38 ± 2.19 mm, and 23.4 ± 2.5 mm, respectively. However, of importance, Zhou et al report that patient sex impacts occipital condyle length with women having shorter occipital condyle length than men. 21 Therefore, it is plausible that our finding is secondary to our patient sample being nearly 60% women. Further, we also found that women, on average, had significantly shorter occipital condyle length than men. Overall, there is a wide range of occipital condyle lengths observed across multiple studies, including the present study. This emphasizes the fact that surgeons should use our findings as a baseline but should consider each patient’s own anatomy.
In summary, surgery involving the occipitocervical junction presents a number of technical challenges to surgeons. This has led to advances in surgical technique aimed at improving patient outcomes. One such operative method includes the use of occipital condyle screws, which requires an understanding of numerous morphological parameters to ensure appropriate placement and decrease the risk of any neurovascular complications. The present study utilized the largest patient sample size to date to calculate 4 key occipital condyle measurements: length, width, height, and medialization angle. In general, our findings are relatively consistent with the prior literature. Therefore, one could view our work as robust confirmation of the present literature. However, the minor discrepancies reinforce the importance of using our findings as a guideline. Individual patient anatomy should be carefully taken into account via radiographic analysis preoperatively to avoid any complications.
Footnotes
Authors’ Note
The Manuscript submitted does not contain information about medical device(s)/drug(s).).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval/Research Ethics Committee Statement
The following work was performed at the Department of Orthopaedics & Physical Performance, University of Rochester, Rochester, NY, USA. The project was approved by our IRB: STUDY00001014. Per the approved protocol, individual patient informed consent was not required.