
Abstract
Study Design
Retrospective, cross-sectional study.
Objectives
Occipitocervical fusion is indicated for various conditions. Some techniques require placement of screws in the occipital condyle. The objective of this study was to analyze the morphometric features of the occipital condyle among Arabs.
Methods
Computed tomography (CT)-based morphometric analysis of occipital condyles of 200 Arab skeletally mature patients (400 condyles) was done. Axial width of at least 8 mm and coronal height of at least 6.5 mm are the cutoff values for feasibility of condylar screw placement.
Results
The mean age of the patients was 48.0 ± 18.3 years. Males were 53.5% (107) of the sample. The mean axial condylar width and length were 8.5 ± 1.5 mm and 20.3 ± 2.6 mm, respectively, while the mean axial screw angle was 35.9° ± 5.5° from midline. The mean sagittal condylar length and height were 16.1 ± 1.9 mm and 8.8 ± 1.5 mm, respectively. The mean condylar coronal height was 8.2 ± 1.4 mm. Based on axial width and coronal height measurements, 150 (37.5%) condyles could safely fit a 3.5 mm condylar screw. One hundred and four (55.9% female condyles) condyles cannot fit a screw in females, while 46 (21.5% male condyles) condyles cannot fit a screw in males.
Conclusions
Condylar screw for occipitocervical fusion is feasible for the majority of Arabs in our sample; however, this applies to slightly less than half of the female condyles. Detailed preoperative radiological planning is critical to avoid complications related to occipital condyle screw placement.
Introduction
Several conditions or injuries of the upper cervical spine, such as trauma, congenital malformations and tumors, can lead to acute or chronic occipitocervical instability.1-8 To avoid serious consequences, occipitocervical fixation is indicated.9,10
Occipitocervical fixation techniques have evolved over the years to optimize treatment outcomes and avoid undesirable consequences from the possible surgical complications with this surgical intervention. Trials of simple posterior onlay bone grafting resulted in high failure rate. 9 This has led to the development of rigid posterior fixation techniques utilizing screws, plates, wires and rods, which provided better biomechanical stability than simple bone grafting.4-7,9-13 Results from the use of the modern plate and screws systems are favorable; however, this technique is not feasible for all patients due to the variations of occipital bone thickness among the patients or having a suboccipital craniectomy.4-7,9-13 Therefore, techniques for occipitocervical fusion are advancing to overcome surgical challenges.
In 2008, Uribe et al described the posterior application of occipital condyle screws for occipitocervical fixation. 14 This technique is biomechanically equivalent to occipital plate and screws, but it has the advantage of preventing wound complications that are associated with the prominent plates.14-17 Also, using the occipital condyle screw technique provides more occipital surface for the bony fusion.9,10,14,17 Placing a screw in the occipital condyle, however, can result in serious complications due to the complex anatomy of the craniovertebral junction, as the condyles are surrounded by the hypoglossal canal, vertebral artery, internal carotid artery, jugular bulb and posterior condylar foramen.14,17,18 Based on previous investigations, the condyle needs to have a minimal axial width of 8 mm to safely fit a 3.5 mm screw with a 4-5 mm margin lateral to the foramen magnum, as well as a minimal coronal condylar height of 6.5 mm for the screw to be 1.5 mm cranial to the atlantooccipital joint and 1.5 mm away from the hypoglossal canal.14,17,18 Accordingly, performing this technique requires thorough preoperative planning and understanding of the detailed anatomy of the upper cervical spine region.
Aiming to ensure surgical safety with posterior condylar screws placement, researchers have studied the detailed morphology of the occipital condyle.18-25 Nevertheless, no study was based on Arab patients. Therefore, the goal of the current study was to assess the feasibility of occipital condyle screws among Arabs by examining occipital condyle morphometric details.
Materials and Methods
Subjects and Setting
A retrospective review of 200 CT scans of the cranial and cervical spine was carried out at a general hospital in Kuwait. The scans included were obtained between September 2023 to January 2023. The inclusion criteria were patients that were Arabs, skeletally mature, and had no evidence of upper cervical spine trauma, deformity, infection, tumor or surgery (ie, normal upper cervical spine). The study protocol was reviewed and approved by our local institutional review board. In such retrospective radiology-based study, informed consent from the patients is not required based on our institutional protocols.
The images were obtained using a 64-slice multidetector CT scanner (highspeed QX/i; GE Medical Systems, Milwaukee, WI, WI). The gantry rotation speed was 0.8 seconds per rotation. Images were obtained while the patients lying in supine position. Slice thickness of 5 mm, pitch of 1.5, table speed of 15 mm per rotation, reconstruction interval of 2 mm, tube voltage of 120 kV, and tube current of 200 mA were used during the scanning process. The transferred transverse CT scans were reviewed as digital images using a picture archiving and communication system workstation monitor (Advantage Windows 4.7, GE, USA). Coronal and sagittal multiplanar images (MPR) were reconstructed. The morphometric measures of the occipital condyle were obtained by a consultant radiologist.
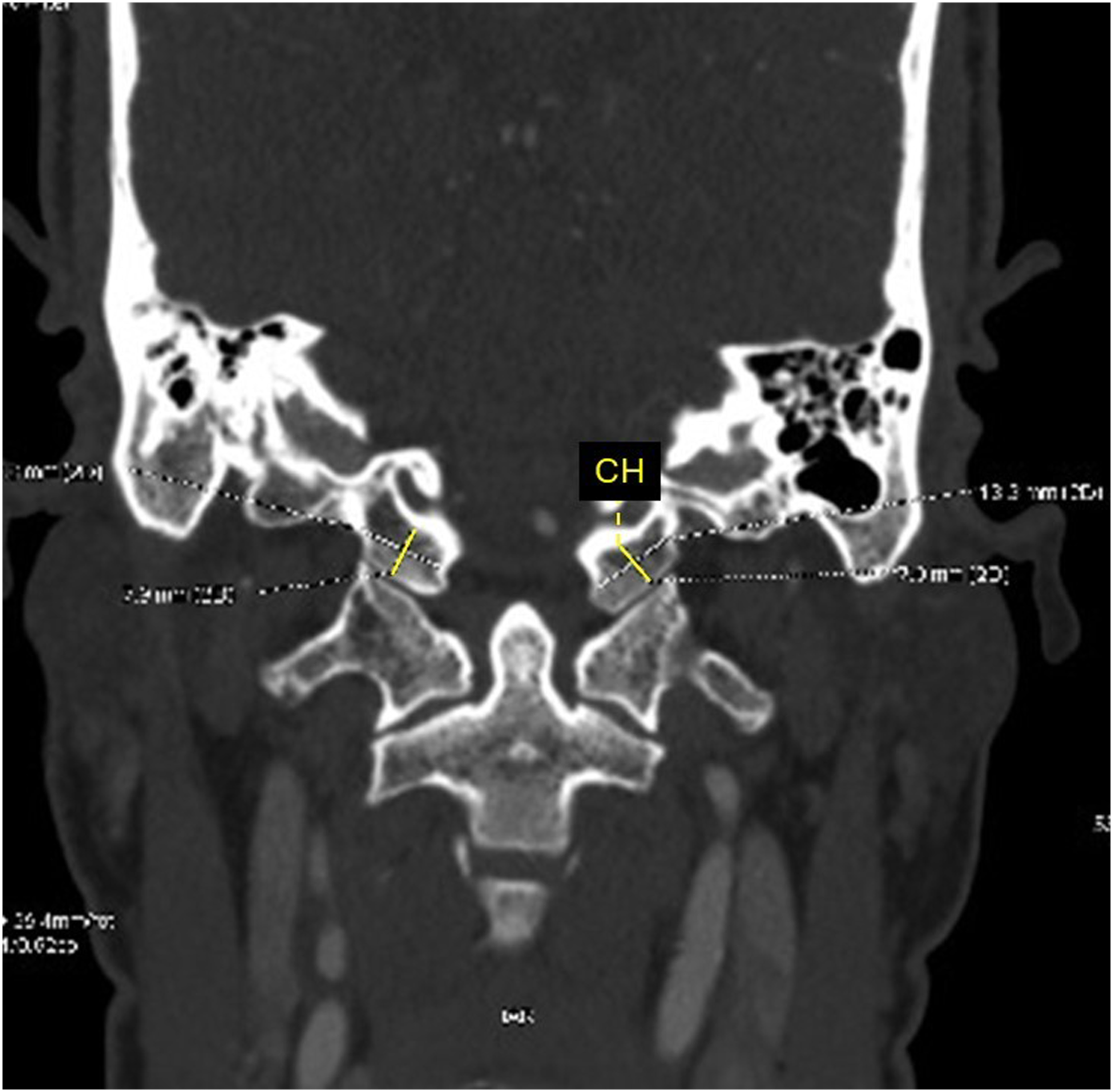
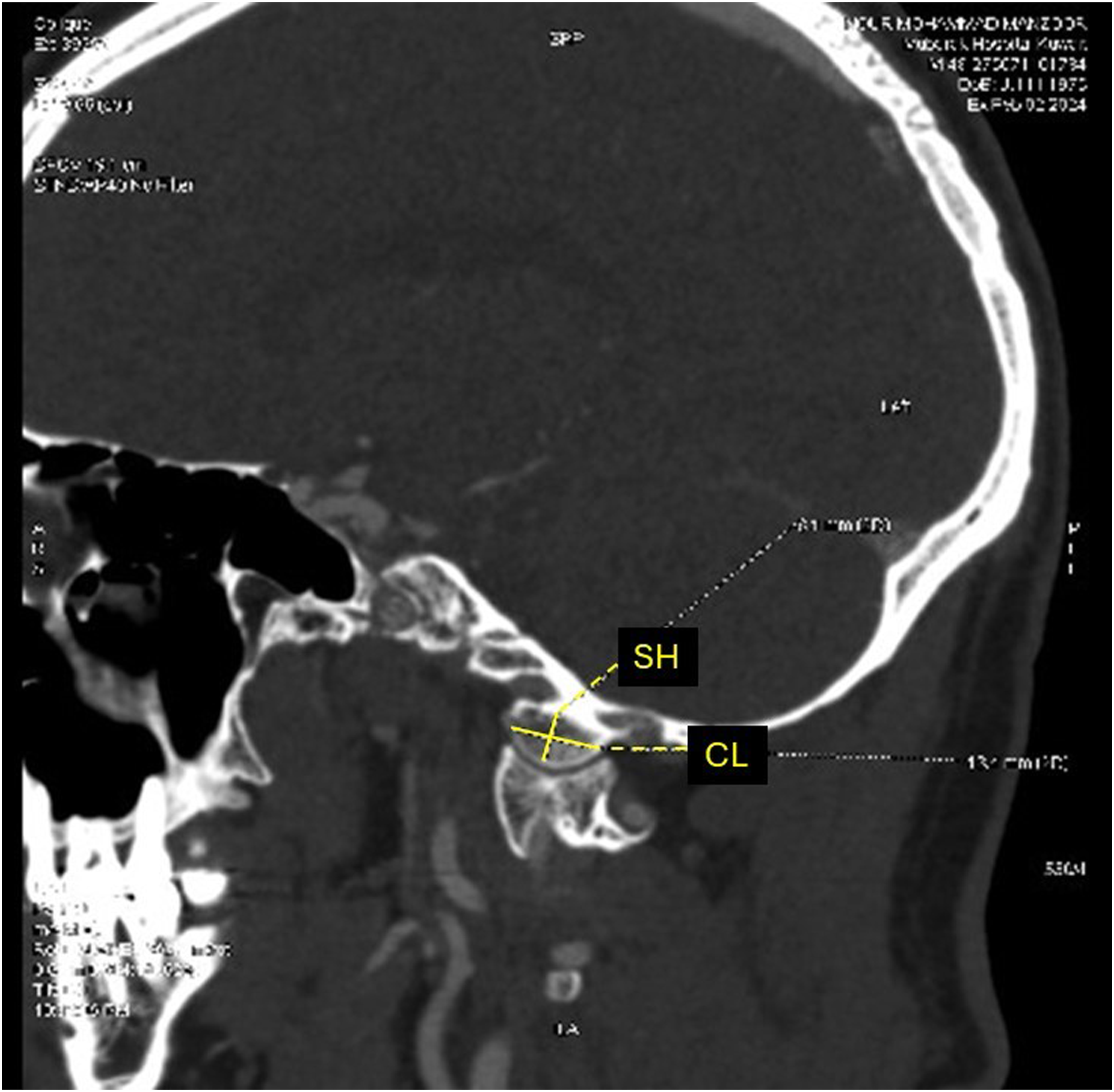
Two hundred patients (400 occipital condyles) were included. Previously described morphometric measurements of the occipital condyle were assessed for each patient, which included the condylar anteroposterior (AP) length, transverse width, height, projected screw angle, and projected screw lengths along the long axis of the condyle (Figures 1-3).18-25 On the sagittal plane, length was measured as the longest axis in the AP orientation (Figure 3), while the transverse width was measured using a line perpendicular to the midpoint of the long axis on the axial plane (Figure 1). Height was measured in the sagittal (Figure 3) and coronal (Figure 2) planes perpendicularly from the hypoglossal canal to the condylar cartilage. The screw length was measured from the outer cortex of the posterior wall to the outer cortex of the anterior wall (Figure 1), while the projected screw trajectory (ie, screw angle) was along the long axis in the center of the condyle (Figure 1). Condylar screw placement was considered feasible if the condyle had a minimal axial width of 8 mm and a minimal coronal condylar height of 6.5 mm.14,18,22 In the axial plane, condylar width of 8 mm would allow a safety margin between 0.5 to 1.5 mm for a 3.5 mm screw inserted 4 to 5 mm lateral to the foramen magnum, while coronal height of 6.5 mm would allow safe insertion of a 3.5 mm condylar screw at a distance of 1.5 mm rostral to the atlantooccipital joint and 1.5 mm distant to the hypoglossal canal.14,17,18,22 Computed tomography (CT) scan axial view of the occipital condyle showing measurements of the condylar width (CW), screw length (SL) and screw angle (SA). Computed tomography (CT) scan coronal view of the occipital condyle showing measurement of the coronal height (CH). Computed tomography (CT) scan sagittal view of the occipital condyle showing measurements of the condylar length (CL) and sagittal height (SH).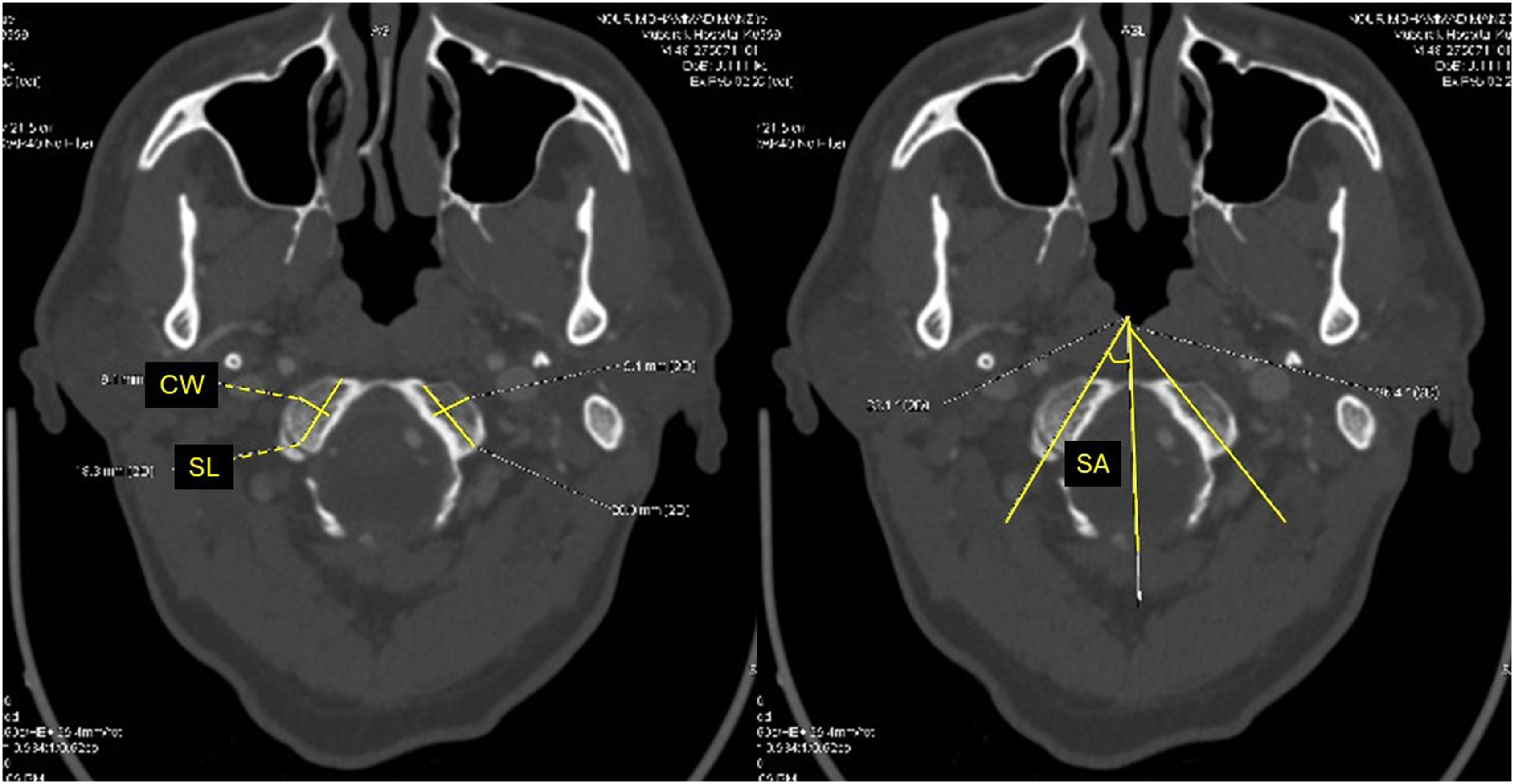
Statistical Analysis
The collected data was analyzed using the Statistical Package for Social Sciences software version 28.0 (SPSS Inc, Chicago, IL, USA). Descriptive results were measured for all the variables, including frequencies, percentages, means, standard deviation (SD) and range. The association between patients’ sex and the CT-based measures of the occipital condyle was evaluated using the t test and chi-square test. A P-value of ≤0.05 was used as the cut-off level of statistical significance.
Results
The mean age of the patients is 48.0 ± 18.3 years (range: 16-87). Out of the 200 patients, 107 (53.5%) were males.
Computed Tomography (CT)-Based Morphometric Features of the Occipital Condyle of Arab Patients (N = 200 Patients, 400 Condyles).
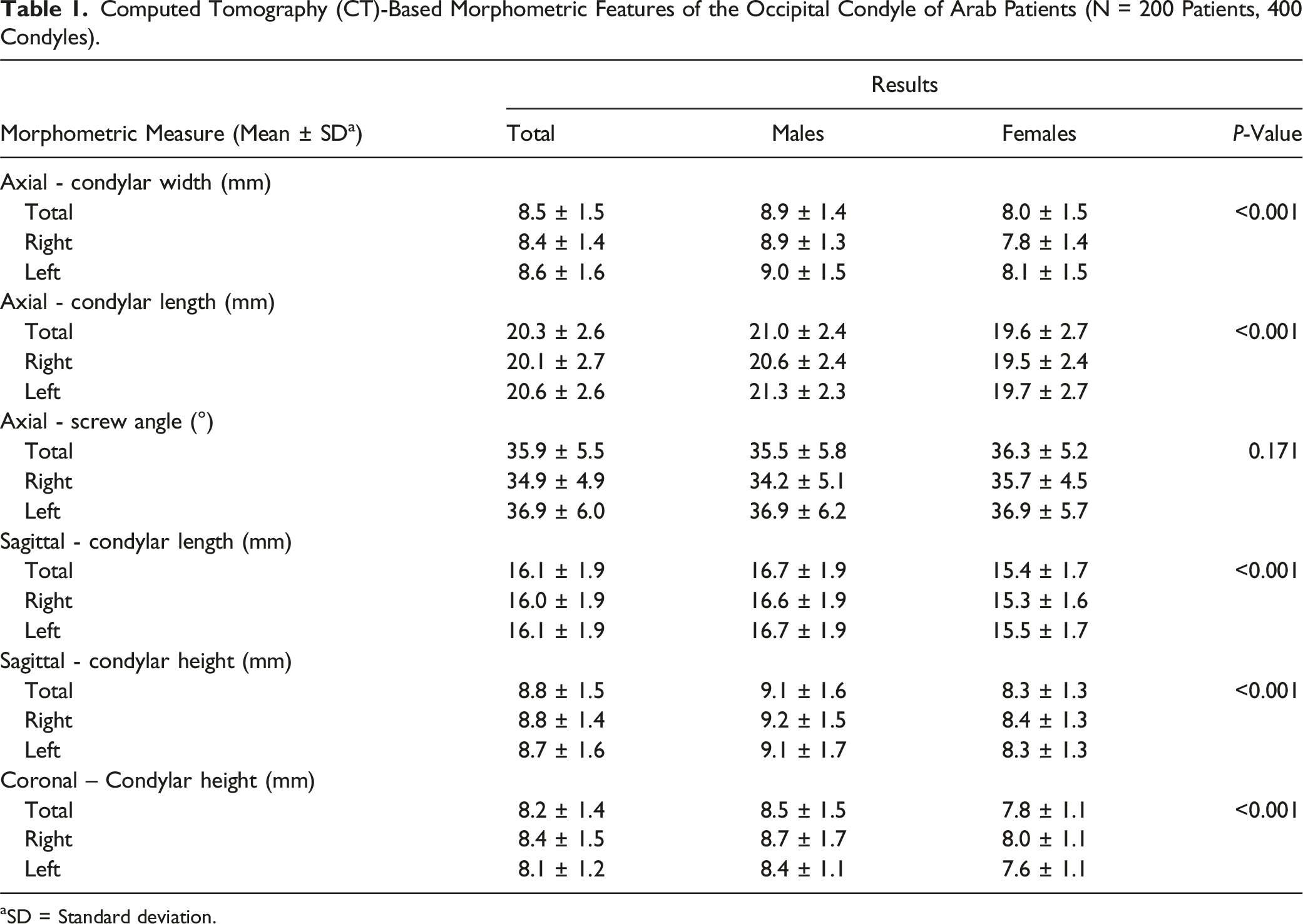
aSD = Standard deviation.
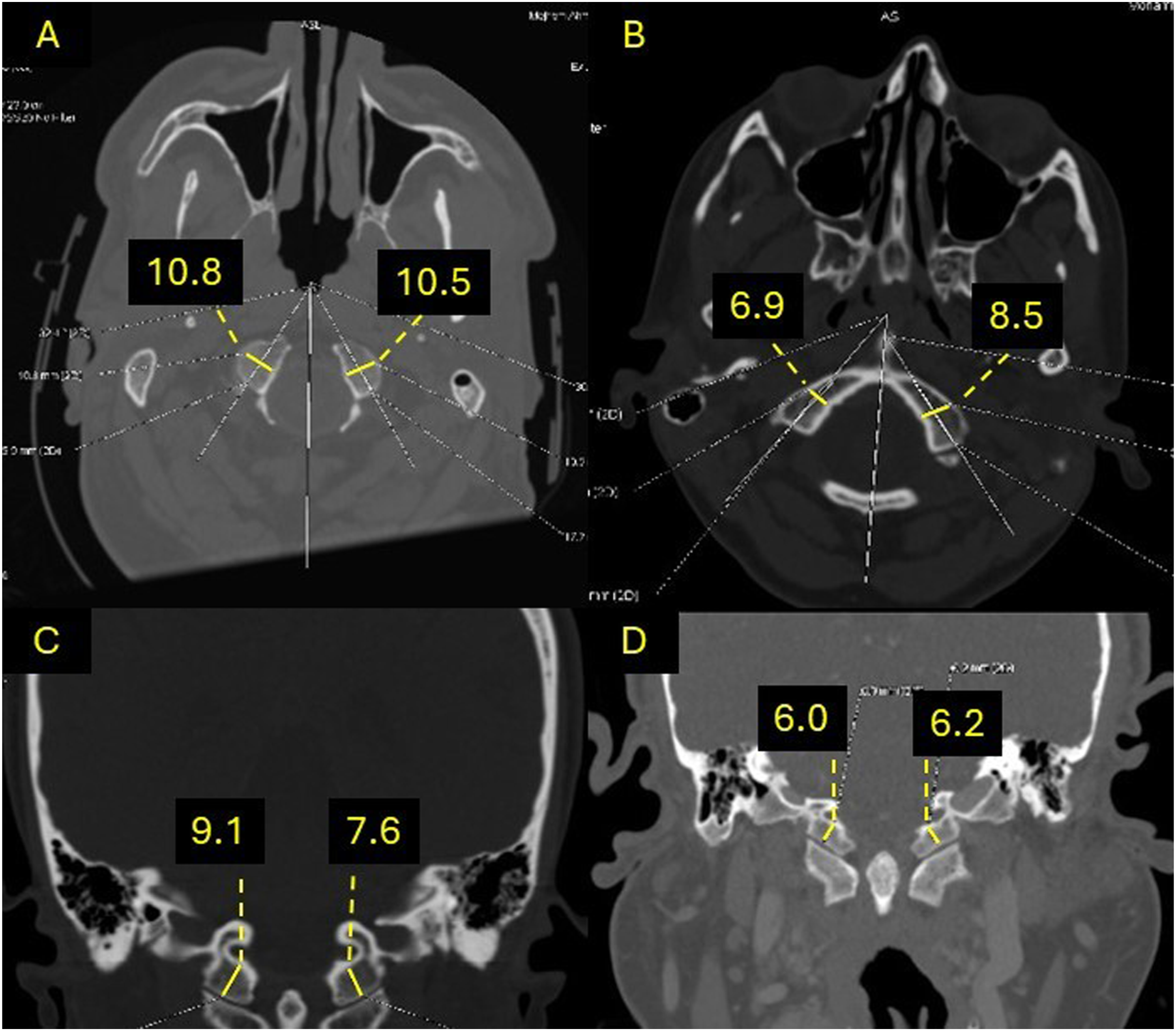
Figure 4 shows the number of occipital condyles that can safely fit a 3.5 mm condylar screw. Based on the axial condylar width and coronal condylar height, occipital condyle screw is not feasible in 150 (37.5%) condyles, with the small axial condylar width being the main limiting factor for this surgical technique. The majority of condyles among females (104; 55.9%) cannot fit a 3.5 mm screw, while only 46 (21.5%) condyles cannot fit a screw in males (P < 0.001). Examples of condyles with different morphometric features are demonstrated in Figure 5. Number of occipital condyles feasible for condylar screw among Arabs (N = 200 patients, 400 condyles). Occipital condyles morphometric measurements from different patients using computed tomography (CT) scan. (A) Condyles with axial width measuring more than 8.0 mm (feasible for screw); (B) Axial width of the right condyle is 6.9 mm (not feasible for screw) and left condyle is 8.5 mm (feasible for screw); (C) Condyles with coronal height measuring more than 6.5 mm (feasible for screw); (D) Condyles with coronal height measuring less than 6.5 mm (not feasible for screw).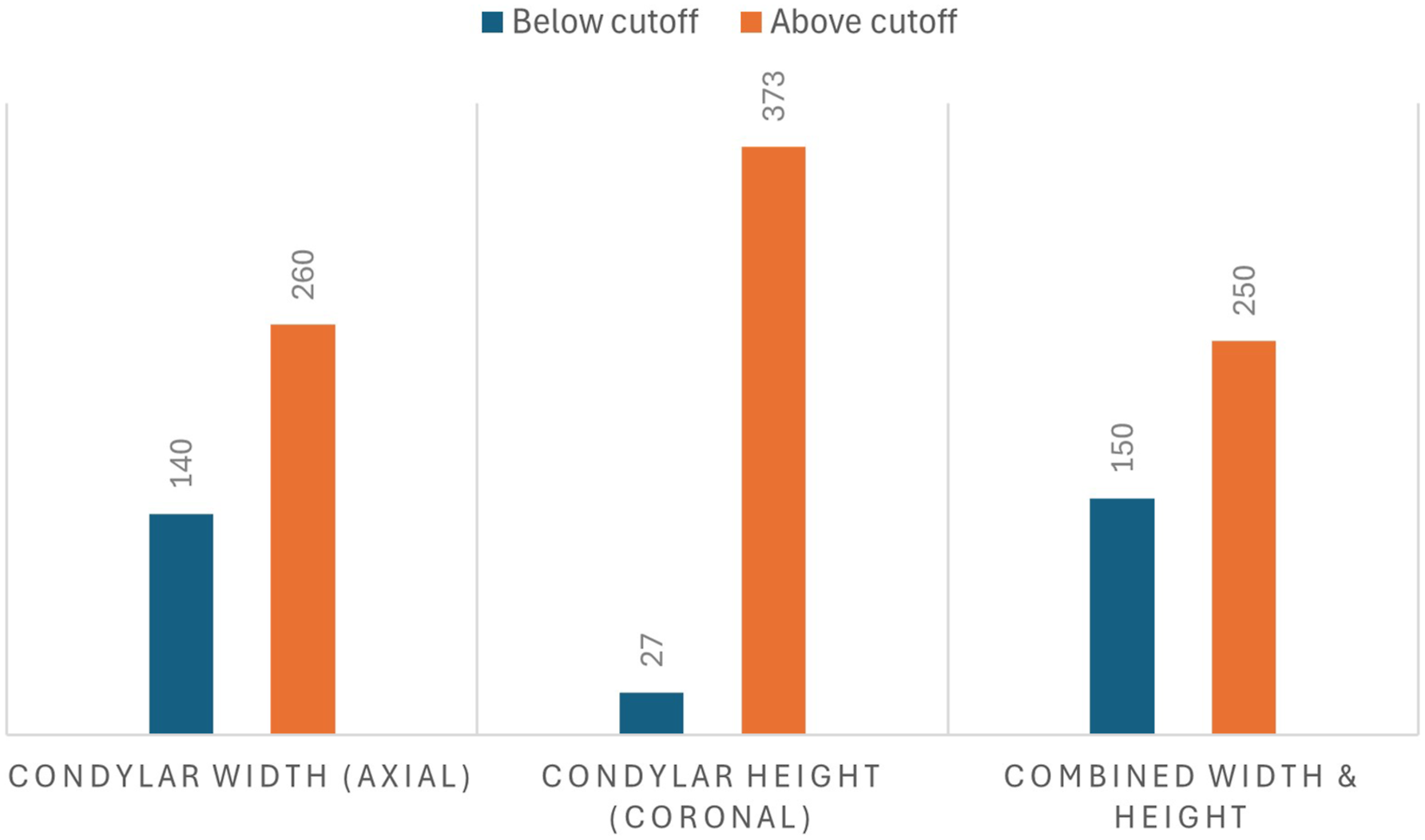
Discussion
Surgical options to treat occipitocervical instability have been advancing to overcome the challenges of the complex regional anatomy of the craniocervical junction. Since its description in 2008, favorable outcomes have been reported with the use of occipital condyle screws for occipitocervical fixation. 14 This technique requires a robust understanding of the morphological anatomy of the occipital condyle to minimize complications and gain desirable outcomes. To our knowledge, the morphology of the occipital condyle of Arabs have not been reported in the literature before. According to the CT-based morphometric measurements in the current study, and based on the feasibility criteria described in the literature (minimal condylar axial width of 8 mm and coronal height of 6.5 mm), placing a 3.5 mm screw in the occipital condyle can be safely done in around 2 thirds of Arab adults.14,17,18 The results, however, demonstrate that this technique is feasible in less than half of the female Arabs. These findings highlight the importance of preoperative planning when indicating an Arab patient for occipitocervical fusion using condylar screws. Moreover, spine surgeons treating Arabs should be familiar with other surgical techniques to address occipitocervical instability in case the patient’s occipital condylar dimensions cannot fit a 3.5 mm screw.
Several studies have reported the CT-based morphometric anatomy of the occipital condyle among different ethnic groups.18-25 Studies from the USA reported a mean axial width and coronal height ranging from 10.5 to 11.2 and 9.9 to 11.3 mm, respectively.19,20,25 On the other hand, the mean axial width and coronal height among Indians was 9.5 to 10.3 mm and 8.5 to 9.0 mm, respectively.22,23 A study from Turkey reported a mean axial width of 10.3 mm and mean coronal height of 9.1 mm. 24 In comparison to our sample of Arab individuals, all other ethnic groups had wider and larger occipital condyles. Placing a 3.5 mm screw in the occipital condyle seems to be more feasible and safer in ethnic groups other than Arabs, a finding similar to what was found in previous investigations regarding the morphometric features of the odontoid process and the subaxial cervical spine pedicles among Arabs.26,27 Knowing this, the spine surgeon should be more careful when indicating an Arab patient for occipital condyle screw placement for occipitocervical fusion.
The occipital condyle is surrounded by the vertebral artery, internal carotid artery, hypoglossal canal containing the hypoglossal nerve, jugular bulb, spinal cord and posterior condylar foramen.17,28 Several complications can result during occipital condyle screw placement due to lack of knowledge of the condyle anatomy and poor preoperative planning. 17 A thorough preoperative CT scan analysis is mandated for occipitocervical fusion and can help prevent complications.14,17-19,28 For example, knowing the condylar height available for occipital condyle screw placement is needed to avoid penetration of the hypoglossal canal superior to the occipital condyle which can result in injury to the hypoglossal nerve. Moreover, measuring the axial width of the condyle and the ideal screw trajectory in this plane can help avoiding screw penetration of the medial and lateral cortices of the condyle, thus preventing injury to the spinal cord or jugular bulb.
When reading and interpreting the findings of this study, the readers should keep in mind some limitations. Arab people from different geographic regions (ie, North Africa vs Southwest Asia) could have different morphometric anatomic features. This subjects’ background characteristic was not investigated in this study. Also, data about the patients’ stature and body mass index were not collected and studied in the current and previous studies. Future studies should look into the relationship of these features and the morphometry of the occipital condyle.
In conclusion, condylar screw for occipitocervical fusion is feasible for the majority of Arabs in our sample; however, this applies to slightly less than half of the female condyles. Detailed preoperative radiological planning is critical to avoid complications related to occipital condyle screw placement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.