
Abstract
We present a literature review of current approaches to craniocervical traumatic injuries. In an attempt to categorize the injuries that involve the upper cervical spine, we divide the injuries into two groups: (1) injuries affecting mainly bone structures and (2) predominantly ligamentous injury. This division is based on the principle that bone injuries have the potential to heal with conservative treatment whereas ligamentous injury would not heal properly, leading to an unstable spine. An accurate diagnosis and treatment are necessary to improve patient's outcome and avoid complications. As a general rule, ligamentous injuries are unstable lesions, requiring surgical treatment. Bony injuries can be conservatively treated, with surgery reserved for more unstable patterns (unstable C1 ring, displaced odontoid or C2 pars fractures).
Craniocervical traumatic injuries represent a small number of cervical spine injuries, affecting the skull base, the atlas, and the axis. 1 , 2 They are generally associated with high-energy trauma; most of them are caused by motor vehicle accidents, but they also can be secondary to low-energy injuries, like a ground-level fall in older individuals with bone fragility.23–4 The complex and unique anatomy and strong stability related to the ligamentous status of this region result in some peculiarities that distinguish this group of injuries from the subaxial cervical spine. 3 , 4 The craniocervical junction is also biomechanically responsible for the majority of axial rotation at the atlantoaxial complex and the greatest range of flexion and extension at the occiput–C1 joint. 5
In this article, we present a brief overview of the most common craniocervical traumatic injuries and their diagnosis and treatment.
Diagnostic Imaging
After the initial evaluation and patient stabilization, screening for spinal injuries should be performed in a standard fashion. Clinical signs of injury (ecchymosis, tenderness to palpation) and neurological examination are of paramount importance and may guide additional imaging given the suspicion of spinal trauma.
Craniocervical injuries were traditionally classified and diagnosed based on plain X-ray examination.6,7–8 However, computed tomography (CT) scans, with axial, sagittal, and coronal reconstructions, are available in a large number of trauma centers and allow for a more detailed evaluation of the craniocervical region, even in patients with severe systemic trauma. 9 Magnetic resonance image (MRI) should be reserved for assessment of the injured spinal cord or when the ligamentous status of the upper cervical spine cannot clearly be inferred based on the CT data. 3 , 4 , 10
Injuries of the Craniocervical Region
In an attempt to categorize the injuries that involve the upper cervical spine, we divide the injuries into two groups: (1) injuries affecting mainly bone structures and (2) predominantly ligamentous injury. This division is based on the principle that bone injuries have the potential to heal with conservative treatment, whereas ligamentous injury would not heal properly, leading to an unstable spine.
Bone Injuries
Occipital Condyle Fractures
Occipital condyle fractures, although reportedly rare in isolation, are more commonly identified with the use of CT, compared with plain radiographs. The presence of lower cranial nerve deficits, basal cranial injury, or persistent neck pain should lead to a suspicious of these injuries, which can be found isolated or in association with other cervical spine injuries or with atlantooccipital dissociation (AOD). 11 The diagnosis of the condyle fractures can be made with a CT scan with sagittal and coronal reconstructions. An MRI may be considered to evaluate the ligamentous status of the occipitocervical joint.
Treatment is based on instability of the occipito–C1 joint, represented by clear displacement of the condyle–C1 lateral mass or the presence of ligamentous injury on the CT scan or MRI. 2 , 11 Anderson and Montesano have proposed a classification system based on three types of injuries 12 (Table 1), with type 3 fractures being the most unstable and suggesting the presence of AOD.
Classification of the Occipital Condyle Fractures According to Anderson and Montesano 12
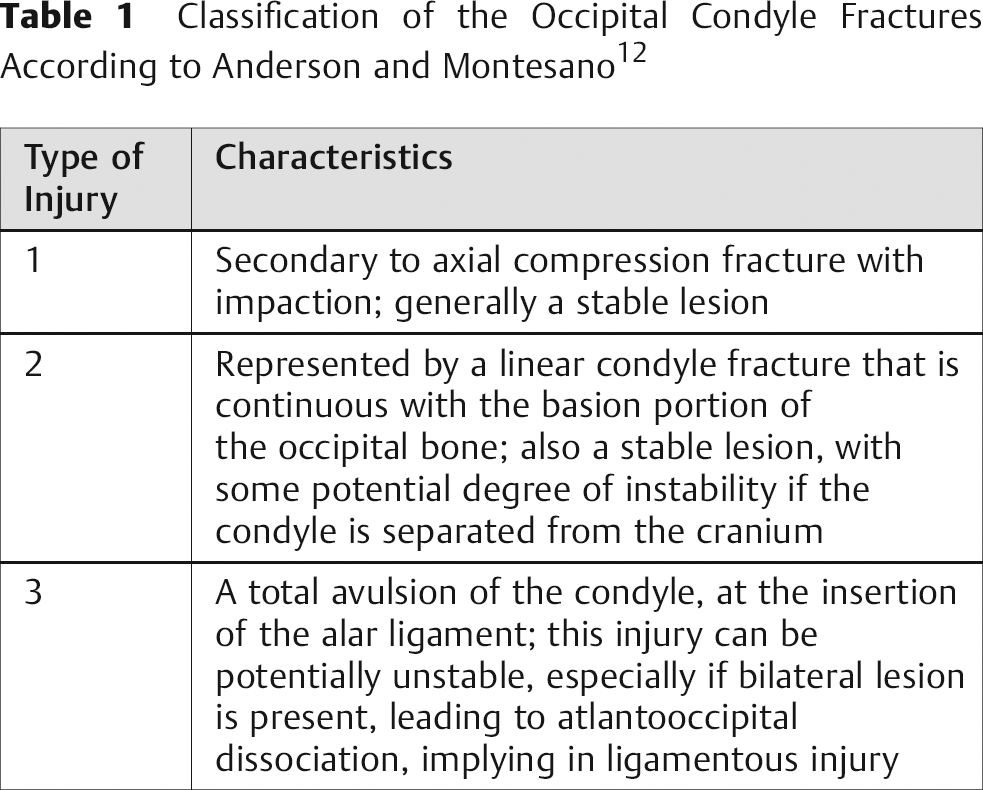
Treatment of stable occipital condyle fractures is generally performed either with a rigid cervical orthosis or with halo vest immobilization. Given the reported risks of halo vest immobilization in the elderly, cervical collars are commonly utilized in this age group. 13 If an associated ligamentous injury or AOD is detected, as in type 3 injuries, an occipitocervical fusion is advised (see section on occipitocervical dislocation [OCD]). 2 , 14 There is no level I or II evidence documenting the outcomes of treatment for occipital condyle fracture.
Atlas Fractures
Atlas fractures represent ∼15% of cervical spine fractures. 15 Atlas fractures may occur with both high-energy and low-energy trauma. High-energy injuries may be seen in combination with AOD. The diagnosis and classification of the atlas fractures can be best made using a CT scan with sagittal and coronal reconstructions. Fractures of the atlas can involve the anterior arch, posterior arch, combined arch fractures (this latter group is also known as Jefferson fractures), and lateral mass fractures. Associated fractures of the axis may exist as well as signs of AOD.
Treatment of atlas fractures can be done successfully with external immobilization with a cervical collar or halo vest. Surgical decision making for atlas fractures is based on the stability of the C1–2 articulation. Instability may be present with a concomitant odontoid fracture or with disruption of the transverse ligament. Transverse ligamentous injury can be suspected when lateral mass separation, as measured on an anteroposterior radiograph or coronal CT, is detected (more than 6.9 mm). 16 Flexion and extension plain radiographs may also demonstrate C1–2 instability. MRI may also be of additional value in the diagnosis of transverse ligament injuries; however, there is no high-quality evidence documenting its sensitivity or specificity. In patients with C1–2 instability associated with atlas fractures, surgical stabilization and arthrodesis of the C1–2 vertebra are recommended. 17
Axis Fractures
Odontoid Fractures
These are the most common injuries of the axis, representing ∼15% of all cervical spine fractures. 18 Many fracture patterns have been described, suggesting different degrees of clinical instability. Some odontoid fractures have similar biomechanical properties of transverse ligament injuries, resulting in loss of the translational restriction of C1 on C2 and creating the potential for spinal cord injury when healing is not obtained. 6 Although the diagnosis can be made with routine plain radiographs in the lateral and/or open-mouth views, CT scans with sagittal and coronal reconstructions allow for a detailed characterization of the fracture characteristics—fracture location, involvement of the C1–2 facet joint, extension into the C2 body, degree of comminution or displacement of bone fragments, and fracture alignment.
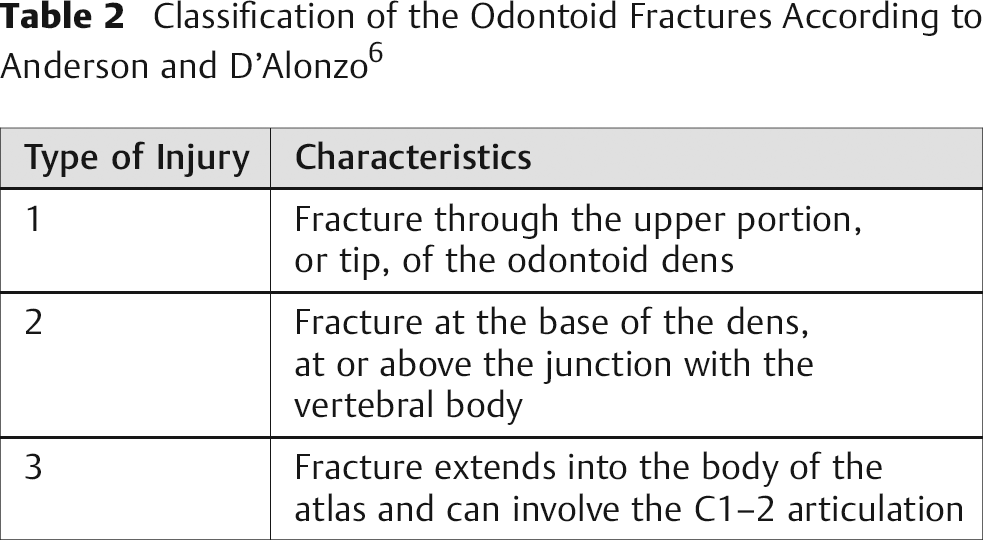
One of the most common classification systems of odontoid fractures is the Anderson and D'Alonzo system, based on three fracture patterns 6 (Table 2).
Classification of the Odontoid Fractures According to Anderson and D'Alonzo 6
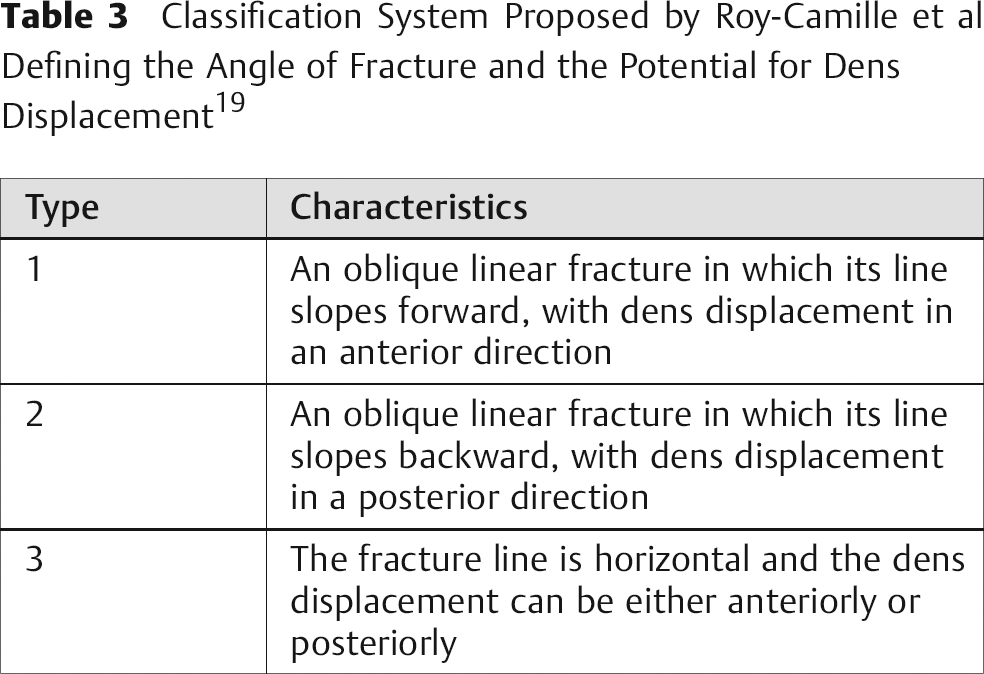
In 1988, Hadley et al proposed a variation of the type II fracture. 15 This new pattern is characterized by the comminution of the fracture at the base of the dens. The system described by Roy-Camille et al 19 defines three types of fractures according to the angle of fracture line and the potential for dens displacement (Table 3).
Classification System Proposed by Roy-Camille et al Defining the Angle of Fracture and the Potential for Dens Displacement 19
The treatment for odontoid fractures is based on many factors: fracture pattern, patient age, degree of comminution, fragment displacement, and angulation. Type I and type III injuries can be typically be managed with cervical immobilization, such as a collar or halo vest. In type III injuries with severe comminution, a halo vest immobilization is recommended. 20 Type II fractures (according to Anderson and D'Alonzo system) 6 are generally surgically treated in older patients (more than 50 years) and patients with rupture of the transverse ligament, severe dens displacement (>6 mm), or type IIA fractures. 21 In such cases, either anterior or posterior fixation options are available. A posterior stabilization of the C1–2 vertebrae can be performed with many posterior fixation techniques available including wires or, more recently, screws.2223–24 An anterior odontoid screw can be used in patients without rupture of the transverse ligament and with a favorable fracture pattern (slopes anterocranial to posterocaudal) and more acute fractures. 25 Anterior screw fixation is contraindicated in patients with severe fracture comminution, unfavorable fracture pattern (slopes anterocaudal to posterocranial), irreducible fracture displacement, or a large barrel-type chest, which can prevent an appropriate path of access to odontoid fixation. 25
Fracture of the Posterior Elements of the Axis
These injuries are also known as “traumatic spondylolisthesis of the axis” or “hangman's fracture.” These fractures make up ∼7 to 20% of cervical fractures. 26 , 27 They can be caused by two mechanisms, one with distraction and hyperextension (such as the injuries in the axis caused hanging) and the other by hyperextension, compression, and a rebound in flexion (as in high-energy motor-vehicle traumas), associated with head injury. 2 , 8
The most widely used classification system for these injuries was the proposed by Effendi et al and then modified by Levine and Edwards. 7 , 8 This system divides these injuries in three types, based on pretreatment lateral cervical plain radiographs. The injuries were described based on the degree of angulation between the second and the third vertebrae (Table 4).
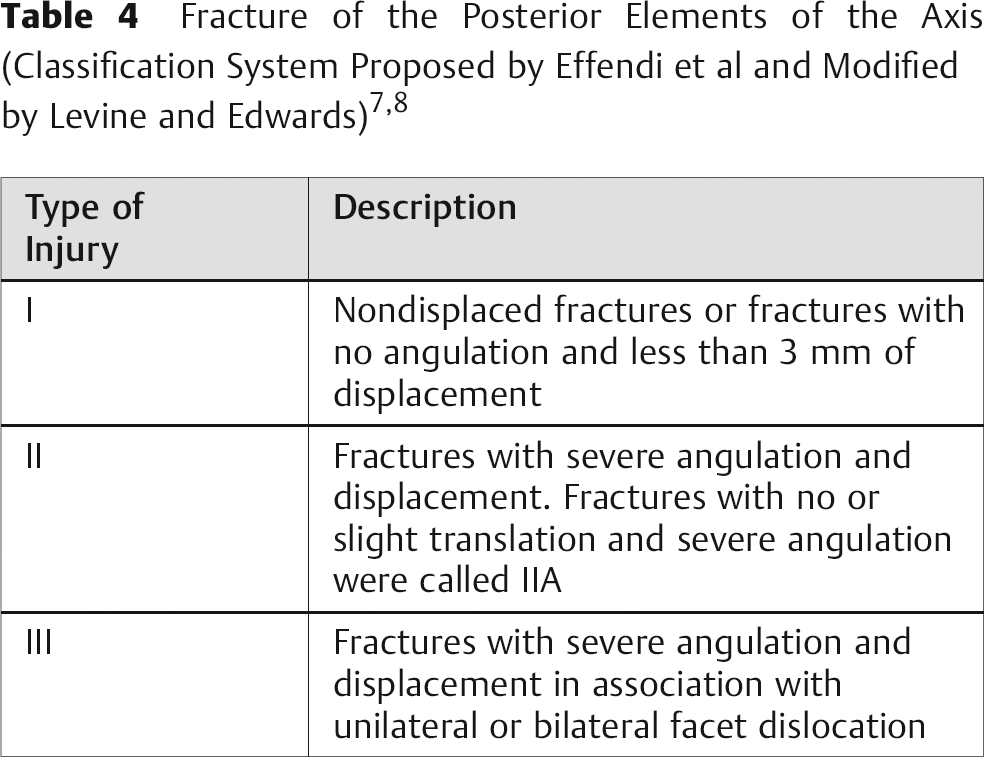
The treatment of C2 pars fractures is based upon implied instability of the injury pattern. Wide fracture displacement, severe fracture angulation, disruption of the C2–3 disc space, and dislocation of the facet joint are all reported operative indications. 2 Closed treatment, though, remains the most common form of treatment. Nondisplaced C2 pars fractures may be treated in either a rigid cervical orthosis or halo vest immobilization. Closed halo traction reduction can be safely performed to reduce and maintain displaced or angled fracture patterns. Traction reduction in the setting of type III fractures is difficult to obtain given the presence of the pars fracture and the facet dislocation. These are often treated surgically. Surgically indicated fractures may be treated with a posterior arthrodesis typically involved C2–3 or C1–3 depending upon fixation method and fracture morphology. Direct osteosynthesis of the C2 pars fracture has been anecdotally discussed but it does not have supporting evidence. 28
Ligamentous Injuries
Occipitocervical Dislocation
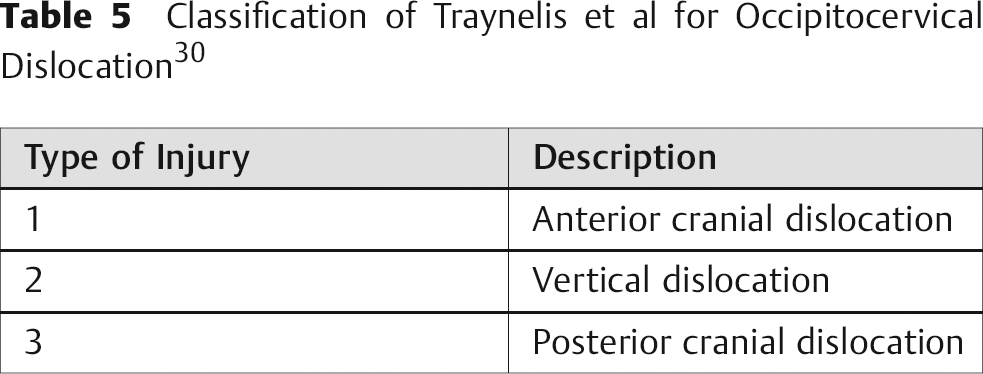
OCD is a rare and severe traumatic situation, commonly fatal. 29 This injury is highly unstable and should be surgically stabilized as soon as possible. Traynelis et al 30 proposed a classification of these injuries according to the cranial dislocation, shown in Table 5.
Classification of Traynelis et al for Occipitocervical Dislocation 30
Many plain radiographs measurements have been proposed to diagnosis AOD, included that proposed by Powers (Powers ratio) et al and others.313233–34 However, sometimes these measurements cannot be performed on plain radiographs and have not demonstrated good reproducibility. 2 CT scans with sagittal and coronal reconstructions provide greater detail of the occipital condyles and C1 lateral masses and are the preferred diagnostic mode. 2 , 3 , 4 Dislocation or distraction across the occipital-cervical junction suggests AOD. Other signs include displaced occipital condyle fractures, fractures of the dens, and marked soft tissue swelling in the prevertebral space. Other comorbidities add to the suspicion of OCD, including subarachnoid hemorrhage in the posterior fossa, cranial nerves palsy, and high spinal cord lesions. 2 , 3 , 4 MRI may be of value to assess the craniocervical junction in cases where CT and physical exam are inconclusive.
Treatment of the OCD initially consists of rigid immobilization including halo vest stabilization. Despite temporary fixation, patients are at risk for progressive neurological decline. 2 Definitive treatment typically consists of surgical stabilization with an occipitocervical fusion. 35
Transverse Ligament Injury
Transverse ligament injury can lead to translational instability of the C1–2 vertebra. Though this is thought to occur most commonly in the setting of widely displaced C1 ring fractures, radiological features have been described for diagnosis transverse ligament injury. This includes an atlanto-dens interval greater than 3 mm and, more recently and possibly more accurately, an MRI showing transverse ligament torn. 2 , 3 , 4 The evidence on the role of MRI is, however, limited.
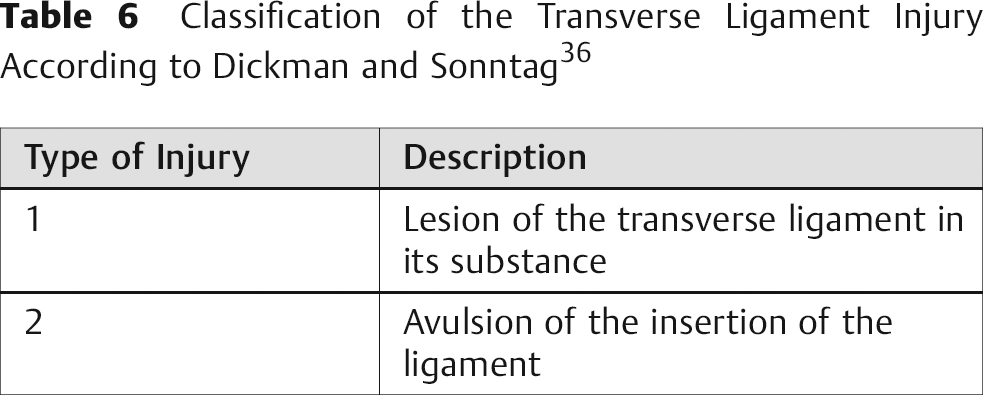
Dickman and Sonntag classified the transverse ligament injury in two types, according to the MRI findings 36 as shown in Table 6. Based on this classification, type 1 injuries should be surgically treated, as the potential for healing of a midsubstance ligamentous injury is unlikely. However, because of the possibility of bone healing in type 2 injuries, a trial of external immobilization can be an option. 36 Instability of the C1–2 articulation due to transverse ligament disruption is most commonly treated through a posterior C1–2 arthrodesis using either wire or screw fixation.
Classification of the Transverse Ligament Injury According to Dickman and Sonntag 36
Conclusion
Diagnosis and treatment of craniocervical traumatic injuries remain a challenge for spine surgeons. The complexity of the anatomic stabilizers of the upper cervical spine combined with challenges in diagnostic imaging make surgical decision making difficult. An accurate diagnosis and treatment are necessary to improve the patient's outcome and avoid complications, such as neurological deterioration. As a general rule, ligamentous injuries are unstable lesions requiring surgical treatment. Bony injuries can be conservatively treated, with surgery reserved for more unstable patterns (unstable C1 ring, displaced odontoid or C2 pars fractures).